ABSTRACT
)DFWRUV LQÀXHQFLQJ RUWKRGRQWLF WUHDWPHQW WLPH
for non- surgical Class I I I m alocclusion
Lívia Monteiro BICHARA, Mônica Lídia Castro de ARAGÓN, Gustavo Antônio Martins BRANDÃO, David NORMANDO
Universidade Federal do Pará, Faculdade de Odontologia, Belém, PA, Brasil.
Corresponding address: David Normando - Rua Boaventura da Silva, 567-1201 - Belém - PA - 66.055-090 - Brazil - Phone: +55 91 991446316 - e-mail: [email protected]
6XEPLWWHG1RYHPEHU0RGL¿FDWLRQ0D\$FFHSWHG-XQH
T
RLPSURYHRUWKRGRQWLFWUHDWPHQWHI¿FLHQF\RUWKRGRQWLVWVPXVWNQRZZKLFKYDULDEOHVcould int erfere w it h ort hodont ic t reat m ent t im e. Obj ect ive: To ident ify variables and t heir effect size on ort hodont ic t reat m ent t im e of Class I I I m alocclusion. Mat erial and0HWKRGV)RUW\¿YH&ODVV,,,PDORFFOXVLRQFDVHVZHUHVHOHFWHGIURPSDWLHQWV¶UHFRUGV
Clinical chart s, cephalom et ric radiographs, and pre and post t reat m ent dent al cast s w ere evaluat ed. Age, sex, PAR index at T1 and T2, overj et , m issing t eet h, ext ract ions, num ber of t r eat m ent phases, m issed appoint m ent s, appliance br eak ages, and cephalom et r ic variables SNA, SNB, ANB, Wit s, SnGoGn, CoA, CoGn, I MPA, 1.PP w ere invest igat ed by m ult iple linear regression analysis and st epw ise m et hod at p< 0.05. The sam ple was also divided int o t w o groups: Group 0- 2 ( pat ient s w ho had m issed t w o clinical appoint m ent s or less) and Group > 2 ( pat ient s w ho m issed m ore t han 2 appoint m ent s) , t o det ect t he
LQÀXHQFHRIWKLVGDWDRQWUHDWPHQWWLPHDQGWKHTXDOLW\RIWKHWUHDWPHQW3$575HVXOWV
Average t reat m ent t im e was 30.27 m ont hs. Mult iple regression analysis showed t hat m issed appoint m ent ( R2= 0.4345) and appliance breakages ( R2= 0.0596) are t he only variables
DEOHWRVLJQL¿FDQWO\SUHGLFWWUHDWPHQWGXUDWLRQ7UHDWPHQWWLPHIRUSDWLHQWVZKRPLVVHG PRUHWKDQDSSRLQWPHQWVZDVQHDUO\RQH\HDUORQJHU+RZHYHUQRVLJQL¿FDQWLQÀXHQFH
on PAR T2 was observed for t hose pat ient s. Conclusion: Ort hodont ic t reat m ent durat ion in
&ODVV,,,SDWLHQWVLVPDLQO\LQÀXHQFHGE\IDFWRUVUHODWHGWRSDWLHQWFRPSOLDQFH3DWLHQWVZKR PLVVHGPRUHDSSRLQWPHQWVGLGQRWVKRZZRUVHRUWKRGRQWLF¿QLVKLQJEXWORQJHUWUHDWPHQW
No occlusal, cephalom et ric, or dem ographic variable obt ained before t reat m ent was able
WRJLYHVRPHVLJQL¿FDQWSUHGLFWLRQDERXWWUHDWPHQWWLPHLQ&ODVV,,,SDWLHQWV
Keyw ords:2UWKRGRQWLFVWUHDWPHQW$QJOH&ODVV,,,PDORFFOXVLRQ7UHDWPHQWHI¿FLHQF\
I N TRODUCTI ON
Ort hodont ic t reat m ent durat ion has always been a m aj or concern t o bot h pat ient s and professionals. I n an at t em pt t o predict t reat m ent cost s, pat ient s want t o know how long t heir ort hodont ic t reat m ent will t ake6. Likew ise, braces can cause discom fort
and inconveniences relat ed t o daily rout ine changes. For or t hodont ist s, a m or e pr ecise pr edict ion of t he durat ion of a t reat m ent can earn pat ient s’ t rust , represent ing a valuable t ool for a successful t reat m ent26. “ Trut h and accurat e t im e est im at ion”
are t w o of t he m ost frequent recom m endat ions, follow ed by “ reduct ion in t reat m ent fees”19. Also,
or t h odon t ic t r eat m en t h as biological cost s an d long t r eat m ent s have been associat ed w it h r oot resorpt ion17,22. Therefore, a bet t er underst anding
of t h e f act or s in f lu en cin g t r eat m en t t im e can
SURYLGHVXSHULRUFRVWEHQH¿WRXWFRPHVDVLWDOORZV
or t h odon t ist s t o m an age t r eat m en t , ach iev in g, t hus, great result s in less t im e.
