www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Diagnosis
of
temporomandibular
joint
disorders:
indication
of
imaging
exams
夽
Luciano
Ambrosio
Ferreira
a,b,c,d,∗,
Eduardo
Grossmann
e,f,g,
Eduardo
Januzzi
h,
Marcos
Vinicius
Queiroz
de
Paula
i,j,
Antonio
Carlos
Pires
Carvalho
daUniversidadeFederaldeJuizdeFora(UFJF),JuizdeFora,MG,Brazil bFaculdadeSeteLagoas(FACSETE),SeteLagoas,MG,Brazil
cHospitalMaternidadeTherezinhadeJesus-HMTJ/JF,Suprema-FaculdadedeCiênciasMédicasedaSaúde,
JuizdeFora,MG,Brazil
dDepartmentofRadiology,FaculdadedeMedicina,UniversidadeFederaldoRiodeJaneiro(UFRJ),RiodeJaneiro,RJ,Brazil ePontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),PortoAlegre,RS,Brazil
fUniversidadeEstadualdeMaringá,Maringá,PR,Brazil
gDepartmentofMorphology,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
hPostgraduateCourseinTemporomandibularJointDysfunctionandOrofacialPain,FaculdadeSeteLagoas(FACSETE),Sete
Lagoas,MG,Brazil
iDisciplineofPropaedeuticandDentalRadiology,UniversidadeFederaldeJuizdeFora(UFJF),JuizdeFora,MG,Brazil
jPostgraduateCourseinDentalRadiologyandImagenology,UniversidadeFederaldeJuizdeFora(UFJF),JuizdeFora,MG,Brazil
Received23October2014;accepted16June2015 Availableonline8January2016
KEYWORDS
Temporomandibular jointdisorders; Diagnosticimaging; Temporomandibular joint;
Magneticresonance imaging;
X-raycomputed tomography; Radiography
Abstract
Introduction:Knowledge of thedifferent imaging tests andtheir appropriate indications is
crucialtoestablishthediagnosisoftemporomandibulardisorders,especiallyinpatientswith
overlappingsignsandsymptoms.
Objective: Topresent andassess the maindiagnostic imaging tests for temporomandibular
disordersandrationallydiscusstheirindicationcriteria,advantages,anddisadvantages.
Methods:LiteraturereviewintheWebofKnowledge,PubMedandSciELOdatabases,aswell
asmanualsearchforrelevantpublicationsinreferencelistsoftheselectedarticles.
Results:Computed tomography andmagnetic resonanceimaging were consideredthe gold
standardassessmentsforthetemporomandibularjointtoevaluatehardandsofttissues,
respec-tively.Eachdiagnosticmethod exhibiteddistinctsensitivityandspecificityforthe different
subtypesofjointdysfunction.
夽 Pleasecitethisarticleas:FerreiraLA, GrossmannE,JanuzziE,dePaulaMVQ,CarvalhoACP.Diagnosisoftemporomandibularjoint
disorders:indicationofimagingexams.BrazJOtorhinolaryngol.2016;82:341---52.
∗Correspondingauthor.
E-mail:[email protected](L.A.Ferreira).
http://dx.doi.org/10.1016/j.bjorl.2015.06.010
PALAVRAS-CHAVE
Transtornosda articulac¸ão
temporomandibular; Diagnósticopor imagem; Articulac¸ão
temporomandibular; Imagempor
ressonância magnética; Tomografia
computadorizadapor raiosX;
Radiografia
Diagnósticodasdisfunc¸õesdaarticulac¸ãotemporomandibular:indicac¸ãodosexames porimagem
Resumo
Introduc¸ão:Oconhecimentodosdistintosexamesdeimagemesuacorretaindicac¸ãoé
funda-mentalparaelaborac¸ãododiagnósticodasdisfunc¸õestemporomandibulares,principalmente
empacientescomgrandesobreposic¸ãodesinaisesintomas.
Objetivo:Apresentareavaliarosprincipaisexamesdediagnósticoporimagemdasdisfunc¸ões
temporomandibulares,alémdediscutirracionalmenteosseuscritériosdeindicac¸ão,vantagens
edesvantagens.
Método: RevisãodaliteraturanasbasesdedadosWebofKnowledge,PubMedeSciELO,além
debuscamanualporpublicac¸õesrelevantesnaslistasdereferênciasdosartigosselecionados.
Resultado:Os examesde tomografia computadorizada eressonância magnética foram
con-siderados ‘‘padrão-ouro’’ para aavaliac¸ão dos tecidosduros emoles, respectivamente,da
articulac¸ãotemporomandibular.Cadamétododediagnósticopesquisadoapresentou
sensibili-dadeeespecificidadedistintasparaosdiferentessubtiposdedisfunc¸ãodaarticulac¸ão.
Conclusão:Considera-se como racionalaindicac¸ão fundamentadanaacurácia, seguranc¸a e
relevância clínica do exame a ser solicitado, o que implicana adequada determinac¸ão do
diagnósticoedoplanodetratamento.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor
ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
The temporomandibular joint (TMJ) is a composite ginglymus-arthrodial joint, whose components are the condyle, glenoid cavity and articular tubercle, articu-lar disc, retrodiscal tissue, synovial membrane, and joint capsule.1Itisthemostfrequentlyusedjointofthehuman bodyandhassimultaneousbilateral capacitytomovethe mandible.2,3
Itscomponentsoftenundergoremodelingandadaptation processes.Inthepresenceoftemporomandibulardisorders (TMD), structural alterations and functional disorders are commonlyobserved.2,3
In most cases, symptoms are diffuse and imprecisely manifested asmasticatory myalgia, arthralgia, headache, otalgia,andneckpain,amongothers.4---8Paininmorethan oneareaiscommonandoftenleadspatientstoseek evalu-ationfromvariousmedicalanddentalspecialists,including otorhinolaryngologists.6,8
For instructional purposes, the American Academy of Orofacial Pain (AAOP) has classified TMD into two major groups: muscle and joint pain.9 It is estimated that temporomandibular joint disorders (TMJD) affect approx-imately 30% of the population in asymptomatic form, as internal joint derangement, comprising disc dislocation and structural changes resulting from osteoarthritis and osteoarthrosis.2,10,11 The diagnostic subtypesTMJD canbe seeninTable1.
