w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Retained
or
expelled
staples
after
transanal
stapled
surgery:
this
is
the
problem!
Alessandro
Sturiale
a,∗,
Jacopo
Martellucci
b,
Gabriele
Naldini
a aCisanelloUniversityHospital,ProctologicalandPerinealSurgicalUnit,Pisa,ItalybCareggiUniversityHospital,EmergencyandMini-invasiveSurgery,Florence,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31March2017 Accepted4June2017 Availableonline13July2017
Keywords:
Stapledtransanalresection Haemorrhoids
STARR ODS Staples
a
b
s
t
r
a
c
t
Studyobjective:Theaimistoassessthepresenceandpersistenceoftheagraphesatthelevel ofstaplelineaftertransanalstapledsurgery.
Methods:FromApriltoDecember2016one-hundred-thirteenpatientswithvariable follow-up(6months–10years)wererandomlyselectedamongallthepatientsundergonetransanal stapledsurgeryforhaemorrhoidaldiseaseorfunctionaldisorderssuchasobstructed defeca-tionsyndrome.Only87patientsagreedtoparticipatethisstudy.Allthepatientsunderwent digitalexploration,anoscopyand360◦tridimensionaltransanalultrasound.
Mainresults:Differenttypesofstapledtransanalsurgicalprocedureswereperformed:48 transanalrectalresectionwithhighvolumedevice,24stapledhaemorrhoidopexy,8Double StapledHaemorrhoidopexy,7Transtarr.In41.4%thestaplelinewasnotidentifiedwith digitalexaminationoranoscopyand17.2%ofpatientshavesomestaplespartiallyexpelled insidethelumen.360◦tridimensionaltransanalultrasoundshowedacompletestapleline
attheano-rectaljunctionwhichappearsasaninterruptedhyperechoiccircularlayer.
Conclusion:Thestaplesafterstapledtransanalsurgeryremainatthelevelofthestapleline independentlyfromthedeviceusedbythesurgeonleadingtothenecessityofasharedand adequatelanguage,infacttheshedstaplesneedtobeconsideredasexpelledinsteadof retained.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileirade Coloproctologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Grampos
retidos
ou
expelidos
em
seguida
à
cirurgia
transanal
com
grampeador:
eis
aí
o
problema!
Palavras-chave:
Ressecc¸ãotransanalcom grampeador
Hemorroidas
r
e
s
u
m
o
Objetivodoestudo:Avaliarapresenc¸aepersistênciadosagrafesaoníveldalinhadeaplicac¸ão dosgrampos,emseguidaàcirurgiatransanalcomgrampeador.
Métodos:Deabrilatédezembrode2016,113pacientescomseguimentosvariáveis(6 meses-10anos)foramaleatoriamenteselecionadosentretodosospacientestratadoscomcirurgia
∗ Correspondingauthor.
E-mail:[email protected](A.Sturiale).
http://dx.doi.org/10.1016/j.jcol.2017.06.005
STARR ODS Grampos
transanal comgramposparatratamentodehemorroidas oudetranstornosfuncionais, por exemplo, síndromede evacuac¸ãoobstruída. Apenas 87pacientes concordaramem participardoestudo.Todosospacientespassaramporexplorac¸ãodigital,anoscopiae ultra-ssonografiatransanaltridimensionalde360◦.
Resultados principais: Foram realizados diferentes tipos de procedimentos cirúrgicos transanaiscomgrampeador:48ressecc¸õesretaistransanaiscomusodegrampeadorde grandevolume,24hemorroidopexiascomgrampeador,8hemorroidopexiascomgrampos duplose7procedimentoscomgrampeadorTranstar.Em41,4%dostratamentos,nãofoi pos-sívelidentificaralinhadegrampeamentocomexamedigitaloucomanoscopia,eem17,2% dospacientesalgunsgramposforamexpelidosparaolúmen.Aultrassonografiatransanal tridimensionalde360◦revelouumalinhadegrampeamentocompletonajunc¸ãoanorretal,
assumindooaspectodeumacamadacircularhiperecoicainterrompida.
