w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Relationship
between
pulmonary
and
cardiac
abnormalities
in
sickle
cell
disease:
implications
for
the
management
of
patients
Maria
Christina
Paixão
Maioli,
Andrea
Ribeiro
Soares,
Ricardo
Bedirian,
Ursula
David
Alves,
Cirlene
de
Lima
Marinho,
Agnaldo
José
Lopes
∗UniversidadedoEstadodoRiodeJaneiro,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20September2015 Accepted7November2015 Availableonline11December2015
Keywords:
Sicklecelldisease Respiratoryfunctiontests Computedtomography Echocardiography
a
b
s
t
r
a
c
t
Objective:Toevaluatetheassociationbetweenclinical,pulmonary,andcardiovascular find-ingsinpatientswithsicklecelldiseaseand,secondarily,tocomparethesefindingsbetween sicklecellanemiapatientsandthosewithothersicklecelldiseases.
Methods:Fifty-nineadultswereincludedinthiscross-sectionalstudy;47hadsicklecell anemia,and12hadothersicklecelldiseases.Allpatientsunderwentpulmonaryfunction tests,chestcomputedtomography,andechocardiography.
Results:Abnormalitiesoncomputedtomography,echocardiography,andpulmonary func-tion tests wereobservedin93.5%, 75.0%;and 70.2%of patients,respectively.A higher frequency ofrestrictiveabnormalitieswasobservedinpatientswitha historyofacute chestsyndrome(85%vs.21.6%;p-value<0.0001)andamongpatientswithincreasedleft ventriclesize(48.2%vs.22.2%;p-value=0.036),andahigherfrequencyofreduced respi-ratorymusclestrengthwasobservedinpatientswitha ground-glasspattern(33.3%vs. 4.3%;p-value=0.016).Moreover,ahigherfrequencyofmosaicattenuationwasobservedin patientswithelevatedtricuspidregurgitationvelocity(61.1%vs.24%;p-value=0.014). Com-paredtopatientswithothersicklecelldiseases,sicklecellanemiapatientshadsuffered increasedfrequenciesofacutepainepisodes,andacutechest syndrome,andexhibited mosaicattenuationoncomputedtomography,andabnormalitiesonechocardiography.
Conclusion: Asignificantinterrelationbetweenabnormalitiesofthepulmonaryand cardio-vascularsystemswasobservedinsicklecelldiseasepatients.Furthermore,theseverityof thecardiopulmonaryparametersamongpatientswithsicklecellanemiawasgreaterthan thatofpatientswithothersicklecelldiseases.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:RuaAraguaia,1266,bloco1/405,Freguesia,Jacarepaguá,22745-271RiodeJaneiro,RJ,Brazil.
E-mailaddress:[email protected](A.J.Lopes).
http://dx.doi.org/10.1016/j.bjhh.2015.11.001
Introduction
Sicklecelldisease(SCD),themostcommonmonogenic hered-itaryconditioninBrazilandworldwide,itaffectsmorethan30 millionpeople.1Itisestimatedthat4%oftheBrazilian
popula-tionhasthesicklecelltraitandthatbetween25,000and50,000 individualshavethediseaseinthehomozygous(SS)or com-poundheterozygousstates(SC,SE,SD,andS-thalassemia).2
InBrazil,SCDisunevenlydistributedamongthepopulation, asitismoreprevalentintheBrazilianstateswiththegreatest numbersofindividualswhoaredescendantsofslaves.3
SCDischaracterizedbythepresenceofphenotypesthat range from almost no symptoms to severe symptoms. Its onset occurs during the first year of life, and the disease extendsthroughoutlife;itisassociatedwithhighmorbidity andmortality.4Thesymptomsareduetohemolyticanemia
and cause severely painful episodes; life-threatening com-plicationsduetobacterialsepsis,andsplenicsequestration, acutechestsyndrome(ACS),andchronicorgandamageare alsoobserved. All ofthese complications are due, at least inpart, tochronic hemolysis and episodes ofintermittent vascularocclusion,whichleadtotissueinjuryandorgan dys-function.AdvancesinthecareofSCDpatients haveledto increasedsurvival, which inturn hasled to the increased occurrenceofchronicdamage.5,6
ThelungisoneoftheorgansmostinvolvedinSCD.7Itis
estimatedthatapproximately90%ofadultswithSCD have abnormalpulmonaryfunction.8Chroniclungdiseaseislikely
associatedwithrecurrentepisodesofACScausedby infec-tions,fatembolism,andpulmonaryinfarction.1,5,9Pulmonary