Fa ct o r s t h a t co u l d i n t er f er e o n t r ea t m en t durat ion include sex11, pret reat m ent ANB value11,27
,
ov er b it e2 7, cr ow d in g2 , 2 7, ex t r act ion s2 , 1 1 , 2 7, t im e
b et w een a p p o i n t m en t s2, t r ea t m en t p h a ses2 9,
age10,20, overj et6,20,t echnique26, pat ient com pliance
( including m issed appoint m ent s and debonds)16,20,27 ,
p u b l i c o r p r i v at e p r act i ce3 0, o r al h y g i en e1 2 , 2 7,
sch olar g r ad es1 2, car ies1 2, r est or at ion s1 2, ar ch
coordinat ion12, parent ’s occupat ion12.
How ev er, t o t h e best of ou r k n ow ledge, all previous st udies, including a syst em at ic review15,
Class I I I m olar r elat ionship and t r eat m ent t im e has been descr ibed31. This m ight be due t o t he
low prevalence of Class I I I m alocclusion, around 5% of a populat ion,7,18 and t he high accept ance of
t reat m ent need by professionals and pat ient s for t hose cases7,9,21.
C l a s s I I I m a l o c c l u s i o n h a s p a r t i c u l a r charact erist ics t hat differ from ot hers m alocclusions. Despit e it s low prevalence9,21, t he im pact on
life-qualit y is high7. Also, Class I I I grow t h pat t ern has
som e part icularit ies w hen com pared w it h Class I and Class I I pat ient s, as m ore vert ical pat t ern and longer grow t h peak for Class I I I t han for Class I pat ient s4. While m andibular grow t h w orks for t he EHQH¿WRI&ODVV,,WUHDWPHQWLQ&ODVV,,,SDWLHQWV¶ PDQGLEXODU JURZWK LPSRVHV RQH PRUH GLI¿FXOW\
Furt herm ore, relapse aft er ort hodont ic t reat m ent is frequent ly report ed8.
The know ledge of w hich variables can int erfere in Class I I I t reat m ent durat ion m ight help clinicians t o act u p on con t r ollab le v ar iab les, p er f or m in g
PRUHHI¿FLHQW&ODVV,,,WUHDWPHQW7KHUHIRUHRXU
obj ect ive is t o evaluat e var iables pr esent in t he ort hodont ic int ervent ion for Class I I I m alocclusion
WKDWFRXOGLQÀXHQFHWUHDWPHQWGXUDWLRQ
MATERI AL AN D METHODS
This st udy received et hical approval from The Research Et hics Com m it t ee of t he Federal Universit y of Pará ( num ber 517.398, 2014) . Sam ple size was est im at ed using GPow er 3.1 soft ware. To det ect a 0.35 effect size using six independent variables, alfa level of 0.05, and pow er of 0.8, w e needed
WR DVVHVV SDWLHQWV )RUW\¿YH 19 fem ale and 26m ale) consecut ively t r eat ed Class I I I pat ient s w er e r et r ospect ively select ed fr om ¿OHVof
an experienced ort hodont ist . The inclusion crit eria were: non- syndrom ic dent al Class I I I subj ect s wit h Class I I I m olar relat ionship; edge t o edge incisor r elat ion sh ip or an t er ior cr ossb it e; p er m an en t dent it ion t reat ed w it h full ort hodont ic appliance in bot h arches. Exclusion crit eria com prised pat ient s w ho had m ore t han one m issing t oot h per hem i-arch, who m issed over 16 appoint m ent s, and t hose w ho w ere surgically t reat ed. No pat ient had TAD’s placed before or during t reat m ent or w ere t reat ed w it h self- ligat ing bracket s.
Dat a were collect ed from clinical records, dent al cast s, and cephalom et ric radiographs. The ages at t he beginning of t reat m ent ( T1) ranged from 9.5 t o 48 years old, and m ean age was 22.02 years. Treat m ent was perform ed using preadj ust ed t w in bracket s w it h .022x.028 slot .