TheetiologyofTMJDis notfullyunderstood6,8,12 andis relatedtothepresenceofriskfactorssuchastrauma, para-functionalhabits,posturalcondition,occlusalmicrotrauma, systemic predisposition, sleep disorders, and deleterious psychosocialalterations.6---8,11,13
The diagnosis of TMJD is achieved by evaluating the medicalhistoryandbyphysicalexamination.6,8,14However, diagnostic TMJ imaging methods are used to assess the integrityofitscomponentsandtheirfunctionalassociation, toconfirmtheextentorprogressionofanexistingdisease, andtoassessanddocumenttheeffectsofanalready estab-lished treatment.9,15 They areessential for assessment in casesoftrauma,occlusalalterationsandsuddenlimitation ofmouthopening, presenceofjointnoises,systemicjoint diseases,infectionandfailureofconservativetreatments.13
Objectives
This study discusses the main imaging techniques for the assessment ofTMJandadjacentstructuresandtheir indi-cations for the diagnosis of joint alterations, rationally evaluatingtheiradvantagesanddisadvantages.
Method
Table1 DiagnosticclassificationproposedbytheAAOP.12
Congenitalordevelopmentaldisorders Aplasia Hypoplasia Hyperplasia Dysplasia
Acquireddisorders Neoplasias
Disordersofdiscderangement Discdisplacementwithreduction Discdisplacementwithoutreduction TMJdisplacement(dislocation)
Inflammatorydisorders Synovitisandcapsulitis Polyarthritis
Non-Inflammatorydisorders Primaryosteoarthritis Secondaryosteoarthritis Ankylosis
Fracture(condylarprocess)
AAOP,AmericanAcademyofOrofacialPain.
in English or Portuguese, that contained the keywords ‘‘temporomandibularjointdisorder’’and‘‘diagnostic imag-ingtest.’’
Therewere51articlesfoundintheISIWebofKnowledge database,117inPubMed,and25inSciELO.Basicresearch
experimentalarticles,letterstotheeditor,andisolatedcase reportswereexcluded.Atotalof23articles,characterized as clinical trials, comparative studies, reviews, and case groupstudiescomprisedthefirststageoftheresearch.
Then,basedonthesameinclusioncriteria,aliterature searchwasperformedinthefivemostfrequentlycited radi-ologyjournalsfortheyears2004---2014. Inthissearch, six new references were found in addition to the previously selectedarticles.Fourotherrelevantpublicationscitedin theselectedarticles’listsofreferenceswereadded, includ-inghistoricalonesdatedpriorto2004.
According to the requirements defined in CNS Resolu-tion 196/96, this study was submitted to the Research EthicsCommittee,approvedunderNo.133/2009,designed todemonstrate themajorchangesintheTMJasdisclosed byimagingtests.
Temporomandibular
joint
imaging
assessment
Radiographicexaminations
TMJradiographsprovideinformationonthemorphological characteristicsof osseuscomponentsofthejointand cer-tainfunctionalassociationsbetweenthecondyle,articular tubercleandfossa,butareinefficientforevaluatingthesoft tissues.1,14,16
Severalanatomicalandtechnicalfactorscanpreventa clearandunobstructedradiographicimageoftheTMJ.16,17 When choosing TMJ radiography, one needs to consider the identification of boney structuraldetails, thespecific suspected clinical disorder, the amount of symptomatic informationclinicallyavailable for the diagnosis,the cost of these examinations, and their radiation dose.3,14 The radiographic techniques most often used in the routine managementofTMJDarepanoramicradiography, planigra-phy,andtranscranialradiography1,3,13,15(Fig.1).
Panoramicradiography
Asitprovidesamaxillaryoverview,itisusefulinthe differ-entialdiagnosisofodontogenicalterationswhosesymptoms overlapwithTMJD.13,18 Itcanrevealadvancedbone alter-ations in the condyle, such as asymmetries, erosions, osteophytes,fractures,changesin sizeandshape, degen-erative and inflammatory processes, growth alterations, maxillarytumors, metastases,and ankylosis.1,13,15,16 How-ever,itdoesnotprovidefunctionalinformationoncondylar excursion.14 Also, only gross alterations in the articular tubercle morphology can be seen because of the super-impositionof imagesof the skull base andthe zygomatic arch.3,14,16,18Thistechniqueisusefulasascreeningtool,asit allowstheinitialdiagnosisandassessmentofTMJalterations thatarenotsosubtle.15Itisalsoindicatedwhenthepatient hasreducedmouthopeningandthedifferentialdiagnosisof fractureisconsidered.1,3
Planigraphy(orpanoramicradiographywith programsforTMJ)
Thismethodprovidesconsiderable accuracy andproduces images without much overlap. It visualizes the articular boneydetail and reveals any anatomical abnormalities in structuresadjacenttotheTMJ,suchasthestyloidprocess, mastoidprocess,andzygomaticarch.3,15Itcanbeobtained inthe sagittal andcoronal planes,documenting the rela-tionshipofthecondylewiththearticularfossainmaximum habitual intercuspation(MHI)and the excursionextension duringmaximalmouthopening(MMO).Itprovidesadirect comparisonof both sidesregardingthe hypo-,normo-, or hyperexcursionofthecondyle,whichisusefulinconfirming aclinicalsuspicionofhypermobility.1,3
