REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Simple
method
for
determining
the
size
of
the
ProSeal
laryngeal
mask
airway
in
children:
a
prospective
observational
study
Murat
Haliloglu
∗,
Sevgi
Bilgen,
Neslihan
Uzture,
Ozge
Koner
YeditepeUniversitySchoolofMedicine,DepartmentofAnesthesiologyandReanimation,Istanbul,Turkey
Received21May2015;accepted22June2015 Availableonline19March2016
KEYWORDS
Child; Earauricle; ProSeallaryngeal maskairway
Abstract
Backgroundandobjectives: ThesizeoftheProSeallaryngealmaskairwayinchildrenis deter-mined by thepatient’s weight.However, insome instances, analternativemethodmay be required.ThisstudyaimedtocomparesizingbytheauriclewithconventionalProSeallaryngeal maskairwaysizingbyweightinchildren.
Methods:Afterapprovalbytheinstitutionalethicsboardandwritteninformedconsentfrom parents,197childrenwithAmericanSocietyofAnesthesiologistsphysicalstatusI---IIwhowere scheduledforaroutinegenitourinaryoperationwereincludedinthestudy.ThecorrectProSeal laryngeal maskairwaysizewas determinedaccordingtothesizeoftheauricle inchildren. Theresultswerecomparedwiththestandardweight-basedmethodrecommendedbythe man-ufacturer’s guidelines. The patients were classified into different groups depending onthe ProSeallaryngealmaskairwaysizesasdeterminedbybothmethods.Agreementbetweenboth techniqueswasevaluatedwithcoefficientstatistics.
Results:Insertionandadequateventilationwereachievedin185patientsatthefirstattempt, and12patients requiredasecondattempt.Threepatientshadtobeintubated.Agreement betweenthetwomethodsofsizeselectionoftheProSeallaryngealmaskairwaywasmoderate usingstatistics.
Conclusions: ChoosingthesizeoftheProSeallaryngealmaskairwayinchildrenaccordingto theauricle ofthechildisvalidandpractical.Inparticular,thisisanalternativemethod in situationswherethepatient’sweightisunknown,suchasinemergencysituations.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](M.Haliloglu).
http://dx.doi.org/10.1016/j.bjane.2015.06.004
otamanhodaorelhaemcrianc¸as.Osresultadosforamcomparadoscomosdométodopadrão, baseadonopeso,recomendadopelasdiretrizesdofabricante.Ospacientesforamclassificados emdiferentesgrupos,dependendodostamanhosdasMLPSconformedeterminadoporambosos métodos.Aconcordânciaentreasduastécnicasfoiavaliadacomasestatísticasdocoeficiente kappa(k).
Resultados: Inserc¸ãoeventilac¸ãoadequadaforamobtidasem185pacientesnaprimeira ten-tativa,e12 pacientesprecisaramde umasegundatentativa. Trêspacientesprecisaramser intubados.Aconcordânciaentreosdoismétodosdeselec¸ãodotamanhodaMLPSfoimoderada usandoaestatística.
Conclusões:AescolhadotamanhodaMLPSemcrianc¸asdeacordocomaorelhadacrianc¸aé válidaeprática.Emparticular,esseéummétodoalternativoemsituac¸õesnasquaisopesodo pacienteédesconhecido,comoemsituac¸õesdeemergência.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The ProSeal laryngeal mask airway (PLMA) has been
fre-quently used for airway management not only in the
operatingroom,butalsointheprehospitalandemergency
caresetting.1,2ThePLMAwasdevelopedbyDr.ArchieBrain
in2000.3The PLMAhastwolumensseparatingthe
alimen-tary and respiratory channels from each other, forminga
more effective seal than the LMA-Classic. This
supraglot-tic airway device has gained popularity in the pediatric
population. Selection of theoptimal size is important for
safeandeffectiveuseofthePLMA.Inchildren,the
manu-facturerrecommends thatthesize ofthePLMAshouldbe
basedonweight.4 The weight-relatedtechnique,which is
thegoldstandardmethod,isnotalwaysapplicable.In
emer-gencyservices,thepatient’sweightissometimesunknown
oremergencyprovidershavesomedifficultiesrecallingthe
relationship between weight and size. In addition,
over-weightandunderweightchildrenmaybeexcludedfromthe
rangedefinedbytheweight-basedtable.5
In the following observational study,we evaluatedthe
suitability of the previously described, auricle size-based
method of PLMA selection for children in the Turkish
population.6 The primarygoal of our study wasto
deter-minewhethertheauriclesize-basedPLMAselectionmethod
isinagreementwiththeweight-basedformulaforpediatric
patients.Oursecondarygoalwastoachieveasuccessrateof
insertionofthePLMAofgreaterthan90%withtheauricle
size-basedtechniqueatthe firstattempt.Tovalidatethis
procedure,the size ofthe PLMAas determinedaccording
totheauricle-basedandage-basedformulawascompared
withthemanufacturer’sweight-basedformula.