hypertension(PH)isbelieved tobeamajorcause ofdeath inadultpatients,althoughmorerecently,its incidenceand pathophysiologyhavebeen extensivelydebated.10,11
Impor-tantly, only 10% of SCD patients are monitored for early detectionofPH.5Itspathophysiologicalmechanismis
com-plexandprobablymultifactorial.11,12
Cardiovascularcomplicationshavebeenincreasingly diag-nosedduetotheincreasedlongevityofSCDpatients,13who
haveenlargedheart chambers,analterationthatbegins in adolescence.11 Cardiomegaly, chesthyperactivity, andheart
murmursare oftenpresent,mostlysecondary toastateof chronicanemia,PH,andmicrocirculatoryobstructionrelated tohemoglobinopathies.11,14 Cardiac ironoverloadisa
pos-tulated but unproven mechanism in SCD patients.14 Heart
failure is uncommon, and its presence is associated with olderage,coexistenceofsystemichypertensionandkidney failure.14Littlehasbeenreportedintheliteratureaboutthe
impactofthehomozygousorheterozygousstateson hemo-dynamicchanges.11,15
DuetotheincreasedlifeexpectancyofSCDpatients,many morphologicalandfunctionalparametersassociatedwiththe respiratoryandcardiovascularsystemsneedtobeelucidated to allow these parameters to be incorporated into patient follow-up.Thehypothesisofthisresearchwasthatthereis arelationshipbetweenabnormalitiesoftherespiratoryand cardiovascular systems in adults with SCD. Therefore, the presentstudyaimedtoevaluatetheassociationbetween clin-ical,pulmonary,andcardiovascularfindingsinSCDpatients and,secondarily,tocomparethesefindingsbetweenpatients
withsicklecellanemia(SCA)andpatientswithothersickle celldiseases(OSCD).
Methods
Thiscross-sectionalstudywasconductedbetweenMay2013 and June2015 and evaluated patientswith SCD in regular follow-upsattheHospitalUniversitárioPedroErnesto(HUPE) oftheUniversidadedoEstadodoRiodeJaneiro(UERJ).Patients aged≥18yearswithSCAorOSCDwereincluded. Exclusion criteria were abloodtransfusion withinthe previousthree months, avaso-occlusive pain episodewithinthe previous month, reports of heart disease or lung disease unrelated toSCD, asmokinghistory of>10 pack-years,and ahistory of respiratory infection in the previous three weeks. Pack-yearswascalculatedbymultiplyingthenumberofpacksof cigarettessmoked perdaybythenumberofyearsthe per-son hadsmoked.16 Basedon thesecriteria,twelvepatients
were excludedforthefollowingreasons:significant history of smoking (n=5), blood transfusion in the previous three months(n=5),andvaso-occlusivepainepisodesinthe pre-viousmonth(n=2).
Amongthe59studyparticipants,forty-sevenhadSCA,and 12hadOSCD(10patientshadtheHemoglobin(Hb)SCform, and twopatientshadthe HbSD form).Nopatienthad the heterozygousSformofSCD.Thestudywasapprovedbythe ResearchEthicsCommitteeofHUPE-UERJ(number231.033), and all participantssignedaninformedconsentform.The studywasconductedinaccordancewiththeHelsinki Decla-rationasrevisedin2008.
Using a computerized system (Collins Plus Pulmonary Function Testing Systems, Warren E. Collins, Inc., Brain-tree,MA,USA),spirometry,whole-bodyplethysmography,and respiratorymusclestrength (RMS)wereevaluated. The pul-monary function tests (PFTs) followed the standards and interpretation established by the American Thoracic Soci-ety(ATS).17TheequationsofPereira(spirometry)andNeder
(whole-body plethysmography and measurement of RMS) wereusedtointerpretthefunctionalparameters.18–20
Restric-tive abnormalities were diagnosed when the total lung capacity (TLC)was belowthelower limitsofnormal(LLN), and obstructive abnormalities were diagnosed when the forcedexpiratoryvolumeinonesecond/forcedvitalcapacity (FEV1/FVC)ratiowasbelowtheLLN.17
findingswereevaluated:reticularpattern,ground-glass opaci-fication (GGO), mosaicattenuation, lobar volume loss, and tractionbronchiectasis.21,22 Thespleensizewasalso
evalu-atedinthisstudybyCT.