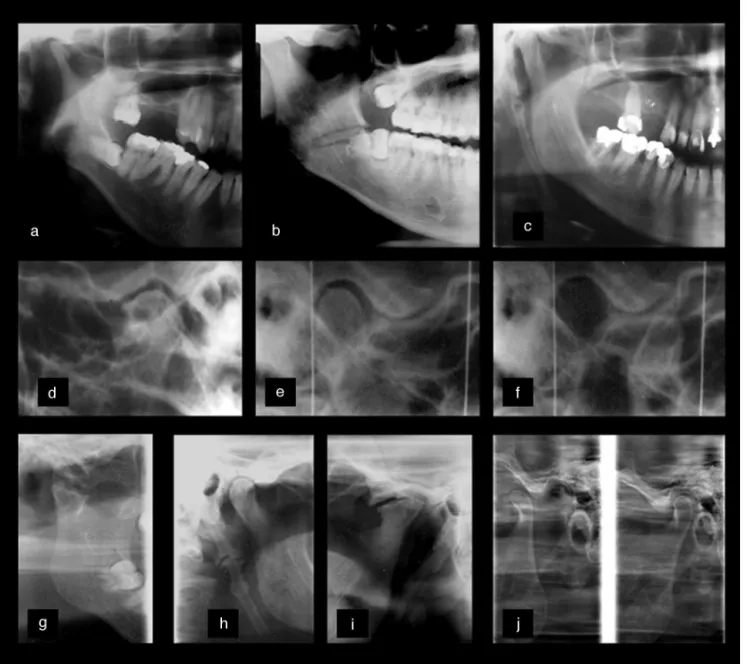
Figure1 RadiographicassessmentsofdifferentTMDs.(a---c)Close-upinpanoramicimageshowingmandibularcondylehypoplasia (a),horizontalimpactionofthethirdmolar(a,b)fracture lineintheregionofgonialangle(b)andelongatedstyloidprocess. Thetranscranialimages(d---f)showthepresenceofosteophytes(d),preservationofjointspacesinmaximumhabitual intercus-pation(MHI)(e)andtheidentificationofcondylarhyperexcursion(f).Theplanographytechniques(g---j)demonstrate:mandibular neckfractureandankylosis(g)elongatedstyloidprocess(h),advancedremodelingprocess,superior-anteriorflattening,cortical irregularities,andosteophyteformation(i)inadditiontomandibularheadhyperexcursion,definingTMJhypermobility(j).
Transcranialradiography
Similarlytotheplanigraphy,this evaluationprovidesgood anatomicalassessmentofthecondyle,fossa,andarticular tubercle.1,14,17Inthistechnique,anX-raybeamisobliquely directedthroughtheskulltothecontralateralTMJ, produc-ingasagittalview.17Thus,thecentralandmedialportions of the condyle areprojected inferiorly and only the lat-eraljointcontourisdisplayed.17Itisusefultoidentifybone alterationsanddisplacedfracturesoftheheadandneckof themandibularcondyle,aswellastoassessexcursionand todetermineradiographicjointspaces.3,14,17
This type of projection is limited by the fact that it producesanimagewithalargeoverlapoftheskullbones;it
alsorequirestheuseofaspecificcephalostatfor standard-ization,usuallyrequiringcomplexpositioning.1,13,14,17
Arthrography
Even though it is useful for disc position identifica-tion, arthrography is not currently recommended as it is an invasiveprocedure andcarriesarisk ofiatrogenicdisc perforationandfacialnervedamage.14 Therearealsothe risksofradiationtoradiosensitivestructures(crystallineand thyroid),painandlimitationofmovementafterthe injec-tions,infections,allergiestotheinjecteddye,anditisan examinationthatisconsidereddifficulttoperform.1,14,15,20
Othercombinedradiographictechniques
Due to the two-dimensional radiographic visualization of the TMJ, the combined use of different techniques is necessarytoprovidean accuratediagnosisandlocationof thealterations.Theevaluationofthestructuresindifferent planes illuminates fracture extension, degenerative joint disease, postoperative status, ankylosis, and neoplasms.3 Additionally,theanatomicrelationsofareasadjacenttothe lesioncanbestudiedwithgreaterdiagnosticaccuracy, pro-viding more efficient surgical and therapeutic planning.15 The main combined views are submental (or submento-vertex), transpharyngeal, transmaxillary, reverse Towne, posterior---anterior,andlateralteleradiography.3,13,15
Despitetheirlowercost,technicalsimplicity,andlower levelsofradiation,theuseofcombinedradiographicimages hasbecome lesscommondue toincreasing useand avail-ability of accurate images such as cone-beam computed tomography,whichassesshardtissuesinthethree anatom-icalplanesandarewidelyusedindentaldiagnosis.13,15
Computedtomography(CT)
CTcomprisesasetof imagesobtainedthrougha sophisti-cated and highly accurate technique, compared toplane radiographs.2 Recently, cone-beam computed tomography (CBCT) technologyhasbeenusedfor dentaldiagnosisdue toitsspecific usefor themaxillofacialregion.3,21 Itsmain advantage is the observation of boney joint structuresin the sagittal, coronal, and axial planes,1,21 in addition to the possible image manipulation at different depths and three-dimensionalreconstruction14,21throughspecific soft-ware.Theexaminationtimevariesbetween10and70s,and theradiation dose is muchlowercomparedtothehelical technique.3,21
The mainindications ofCBCTincludestructural assess-ment of bone components of the TMJ, which precisely determines the location and extent of boney alterations: fractures, neoplasms, and ankylosis; erosive degenera-tive,pseudocystic,andosteophyticalterations;presenceof asymptomaticboneremodeling;evaluationofpost-surgical conditions; hyperplasia of condylar, coronoid, and styloid processes;persistentforamenofHuschke;aswellas intraar-ticularcalcificationderivedfromsynovialchondromatosisor metabolicarthritis.2,14,15
Hard tissues, teeth, and bones are well demonstrated and measured in their real morphological condition, with minimalnoiseandartifacts.1,18,22 However,fewdetailsare providedonsofttissueanditisnotpossibletoevaluatethe jointdisc.3,22
Significantdisadvantagesarethecostoftheexamination andexposuretosignificantlevelsofradiationcomparedto conventionalradiographictechniques.1,14,15,18
Fig.2showsmorphologicalalterationsinjointbone com-ponentsdiagnosedbytheCBCTtechnique.
