www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Adult
tonsillectomy:
postoperative
pain
depends
on
indications
夽
Olaf
Zagólski
a,∗,
Mariusz
Gajda
b,
Paweł
Str˛
ek
c,
Michael
John
Kozlowski
b,
Artur
G˛
adek
d,
Jerzy
Nyzio
aaSt.JohnGrande’sHospital,ENTDaySurgeryDepartment,Kraków,Poland bJagiellonianUniversityMedicalCollege,DepartmentofHistology,Kraków,Poland cJagiellonianUniversityMedicalCollege,DepartmentofOtolaryngology,Kraków,Poland dUniversityHospital,DepartmentofOrthopedicsandRehabilitation,Kraków,Poland
Received8May2015;accepted5November2015 Availableonline16February2016
KEYWORDS
Palatinetonsils; Tonsillectomy; Lasertonsillectomy; Tonsillitis;
Pain; Nervefibers
Abstract
Introduction:Intense painisoneofthemostimportantpostoperative complaintsafter ton-sillectomy. Itisoftendescribed bypatientsascomparabletothepainthataccompaniesan acutetonsillitis.Althoughrecurrenttonsillitisisthemostfrequentindicationforsurgery,many tonsillectomiesareperformedduetootherindicationsandthesepatientsmaybeunfamiliar withsuchpain.
Objective: Toverifywhetherindividualswithrecurrenttonsillitis experiencedifferent post-tonsillectomypainintensitythanthosewithotherindicationsforsurgery,withnohistoryof episodesofacutetonsillitis.
Methods:Atotalof61tonsillectomieswereperformedundergeneralanesthesia,usinga potas-siumtitanylphosphate(KTP)laser(toeliminatethepotentialinfluenceonthestudyresultsof forcefuldissectionoffibrotictonsilsinpatientswithhistoryofrecurrenttonsillitis)and multi-pleligationsofbloodvesselswithinthetonsillarbeds.Thepatientsreceived37.5mgTramadoli hydrochloridum+325mgParacetamoltabletsfor10days.Postoperativevariablesincludedthe durationofhospitalstay,postoperativehemorrhageandreadmissionrate.Thepatientsreported painintensityonconsecutivedays,painduration,weightlossonpostoperativeday10, char-acter,intensityanddurationofswallowingdifficulties,andtheneedfor additionaldosesof painkillers. Healingwas alsoassessed.Capsularnervefibers werehistologicallyexaminedin theresectedtonsilsbyimmunostainingsforgeneralandsensorymarkers.
Results:Indicationsforthesurgerywere:recurrentacutetonsillitis(34patients),nohistoryof recurrenttonsillitis:focustonsil(20)andintensemalodour(7).Painintensityonpostoperative days 3---4andincidenceofreadmissionsdueto dehydrationwere significantlyhigher inthe
夽 Pleasecitethisarticleas:ZagólskiO,GajdaM,Str˛ekP,KozlowskiMJ,G˛adekA,NyzioJ.Adulttonsillectomy:postoperativepaindepends
onindications.BrazJOtorhinolaryngol.2016;82:589---95.
∗Correspondingauthor.
E-mail:[email protected](O.Zagólski).
http://dx.doi.org/10.1016/j.bjorl.2015.11.010
groupwithnohistoryofrecurrenttonsillitis.Nosignificantdifferencesinrelativedensitiesof proteingeneproduct(PGP)9.5-andcalcitoningene-relatedpeptide(CGRP)-immunoreactive nervefiberswereobserved.
Conclusion:Patientswithrecurrenttonsillitisqualifiedfortonsillectomyreportedlowerpain intensitythanthosewithoutrecurrenttonsillitisandthepainscoreswereunrelatedtonerve fibersdensity.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Tonsilaspalatinas; Tonsilectomia; Tonsilectomiaalaser; Tonsilite;
Dor;
Fibrasnervosas
Tonsilectomianoadulto:adorpós-operatóriadependedasindicac¸ões
Resumo
Introduc¸ão:Dorintensaéumadasqueixasmaisimportantesnopós-operatóriodeuma ton-silectomia.Comfrequência,essadorédescritapelospacientes,comocomparávelàdorque acompanhaatonsiliteaguda.Apesardatonsiliterecorrenteseraindicac¸ãomaisfrequentepara cirurgia,muitastonsilectomiassãorealizadasporoutrasindicac¸ões,eessespacientespodem nãoestarfamiliarizadoscomessador.