TransthoracicDopplerechocardiographywasperformedby thesameexaminerusinganiE33system(PhilipsMedical Sys-tems,MA,USA).Theimageswerestoredondigitalmediaand reviewedbyasecondexaminer;bothexaminerswereblinded tothe patientgroups.Tricuspidregurgitationvelocity(TRV) wasconsideredhighwhenthevaluewas≥2.5ms−1.23
Statisticalanalysis
TheShapiro–Wilktestwas usedtoevaluatesample homo-geneity. The results are expressed as median values and interquartile ranges or numbers (percentages). Inferential analysisincluded the chi-square test or Fisher’s exact test to compare the findings with categorical data and the Mann–Whitney test or Kruskal–Wallis ANOVA to compare findings with numericaldata. Dunn’s multiple comparison testwasappliedtoidentifysubpopulationsthatdiffered sig-nificantly.DatawereanalyzedusingSASsoftwareversion6.11 (SASInstitute,Inc.,Cary,NC,USA).p-Values<0.05were con-sideredstatisticallysignificant.
Results
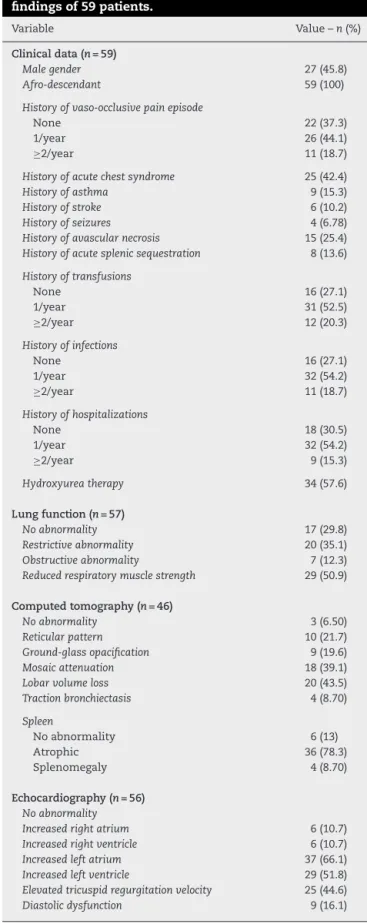
Thestudypopulation(n=59)included32womenand27men, withamedianageof27(range:22–39)years.ThemedianHb levelwas8.32(range:7.60–10)g/dL.AbnormalitiesonCTscans, echocardiography,and PFTs wereobservedin93.5%,75.0%, and70.2%ofthepatients,respectively.Theclinicalfeaturesas wellasthePFT,CT,andechocardiographyresultsareshown inTable1.
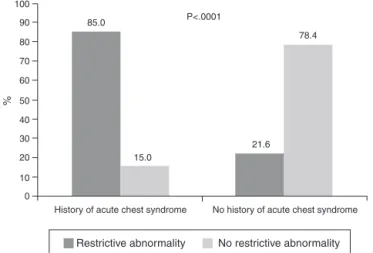
Acomparisonofpatientswithandwithoutabnormalities inthePFTs foundno significant differencesinclinical,CT, orechocardiographyfindings.However,ahigherfrequencyof restrictiveabnormalitieswasobservedinthePFTsofpatients withahistoryofacutechestsyndrome(Figure1).Ahigher frequencyofreducedRMSwasalsoobservedinthePFTsof patientswithaGGOpatternonCT(Figure2).
Acomparisonofpatientswithandwithoutabnormalities on CT scans found no significant differences in the clini-cal,PFT,orechocardiographyfindings.However,theHblevels weresignificantlydifferentbetweenpatientswithanormal spleen[8.90(range:7.40–10)g/dL],splenicatrophy[8.20(range: 7.70–9.70)g/dL],andsplenomegaly[10.9(range:10–12)g/dL]on CTscans(p-value=0.025).
Acomparisonofpatientswithandwithoutabnormalities onechocardiographyfoundasignificantdifferencebetween patients with and without a mosaic attenuation pattern observedonCTscans,aswellasahigherfrequencyofmosaic attenuationpatterninpatientswithabnormal echocardiog-raphy(50%vs.15.4%;p-value=0.033)andwithelevatedTRV (Figure 3). Moreover, lower serum Hb levels were observed in patients with abnormal echocardiography [(8.13 (range: 7.32–8.37) vs. 10.1 (range: 9.40–11.7)g/dL; p-value=0.0006)] and in those withelevated TRV [8.10 (range: 7.25–9.34) vs. 9.42 (range: 7.81–10.6)g/dL; p-value=0.023]. A comparison
Table1–Clinicaldata,lungfunction,computed
tomographyabnormalities,andechocardiography
findingsof59patients.