Conclusão: Emseguidaàcirurgiatransanalcomgrampeamento,osgrampospermanecem aoníveldalinhadegrampeamento,independentementedotipodegrampeadorusadopelo cirurgião,oquetornanecessáriaumalinguagemcompartilhadaeadequada;defato,os grampossoltosdevemserconsideradoscomoexpelidos,emlugarderetidos.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade Coloproctologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Mechanicalstaplerisoneofthegreatestsurgicalinnovation ofthelastcentury.Itallowstoperformquickandeasy pro-ceduresresultingsafeand effective.Thepioneerofstapler procedureswithhisprototypeweighted3.6kgwasHúmerHült alsoknownasthe“fatherofsurgicalstapling” in1908.The technologicaldevelopmentpassedthroughseveralcountries andlotsofdifferentdevices,firstlyusedforbloodvesselsand thenappliedtotheboweltoo.1–5 Fromtheinitialapplication
intheabdominalopensurgerythetechnologyfollowedthe trendofcontinuoussurgical improvementmaintainingthe samestandardlevelsalsointhenewlaparoscopicapproach and it always leaded to new devices. Stapled surgery for thetreatmentofhaemorrhoidalprolapse, theso-called sta-pledhaemorrhoidopexy(SH),wasfirstlydescribedbyLongo in 1998 as a less painful alternative to the conventional haemorroidectomy.6 Sincethatmoment,therewere lots of
technologicalchanges,someofthemareclearlyvisiblesuch astheshapeand ergonomicswhileothers areless evident butfundamentaltoimprovedeviceperformance.Acommon elementtoallthedifferenttypeofstapleristheuseof non-magnetic,inert metalstaples which may guaranteea long lasting.Lotsofstudywereperformedtoassessmetals prop-ertiesandtheyconcludethatthebestchoiceistitaniumor titaniumalloy7ratherthanstainlesssteelwhichwasusedat
first.Althoughitmayseemfairlyclearthefateofthestaples afterbowel anastomosis, the surgeons are oftennot well-informedaboutthisand theyuseinaccuratetermscausing lotofconfusionabouttheprocedure,itseffectsandthe possi-blepostoperativecomplications.Theaimofthepresentstudy istoassessthepresenceandpersistenceoftheagraphesat thelevelofstaplelineaftertransanalstapledsurgery.
Methods
From April 2016 to December 2016 one-hundred-thirteen patientswithvariable follow-up(range:6months–10years)
were randomly selected amongall the patients undergone transanalstapledsurgeryforhaemorrhoidaldiseaseor func-tional disorders such as obstructed defecation syndrome (ODS). They were retrospectively collected through clinical records and then telephone called for an outpatient eval-uation. Only 87 patients agreed to undergo this further follow-upnotscheduled.Allthepatientsunderwentphysical examinationthroughdigitalexploration,anoscopyand360◦ tridimensionaltransanalultrasound.Theevaluationwas per-formedbytwoexperiencedsurgeonsspecializedincolorectal andproctologicalsurgery.
Results
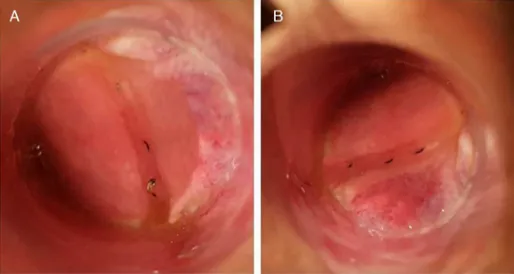
Fig.1–(A,B)Anoscopy:partiallyexpelledstaplesatthelevelofthestapledlinewithoutanysignofinflammation.