Objetivo:Verificarseindivíduoscomtonsiliterecorrenteapresentamdiferenc¸asnaintensidade dolorosapós-tonsilectomiavs.pacientescomoutrasindicac¸õesparacirurgia,semhistóricode episódiosdetonsiliteaguda.
Método: Foramrealizadas61tonsilectomiassobanestesiageral,comousodeumlaser potas-siumtitanylphosphate(KTP)(paraquefosseeliminadaumapossívelinfluênciadeumadissecc¸ão agressivadastonsilasfibrosadasempacientescomhistóriadetonsiliterecorrente),e hemosta-siaatravésdeligadurasdevasossanguíneosnosleitostonsilares.Ospacientesforammedicados com37,5mgdecloridratodetramadol+325mgdeparacetamol(comprimidos)durante10dias. Asvariáveispós-operatóriasforamtempodeinternac¸ãohospitalar,hemorragiaepercentualde readmissão. Ospacientesforneceraminformac¸ões sobreaintensidade dadorem dias con-secutivos,durac¸ãodador,perdadepesocorpóreonodia10dopós-operatório,intensidade edurac¸ãodadificuldadededeglutic¸ão,enecessidadededosesadicionais deanalgésicos.A velocidadedecicatrizac¸ãotambémfoiavaliada.Fibrasnervosascapsularesforamexaminadas histologicamentenastonsilasresecadascomousodeimunocorantesparamarcadoresdefibras nervosasgeraisedesensibilidade.
Resultados: Asindicac¸ões para a cirurgia foram: tonsiliteaguda recorrente(34 pacientes), ausência de históriade tonsilite recorrente--- Tonsilitefocal (20) e halitose(7). A intensi-dadedadornosdias3-4dopós-operatórioeaincidênciade reinternac¸ões em decorrência dedesidratac¸ãoforamsignificativamentemaisaltasnogruposemhistóriadetonsilite recor-rente.Nãoforamobservadasdiferenc¸assignificantesnasdensidadesrelativasdefibrasnervosas imunorreativasparaproteingeneproduct(PGP)9.5ecalcitoningene-relatedpeptide(CGRP). Conclusão:Ospacientescomtonsiliterecorrenteequalificadosparatonsilectomiainformaram menorintensidadedadoremrelac¸ãoaospacientessemhistóricosetonsiliterecorrente,eos escoresparadornãoapresentaramrelac¸ãocomadensidadedasfibrasnervosas.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Intense pain is one of the most important postoperative complaints after tonsillectomy, and in 20% of patients it becomes the reason for a hospital revisit, often due to subsequent dehydration.1---3 Pain intensity differs depending on the surgical technique2,4,5 and the type of pharmacological pain treatment.6,7 There are different patterns of postoperative pain after tonsillectomy; most frequently,painpresentsadecreasingcharacter,butsome patientsreportincreasing painscores duringthe firstfew
postoperative days.8 In some individuals, pain intensity decreasesaweekafterthesurgeryandinothersitpersists formorethantwoweeks.8Thereisalsoagroupofpatients suffering from a very high level of pain from the begin-ning, which decreases only gradually.8 Nevertheless, the majorityofadultpatientsundergoingtonsillectomycanbe appropriatelyadvisedpre-operativelyregardingthe proba-bledurationofpostoperativepainandthetimewhenthey canexpecttoresumeworkandnormalswallowing.9
accompanies an episode of acute tonsillitis. Most of the patients qualified for tonsillectomy had experienced such painnumeroustimesbeforethesurgery,sincechronic ton-sillitis, defined by American Academy of Otolaryngology --- Head and Neck Surgery criteria, as chronic tonsillithi-asis or recurrent acute tonsillitis (disabling sore throat episodesfiveormoretimesperyear,andsymptomsforat least a year),10 constitutes the chief indication for adult tonsillectomy.11Otherindicationsare:tonsillarhypertrophy andsuspectedneoplasm.12,13 However,anumberof tonsil-lectomies areperformed due tothe followingindications, often established by otorhinolaryngologists together with non-ENTphysicians:focus-tonsil,14 resultinginrheumatoid arthritis, psoriasis vulgaris, pustulosis palmaris and plan-taris,and/orsternocostoclavicularhyperostosis,14,15aswell as tonsillitis-induced immunoglobulin A nephropathy.16 In selected cases, intense malodour can also be the indica-tion for tonsil removal.17 These patients usually do not reportahistoryofrecurrenttonsillitisandmaybe unfamil-iarwithintensepharyngeal painbeforetheyarequalified fortonsillectomy.14,15,18