Methods
ThisstudywasconductedwithIRBapprovalandwas
regis-teredwiththewww.clinicaltrials.govprotocol registration
system (NCT02257411).After obtaining approval fromthe
EthicsCommitteeof ourhospital(no346:18.06.2013) and
writtenparentalinformedconsent,thestudywasconducted
according tothe Declaration of Helsinki. This prospective
studywasperformedin197patientsoveraperiodof1year.
Childrenwith AmericanSociety of Anesthesiologists (ASA)
physicalstatusI---II,whowerescheduledforagenitourinary
operation,andin whomaPLMAwasindicatedfor general
anesthesia, wereeligibletoparticipatein thestudy.
Chil-drenandtheirparentswereseen1daybeforetheplanned
operationintheanesthesiapre-assessmentclinic.Exclusion
criteriaincludedanexpecteddurationofsurgerymorethan
3h,patientswhowereoutsidetherangeofthe15thto85th
growthpercentilesforweightand/orheightinchildrenup
to15yearsofage,gastro-esophagealreflux,ariskof aspira-tion,anairwayinfectioninthelast6weeks,orthepresence
ofdecreasedpulmonaryorchestwallcompliance.
Patientsfastedfor at least 6---8h for solids and2h for
clear fluids. According to the hospital protocol of
pre-medication,oralMidazolam0.5mg·kg−1wasprovided30min
beforeinductiontoallchildren.The childrenwereplaced
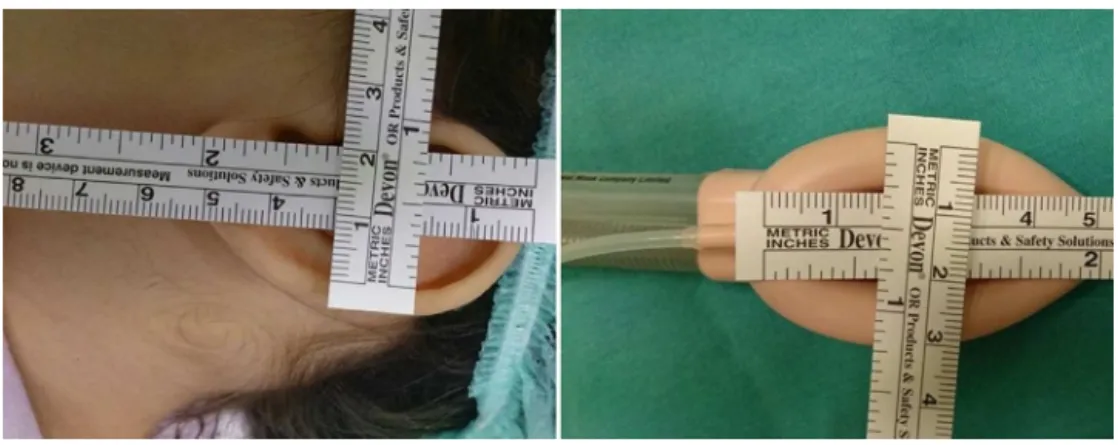
Figure1 SizeofthePLMA.