Variable Value–n(%)
Clinicaldata(n=59)
Malegender 27(45.8)
Afro-descendant 59(100)
Historyofvaso-occlusivepainepisode
None 22(37.3)
1/year 26(44.1)
≥2/year 11(18.7)
Historyofacutechestsyndrome 25(42.4)
Historyofasthma 9(15.3)
Historyofstroke 6(10.2)
Historyofseizures 4(6.78)
Historyofavascularnecrosis 15(25.4) Historyofacutesplenicsequestration 8(13.6)
Historyoftransfusions
None 16(27.1)
1/year 31(52.5)
≥2/year 12(20.3)
Historyofinfections
None 16(27.1)
1/year 32(54.2)
≥2/year 11(18.7)
Historyofhospitalizations
None 18(30.5)
1/year 32(54.2)
≥2/year 9(15.3)
Hydroxyureatherapy 34(57.6)
Lungfunction(n=57)
Noabnormality 17(29.8)
Restrictiveabnormality 20(35.1)
Obstructiveabnormality 7(12.3)
Reducedrespiratorymusclestrength 29(50.9)
Computedtomography(n=46)
Noabnormality 3(6.50)
Reticularpattern 10(21.7)
Ground-glassopacification 9(19.6)
Mosaicattenuation 18(39.1)
Lobarvolumeloss 20(43.5)
Tractionbronchiectasis 4(8.70)
Spleen
Noabnormality 6(13)
Atrophic 36(78.3)
Splenomegaly 4(8.70)
Echocardiography(n=56)
Noabnormality
Increasedrightatrium 6(10.7)
Increasedrightventricle 6(10.7)
Increasedleftatrium 37(66.1)
Increasedleftventricle 29(51.8)
Elevatedtricuspidregurgitationvelocity 25(44.6)
Diastolicdysfunction 9(16.1)
100
90
80
70
60
50
%
40
30
20
10
0
History of acute chest syndrome
Restrictive abnormality
No history of acute chest syndrome 85.0
15.0
21.6 78.4 P<.0001
No restrictive abnormality
Figure1–Comparisonbetweenpatientswithandwithout ahistoryofacutechestsyndromeinrelationtorestrictive abnormalitiesasmeasuredbypulmonaryfunctiontests (chi-squaretest).
increasedrightatrium(RA)sizeandincreasedrightventricle (RV)sizerevealedahigherfrequencyofparenchymal abnor-malitiesonCTscans(40%vs.2.6%;p-value=0.028).
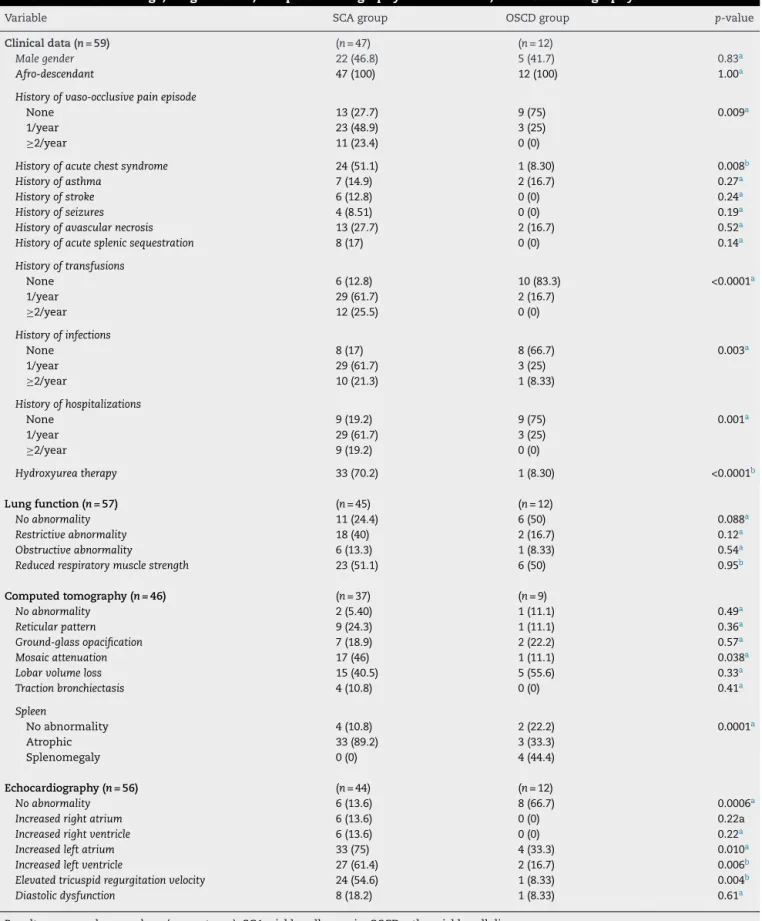
AcomparisonofSCAandOSCDpatientsrevealedno signifi-cantagedifference[27(range:22–41)yearsintheSCAgroupvs. 26(range:23–36)yearsintheOSCDgroup;p-value=0.90]. How-ever,Hblevelsdifferedsignificantlybetweenthesetwogroups [8.10(range:7.40–8.90)g/dLintheSCAgroupvs.11.1(range: 10.0–12.9)g/dLintheOSCDgroup;p-value=0.0001].Ahistory oflegulcersandpriapismwasreportedinsevenandsixSCA patients,respectively;however,noneoftheOSCDpatientshad ahistoryofpriapism orlegulcers.Comparisonsofclinical, PFT,CT,andechocardiographydatabetweenthetwogroups areshowninTable2.