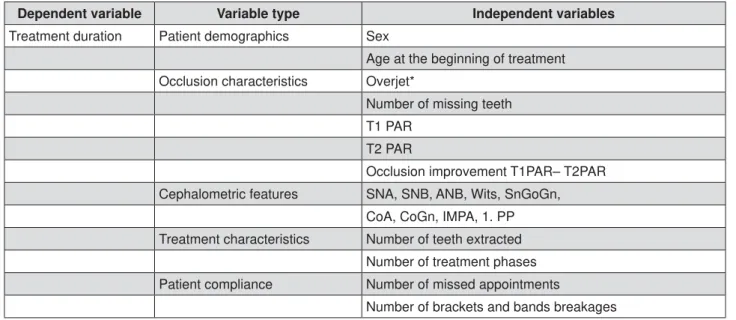
The inform at ion collect ed from dent al records w ere age, sex, durat ion of ort hodont ic t reat m ent , n u m ber of t r eat m en t ph ases, n u m ber of t eet h extractions due to treatm ent plan, num ber of m issing t eet h before t reat m ent , m issed appoint m ent s, and appliance br eak ages ( Figur e 1) . Sagit t al incisor relat ionship was evaluat ed based on t he overj et sect ion of PAR index. Each int erval longer t han 45 days bet w een t w o consecut ive clinical visit s w ere considered as m issed appoint m ent . The num ber of ext ract ions or m issing t eet h was sought in t he
FOLQLFDO UHFRUGV DQG FRQ¿UPHG XVLQJ SDQRUDPLF
r ad iog r ap h s f r om b ef or e an d af t er t r eat m en t . Dent oskelet al m easurem ent s SNA, SNB, ANB, Wit s, SnGoGn, CoA, CoGn, I MPA, and 1.PP were obt ained
IURP FHSKDORPHWULF UDGLRJUDSKV DLPLQJ WR ¿QG LI WUHDWPHQW WLPH LV LQÀXHQFHG E\ FHSKDORPHWULF
variables.
Dent al cast s w ere assessed t o obt ain PAR index before ( T1) and aft er ort hodont ic t reat m ent ( T2) ,
Dependent variable Variable type Independent variables
Treatment duration Patient demographics Sex
Age at the beginning of treatment
Occlusion characteristics Overjet*
Number of missing teeth
T1 PAR
T2 PAR
Occlusion improvement T1PAR– T2PAR
Cephalometric features SNA, SNB, ANB, Wits, SnGoGn,
CoA, CoGn, IMPA, 1. PP
Treatment characteristics Number of teeth extracted
Number of treatment phases
Patient compliance Number of missed appointments
Number of brackets and bands breakages
*Measured by PAR index
accor ding t o Richm ond, et al.23 ( 1992) , using a digit al caliper ( Mit ut oyo- Suzano, São Paulo, Brazil). PAR index23 was doubled m easured in t went y dent al cast s w it h a 30- day int er val. All dat a r et r iev ed from dent al cast s and cephalom et ric radiographs
ZHUHFRQ¿UPHGE\DVHFRQGH[DPLQHU,QWUD&ODVV
cor r elat ion t est w as calcu lat ed t o evalu at e t h e reliabilit y of m easurem ent s.
Co r r e l a t i o n b e t w e e n t r e a t m e n t d u r a t i o n ( depen den t v ar iable) an d con t in u ou s v ar iables ret rieved from pat ient s’ records was analyzed using Pearson’s Correlat ion t est . The St udent ’s t t est for 2 independent sam ples was applied t o search for differences in t reat m ent durat ion bet ween genders. Th en , m u lt ip le lin ear r eg r ession w as u sed t o
H[DPLQHWKHLQÀXHQFHRILQGHSHQGHQWYDULDEOHVRQ
ort hodont ic t reat m ent t im e ( dependent variable) . The sam ple was divided in 2 groups regarding t he num ber of m issed appoint m ent s t o verify if it was relat ed t o t reat m ent durat ion and PAR at T2. Pat ient s w it h 0 t o 2 m issed appoint m ent s w er e
gat hered in Group 0- 2 ( n= 27; 18 m ale, 9 fem ale) , and pat ient s wit h m ore t han 2 m issed appoint m ent s in Group > 2 ( n= 18; 9 m ale and 9 fem ale) . Norm al
GLVWULEXWLRQZDVYHUL¿HGXVLQJ'¶$JRVWLQR3HDUVRQ¶V
t est an d descr ipt iv e st at ist ics w er e calcu lat ed. St udent t t est was applied t o evaluat e differences bet w een group variables w it h norm al dist ribut ion, and, for variables wit h abnorm al dist ribut ion, Mann-Whit ney t est was applied.
St at ist ical analysis was perform ed w it h Bioest at 5. 3 soft w ar e ( Mam irauá I nst it ut e, Belém , Par á,
%UD]LO$OOWHVWVDSSOLHGXVHGWKHOHYHORIVLJQL¿FDQFH
at 5% .
RESULTS
An excellent reliability of PAR index m easurem ents w as o b ser v ed ( I CC= 0 . 9 5 4 1 , p < 0 . 0 0 1 ) . Mean t reat m ent t im e for Class I I I subj ect s was of 30.27 m ont hs ( ranging from 11.12 t o 54.96) .