pillow to achieve an optimal position. Routine
monitor-ingwas performed, includingan electrocardiogram,pulse
oximeter,gasanalyser,non-invasivearterialpressure moni-tor,tidalvolumemonitor,andairwaypressuremonitor.After
four breaths of oxygen in 60% nitrous oxide,the
vaporiz-ers were set at 7% for sevoflurane. Facemaskventilation
wasperformed untilconditionsweresuitablefor insertion
of the laryngeal mask (loss of eyelash reflex, jaw
relax-ation, absence of movement). Muscle relaxants were not
used in the patients. As part of the pilot study,the size
of the auricle was measured with a ruler in the vertical
and horizontaldimensions in thefirst 20 participants and
theclosestcorrespondingsizeofthePLMAwaschosenfor
insertion (Fig. 1). Following the pilot study, selection of
thePLMAwasperformedbasedonvisualobservationrather
thanmeasurement(Fig.2).Iftheauriclefellbetweentwo
sizesof PLMA,theweight-based sizewaspreferred.Allof
thePLMAswereinsertedbytwoexperienced
anesthesiolo-gists,accordingtothemanufacturer’sinstructionswiththe
cuff fully deflated using the digital technique. Following
insertionof thePLMA,thedeviceswere inflateduntil the
cuffpressurereached60cmH2O,andtheywereconnected
tothebreathingcircuit.Fixationwasperformedaccording
tothemanufacturer’sinstructions.7Thevolume-controlled
mode with tidal volume at 8mL/kg was applied to the
patients.Respiratoryrateswereadjustedbyestablishingthe
inspiratory/expiratoryratioat1:2andtheend-tidalcarbon
dioxide at 30---35mmHg.Anesthesia wasmaintained using
sevoflurane in 66% nitrousoxide at 1.3 minimumalveolar
concentrations.Informationonthepatients’characteristics
wasobtainedaftertheoperationtoavoidbiaswhen
choos-ingthesizeofthePLMA.Foreachpatient,thesizechosen
withourmethod wascomparedwiththe sizedetermined
by the patient’s weight,according to the manufacturer’s
guidelines.
Initialassessmentofventilationwasperformedby
obser-vationofsquarewavetracingoncapnographyand
thoraco-abdominalmovement. In case of failure of insertion, the
PLMAwasremoved andtheweight-based suitablesizefor
childrenwasinserted.Theinsertiontimewasdefinedasthe
timebetweenremovalofthefacemaskandobservationof
thefirstend-tidalcarbondioxidewaveafterinsertionofthe PLMAintothemouth.Ifinsertioncouldnotbeachievedafter twoattemptsorifmechanicalventilationfailed(i.e.,high
peakairway pressure, high gas leakage, and an improper
airwaypressuretrace),itwasregardedasafailureandthe
childwasexcludedfromthestudy.Oropharyngealleak
pres-surewasdeterminedbyclosingtheexpiratoryvalveofthe
circuitwhen anaudiblenoisewasheard overthemouth.8
Becauseofsafetyconcerns;themaximalacceptable
oropha-ryngealleakpressurewas40cmH2O.Thecuffpressurewas
standardizedat60cmH2Oinallofthepatients.
The PLMA was removed at the end of surgery after
thechild returnedto an appropriatespontaneous
breath-ing pattern and was fully awake. Side effects (stridor,
laryngospasm,bronchospasm, orblood onthePLMA)were
recordedduringmaintenanceandrecoveryfromanesthesia.
Aftercompletion of thesurgery, the weight-based and
auricle-based PLMA selection techniques were compared
withthePLMAselectionaccordingtoage.
http://graphpad.com/quickcalcs/kappa2).SPSS(Statistical
Package for Social Sciences) for Windows 15.0 software
(SPSS,Chicago,IL)wasusedforstatisticalanalysis.
Results
Thepatients’demographiccharacteristicsandsurgicaland
anestheticpropertiesareshowninTable1.Themeantimeof
insertionofthePLMA,thenumberofinsertionattemptsand
successtoadequate ventilationarealsoshowninTable1.
Inthreeofthepatients,attemptsatinsertionofthePLMA
failedandthepatientshadtobeintubated.