Inflammatory processes have been found to influence sensoryinnervationinvariousorgansandtissues.19---23 Exper-imentalstudieshave shownthatinflammation isgenerally accompanied by abnormalsproutingof peripheral sensory and autonomic nerve fibers and it significantly intensifies painsensation.20---22Onthecontrary,inflammationcanalso beassociated withatrophy, apoptosisandnecrosis of the sensorynervefibers,leadingtoneuropeptide-mediated neu-ropathyinsalivaryglands.19
Inthisstudywesetouttoverify:(1)whetherindividuals withrecurrenttonsillitisinanamnesisexperiencedifferent post-tonsillectomypainintensitythanthosewithother indi-cationsforsurgeryandnohistoryofrecurrenttonsillitis,and (2)todeterminewhetherdensitiesofcapsularnervefibers inresectedtonsilsdifferbetweenthesegroups.
Methods
Prior to examination, all the participants signed writ-ten informedconsent for their participationin the study. The research plan was approved by the institutional researchcommitteeandthelocalmedicalethicscommittee (75/KBL/OIL/2010).Thetenets oftheHelsinkideclaration werefollowed.
The study sample size was estimated with the use of a minimum expected difference of pain scores of 2, an estimated standard deviation of the variable of 1.5 with a resulting standardized differenceof 1.3, and a desired test powerof 0.8.Atotalof 61tonsillectomieswere per-formed during the period of January 2013---March 2014. There were 33 female and28 male patients, aged20---40 years (mean=29.0; SD=6.6). This study did not analyze patientsinwhomtonsillectomywasperformedduetoupper airwayobstructionsecondarytotonsillarhypertrophy,asall these procedures were combinedwith laser-assisted uvu-lopalatoplasty.General anesthesiainduction wasachieved with 1.0---2.0mg/kg fentanyl and 1.0---2.0mg/kg propofol 0.6---1.0mg/kg. Rocuronium was used as a muscle relax-antforendotrachealintubation.Anesthesiawasmaintained by sevoflurane in an O2/air 50% mixture and intermittent
positive pressure ventilation. Intravenous 5.0---10.0mg morphine and 50.0---100.0mg ketoprofen were used for analgesia.
Surgerywasperformedwithpotassiumtitanylphosphate laser(KTP/532AMSAuraXP---SanJose,CA,UnitedStates). Thelaserpowerwassetat15W.Multipleligations(Vicryl 4-0;Ethicon,Johnson&Johnson---NewBrunswick,NJ,United States)ofbloodvesselswithintonsillarbedswereapplied. Difficulttoaccesspartsofthepillars,adjacenttothetongue base, were cauterized withthe laser in order to prevent postoperativebleeding.Excisedtonsilsweresubmittedfor histologicalexamination.
Asingle dose of intravenoussteroids wasadministered at the time of surgery. Each patient received a single intravenous dose of 150.0g/kg (maximum dose 8.0mg)
dexamethasonesodium phosphate at the timeof surgery, aswellasthreesubsequentdailyoraldosesof37.5mg tra-madol+325.0mg paracetamol, and in addition four daily 500.0mgtablets ofparacetamolfor ten days.Further,up toone tablet of 50.0mg tramadoldaily wasallowed. No allergytothedrugswasreported.Alloperationswere car-riedoutbyasinglesurgeon.Aftersurgery,thepatientshad atminimumanovernighthospitalrecovery.