Magneticresonanceimaging(MRI)
MRIhas been the method of choiceto study disease pro-cesses involving the TMJ soft tissues,2,20,23 such as the articulardisc,ligaments, retrodiscaltissues,intracapsular synovialcontent,adjacentmasticatorymuscles,aswellas corticalandmedullaryintegrityofbonecomponents.1,3,15,22 The techniqueallowsthree-dimensionalanalysis inthe axial,coronal,andsagittalplanes.Itisconsideredthegold standardfor assessing disc positionand ishighly sensitive forintraarticulardegenerativealterations.3,20,23
Theclinical conditionsthatsuggest itsuseinclude per-sistentsymptomsofjointorpre-auricularpain,presenceof clickingandcrepitationnoises,functionalalterationssuch aslateral projections of the condyleduring mouth open-ing,frequent subluxationsanddislocations,limitedmouth openingmovementwithterminalstiffness,suspected neo-plasticprocesses,andpresenceofosteoarthriticsymptoms orasymptomaticosteoarthrosis.1,2,13,15
Thisdiagnostictestprotocolsusuallyincludethe recor-dinginthe MHIandMMOposition,usingweightedT1,T2, andprotondensity(PD),inthesagittalandcoronalplanes.15 WithT1-weightedimages,itispossibletoobtainexcellent anatomicdetail;protondensityresultsinsatisfactoryspatial resolutionofjointdiscinjuries,andisanexcellentchoicefor theevaluationofmedialandlateral discdisplacements.20 T2-weightedimages recordthe presence ofjoint effusion andmedullaryboneedema.2,3,20
Themainadvantagesincludedetectingsofttissue alter-ations,necrosis, edema, presenceor absenceof invasion, andlackofexposuretoionizingradiation.2,3,15,16,20
MRI is also indicated for the assessment of the integrity and anatomical relation of neural structures, which, when compressed by tumor or vascular pro-cesses, can produce orofacial pain by demyelination and deafferentation.2,3,13,14,16
Itsdisadvantages arerelated tothe high costand the need for sophisticated facilities. It is contraindicated in claustrophobicpatients,thosewithpacemakersand metal-licheartvalves,ferromagneticforeignbodies,andpregnant women.14,15,23
Fig.3illustratesmorphologicaljointdiscandbone struc-turesalterationsdiagnosedbyMRI.
Other
imaging
techniques
Ultrasonography(US)
a
f
i
R
g
h
b
c
d
e
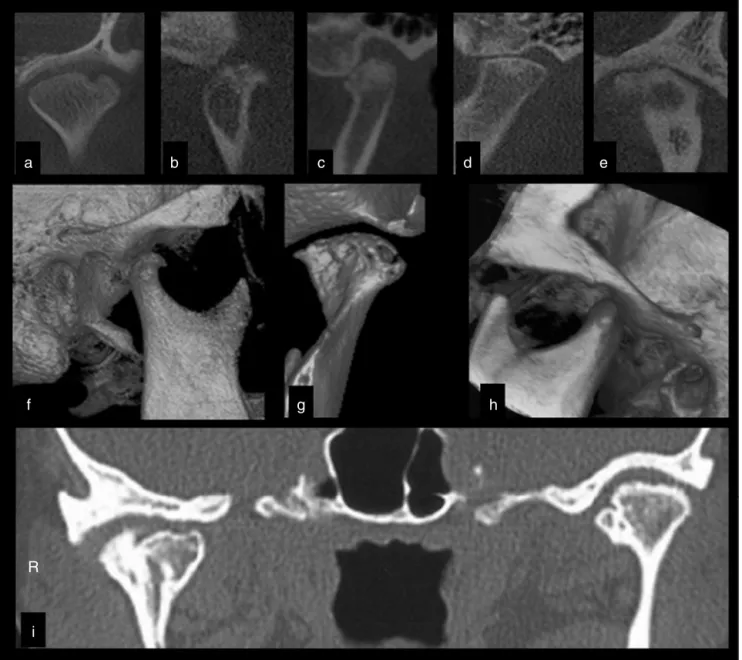
Figure2 Cone-beamcomputedtomography(CBCT) assessmentofdifferentTMJsinthecoronal(a, e)andparasagittal(b---d) views.(a)Coronalviewshowing extensiveerosion.Notethepresenceofbonesclerosis, corticalirregularities,andosteophytic formationin(b),(c), and(e).The presenceofsubchondralcystscan beobservedin(c)and(e). Advancedflatteningofbone componentsanddecreasedjointspacearerecordedin(d).Advanceddegenerativeosteoarthritisalterationisobservedine. Three-dimensionalreconstructions(f---h)showosteophytes(f,g),advancederosion(g)andhyperexcursionofthemandibularcondyle(h). (i)ThecoronalviewoftherightandleftTMJshowsalterationofthemandibularcondyleandhyperdenseimagesinthejointspaces compatiblewithsynovialchondromatosis.
Even with limitations, it can become a useful option for the initial study of the internal dysfunctions of the TMJ,15,23 particularlyin patients withcontraindications to MRI.14Moreover,itislessexpensive,allowsreal-time visu-alizationwithouttheuseofionizingradiation,andisquick andcomfortable.4,23,24
USassessmentiscommonlyusedinthedifferential diag-nosisofglandularandadjacentstructuresalterations,such astheTMJandthemassetermuscle.Thesymptomspresent in cases of sialadenitis and sialolithiasis can be mistaken forEaglesyndrome,TMD,myofascialpain,nervepain,and otherorofacialpainconditions.