Pat ient com pliance, feat ur ed as t he num ber
Variables
Mean/ Median
SD Min Max r p-value
Treatment duration 30.27 10.76 10 54.93 -
-Age at the beginning of treatment 22.2 9.57 9.58 48.75 0.095 0.532
Overjet (PAR index for incisors) 14.60 7.65 0 24 0.159 0.2912
Number of broken brackets or bands 2 3.89 0 16 0.419 0.0041*
Missed appointments 2 3.87 0 16 0.659 <0.0001*
Missing teeth 0 1.32 0 4 0.068 0.6546
Extracted teeth 0 1.21 0 4 -0.044 0.7713
PAR T1 30.28 12.28 3 54 0.3251 0.0292*
PAR T2 2.95 2.17 0 8 0.3229 0.0304*
Occlusion improvement (PAR T1 - PAR T2)
27.3 11.96 2 53 0.177 0.2386
SNA 82.25 4.55 69 93 -0.252 0.0946
SNB 83.09 3.93 73.9 91 -0.343 0.0209*
ANB -0.95 2.55 -7.5 3.6 0.1152 0.45
Wits -5.7 2.61 -12 0 -0.036 0.7806
SnGoGn 32.43 5.8 17.9 44.9 0.3532 0.0173*
CoA 92 7.3 74 106 0.0413 0.7878
CoGn 127.4 10.06 104 151 0.0674 0.662
IMPA 83.37 6.47 64.2 94.2 0.0338 0.8257
1.PP 118.51 7.8 97.9 132.4 -0.282 0.0587
Frequency
Number of treatment phases 1 Phase 64% 2 Phase 36%
-0.102 0.5040
6WDWLVWLFDOVLJQL¿FDQFHSYDOXH
of appliance breakages ( r= 0.4195, p= 0.004) and m i ssed ap p o i n t m en t s ( r = 0 . 6 5 9 5 , p < 0 . 0 0 0 1 ) , t r eat m en t ch ar act er ist ics PAR at T1( r = 0 . 3 2 5 1 , p = 0 . 0 2 9 ) , PAR a t T2 ( r = 0 . 3 4 9 , p = 0 . 0 3 2 2 9 ) , and skelet al feat ures SNB ( r= - 0.3434, p= 0.02) , SnGoGn ( r= 0.3532, p= 0.017) w ere found t o have
VLJQL¿FDQWFRUUHODWLRQZLWKRUWKRGRQWLFWUHDWPHQW
durat ion ( Table 1) . These variables w ere included i n t h e m u l t i p l e r e g r e ssi o n m o d e l . Pa t i e n t ’s dem ographics, num ber of or t hodont ic t r eat m ent phases, overj et , num ber of m issing t eet h, num ber of t eet h ext ract ed, t reat m ent im provem ent ( PAR T1-T2) , and t he ot her cephalom et ric m easurem ent s SNA, ANB, Wit s, CoA, CoGn, I MPA and 1.PP had no associat ion w it h t reat m ent durat ion. Also, no differ ence was found bet w een m ale and fem ale concer ning t r eat m ent t im e ( p= 0.41) . Ther efor e, t hese variables w ere not included in t he m ult iple regression m odel.
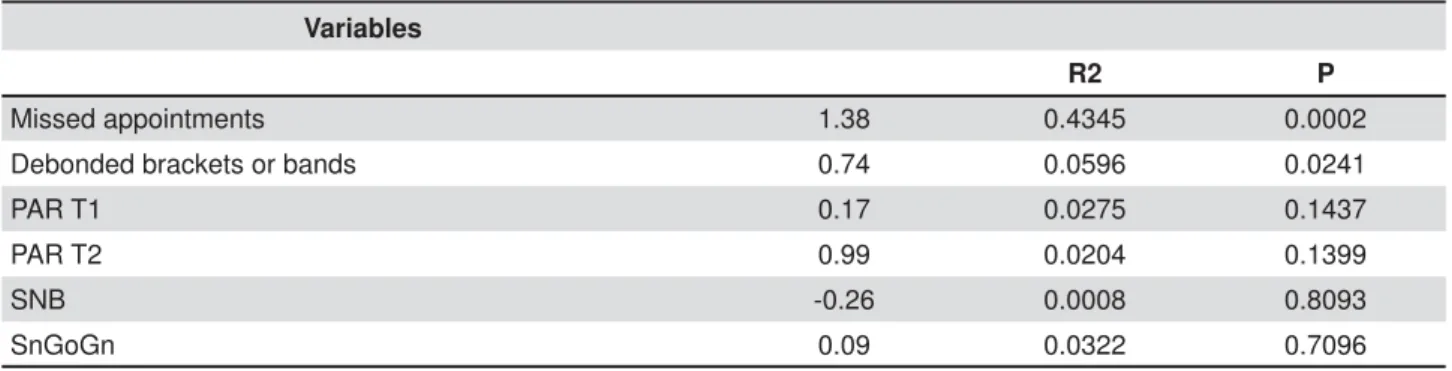
Result s aft er m ult iple regression linear t est and st epw ise r egr ession show ed t hat ar ound half of t reat m ent durat ion ( R2= 0.4944) could be predict ed
by t wo variables: m issed appoint m ent s ( R2= 0.4345,
p= 0.0002) , follow ed by t he num ber of debonded bracket s and bands ( R2= 0.0596, p= 0.0241) . The
cephalom et ric m easurem ent s SnGoGn ( R2= 0.0322)
and SNB angle ( R2= 0.0008) , and m alocclusion index
PAR at T1 (R2= 0.0275) and PAR at T 2 ( R
2= 0.0204) KDGVRPHLQÀXHQFHRYHUWUHDWPHQWGXUDWLRQWKRXJK QRWVWDWLVWLFDOO\VLJQL¿FDQW7DEOH(DFKPLVVHG
appoint m ent was found t o add about 1.5 m ont hs t o t he t reat m ent durat ion.