100 90
80 70 60 50
33.3 66.7
4.3 95.7
40 30 20 10
0
%
P<.016
Ground-glass opacification No ground-glass opacification
Reduced respiratory muscle strength
Normal respiratory muscle strength
Figure2–Comparisonbetweenpatientswithandwithout apatternofground-glassopacificationinrelationto reducedrespiratorymusclestrengthasmeasuredby pulmonaryfunctiontests(Fisher’sexacttest).
Discussion
The main findings of this study are that cardiopulmonary abnormalities,comprisingboththestructureandfunctionof the cardiacand pulmonarysystems,are frequentinadults withSCD.TherestrictiveabnormalitiesobservedonthePFTs are associated with a much higher frequency of ACS and increasedLVsize.Inaddition,asignificant associationwas foundbetweendecreasedRMSandahigherfrequencyofa GGOpatternonCTscans.PatientswithelevatedTRVshowed ahigher frequencyofmosaicattenuationonCTscans and lower serum Hb levels. Compared tothe OSCD group,SCA patientsweremorelikelytohaveahistoryofvaso-occlusive painepisodes,ahistoryofACS,amosaicattenuationpattern onCTscans,and abnormalitiesonechocardiography;allof thesefindingsshowedsignificantdifferencesbetweenthetwo groups.
Therespiratoryandcardiovascularsystemsarethemost importantsystemsinvolvedinSCDand areresponsiblefor thesignificantmorbidityandmortalityofthedisease.Inthe presentstudy,evaluationsusingPFTs,CT,and echocardiogra-phyinadultpatientsshowedahighfrequencyofimpairment ofthelungs(93.5%)andheart(75%),withtheseresultsbeing similar to those found in other studies.8,10,21,22,24 With an
increasinglifeexpectancyofSCDpatients,ahigherpercentage ofthispopulationisexpectedtodevelopchronic complica-tions,includingpulmonaryfibrosisandPH.25
Previous studies have suggested that the detection of abnormalitiesinPFTsisthefirstclearsignofchronicsickle celllungdisease;therefore,thesetestscouldbevaluablefor patientmanagementandfollow-up.7,8 Similartothestudies
conductedbyLuntet al.21 and Sylvesteret al.,22 restrictive
abnormalitieswereobservedin35.1%ofthepatients evalu-atedinthecurrentstudy.Anassociationbetweenrestrictive damageand ahigher frequencyofACSwas alsoobserved, whichcanbeexplained,atleastinpart, bychronic hemol-ysisandrepeatedepisodesofintermittentvascularocclusion, which lead to tissue damage.8,22 In contrast to the study
100
61.1
P=.014
38.9
76.0
24.0 90
80
70
60
50
40
30
20
10
0
Normal TRV Elevated TRV
Mosaic attenuation No mosaic attenuation
%
Figure3–Comparisonbetweenpatientswithandwithout elevatedtricuspidregurgitationvelocityinrelationtothe mosaicattenuationpatternshownonchestcomputed tomography(chi-squaretest).
Table2–Clinicalfindings,lungfunction,computedtomographyabnormalities,andechocardiography.