Another indication of the US assessment is the cor-rect location of joint spaces for infiltrative therapies,
arthrocentesis, andviscosupplementation (Fig.4a andb). Itshows,dynamicallyandinrealtime,thelocationofjoint components, providing adequate lubrication and washing, which are verified by the increase in joint space after treatment.25
Nuclearmedicineevaluation
Nuclear medicine facilitates establishing a diagno-sis by detecting minute concentrations of radioactive pharmacologicalsubstancesthatdetermineosteometabolic alterationsexpressedinimagingexams.26
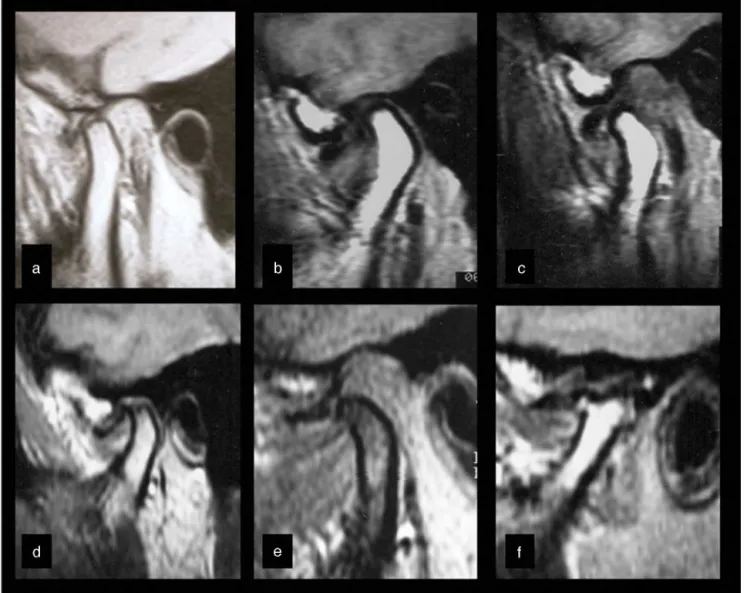
Figure3 DifferentMRIassessmentsdisclosingpreviousjointdiscdisplacement,withnoreductionintheparasagittalviews.One canobservecompressivedeformationofthejointdiscin(a),alsoduringdynamiccomparisonofthemandibularcondylarmovement in(b)and(c).Osteophyticformations(d---f),subchondralcyst(d),andseverechangeinform(f)definethediagnosisofosteoarthritis degenerativealterationsinbonecomponents.ThepresenceofhyperintenseT2-weightedimagesdefinesthediagnosisofeffusion in(b---f).
to evaluate synovitis and osteoarthritis.18 It is an exami-nationwithconsiderable sensitivity,low invasiveness,and highorganspecificity,withlowlevelsofradiation.27 Ithas someadvantagesover radiographies,conventionalCT,and MRIbecauseitprovidesanestimateofmetabolicand inflam-matoryactivity.26,27Itcanfacilitateanearlydiagnosisandis lesscostlythanCTandMRI.However,itdoesnot differen-tiateamongbone scardisorders,infections,osteoarthritic manifestations,ortumors.15
Positron-emissiontomography(PET) isusuallyindicated for the assessment and staging of metastatic tumors. It isabletoprovideaccuratefunctional,morphological,and metabolic information.28 Three-dimensional images facili-tate anatomicalvisualization andcan significantly reduce the time required for diagnosis, in addition to prop-erly direct treatmentsby ensuring that the therapies are appropriate.15
Currently,singlephotonemissioncomputedtomography with technetium-99m methylene diphosphate (SPECT/CT
with 99m Tc-MDP) is largely employed.26 This technol-ogy allows for multiplane image acquisition and 3-D display. The radiotracer 99m Tc is able to reflect the localosteometabolicrate,while the anatomicmapping is obtainedbytomographictechnique.26AsinthePET, anatom-ical and functional data are fused into a single image28 (Fig. 4c and d). Its main advantage is its sensitivity and specificity.26,28
Nuclearmedicine examinationsdiffer bythe radiotrac-ers/radioisotopesused,imagecapturetechnique,radiation dose,sensitivity,andpresentationofresults.15
Imaging
test
indication
criteria
in
the
diagnosis
of
temporomandibular
joint
disorders
Joint disc
a
c
d
b
Condyle
Figure4 Other imagingtechniques.(a)UltrasoundexaminationoftheTMJ25 usedduringthearthrocentesisassessment.Note
thearthrocentesisneedleasahyperechoicpoint(whitearrow).(b)UltrasoundexaminationoftheTMJshowingthejointdiscand condyle.(c)Tomographicaxialview28showingmassofsofttissuegrowthintheleftTMJregionextendingtotheipsilateralpterygoid
region.Infra-temporalspacewithabsenceofcondylarprocess,thepresenceofhyperdenseareas,swelling,andasymmetry.(d) PET/CTassessmentinaxialview28 showinghighmetabolicactivityintheleftTMJregion.Imagesreproducedwithpermissionof
theauthors’copyrights25,28byElsevier.
part of the professionals regarding the indications of the applicabletests.29
The correct indication of an imaging study should be based on the patient’s need for legal documentation, his/her individual complaints, and the identified clinical signsandsymptomsobtainedduringhistory-takingand phys-icalexamination.15,29,30Thebasicprinciplethatshouldguide theprofessionalisthatsupplementary testsareonly indi-catedwhentheclinicalassessmentisnotsufficienttoarrive atadiagnosisanddeviseatreatmentplan.21
ForTMJD,thephysicalexaminationsofpalpation, mea-surementof movement, functional testing andevaluation
ofjointnoisesareinstrumentsofgreatdiagnosticvalidity whenperformedbytrainedandexperiencedprofessionals.6 However,theoverlappingofmuscleandjointsymptomscan impairdiagnostic accuracy,asboth conditionsshow func-tionalimpairment.Inthiscaseandincasesofnon-specific symptoms(from,forexample,inflammation,neoplasia,and trauma), complementary imaging tests are essential for diagnostic clarificationanddelineation of theappropriate therapy.2,6
of
TMD:
indication
of
imaging
exams
349
Table2 IndicationofimagingteststodiagnosejointTMDandalterationsinstructuresadjacenttothestomatognathicsystem.