7KHUH ZDV D VWDWLVWLFDOO\ VLJQL¿FDQW GLIIHUHQFH
( p= 0.02) bet w een Group 0- 2 ( m ean= 27.01± 7.56 m on t h s) an d Gr ou p > 2 ( m ean = 3 6 . 1 5 ± 1 1 . 2 9 m ont hs) for t reat m ent durat ion. The PAR index at T2 GLG QRW VKRZ VWDWLVWLFDOO\ VLJQL¿FDQW GLIIHUHQFH ( p= 0.098) when pat ient s wit h fewer m issed clinical visit s w er e com par ed w it h t hose w ho had m or e m issed appoint m ent s.
DI SCUSSI ON
“ How long w ill m y t reat m ent last ?” is one of t he m ost com m on quest ions ask ed by pat ient s seeking for ort hodont ic t reat m ent . To answ er it , t he ort hodont ist should focus on w hich variables co u l d i n t er f er e w i t h t h e t r eat m en t p r o g r ess. Alt hough several st udies have invest igat ed fact ors associat ed w it h t reat m ent durat ion for Class I or Class I I m alocclusion pat ient s, t o t he best of our knowledge, j ust one st udy31 gives som e inform at ion
about durat ion of Class I I I m alocclusion t reat m ent .
7KLV SUHYLRXV VWXG\ RQO\ DQDO\]HV WKH LQÀXHQFH
of m olar Class I I I posit ion on t reat m ent durat ion
LQDVPDOOVDPSOH1RVLJQL¿FDQWDVVRFLDWLRQZLWK
t reat m ent durat ion was found. These dat a w ould be also indispensable for fut ure invest igat ions on t reat m ent t ypes and effect iveness of result s.
Pr ev iou s r epor t s ev alu at in g adu lt pat ien t s1 6
showed t hat t he am ount of m issed appoint m ent s is t he fact or t hat affect s t reat m ent durat ion ( 43.75% ) of Class I and Class I I pat ient s t he m ost . These
¿QGLQJVDUHVXSSRUWHGE\RXU¿QGLQJV
This is a valuable infor m at ion for or t hodont ist s, si n ce t h e p a t i en t a l so a ssu m es so m e o f t h e r esponsibilit y for t he t r eat m ent t im e and it can persuade t he pat ient int o having good com pliance.
Appliance breakages were weak, but st at ist ically associ at ed w i t h t r eat m en t t i m e i n t h i s st u d y ( R2= 0 . 0 5 9 6 ) , a s p r e v i o u s l y d e s c r i b e d6 , 1 6 , 2 0.
I ncr em ent s in t r eat m ent durat ion m ight be due t o t he necessit y of ret urning t o a light er arch w ire or t he im possibilit y of t reat m ent evolut ion in t hat m ont h.
2XU ¿QGLQJV LQGLFDWH WKDW SDWLHQW FRRSHUDWLRQ
appear s t o have a gr eat er effect on durat ion of ort hodont ic t reat m ent in Class I I I pat ient s. This m ig h t occu r sin ce it is k n ow n t h at m od er at e t o sev er e Class I I I m alocclu sion s can h av e a considerable im pact on pat ient ’s aest het ics and qualit y of life, keeping t hem m ore m ot ivat ed and easy t o handle. Clinically, t his m ot ivat ion should be increasingly ut ilized t oward a short er t reat m ent durat ion.
Variables
R2 P
Missed appointments 1.38 0.4345 0.0002
Debonded brackets or bands 0.74 0.0596 0.0241
PAR T1 0.17 0.0275 0.1437
PAR T2 0.99 0.0204 0.1399
SNB -0.26 0.0008 0.8093
SnGoGn 0.09 0.0322 0.7096
A p r e v i o u s s t u d y1 r e p o r t e d t h a t m i s s e d
ap p oin t m en t s an d ap p lian ce r ep air s ex p lain ed 30.6% of t reat m ent durat ion. A different st udy20 also
shows t hat t ot al bracket s or bands breakage affect s ort hodont ic t reat m ent durat ion in t eenage pat ient s;
KRZHYHUQRVLJQL¿FDQWLQÀXHQFHZDVIRXQGE\WKH
aut hors regarding m issed appoint m ent s. Maybe t his could be explained by t he fact t hat adolescent s are m ore likely t o accept parent cont rol; t herefore m ore assiduous t han older adolescent s or young adult s.