All the patients operated on during the study period were invited to participate in the prospective, observa-tional,questionnaire basedstudy, and they accepted the invitation.Theywerefollowed-upfor threeweeks.24 Data collected included patient variables such asage, gender, medicalhistory,andtheindicationforsurgery.Postoperative variablesstudiedincludeddurationofhospitalstay, postop-erativehemorrhageandreadmission rate,aswellasother complicationsoccurring during recovery fromsurgery. Re-admission was necessary when a patient could not drink enough fluids and required intravenous rehydration. The participantskeptadailylogtoassesspostoperative symp-toms and reported them by completing a questionnaire duringfollow-upvisitsonpostoperativedaysfour,ten,and 21.Theyansweredasetofquestionsconcerningpain inten-sityonconsecutivedays,painduration,bodyweightlosson anemptystomachnotedbeforetonsillectomyandon post-operativedayten(aftertheperiodofthemostaggravated swallowingdisorders),characterandintensityofswallowing difficultiesandtheirduration,aswellasadditionaldosesof analgesics.Postoperativemaximumpainonswallowingwas ratedonasubjectivescaleof1---5,with1indicating‘nopain’ and5‘severepain’.25 Swallowingdifficultieswereratedon ascale1---4: 1---mild swallowingdisorders,drinking unaf-fected;2 ---moderate difficultieseatingand drinking;3 ---markeddifficultieseatinganddrinking;4---serious difficul-tieseatinganddrinking.
Onpostoperativedaysfourandten,thepharynxofeach patientwasexaminedtoassessthehealingprocess,rated onafive-pointscale:4---rednessandedemaofvastregions ofpharyngeal mucosa, includingthe uvula;3 --- edema of theuvula withor without rednessand/or edemaof ante-riorpillarmucosa;2--- rednessandedemaof peritonsillar tissuesexcluding the uvula; 1 ---redness ofanterior pillar mucosawithoutedema;0---normalmucosa,withoutredness oredema.26
Inordertoverifywhetherthedifferencesinpain inten-sitybetween the groups couldresultfromchanges ofthe tonsil innervation caused by repeated acute and subse-quent chronic inflammation, histological examination of the densities of nerve fibers in the dissected tonsils was performed.
Both dissected tonsils were fixed overnight in 10% buffered formalin and then rinsed in phosphate buffered saline(PBS)andimmersedin25%sucrosesolution.Regions ofthetonsilscontainingthecapsulewerefurtherprocessed. Tissueblocksweremountedinoptimalcuttingtemperature (OCT) compound and snap-frozen. Ten-micrometer-thick cryosectionswerecut andthaw-mountedonpoly-l
-lysine-coatedslides.
Thesectionsweresubjectedtoindirect immunofluores-cence staining.27 Briefly, a pre-incubation step with 10% normal goat serum was applied for 40min. The sections were incubated overnight with primary rabbit antibod-ies raised for general nerve fiber marker --- protein gene product9.5(PGP9.5;AB1761,Chemicon---Temecula,CA, United States; 1:2000) and sensory marker --- calcitonin gene-related peptide (CGRP; AB5920,Chemicon; 1:4000). Subsequently, secondary incubations were applied using Cy3-conjugatedgoatanti-rabbitserum(111-165-144, Jack-sonIR---WestGrove,PA,UnitedStates;1:500)for2h.The sectionsweremountedwithVectashieldmedium(H-1000 ---Vector,Burlingame,CA,UnitedStates).
The sections were examined using an Olympus BX-50 (Olympus --- Tokyo, Japan) epifluorescence microscope equipped withappropriate filter set U-MNG for Cy3 visu-alization.Digital imageswereacquired by OlympusDP-71 camera.Relativedensities ofnervefibers indistinct loca-tionsweresemi-quantitativelyevaluatedintissuesections
bytwoindependentobservers. Arbitraryscoringfor nerve fiber densities wasdefined:0 ---no fibers,1 --- single,2 ---sparse,3---numerous.
Nohealthy(control)tonsilswereexamined,astheaim wastocomparepatientswithpotentiallydifferent postop-erativepainintensities.