Disorders Assessedsign Panoramic1,3,13,14,16,18,29 Transcranial1,3,13,14,16---18,29 Planigraphy1,3,13,14,16,18,29 Arthrography1,3,13,14,16---18,20,29 Congenitalanddevelopmental
Aplasia Absenceofstructure b c c a
Hypoplasia Dimensionalreduction b c c a
Hyperplasia Dimensionalincrease b c c a
Dysplasia Structuralalteration b c c a
Acquired
Neoplasias Boneformation/destruction b c c a
Softtissuegrowth --- --- ---
---Metastasis a a a
---Discderangement
Withreduction RecaptureinMMO --- --- --- c
Withoutreduction NorecaptureinMMO --- --- --- c
TMJdisplacement Openlocking,clinical diagnosis
a c c a
Inflammatorydisorders
Synovitis/capsulitis Effusion,inflammation, capsularedema
--- --- ---
---Polyarthritis Polyarticular,cortical alteration,remodeling
b b b a
Non-inflammatory disorders/primaryor secondaryosteoarthritis
Uni-/bilateral,cortical alteration,remodeling
b b b a
Ankylosis Boneformation,impaired excursion
c c c b
Fracture(condylarprocess) Asymmetry,fractureline c b c b
Odontogenicconditions Cists,tumors,periapical disease
c --- ---
---Ofthestyloidprocess Elongationcalcification c --- c
---Ofthemajorsalivaryglands Sialolithiasis,inflammation a --- ---
---Ofthecondylarexcursion (hypo/hyper)
Condylarxmandibular tubercleratioinMMO
--- c c b
Ofthejointdiscform TMJdiscformalterationand perforation
--- --- --- d
Oftheadjacentbone structures
Alterationsincoronoidand mastoidprocesses
c --- c
---Ofadjacentsofttissues Alterationsintheligaments, retrodiscalarea,masticatory muscles
---Ferreira
LA
et
al.
Hyperplasia Dimensionalincrease d c a a
Dysplasia Structuralalteration d c a a
Acquired
Neoplasias Boneformation/destruction d d a d
Softtissuegrowth a d c d
Metastasis c c a d
Discderangement
Withreduction RecaptureinMMO --- d c
---Withoutreduction NorecaptureinMMO --- d c
---TMJdisplacement Openlocking,clinical diagnosis
d c a
---Inflammatorydisorders
Synovitis/capsulitis Effusion,inflammation, capsularedema
--- d c a
Polyarthritis Polyarticular,cortical alteration,remodeling
d c --- a
Non-inflammatory disorders/primaryor secondaryosteoarthritis
Uni-/bilateral,cortical alteration,remodeling
d c --- a
Ankylosis Boneformation,impaired excursion
d c ---
---Fracture(condylarprocess) Asymmetry,fractureline d c ---
---Odontogenicconditions Cists,tumors,periapical disease
d a a c
Ofthestyloidprocess Elongationcalcification d b ---
---Ofthemajorsalivaryglands Sialolithiasis,inflammation b d d
---Ofthecondylarexcursion (hypo/hyper)
Condylarxmandibular tubercleratioinMMO
d c ---
---Ofthejointdiscform TMJdiscformalterationand perforation
--- c ---
---Oftheadjacentbone structures
Alterationsincoronoidand mastoidprocesses
d b --- b
Ofadjacentsofttissues Alterationsintheligaments, retrodiscalarea,masticatory muscles
--- d c a
a Occasionalfinding,notthediagnosticpurposeoftheexamination.Othertestsarerequiredtoconfirm. b Frequentlydiagnosedcondition,butrequiresothermoreaccuratetests.
c Accuratediagnosisisestablished.
d Goldstandarddiagnosticevaluation,measurement,staging,location,andtreatmentplanning.
In general, MRI and CTare methods withhigher accu-racywhencomparedtoconventionalradiology,duetothe higheranatomicalresolutiontheyprovide.CTisconsidered the gold standard for the assessment of boney structures andthemethodofchoiceforfacialtrauma,whereasMRIis similarlyregardedforthestudyofsofttissues.1,2,16,23,29The twomethodsoftencomplementeachotherinthestudyof TMJalterations,constitutingimportanttoolsformuscleand jointdifferentialdiagnosis.4 Although abletodiagnose all bonealterationsoftheTMJ,MRIisconsideredlimitedwhen comparedtothehighaccuracyofCTforhardtissue.19,22
However, low-technical-complexity tests may possess high diagnostic accuracy,18 asin the case of radiographic records of condylar hyperexcursion in patients with the clinical presentation of terminal joint clicking. These characteristics suggest a diagnosis of joint hypermobility, verifiedbyasimpletranscranialor planigraphyimage.3 In thisexample,theimagehasgreatsensitivity,whileclinical dataconferspecificity,rulingoutotherdiagnostic possibili-ties.