Fu r t h er m or e, in t er m ax illar y elast ics2 4 ar e qu it e
oft en required in Class I I I com pensat ory t reat m ent , dem anding good pat ient com pliance.
Peer Assessm en t Rat in g ( PAR) w as u sed t o quant ify t he sev er it y of t he m alocclusion giv en t hat it is a valid and reliable m et hod: t he higher t he index, t he great er t he am ount of m alocclusion of t he pat ient . PAR index at T1 and T2 show ed no
VLJQL¿FDQW DVVRFLDWLRQ S! ZLWK WUHDWPHQW
t im e. A possible explanat ion for t his is t he high PAR T1,ZKLFKUHÀHFWVSRRUSDWLHQWFRPSOLDQFH:KHQWKH requirem ent of cont inuously using elast ics is not m et , t he est ablishm ent of good occlusal relat ionship
LVDIIHFWHGLQÀXHQFLQJWKH¿QDO3$5LQGH[
No st at ist ical d if f er en ce w as f ou n d am on g pat ient s w ho m issed zero t o t w o appoint m ent s and pat ient s w ho m issed m ore t han t w o appoint m ent s
GXULQJWUHDWPHQWUHJDUGLQJWKH¿QDO3$5LQGH[7KH
fact t hat a longer t reat m ent t im e was necessary in Group > 2 t o obt ain an ort hodont ic out com e sim ilar t o t hat of group 0- 2 indicat es t hat obt aining good
RFFOXVDO¿QLVKLQJLQQRQFRPSOLDQWSDWLHQWVUHTXLUHV
longer t reat m ent t im e.
$JHKDGQRLQÀXHQFHRQWUHDWPHQWWLPHLQWKLV
st u dy at t h e begin n in g of Class I I I t r eat m en t , differ ing fr om pr evious invest igat ions exam ining Class I and Class I I m alocclusion6,20,30. Therefore,
ot her pret reat m ent or ext ernal fact ors, not included in t his st udy, m ight be t he reason w hy pat ient s are skipping appoint m ent s.
:KHQ FRPSDULQJ RQO\ ¿[HG WUHDWPHQWOHQJWK
t he lit erat ure show s no difference am ong pat ient s t reat ed for Class I I m alocclusion in one and t w o phases9 DV RXU ¿QGLQJV +RZHYHU WKLV GRHV QRW PHDQ WKDW WKH ¿UVW SKDVH RI WKH WUHDWPHQW LV
u n n ecessar y. Most Class I I I pat ien t s w h o seek for t reat m ent in a younger age have m ore severe m alocclusion14,258VXDOO\WKH¿UVWSKDVHLQFOXGHV
an ort hopedic expansion and m axillary prot ract ion. Con sequ en t ly, m ost of t h e t im e, secon d ph ase
LQYROYHVRQO\DFRPSHQVDWRU\WUHDWPHQWZLWK¿[HG
appliance.
'LIIHUHQWO\IURPRXU¿QGLQJVFRQFHUQLQJ&ODVV
I I I m alocclusion, som e report s on Class I I pat ient s d escr i b e an asso ci at i o n b et w een ov er j et an d t reat m ent durat ion12,20. I nit ial posit ioning of upper
and lower ant erior t eet h and m andibular growt h are not favorable t o non- surgical Class I I I t reat m ent13,28.
Frequent ly, t he upper incisors show com pensat ory prot rusion while t he lowers have lingual inclinat ions, lim it ing t he am ount of negat ive overj et t hat can be t reat ed w it hout surgery. Nevert heless, Class I I division 1 pat ient s have proclined upper incisors25,
w hich is favorable for com pensat ory t reat m ent . Anot her fact or regarding Class I I I t reat m ent is t hat severe ant erior crossbit e is oft en relat ed w it h su bst an t ial an d ev iden t sk elet al discr epan cies, r eq u i r i n g su r g i cal t r eat m en t3, u n l i k e Cl ass I I
pat ient s, w hich skelet al discr epancies ar e m or e “ aest het ically accept able”1,5 and can be t reat ed in
a com pensat ory m anner.
Tr eat m ent inv olv ing ex t ract ions and m issing
WHHWKEHIRUHWUHDWPHQWKDGQRVWDWLVWLFDOO\VLJQL¿FDQW LQÀXHQFHRQWUHDWPHQWGXUDWLRQ. Space closure can
be a t im e- consum ing t reat m ent phase23; how ever, H[WUDFWLRQVFDQLQFUHDVHWUHDWPHQWHI¿FLHQF\ZKHQ
t hey are correct ly indicat ed.
This st udy had som e m et hodological lim it at ions, such as using a ret rospect ively select ed unicent er sam ple. How ev er, it is a con secu t iv ely t r eat ed sam ple, w hich decreases t he risk of bias. Anot her lim it at ion of ou r st u d y is t h e n on - in clu sion of su r gical p at ien t s in t h e sam ple, leav in g ou t a large num ber of Class I I I cases available in t he
RI¿FH¿OHV(YDOXDWLQJWKLVYDULDEOHLWZRXOGKDYH
been im port ant t o verify t he im pact of conduct ing surgical t reat m ent on t reat m ent durat ion in Class I I I pat ient s.