Todeterminesignificantdifferencesbetweenthe distri-butionsoftheparticipants’age,painintensities,maximum painscores,meandayofreturntoanormaldiet,intensity ofswallowingdifficulties,bodyweight,andnumberof addi-tional dosesof analgesics,the Mann---WhitneyU rank sum testwasperformedwithStatisticaversion5software (Stat-soft, Inc.--- Tulsa, OK,United States). Contingencytables werecreatedandthechi-squaredtestwasusedtoconfirm differencesinrelativenervefiberdensities.Logistic regres-sionwasusedtocomparetheincidenceofreadmissiondue todehydrationinbothgroups.
Results
The indications for tonsillectomy allowed defining two groups of patients: (1) with a history of recurrent acute tonsillitis(34participants),and(2)withnohistoryof recur-renttonsillitis(27participants:focus-tonsil---20andintense malodor---7).
Theparticipants’ageandgenderdistributiondidnot dif-ferbetweenthegroups.Thelengthofhospitalstaydidnot differeither.Differencesinpainintensityonpostoperative daysone,two,andfiveto13werenon-significant(Table1). Painintensityondaysthreeandfourwassignificantlyhigher inthegroupwithnohistoryofacutetonsillitis.Differences in the following were non non-significant: pain duration,
Table1 Comparisonofmeanvalues(standarddeviations)ofthemeasuresobservedinthegroups.
Indicationsfortonsillectomy Recurrenttonsillitis Otherindications Statistics
Painintensityonpostoperativedays
1 2.8(0.9) 2.7(1.2) NS
2 3.4(0.9) 3.2(1.5) NS
3 2.7(0.7) 4.1(0.9) p<0.01
4 2.4(0.8) 4.0(0.9) p<0.01
5 2.6(0.6) 3.5(1.2) NS
6 2.7(1.1) 2.9(1.7) NS
7 2.0(0.6) 2.5(1.4) NS
8 1.6(0.7) 2.0(1.1) NS
9 1.3(0.8) 2.1(1.5) NS
Painduration(days) 12.4(2.6) 11.0(2.0) NS
Healing(0---4) 1.0(1.0) 1.2(1.1) NS
Intensityofswallowingdifficulties(1---4) 1.9(0.8) 2.2(1.1) NS
Dysphagiaduration(days) 11.7(1.8) 11.0(2.6) NS
Bodyweightloss(kg) 4.6(1.4) 5.4(3.4) NS
Bodyweightloss(%) 7.0(1.4) 6.5(3.9) NS
Additionaldosesofanalgesics 5.3(1.4) 4.6(2.8) NS
Table2 ComparisonofrelativedensitiesofPGP9.5-and CGRP-immunoreactivenervefibers.
PGP9.5 CGRP
Recurrenttonsillitis 2 0
Otherindications 2 1
Statistics NS NS
PGP 9.5, protein gene product 9.5; CGRP, calcitonin gene-relatedpeptide;NS,nostatisticalsignificance.
body weightloss on an empty stomach noted before and onthe10thdayafterthesurgery,characterandintensityof swallowingdifficultiesandtheirduration,aswellas addi-tionaldosesofanalgesics.Healingofthepharyngealmucosa alsodidnotdiffersignificantlybetweentheanalyzedgroups. Seriouspostoperativecomplicationsdidnotoccur.There wasnomajorpostoperativehemorrhageineithergroupthat required surgical attention. Hemorrhage was considered an early one if it occurred within the first 24 postopera-tive hours and late when bleeding occurred after 24h. Mild,spontaneouslysubsidinghemorrhageoccurredinfour patients, equally divided between the groups. All cases ofpostoperativehemorrhage occurredafter24h fromthe surgery.Fivepatientsinthegroupwithoutahistoryof recur-renttonsillitisvs.oneinthegroupwithahistoryofrecurrent tonsillitisrequiredreadmissionduetodehydration (signifi-cantdifference,withp<0.05).