Variable SCAgroup OSCDgroup p-value
Clinicaldata(n=59) (n=47) (n=12)
Malegender 22(46.8) 5(41.7) 0.83a
Afro-descendant 47(100) 12(100) 1.00a
Historyofvaso-occlusivepainepisode
None 13(27.7) 9(75) 0.009a
1/year 23(48.9) 3(25)
≥2/year 11(23.4) 0(0)
Historyofacutechestsyndrome 24(51.1) 1(8.30) 0.008b
Historyofasthma 7(14.9) 2(16.7) 0.27a
Historyofstroke 6(12.8) 0(0) 0.24a
Historyofseizures 4(8.51) 0(0) 0.19a
Historyofavascularnecrosis 13(27.7) 2(16.7) 0.52a
Historyofacutesplenicsequestration 8(17) 0(0) 0.14a
Historyoftransfusions
None 6(12.8) 10(83.3) <0.0001a
1/year 29(61.7) 2(16.7)
≥2/year 12(25.5) 0(0)
Historyofinfections
None 8(17) 8(66.7) 0.003a
1/year 29(61.7) 3(25)
≥2/year 10(21.3) 1(8.33)
Historyofhospitalizations
None 9(19.2) 9(75) 0.001a
1/year 29(61.7) 3(25)
≥2/year 9(19.2) 0(0)
Hydroxyureatherapy 33(70.2) 1(8.30) <0.0001b
Lungfunction(n=57) (n=45) (n=12)
Noabnormality 11(24.4) 6(50) 0.088a
Restrictiveabnormality 18(40) 2(16.7) 0.12a
Obstructiveabnormality 6(13.3) 1(8.33) 0.54a
Reducedrespiratorymusclestrength 23(51.1) 6(50) 0.95b
Computedtomography(n=46) (n=37) (n=9)
Noabnormality 2(5.40) 1(11.1) 0.49a
Reticularpattern 9(24.3) 1(11.1) 0.36a
Ground-glassopacification 7(18.9) 2(22.2) 0.57a
Mosaicattenuation 17(46) 1(11.1) 0.038a
Lobarvolumeloss 15(40.5) 5(55.6) 0.33a
Tractionbronchiectasis 4(10.8) 0(0) 0.41a
Spleen
Noabnormality 4(10.8) 2(22.2) 0.0001a
Atrophic 33(89.2) 3(33.3)
Splenomegaly 0(0) 4(44.4)
Echocardiography(n=56) (n=44) (n=12)
Noabnormality 6(13.6) 8(66.7) 0.0006a
Increasedrightatrium 6(13.6) 0(0) 0.22a
Increasedrightventricle 6(13.6) 0(0) 0.22a
Increasedleftatrium 33(75) 4(33.3) 0.010a
Increasedleftventricle 27(61.4) 2(16.7) 0.006b
Elevatedtricuspidregurgitationvelocity 24(54.6) 1(8.33) 0.004b
Diastolicdysfunction 8(18.2) 1(8.33) 0.61a
Resultsexpressedasnumbers(percentages).SCA:sicklecellanemia;OSCD:othersicklecelldiseases. a ComparisonusingtheFisher’sexacttest.
by Delclaux et al.,24 which found no association between
echocardiographicfindingsand the parametersobtainedin the PFTs, an association between restrictive abnormalities andincreasedLVsizewasobservedinthisstudy.Thisisnot surprisingbecauseLVdilationcanreducelungvolumevia sev-eralmechanisms, including pulmonarycongestionand the directeffectofcompressionoftheheart onthepulmonary parenchyma.26Therefore,acardiacevaluationshouldbe
per-formedintheabsenceofanapparentpulmonarycausethat justifiestherestrictiveabnormalityobservedinPFTs.