Similarly,morphologicalalterationsofthestyloid, coro-noid, and condylar processes can be evaluated with high diagnostic accuracy through low-cost and easy-to-performradiographicexaminations,suchasplanigraphyand panoramicX-rays,29eventhoughtheCTisthegoldstandard forassessmentofthesealterations.2
Thedecisioninchoosingtheexaminationmustconsider itsinfluenceontheproposeddiagnosisandtherapy.Ifthe clinical indicationis a conservativetherapy that can con-trol symptoms in the short term, image requests can be considered.1,15 Moreover, when conservative therapy has failedandaninvasivetherapyisindicated,highlysensitive diagnostictests,suchasCTandMRIareselected.15,31
Elaborate treatment plans also require complete and accurate images,29,31 for example, suspected fractures, where the CT, in addition to establishing the diagnosis, illustrates theexact locationand size,andallows for the selectionoftheappropriatesurgicaltherapy.2
Similarreasoningisusedfortheassessmentof neoplas-tic conditions. A study32 that compared the accuracy of imaging tests for bone tumor detection showed that the nuclear medicine diagnostic tests had greater sensitivity andspecificitythanCTscans,MRI,andradiographic assess-ment, although thelatter areuseful in the initialclinical investigations.26,28,29,32
Especially for non-surgical jointconditions,one should consider the risk of injuries and the safety of diagnostic techniques.15 Althougharthrographycaneffectively deter-mine disc position and perforation,33 it is considered an invasiveand potentially hazardousmethod.Thus,MRI has becomethemethodofchoiceforsuchconditions.1
Similarly, recent studies4,5,23---25,30 have recommended US as a safe, noninvasive diagnostic technique with con-siderable accuracy for joint disc positioning, especially for patients with contraindication toMRI or submitted to real-time interventions, suchas arthrocentesis and visco-supplementation.Inthesetechniques, theUSexamination isespeciallyappropriatefortheidentificationoftheinferior jointspace.Itspreciseidentificationandcorrectaccessare factorsthatcontributetothetechnique’ssuccess.11
Long-termrisksandtissuedamageshouldalsobe consid-eredforradiationexposure.Asinconventionalradiographs,
CTshouldonly cautiouslybechosen becauseofitshigher radiationabsorption,15,29although CBCThasshorter radia-tionexposuretimewhencomparedtohelicalCT.21
Eveniftheyposesomerisk,teststhatusehigherdoses ofradiationareneededfordiseasestagingandareessential for defining the treatment plan. Nuclear medicine exam-inations, for instance, are indicated to assess metabolic alterations of growth and assessment of metastases.26---28 However, they still require confirmation of the type of growththroughspecific tests,suchashistopathological or immunohistochemicalanalysis.15
Table 2 lists and classifies information that can be obtained by several examination techniques through TMJ images, based on their indications, risks, and diagnostic power.
Conclusion
Individually,theseveralimagingtestshavespecific indica-tionsforthediagnosisofTMJD.
Despitetheir lowersensitivity, radiographic techniques havelowercostandemploylowerradiationdoses.Theyare indicatedfortheearlyassessmentoflesscomplexsymptoms andthedifferentialdiagnosis betweenTMDand inflamma-torydental-maxillofacialconditions.
Morphological, degenerative bone abnormalities, and fracturesarepreciselydiagnosed,identified,andmeasured by CT. Mainly,CBCT has a lower radiation dose and arti-factreduction,andisconsideredthegoldstandardforthe assessmentofmaxillofacialhardtissues.Inflammatory alter-ations,jointdisc position,andother softtissuestructures areclearlyidentifiedandevaluatedbyMRI,thatissaferthan arthrography.
US examination accurately identifies the joint disc, mainly when the MRI assessment is contraindicated. It is indicated for the differential diagnosis between TMDand painfulconditionsofmajorsalivaryglands,aswellas pre-andpost-evaluationofinfiltrationtherapies,suchas visco-supplementationandarthrocentesis.
Nuclearmedicineassessmentsareprimarilyindicatedfor theassessmentofmetabolicandgrowthalterations,suchas tumorsandmetastases.
Arthrographyisaninvasive intra-articularexamination; itsusualindication is thevisualization of jointdisc alter-ations.Duetotheriskinherenttothetechnique,ithasbeen replacedbyMRIassessment.
Factors thatneed to beevaluatedfor the selection of TMJimagingtestsincludethefollowing:theneedto deter-mine the presence of the disease and its prognosis, the qualityandquantityofavailableclinicalinformation; uncer-taintyinthedifferentialdiagnosis;determiningthestageof diseasedevelopment;needforlegaldocumentation; preop-erativepreparation;evaluationoftreatmentevolution;and thesafetyandaccuracyoftheproposedexamination.
Conflicts
of
interest
néticaetomografiacomputadorizadadaarticulac¸ão temporo-mandibular:alémdadisfunc¸ão.RadiolBras.2008;41:337---42.
3.Ferraz Júnior AML, Guimarães JP, Ferreira LA. Técnicas de obtenc¸ão de imagens da articulac¸ão temporomandibular.In: GuimarãesJP, FerreiraLA, editors.Atlas de diagnóstico por imaginologiadasdesordenstemporomandibulares.JuizdeFora: EditoraUFJF;2012.p.28---66.
4.Landes CA, Goral WA, Sader R, MackM. 3Dsonography for diagnosis of discdislocation ofthetemporomandibular joint comparedwithMRI.UltrasoundMedBiol.2006;32:633---9.
5.C¸akir-Özkan N, Sarikaya B, Erkorkmaz U, Aktürk Y. Ultra-sonographicevaluationofdiscdisplacementofthe temporo-mandibularjointcomparedwithmagneticresonanceimaging. JOralMaxillofacSurg.2010;68:1075---80.
6.CunhaSC,NogueiraRVB,DuarteAP,VasconcelosBCE,Almeida RAC. Análise dos índices de Helkimo e craniomandibu-lar para diagnóstico de desordens temporomandibulares em pacientes com artrite reumatoide. Braz J Otorhinolaryngol. 2007;73:19---26.
7.Ferreira LA, Oliveira RG, GuimarãesJP, Carvalho ACP, Paula MVQ.Laser acupunctureinpatientswithtemporomandibular dysfunction: a randomized controlled trial. Lasers Med Sci. 2013;28:1549---58.