Fig.2–360◦tridimensionaltransanalultrasound:yellowarrowsindicatethestapleline.(A)2Dvisualization;(B,C)3D
Discussion
Starting from the beginning of the last century the tech-nology simplified and made it easier some surgical steps. A central role in this field was played by the mechanical staplerwhichwere usedtoperformblood vesselsorbowel anastomosis.1,3 In1998Longo describedthe useofa
circu-larstaplertotreatthehaemorrhoidalprolapse6thenapplied
forobstructeddefecationsyndrometoo.Afterthisexperience stapledhaemorrhoidopexyspreadworldwideandthesaleof thedevices widelyincreased.Thegrowingsurgical innova-tion and theneed toimprove the outcome haveleaded to the introduction ofthe double stapled procedure toresect alltheprolapsedtissuewhichotherwisewouldnotenterin asingledevicecasing.8However,incaseofmultiplesuture
line there are some weak and fixed points atthe level of thecrossingsutures.Anotherconsequenceofmultiple rec-talresectionisthattherectalprolapseisresectedinpieces anditisnotsymmetrical.Whereby,newdedicatedhigh vol-umedeviceswererecentlyintroducedtoallowacylindrical rectal resection.9,10 In all ofthese different phases of
sta-pledprocedureevolutionforthetreatmentofhaemorrhoidal diseaseandODStoo,thecommondenominatorwasthe fash-ioningofrecto-rectalanastomosisusingtitaniumortitanium alloy agraphes.This typeof staples allowsthe patients to undergowhateverradiologicalimagingsuchasCTscanorMRI becausetheyarenonmagneticandinertandtheyguarantee toremaininthesamesite. Althoughit maybeanobvious andsimpleconcept ofthestaplers use, it isnot.In fact, a recent paper reported a surveycarried out among 16 sur-geonsexperiencedinSH.Theauthors askedthemthe fate ofthestaples.Ten(62.5%)ofthemanswered thattheywill beshedwithin3months,3answeredthatthestapleswillbe retainedinsidepermanently,2answered thatonlysomeof themareshedand1expressedignoranceaboutthistopic.11
Thisisaclarifyingstudyregardingtheignoranceand confu-sionaboutthefateofthestaplesusedtotreathaemorrhoidal prolapseorODS-relatedalteredanatomy.Italsorevealedan importantissue, approximately75% ofpatients undergoing stapledsurgerywishestoknowmoreabout thetechnology usedto treattheir disease.11 Besides, the presenceof
par-tiallyexpelledstaplesinsidetherectallumenwhicharenot correctlyintegratedinsidethestaplelineandcoveredbythe mucosallayermaybethecause ofsomebothersome post-operativesymptoms.Thespectrumofthesesymptomscan varyfromsporadicbleedingduetothepresenceofgranuloma abovethepartiallyexpelledstaplestochronicpain, inflamma-torypolyporevenproctitis.12–15Onlyfewcasesarereported
aboutpeniletrauma,condomruptureoranalpainduringanal intercourseafterstapledhaemorroidopexy.16–19
Inthe presentstudy the associationofdigital examina-tion,anoscopyand360◦tridimensionaltransanalultrasound confirmedthatthestaplesaftertransanalstapledprocedure remaininsidetherectal wallatthe levelofthe anastomo-sis and that sometimes only few of them are completely orpartially expelled.Moreover,the long lastingofthe sta-plesresultedtobeindependentfromthetypeofthedevice chosenbythe surgeon (PPH, ContourCCS-30, TST STARR+ 36).