Inthepresentstudy,theimpairmentofRMSwasobserved in 50% ofpatients and was the most commonly observed abnormalityinthePFTs.Oharaetal.27recentlyreportedcases
ofweaknessoftherespiratorymusclesinSCDpatients. Sev-eralmechanismsmaybeinvolvedindecreasedRMSinthese patients,includingshallowbreathingduetochestpain, sub-acutevaso-occlusion,whichaffectsmuscleperformance,and deformitiesofthethoraciccavityresultingfrom successive boneinfarctionsandosteoporosis.27,28Interestingly,an
asso-ciationbetweendecreasedRMSandtheappearanceofaGGO patternonCT scanswasfoundinthe currentstudy. Previ-ousresearchhadreportedahighfrequencyofaGGOpattern in SCD patients but did not evaluate its association with pulmonaryfunction.8,21,22 TheGGO pattern on CTscans is
nonspecificandmayreflecttheoccurrenceofdifferent mech-anisms. The results of this study suggest that the partial collapseoftheairwayspacesafterinspirationresultingfrom respiratorymuscleweaknesscouldexplain,atleastinpart, thisassociation.29
Recentstudieshaveshownthatincreasedcardiacoutput, rather than primary changes in pulmonary microvascula-ture, appears to be responsible for changes in pulmonary hemodynamicsinSCDpatients.10,11 Mushemi-Blakeetal.10
recentlydemonstrated,viarightheartcatheterization(RHC), thatalthoughmorethan35%ofpatientshaveelevatedTRV, less than 5% have PH. Therefore, the present study used the measurementofTRVinstead ofthe estimation of sys-tolicpulmonaryarterypressure.Interestingly,anassociation betweenelevatedTRVandtheappearanceofamosaic atten-uation pattern on CTwas observed, which isindicative of both occlusive vascular disease and obstructive disease of the small airways.30 The elevated TRV and low serum Hb
levels observed in the present study have been reported previously.10
Thepresentstudyshowedhigherfrequenciesofhistoryof vaso-occlusivepainepisodes,historyofACS,amosaic atten-uationpatternonCTscans,andechocardiographicchanges inSCApatientsthaninthosewithOSCD.However,no signifi-cantdifferenceswereobservedintheparametersfoundinthe PFTs.Koumbourlisetal.15observednormalpulmonary
func-tioninchildrenwiththeHbSCformofSCDanddecreases inpulmonaryfunctionovertimeinamannersimilartothat observedinSCAchildren.Becausethisstudyevaluatedonly adultpatients,theabsenceofsignificantdifferencesbetween thetwogroupsinthePFTsseemstobesupported,atleastin part,bytheprogressivedeclineinlungfunctionthatoccurs from childhoodtoadulthood.Notably,the twogroups pre-sentedahighpercentageofpatientswithreducedRMS(51.1% vs.50.0%).
Somelimitationsofthisstudyshouldbementioned.First, the small sample sizeof the study and its cross-sectional nature limitan analysis ofcause and effect. Second,RHC, which could help assess the impact of cardiopulmonary hemodynamics onthe parameters evaluated, was not per-formedinthestudyparticipants.However,RHCisaninvasive methodandhasinherentrisks,whichmakesits implemen-tation impracticalinallpatients. Despitetheselimitations, theresultsjustifyfurtherresearchoncertainaspectsofSCD, including the involvementofRMS, asit may elucidate the pathophysiologicalmechanismsinvolvedinthisdiseaseand assistinthedesignofrehabilitationprograms.
Conclusion
In SCD patients, asignificant interrelation between abnor-malities of the structure and function of pulmonary and cardiovascularsystemswasobserved.Restrictive abnormal-itiesareassociatedwithincreasedLVsize,whereasamosaic attenuation pattern on CT scans is associated with ele-vated TRV. In these patients, an association was observed betweenreducedRMSandtheappearanceofaGGOpattern onCTscans.Furthermore,theseverityofthecardiopulmonary parametersamongSCApatientswashigherthanthatamong OSCDpatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MachadoRF,GladwinMT.Pulmonaryhypertensionin hemolyticdisorders:pulmonaryvasculardisease:theglobal perspective.Chest.2010;1376Suppl.:30S–8S.
2.Canc¸adoR,JesusJA.Adoenc¸afalciformenoBrasil.RevBras HematolHemoter.2007;29(3):204–6.
3.LoggettoSR.Sicklecellanemia:clinicaldiversityandbeta S-globinhaplotypes.RevBrasHematolHemoter.
2013;35(3):153–62.
4.SteinbergMH.Predictingclinicalseverityinsicklecell anaemia.BrJHaematol.2005;129(4):465–81.
5.CastroO,GladwinMT.Pulmonaryhypertensioninsicklecell disease:mechanisms,diagnosisandmanagement.Hematol OncolClinNorthAm.2005;19(5):881–96.
6.FrenettePS,AtwehGF.Sicklecelldisease:olddiscoveries,new concepts,andfuturepromise.JClinInvest.2007;117(4):850–8.
7.PowarsD,WeidmanJA,Odom-MaryonT,NilandJC,JohnsonC. Sicklecellchroniclungdisease:priormorbidityandtherisk ofpulmonaryfailure.Medicine(Baltimore).1988;67(1):66–76.
8.KlingsES,WyszynskiDF,NolanVG,SteinbergMH.Abnormal pulmonaryfunctioninadultswithsicklecellanemia.AmJ RespirCritCareMed.2006;173(11):1264–9.