8.SilveiraAM,FeltrinPP,ZanettiRV,MautoniMC.Prevalênciade portadoresdeDTMempacientesavaliadosnosetorde otorri-nolaringologia.BrazJOtorhinolaryngol.2007;73:528---32.
9.LeeuwR.Disfunc¸ãotemporomandibular.In:LeeuwR,editor. Dororofacial.SãoPaulo:Quintessence;2010.p.129---204.
10.Fujiwara M, Honda K, Hasegawa Y, Hasegawa M, Urade M. Comparisonofjointpaininpatientsdiagnosedwithand with-out articular disc displacement without reduction based on the ResearchDiagnostic Criteriafor Temporomandibular Dis-orders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2013;116:9---15.
11.Grossmann E,JanuzziE,IwakiFilhoL. O usodohialuronato de sódionotratamentodasdisfunc¸õestemporomandibulares articulares.RevDor.2013;14:301---6.
12.Güler N, Uc¸kan S, Imirzalıo˘glu P, Ac¸ikgözo˘glu S. Temporo-mandibularjoint internalderangement:relationshipbetween joint pain and MR grading of effusion and total protein concentration in the joint fluid. Dentomaxillofac Radiol. 2005;34:175---81.
13.Hunter A, Kalathingal S. Diagnostic imaging for temporo-mandibulardisordersand orofacialpain.DentClinNorthAm. 2013;57:405---18.
14.VasconcelosBCE,SilvaEDO,KelnerN,MirandaKS,SilvaAFC. Meiosdediagnósticodasdesordenstemporomandibulares.Rev CirTraumatBuco-Maxilo-Facial.2002;1:49---57.
15.LewisEL,DolwickMF,AbramowiczS,ReederSL.Contemporary imagingofthetemporomandibularjoint.DentClinNorthAm. 2008;52:875---90.
16.Cozzolino FA, RapoportA, FranziSA, SouzaRP,Pereira CAB, Dedivitis RA. Correlac¸ão entre os achados clínicos e imagi-nológicos nas disfunc¸ões temporomandibulares. Radiol Bras. 2008;41:13---7.
17.Almeida SM, Bóscolo FN, Pereira TCR. Estudo comparativo entre duas técnicas radiográficas transcranianasutilizando o cefalostatoACCURAD-200,nasposic¸õespadrãoecorrigida,e
mandibular joint disorders. Part 1: bone marrow abnormal-ities of the mandibular condyle. Dentomaxillofac Radiol. 2000;29:7---10.
20.Ramos ACA, Sarmento VA, Campos PSF, Gonzalez MOD. Articulac¸ãotemporomandibular---aspectosnormaise desloca-mentosde disco:imagemporressonância magnética. Radiol Bras.2004;37:449---54.
21.RodriguesMGS,Alarcón OMV,CarraroE,RochaJF, Capelozza ALA.Tomografiacomputadorizadaporfeixecônico:formac¸ão daimagem,indicac¸ãoecritériosparaprescric¸ão.Odontol Clín-Cient.2010;9:115---8.
22.AlkhaderM,OhbayashiN,TetsumuraA,NakamuraS,OkochiK, MominMA,etal.Diagnosticperformanceofmagneticresonance imagingfordetecting osseousabnormalities ofthe temporo-mandibularjointanditscorrelationwithconebeamcomputed tomography.DentomaxillofacRadiol.2010;39:270---6.
23.JankS,Zangerl A,KlossF,LaimerK,MissmannM,Schroeder D,etal.Highresolutionultrasoundinvestigationofthe tem-poromandibularjointinpatientswithchronicpolyarthritis.Int JOralMaxillofacSurg.2011;40:45---9.
24.BasB,YilmazN,GökceE,AkanH,TurkeyS.Ultrasound assess-mentofincreasedcapsularwidthintemporomandibularjoint internalderangements:relationship withjointpainand mag-neticresonancegradingofjoint effusion.OralSurgOralMed OralPatholOralRadiolEndod.2011;112:112---7.
25.DayisoyluEH,CifciE,UckanS.Ultrasound-guided arthrocente-sisofthetemporomandibularjoint.BrJOralMaxillofacSurg. 2013;51:667---8.
26.CoutinhoA, Fenyo-Pereira M, Dib LL, LimaENP. Therole of SPECT/CTwith99mTc-MDPimagefusiontodiagnose
temporo-mandibulardysfunction. OralSurgOralMedOralPatholOral RadiolEndod.2006;101:224---30.
27.Bittencourt LP, SouzaSAL, Magnanini M, Fonseca LMB, Gut-filenB. Verificac¸ão da atividadecondilar em pacientes com padrão esquelético classe III por intermédio da cintilografia óssea.RadiolBras.2005;38:273---7.
28.ShintakuWH, VenturinJS,YepesJS.Applicationofadvanced imagingmodalitiesfor thediagnosis ofmetastatic adenocar-cinoma of the lungs in the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107: 37---41.
29.PharoahM.Theprescriptionofdiagnosticimagesfor temporo-mandibularjointdisorders.JOrofacPain.1999;13:251---4.
30.BasB,YilmazN,GökceE,AkanH.Diagnosticvalueof ultra-sonographyintemporomandibulardisorders.JOralMaxillofac Surg.2011;69:1304---10.
31.Calderon PDS, Reis KR, Araujo CDRP, Rubo JH, Conti PCR. RessonânciamagnéticanosdesarranjosinternosdaATM: sen-sibilidade eespecificidade. RevDent Press Ortodon Ortoped Facial.2008;13:34---9.
32.Shintaku WH, Venturin JS, Langlais RP, Clark GT. Imaging modalities to access bonytumors and hyperplasic reactions of the temporomandibular joint. J Oral Maxillofac Surg. 2010;68:1911---21.