Theseresultsareinkeepingwithotherpublishedpapers aboutstapledproceduresindifferentsurgicalfieldssuchas abdominalsurgery.Nevertheless,nowadaysthepersistenceof thestaplesinsidetheabdomenafterbowelsurgeryorinside the thorax afterlung resection is notso debated. Two are thepossiblereasons.Firstly,staplerinabdominalorthoracic surgeryisroutinelyusedandtheyrepresentonlyastepofthe wholesurgicalprocedure.Theuseofthemechanicaldeviceis notnecessaryanddependsonthesituationandanatomical condition,infact,atpresent,ithasbeenalsodemonstrated that stapled anastomosis iscomparable to the hand-sewn withoutanysuperiorityofoneovertheother.20Secondly,in
upperGI,colorectal21andbariatric22surgerythepresenceand
persistenceofthestaplesattheleveloftheanastomosisis consideredasamarkertoeasilyidentifyitinfluoroscopyor throughCTscananditisusedinthepost-operativeevaluation ofdehiscenceorleak.Ontheotherhand,thechooseofstaple procedureforhaemorrhoidaldiseaseorODSrepresentsthe wholesurgicaltreatment.Animportantkeypointisthatthe staplelineisveryclosetotheexternalanalverge,around4cm, sothatthepatientsthemselvesmayfeelit,differentlyfrom abdominalorthoracicsurgeryinwhichthepatients,evenif theyknow,theyhavenotarealperceptionandawarenessof thestaples.Anotherissue,whichisnotsodebated,isrelated to the anal intercoursesafter this typeofsurgery because boththepatientand/orhis/herpartnersmayexperiencepain, stiffnessorpeniletrauma.Thisconditionrevealedtohavean importantimpactonthequalityoflife,sexualhabitsand per-sonalandsocialsexualityonhomo/bisexualandheterosexual population. However,so farthe literaturelacksacomplete and exhaustivestudy analysingthe impactofthe different proctologicsurgicalproceduresonanalintercourses.
Thisbackgroundclearlyexplainswhythesurgeonsneed todeepenstaplestopic,especiallyforthetreatmentofbenign proctologicdiseaseandalsoclarifywhyitwasnotsodeeply analyzedbefore.Thepresentpaperfirstanalysestherealfate oftheagraphesinpatientswithdifferentfollow-up,upto10 years,aftertransanalstapledsurgery. Theprocedureswere performedwithdifferentdevicestotreathaemorrhoidal dis-ease or functional disorders suchas obstructeddefecation syndrome.
Therefore,itistimetomoveonandtouseacorrectand sharedmedicallanguage. Itisnotmoreadequate tospeak aboutretainedstaplesbecauseallthestaplesormostofthem are usually retained,whereby it is moreaccurateto speak aboutexpelledstaples.Theexpelledstaplesarethosewhich are partiallyor completely shed from the staple line. This may beaconsequenceofanimperfectfire ofthe machine andforthisreasonthecompaniesproducingstaplingdevices continuouslyimprovethefeaturesofthestaplers.Infact, tech-nologicalinnovationleadstotheintroductionandapplication ofnewpatentedchanges,suchaspermanentparallelcontrol system,allowingagreaterstabilityandbalanceduringthefire. Neverthelesssomestaplesaresometimespartiallyexpelled andtheycanremainasymptomaticorarethecauseof postop-erativehassles.Thisconcepthasalsoimportantimplications inthefieldofforensicmedicineregardingcompensationof damagesaftertransanalstapledsurgery.
ofthechosenprocedurewhichneedstobeclearlyreported insidetheinformedconsent.Itmustbeperformedusing pre-ciseand specific terms that the canbe understood bythe patientsand atthe sametime didnotgenerate misunder-standingintheassessmentdonebyforensicdoctors,lawyers andjudges.
Conclusion
Thestaplesafterstapledtransanalsurgeryremainatthelevel ofthestaplelineindependentlyfrom thedeviceused.This conceptleadstothenecessityofacorrectlanguagewhereby theshedstaplesneedtobecalledexpelledinsteadofretained. Besides,theknowledgeofthedeviceanditsrelatedfeatures andpossiblepostoperativeconsequencesisatthebaseofa correctuseofthestapleranditisessentialforanadequate managementofpostoperativecomplicationsortroublesome symptoms.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. UnitedStatesSurgicalCorporationHistory.International directoryofcompanyhistories,vol.34.St.JamesPress;2000.