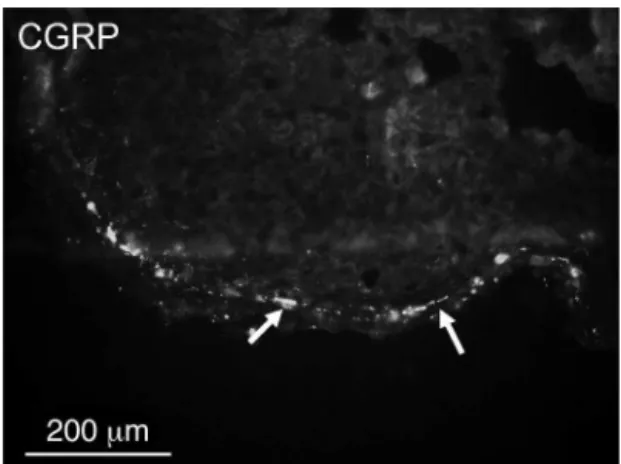
Overalldensitiesofnervefibersfoundinthetonsillar cap-suleswerelow.PGP9.5-immunoreactive fibersweremore numerousthanCGRP-positivefibers(Table2,Figs.1and2). CGRP fibers were found almost exclusively in thecapsule (Fig.2) while numerous PGP 9.5fibers (mostly relatedto blood vessels) wereverynumerous in thelymphoid tissue (Fig.3).Nosignificantdifferencesindensities ofPGP 9.5-aswellasCGRP-immunoreactivenervefiberswereobserved (Table2).
External validity of the findings was confirmed by the fact that all the patients gave consent to participation (there was noinfluence of potential differencesbetween thosewhogaveconsentandnon-consenters);theexamined groupsofpatientswerecoherentintermsofageandlack ofco-morbidities,andthattheyreflectedthedemographic
Figure 1 A few protein gene product (PGP) 9.5-immunoreactive nerve fibers (arrows) in the capsule of thetonsil.
Figure 2 Single calcitonin gene-related peptide (CGRP)-immunoreactive nerve fibers (arrows) in the capsule of the tonsil.
andsocioeconomiccharacteristicsofthegeneralpopulation treatedin a community-based hospital. Also,the surgical techniquewasthesameinalltheparticipants.
Discussion
The data from this study demonstrate that post-tonsillectomy pain intensity recorded after KTP laser tonsillectomy on postoperative days three and four in patientswithnohistoryof recurrenttonsillitiswas signif-icantly higher than in those in whom recurrent tonsillitis wastheindication for surgery. Also,the readmission rate duetodehydrationwashigherintheformergroup.Sofar, evidenceconcerningeffectsof indications for thesurgery onpost-tonsillectomypainhasnotbeenreported.
Logically,postoperativepaininpatientstonsillectomized duetorecurrenttonsillitisshouldbemoreintensethanin theothergroup, asdissection ofthetonsilsfromthe sur-roundingscarred tissues couldbe associated withgreater intra-operativetrauma.Therefore,whileplanningthestudy, itwasdecidedtouselaserinsteadofperformingcoldsteel surgery,inordertoeliminatepotentialinfluenceof force-fuldissectionofthetonsilsinthisgroupofpatientsonthe resultsofthestudy.Thus,itwaspossibletoeliminatefactors
relatingtothe surgical procedure itself fromtheanalysis ofpost-tonsillectomyoutcomes.Thisstudydidnotconfirm moreintensepainin thegroupof patientswithrecurrent tonsillitisinanamnesis,mostprobablybecauselaserenables easydissectionofthetonsilsfromtheirbeds.
Significant differences in reported pain intensity were observedonthedayswhenpost-tonsillectomypaininmost patients was most aggravated.8 In previous studies, pain scores after dissection tonsillectomy, as measured by a visual analog scale, differed significantly between every third consecutive day following postoperative day four.9 Two-thirdsofthepatientsrequiredanalgesicsafterthefirst postoperative day. About 80% of the individuals returned towork within14daysof surgeryandalmostall reported normal swallowing within 14 days of surgery,9 which is consistent with the authors’ observations relating to the laser-assistedtonsillectomy.However,thisstudydidnot con-firm the observation that post-tonsillectomypain, though initially slightly less after KTP laser than after standard coldsteeltonsillectomy,becameworseattwoweeksafter surgeryinpatientsoperated usingthelaser.28 The present results relating to wound healing and subsequent pain might be hard to compare with the results obtained in patients after tonsillectomy performed with the conven-tionalmethod,duetoslightlydelayedwoundhealingafter KTPlasersurgeryofthethroat.29
Sincenodifferenceswereestablishedbetweenthe exam-ined groups on histological examination, the observation thatpainexperiencedbypatientswithnohistoryof recur-rent tonsillitis was significantly more intense could be explainedby the fact that the patients with a history of recurrentacutetonsillitisweremorefamiliarwiththiskind ofpharyngealpain,andthereforetolerateditbetter.