Failure t o m eet t he est im at ed t reat m ent t im e frequent ly dam ages t he doct or- pat ient relat ionship b y d ecr easin g t h e p at ien t ’s t r u st . Biolog ically, el o n g at ed t r eat m en t t i m e h av e b een r el at ed t o in cr eased pr obabilit y of r oot r esor pt ion1 7 , 2 2.
Therefore, t he awareness of t he fact ors cont ribut ing t o t reat m ent overt im e can help ort hodont ist s t o cont r ol som e of t hese var iables and per for m a
PRUHHI¿FLHQWWUHDWPHQWIRU&ODVV,,,PDORFFOXVLRQ
hav ing sm oot her r elat ionship w it h pat ient s and
JUHDWHU SUDFWLFH VXFFHVV 2XU ¿QGLQJV VKRZHG
t hat durat ion of ort hodont ic t reat m ent in Class I I I
GHQWDOPDORFFOXVLRQSDWLHQWVLVPDLQO\LQÀXHQFHGE\
pat ient com pliance. Thus, it seem s crucial t o inform pat ient s about t heir role in t he t reat m ent progress
DQGSURYLGHVFLHQWL¿FDOO\VRXQGGDWDWRVWLPXODWH
pat ient ’s cooperat ion.
CON CLUSI ON
No variable obt ained before t reat m ent was able t o give som e predict ion about t reat m ent t im e in t his sam ple of Class I I I pat ient s.
Ot h er v ar iables, su ch as su r ger y n eed, n ot included in t his st udy, should be invest igat ed.
REFEREN CES
$EX $UTRXE 6+ $O.KDWHHE 61 3HUFHSWLRQ RI IDFLDO SUR¿OH
a t t r a ct i v e n e ss o f d i f f e r e n t a n t e r o - p o st e r i o r a n d v e r t i ca l proport ions. Eur J Ort hod. 2011; 33: 103- 11.
2- Alger DW. Appoint m ent versus t reat m ent t im e. Am J Ort hod Dent ofacial Ort hop. 1988; 94: 436- 9.
3- Auconi P, Scazzocchio M, Cozza P, McNam ara JA Jr, Franchi L. Predict ion of Class I I I t reat m ent out com es t hrough ort hodont ic dat a m ining. Eur J Ort hod. 2015; 37: 257- 67.
4- Baccet t i T, Franchi L, McNam ara JA Jr. Grow t h in t he unt reat ed Class I I I subj ect . Sem in Ort hod. 2007: 13: 130- 42.
5- Barroso MC, Silva NC, Quint ão CC, Norm ando D. The abilit y of ort hodont ist and laypeople t o discrim inat e st epwise advancem ent s in Class I I ret rognat hic m andible. Prog Ort hod. 2012; 13: 141- 7. 6- Beckw it h FR, Ackerm an RJ Jr, Cobb CM, Tira DE. An evaluat ion of fact ors affect ing durat ion of ort hodont ic t reat m ent . Am J Ort hod Dent ofacial Ort hop. 1999; 115: 439- 47.
%HUQDEp(6KHLKDP$2OLYHLUD&0&RQGLWLRQVSHFL¿FLPSDFWV
on qualit y of life at t ribut ed t o m alocclusion by adolescent s w it h nor m al occlusion and Class I , I I and I I I m alocclusion. Angle Ort hod. 2008; 78: 977- 82.
8- Bondem ar k L, Holm AK, Hansen K, Axelsson S, Mohlin B, Brat t st rom V, et al. Long- t erm st abilit y of ort hodont ic t reat m ent and pat ient sat isfact ion. A sy st em at ic r ev iew. Angle Or t hod. 2007; 77: 181- 91.
9 - Dim b er g L, Len n ar t sson B, Söd er f eld t B, Bon d em ar k L. Malocclusions in children at 3 and 7 years of age: a longit udinal st udy. Eur J Ort hod. 2013; 35: 131- 7.
10- Dyer GS, Har r is EF, Vaden JL. Age effect s on or t hodont ic t r eat m ent : adolescent s cont rast ed w it h adult s. Am J Or t hod Dent ofacial Ort hop. 1991; 100: 523- 30.
11- Fink DF, Sm it h RJ. The durat ion of ort hodont ic t reat m ent . Am J Ort hod Dent ofacial Ort hop. 1992; 102: 45- 51.
12- Fisher MA, Wenger RM, Hans MG. Pret reat m ent charact erist ics associat ed w it h or t hodont ic t r eat m ent durat ion. Am J Or t hod Dent ofacial Ort hop. 2010; 137: 178- 86.