2. HultlH.IIKongressderUngarischenGesellschaftfur Chirurgie,Budapest,May,1908.PesterMedChirPresse. 1909;45:108–10.
3. RobicsekF.Thebirthofthesurgicalstapler.SurgGynecol Obstet.1980;150:579–83.
4. RobicsekF.Developmentofthesurgicalstaplingdevice. ThoracCardiovascSurg.1993;41:207–15.
5. RobicsekF,KonstantinovI.HumerHultl:thefatherofthe surgicalstapler.JMedBiogr.2001;9:16–9.
6. LongoA.Treatmentofhaemorrhoiddiseasebyreductionof mucosaandhaemorrhoidalprolapsewithcirculastapling device:anewprocedure.In:Proceedingsofthe6thworld congressofendoscopicsurgery.1998.
7. GentilliS,PortigliottiL,AroniciM,FerranteD,SuricoD, MilanesioM,etal.Ultrastructuralanalysisofdifferent-made staplers’staples.MinervaChir.2012;67:439–44.
8. NaldiniG,MartellucciJ,TalentoP,CavigliaA,MoraldiL,Rossi M.Newapproachtolargehaemorrhoidalprolapse:double
stapledhaemorrhoidopexy.IntJColorectalDis. 2009;24:1383–7.
9.NaldiniG,FabianiB,MenconiC,GianiI,TonioloG,Martellucci J.Tailoredprolapsesurgeryforthetreatmentofhemorrhoids withanewdedicateddevice:TSTStarrplus.IntJColorectal Dis.2015;30:1723–8.
10.ReboaG,GipponiM,GalloM,CiottaG,TarantelloM,Caviglia A,etal.High-volumetransanalsurgerywithCPH34HVfor thetreatmentofIII–IVdegreehaemorrhoids:finalshort-term resultsofanItalianmulticenterclinicalstudy.SurgResPract. 2016;2016:2906145.
11.GargP,SidhuG,NairS,SongJ,SinglaV,LakhtariaP,etal.The fateandsignificanceofretainedstaplesafterstapled haemorrhoidopexy.ColorectalDis.2011;13:572–5.
12.FondranJC,PorterJA,SlezakFA.Inflammatorypolyps:a causeoflatebleedinginstapledhemorrhoidectomy.Dis ColonRectum.2006;49:1910–3.
13.PescatoriM,GagliardiG.Postoperativecomplicationsafter procedureforprolapsedhemorrhoids(PPH)andstapled transanalrectalresection(STARR)procedures.Tech Coloproctol.2008;12:7–19.
14.MenconiC,FabianiB,GianiI,MartellucciJ,TonioloG,Naldini G.PersistentanalandpelvicfloorpainafterPPHandSTARR: surgicalmanagementofthefixedscarstapleline.IntJ ColorectalDis.2016;31:41–4.
15.BruscianoL,AyabacaSM,PescatoriM,AccarpioGM,DodiG, CavallariF,etal.Reinterventionsaftercomplicatedorfailed stapledhemorrhoidopexy.DisColonRectum.
2004;47:1846–51.
16.CapomagiA,MannettaV,BalestrieriA.Circular
hemorrhoidectomyusingstapleristhegoldstandardforthe treatmentofhemorrhoids?Preliminarydataregarding206 consecutivepatients.ItalJColoproctol.1990;2:782–5.
17.KekezT,BulicK,SmudjD,MajerovicM.Isstapled hemorrhoidopexysafeforthemalehomosexualpatient? Reportofacase.SurgToday.2007;37:335–7.
18.MlakarB.Shouldweavoidstapledhemorrhoidopexyinmales andfemaleswhopracticereceptiveanalsex?DisColon Rectum.2007;50:1727.
19.RavoB,AmatoA,BiancoV,BoccasantaP,BottiniC,CarrieroA, etal.Complicationsafterstapledhemorrhoidectomy:can theybeprevented.TechColoproctol.2002;6:83–8.
20.NeutzlingCB,LustosaSA,ProencaIM,daSilvaEM,MatosD. Stapledversushandsewnmethodsforcolorectalanastomosis surgery.CochraneDatabaseSystRev.2012:CD003144.
21.ShynPB,MadanR,WuC,ErturkSM,SilvermanSG.PET/CT patternanalysisforsurgicalstaplelinerecurrenceinpatients withcolorectalcancer.AJRAmJRoentgenol.2010;194:414–21.