Densities and distribution of nerve fibers within the tonsillar capsule and lymphatic tissue differed between individualsandanatomicalregionsofthetonsil,andthe dis-tributionwasdependent onthe tissueintersection plane. Hence,considerabledifferencesindensitiesofnervefibers were found locally in various examined tonsils. However, the observed overall differences were statistically non-significant.
The strengths of this study include direct comparison of statistically significant groups of participants operated forthesamesymptomsusingthesametechniqueandwith long-termfollow-up.Weaknessesincludethefactthatthere couldbeotherfactorsdeterminingdifferencesin postopera-tivepainperception,notaccountedforinthecurrentstudy. Determiningthesefactorswould fosterfutureresearchin thisfield.Inaddition,thescalesusedfor swallowing diffi-cultyandpostoperativewound healingwasnotvalidated, andthereforesubjecttobias.
Several important conclusions can be drawn from this study. The results obtained will assist in preop-erative counseling of patients undergoing tonsillectomy regardingpossible postoperativepainintensity and estab-lishingimprovedfollow-upprotocols.Basedontheobtained results, prior to surgery detailed medical history is col-lected from all candidates for tonsillectomy. If a patient hasno history of recurrent tonsillitis, she/heis informed aboutincreasedprobabilityofintensepostoperativepaina fewdaysaftertonsillectomy,andanalgesic dosage adjust-mentisadvocated.Thesepatientsarealsoadvisedtostay
in hospital longer,until their aggravatedswallowing diffi-cultiessubside, astheyareat riskof re-admission dueto dehydration.
Conclusion
Patients qualified for tonsillectomy due to recurrent ton-sillitis report lower pain intensity than those with other indicationsforthesurgery.Postoperativepainintensitywas unrelatedtonervefiberdensity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Bhattacharyya N, Kepnes LJ. Revisits and postopera-tive hemorrhage after adult tonsillectomy. Laryngoscope. 2014;124:1554---6.
2.Kamal SA, Basu S, Kapoor L, Kulandaivelu G, Talpalikar S, PapasthatisD.Harmonicscalpeltonsillectomy:a prospective study.EurArchOtorhinolaryngol.2006;263:449---54.
3.Valtonen H, Qvarnberg Y, Blomgren K. Patient contact with healthcare professionals after elective tonsillectomy. Acta Otolaryngol.2004;124:1086---9.
4.Ozkiris¸M,Kapusuz Z,Saydam L. Comparison of three tech-niques in adult tonsillectomy. Eur Arch Otorhinolaryngol. 2013;270:1143---7.
5.RagabSM.Sixyearsofevidence-basedadultdissection tonsil-lectomywithultrasonicscalpel,bipolarelectrocautery,bipolar radiofrequency or ‘cold steel’ dissection. J Laryngol Otol. 2012;126:1056---62.
6.StewartR,BillR,UllahR, McConaghyP,HallSJ. Dexametha-sonereducespainaftertonsillectomyinadults.ClinOtolaryngol AlliedSci.2002;27:321---6.
7.HillerA,SilvantoM,SavolainenS,TarkkilaP.Propacetamoland diclofenacaloneandincombinationforanalgesiaafterelective tonsillectomy.ActaAnaesthesiolScand.2004;48:1185---9. 8.Sarny S,Habermann W, Ossimitz G, StammbergerH.
Signifi-cantpost-tonsillectomypainisassociatedwithincreasedrisk ofhemorrhage.AnnOtolRhinolLaryngol.2012;121:776---81. 9.MurthyP,LaingMR.Dissectiontonsillectomy:patternof
post-operativepain,medicationandresumptionofnormalactivity. JLaryngolOtol.1998;112:41---4.