9.MillerAC,GladwinMT.Pulmonarycomplicationsofsicklecell disease.AmJRespirCritCareMed.2012;185(11):1154–65.
3-dimensionalechocardiography/Dopplerstudy.PLOSONE. 2015;10(8):e0135472.
11.ParentF,BachirD,InamoJ,LionnetF,DrissF,LokoG,etal.A hemodynamicstudyofpulmonaryhypertensioninsicklecell disease.NEnglJMed.2011;365(1):44–53.
12.GladwinMT,SachdevV,JisonML,ShizukudaY,PlehnJF, MinterK,etal.Pulmonaryhypertensionasariskfactorfor deathinpatientswithsicklecelldisease.NEnglJMed. 2004;350(9):886–95.
13.VasconcelosMC,NunesMC,BarbosaMM,FernandesBM, PassagliaLG,SilvaCM,etal.Leftventricularremodelingin patientswithsicklecelldisease:determinantsfactorsand impactonoutcome.AnnHematol.2015;94(10):1621–9.
14.GladwinMT,SachdevV.Cardiovascularabnormalitiesin sicklecelldisease.JAmCollCardiol.2012;59(13):1123–33.
15.KoumbourlisAC,LeeDJ,LeeA.Lungfunctionandsomatic growthinpatientswithhemoglobinSCsicklecelldisease. PediatrPulmonol.2008;43(2):175–8.
16.MurrayJF,NadelJA.Textbookofrespiratorymedicine.2nded. Philadelphia:WBSaundersCompany;1994,2739pp.
17.MillerMR,HankinsonJ,BrusascoV,BurgosF,CasaburiR, CoatesA,etal.Standardizationofspirometry.EurRespirJ. 2005;26(2):319–38.
18.PereiraCA,SatoT,RodriguesSC.Newreferencevaluesfor forcedspirometryinwhiteadultsinBrazil.JBrasPneumol. 2007;33(4):397–406.
19.NederJA,AndreoniS,Castelo-FilhoA,NeryLE.Reference valuesforlungfunctiontests.I.Staticvolumes.BrazJMed BiolRes.1999;32(6):703–17.
20.NederJA,AndreoniS,LerarioMC,NeryLE.Referencevalues forlungfunctiontests.II.Maximalrespiratorypressuresand voluntaryventilation.BrazJMedBiolRes.1999;32(6):719–27.
21.LuntA,DesaiSR,WellsAU,HansellDM,MushemiS,Melikian N,etal.Pulmonaryfunction,CTandechocardiographic abnormalitiesinsicklecelldisease.Thorax.2014;69(8):746–51.
22.SylvesterKP,DesaiSR,WellsAU,HansellDM,AwogbadeM, TheinSL,etal.Computedtomographyandpulmonary functionabnormalitiesinsicklecelldisease.EurRespirJ. 2006;28(4):832–8.
23.LangRM,BadanoLP,Mor-AviV,AfilaloJ,ArmstrongA, ErnandeL,etal.Recommendationsforcardiacchamber quantificationbyechocardiographyinadults:anupdatefrom theAmericanSocietyofEchocardiographyandtheEuropean AssociationofCardiovascularImaging.EurHeartJCardiovasc Imaging.2015;16(3):233–70.
24.DelclauxC,Zerah-LancnerF,BachirD,HabibiA,MoninJL, GodeauB,etal.Factorsassociatedwithdyspneainadult patientswithsicklecelldisease.Chest.2005;128(5): 3336–44.
25.VijR,MachadoRF.Pulmonarycomplicationsof hemoglobinopathies.Chest.2010;138(4):973–83.
26.MottramCD.Ruppel’smanualofpulmonaryfunctiontesting. 10thed.MarylandHeights:Elsevier/Mosby;2013,514pp.
27.OharaDG,RuasG,WalshIA,CastroSS,JamamiM.Lung functionandsix-minutewalktestperformanceinindividuals withsicklecelldisease.BrazJPhysTher.2014;18(1):
79–87.
28.OngBA,CabootJ,JawadA,McDonoughJ,JacksonT,ArensR, etal.Respiratorymuscleforceandlungvolumechangesina populationofchildrenwithsicklecelldisease.BrJHaematol. 2013;163(1):112–7.
29.SilvaCI,MarchioriE,SouzaJúniorAS,MüllerNL,Comissãode ImagemdaSociedadeBrasileiradePneumologiaeTisiologia. IllustratedBrazilianconsensusoftermsandfundamental patternsinchestCTscans.JBrasPneumol.2010;36(1):99–123.