13- Janson G, Souza JE, Alves FA, Andrade P Jr, Nakam ura A, Fr eit as MR, et al. Ext r em e dent oalveolar com pensat ion in t he t r eat m ent of Class I I I m alocclusion. Am J Or t hod Dent ofacial Ort hop. 2005; 128: 787- 94.
14- Jerem iah HG, Cousley RR, New t on T, Abela S. Treat m ent t im e ad oclusal out com e of ort hognat hic t herapy in t he east of England region. J Ort hod. 2012; 39: 206- 11.
15- Mavr eas D, At hanasiou AE. Fact or s affect ing t he durat ion of or t hodont ic t r eat m ent : a sy st em at ic r ev iew. Eur J Or t hod. 2008; 30: 386- 95.
1 6 - Melo AC, Car n eir o LO, Pon t es LF, Cecim RL, Mat t os JN, Norm ando D. Fact ors relat ed t o ort hodont ic t reat m ent t im e in adult pat ient s. Dent al Press J Ort hod. 2013; 18: 59- 63
17- Nanek r ungsan K, Pat anapor n V, Janhom A, Kor wanich N. Ext ernal apical root resorpt ion in m axillary incisors in ort hodont ic pat ient s: associat ed fact ors and radiographic evaluat ion. I m aging Sci Dent . 2012; 42: 147- 54.
1RUPDQGR 76 %DUURVR 5) 1RUPDQGR ' ,QÀXHQFH RI WKH
socioeconom ic st at us on t he prevalence of m alocclusion in t he prim ary dent it ion. Dent al Press J Ort hod. 2015; 20: 74- 8. 19- O’Connor PJ. Pat ient s’ percept ions before, during and aft er ort hodont ic t reat m ent . J Clin Ort hod. 2000; 34: 591- 2.
20- Popow ich K, Nebbe B, Heo G, Glover KE, Maj or PW. Predict ors for Class I I t reat m ent durat ion. Am J Ort hod Dent ofacial Ort hop. 2005; 127: 293- 300.
3URI¿W:5)LHOGV+:-U0RUD\/-3UHYDOHQFHRIPDORFFOXVLRQ
and ort hodont ic t reat m ent need in t he Unit ed St at es: est im at es from t he NHANES I I I survey. I nt J Adult Ort hod Ort hognat h Surg. 1998; 13: 97- 106.
2 2 - Rak h sh an V, Nat eg h ian N, Or d ou b azar i M. Risk f act or s associat ed w it h ext ernal apical root resorpt ion of t he m axillary i n ci so r s: a 1 5 - y e a r r e t r o sp e ct i v e st u d y. Au st Or t h o d J. 2012; 28: 51- 6.
23- Richm ond S, Shaw WC, O’Brien KD, Buchanan I B, Jones R, St ephens CD, et al. The developm ent of t he PAR index ( Peer Assessm en t Rat in g ) : r eliab ilit y an d v alid it y. Eu r J Or t h od . 1992; 14: 125- 39.
2 4 - Say in MO, Tür k k ahram an H. Cephalom et r ic evaluat ion of non- grow ing fem ales w it h skelet al and dent al Class I I , division 1 m alocclusion. Angle Ort hod. 2005; 75: 656- 60.
25- Shelt on CE Jr, Cisneros GJ, Nelson SE, Wat kins P. Decreased t r eat m en t t im e d u e t o ch an g es in t ech n iq u e an d p r act ice philosophy. Am J Ort hod Dent ofacial Ort hop. 1994; 106: 654- 7. 26- Shia GJ. Treat m ent overruns. J Clin Ort od. 1986; 20: 602- 4. 27- Skidm ore KJ, Brook KJ, Thom son WM, Harding WJ. Fact ors
LQÀXHQFLQJWUHDWPHQWWLPHLQRUWKRGRQWLFSDWLHQWV$P-2UWKRG
Dent ofacial Ort hop. 2006; 129: 230- 8.
28- Troy BA, Shanker S, Fields HW, Vig K, Johnst on W. Com parison of incisor inclinat ion in pat ient s wit h Class I I I m alocclusion t reat ed
ZLWKRUWKRJQDWKLFVXUJHU\RURUWKRGRQWLFFDPRXÀDJH$P-2UWKRG
Dent ofacial Ort hop. 2009; 135: 146.e1- 9.
7XOORFK -) 3URI¿W :5 3KLOOLSV & 2XWFRPHV LQ D SKDVH
random ized clinical t rial of early Class I I t reat m ent . Am J Ort hod Dent ofacial Ort hop. 2004; 125: 657- 67.
3 0 - Tu r b ill EA, Rich m on d S, Wr ig h t JL. Th e t im e f act or in
RUWKRGRQWLFV ZKDW LQÀXHQFHV WKH GXUDWLRQ RI WUHDWPHQWV LQ
nat ional healt h service pract ices? Com m unit y Dent Oral Epidem iol. 2001; 29: 62- 72.
9X &4 5REHUWV ( +DUWV¿HOG -. -U 2IQHU 6 7UHDWPHQW