10.Silva S, Ouda M, Mathanakumara S, Ridyard E, Morar P. Tonsillectomyunder threat:auditingtheindications for per-formingtonsillectomy.JLaryngolOtol.2012;126:609---11. 11.Mattila PS, Tahkokallio O, Tarkkanen J, Pitkäniemi J,
Karvonen M, Tuomilehto J. Causes of tonsillar disease and frequencyoftonsillectomyoperations.ArchOtolaryngolHead NeckSurg.2001;127:37---44.
12.Hoddeson EK, Gourin CG. Adult tonsillectomy: current indications and outcomes. Otolaryngol Head Neck Surg. 2009;140:19---22.
13.PowellHR,MehtaN,DalyN,WattersGW.Improvedqualityof lifeinadultsundergoingtonsillectomyforrecurrenttonsillitis. Isadulttonsillectomyreallyalowprioritytreatment?EurArch Otorhinolaryngol.2012;269:2581---4.
14.Kataura A, Tsubota H. Clinical analyses of focus tonsil and related diseases in Japan. Acta Otolaryngol Suppl. 1996;523:161---4.
tonsilandsynoviuminapatientwithrheumatoidarthritisand chronictonsillitis.ArthritisRheum.2003;48:2483---8.
16.LiessBD,MytykC,CalhounKH,Whaley-ConnellAT. Tonsillec-tomyforthetreatmentoftonsillitis-inducedimmunoglobulinA nephropathy.AmJOtolaryngol.2010;31:485---8.
17.DelangheG,GhyselenJ,FeenstraL,vanSteenbergheD. Expe-riencesofaBelgianmultidisciplinarybreathodourclinic.Acta OtorhinolaryngolBelg.1997;51:43---8.
18.FujikawaS,HanawaY,ItoH,OhkuniM,TodomeY,OhkuniH. Streptococcalantibody:asanindicatoroftonsillectomy.Acta OtolaryngolSuppl.1988;454:286---91.
19.BatbayarB,NagyG,KövesiG,ZellesT, FehérE. Morphologi-calbasisofsensoryneuropathyandneuroimmunomodulationin minorsalivaryglandsofpatientswithSjögren’ssyndrome.Arch OralBiol.2004;49:529---38.
20.DicksonA,AvelinoA,CruzF,Ribeiro-da-SilvaA.Peptidergic sen-soryandparasympatheticfibersproutinginthemucosaofthe raturinarybladderina chronicmodelof cyclophosphamide-inducedcystitis.Neuroscience.2006;141:1633---47.
21.AlmarestaniL, Longo G, Ribeiro-da-Silva A. Autonomic fiber sprouting in the skin in chronic inflammation. Mol Pain. 2008;14:56.
22.ChakrabartyA, McCarson KE,SmithPG. Hypersensitivityand hyperinnervationoftherathindpaw following carrageenan-inducedinflammation.NeurosciLett.2011;495:67---71.
23.HukkanenM,KonttinenYT,ReesRG,GibsonSJ,SantavirtaS, PolakJM.Innervationofbonefrom healthyand arthriticrats bysubstancePandcalcitoningenerelatedpeptidecontaining sensoryfibers.JRheumatol.1992;19:1252---9.
24.Salonen A, Kokki H, Nuutinen J. Recovery after tonsillec-tomyinadults: athree-week follow-upstudy.Laryngoscope. 2002;112:94---8.
25.JonesDT,YoonMJ,LicameliG.Effectivenessofpostoperative follow-up telephone interviews for patients who underwent adenotonsillectomy: a retrospective study. Arch Otolaryngol HeadNeckSurg.2007;133:1091---5.
26.ZagólskiO,KulisiewiczJ.Perioperativeantibioticin adenoidec-tomy with partial tonsillectomy: a randomized trial. ORL J OtorhinolaryngolRelatSpec.2012;74:86---92.
27.Gajda M, Litwin JA, Tabarowski Z, Zagólski O, Cichocki T, TimmermansJP,etal.Developmentofautonomicinnervation inrattibia---colocalizationofvariousautonomicmarkerswith growth-associatedprotein43(GAP-43). CellsTissuesOrgans. 2010;191:489---99.
28.AufI,OsborneJE,SparkesC,KhalilH.IstheKTPlaser effec-tive in tonsillectomy? Clin Otolaryngol Allied Sci. 1997;22: 145---6.