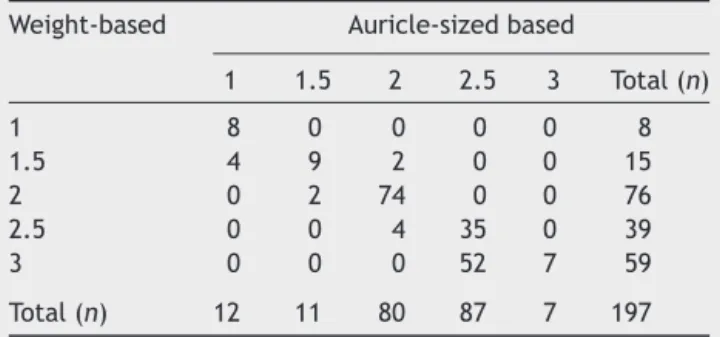
Tables2and3showsacomparisonofthetwomethodsof
sizeselectionforthePLMA(weight-basedandauricle
size-based).InTable2,patientsweighing30kgwereincludedin thesizeofthe2.5PLMAgroup.InTable3,patientsweighing 30kgwereincludedinthesizeofthe3PLMAgroup.
Seventy-threepercentofthe patientsin Table2 and67.5% ofthe
patients in Table 3were found tobe in the rangeof the
recommendedweightbasedsize.
Agreementbetween the twomethods ofsize selection
of the PLMA (weight-based and auricle size-based) when
30kgpatientswereincludedinthe2.5sizePLMAgroupwas
goodusingstatistics(=0.62;SE=0.039,95%confidence
Table 1 Demographic data and surgical and anesthetic
properties.
Age(years) 4.7±2.9
Sex(female/male) 84(42.6%)/113(57.4%)
Weight(kg) 20.3±9.8
Height(cm) 106.8±22.5
ASAI/II 180(91.4%)/17(8.6%)
InsertiontimeofPLMA(s) 15±1.6
Durationofanesthesia (min)
70.5±14.7
Successrateplacement
Atthefirstattempt 185(93.9%)
Atthesecondattempt 12(6.1%)
Oropharyngealleak pressure;cmH2O
28.6±1.4
Peakinspiratorypressure; cmH2O
13.8±1.9
Complications
Bloodtingedequipment 7(3.6%)
Dataareshownasmean±standarddeviationornumber(%). PLMA,ProSeallaryngealmaskairway.
Total(n) 12 11 80 87 7 197
Dataareshownasnumber(n)ofpatients.
Table3 PLMAsizeaccording toweightandauricle
size-basedtechniques(30kgpatientswereincludedinthe3size PLMAgroup).
Weight-based Auricle-sizedbased
1 1.5 2 2.5 3 Total(n)
1 8 0 0 0 0 8
1.5 4 9 2 0 0 15
2 0 2 74 0 0 76
2.5 0 0 4 35 0 39
3 0 0 0 52 7 59
Total(n) 12 11 80 87 7 197
Dataarepresentedasnumber(n)ofpatients.
interval [CI]=0.54---0.70). The strengthwith theweighted
-testwas0.74,whichshowedgoodstrengthofagreement
between the two methods. Agreement between the two methodsofsizeselectionofthePLMAwhen30kgpatients were included in the 3 size PLMA group was moderate using statistics ( =0.56; SE=0.039, 95%CI=0.48---0.63). The strength of agreement withthe weighted kappatest was0.70, which alsoshowed goodstrength of agreement betweenthetwomethods.Theauriclesize-basedPLMAsize of 2.5 corresponded toaPLMA sizeof 3 according tothe weight-basedchart(Tables2and3).
Table4shows comparisonof theauricle-based method
size selection of the PLMA with age groups. Agreement
between thetwomethodsof sizeselection wasmoderate
Table4 PLMAsizesbasedonauriclesizeandage.
Age-based Auriclesize-based
1 1.5 2 2.5 3 Total(n)
<6months 12 0 0 0 0 12
6m---1.5yr 0 10 5 0 0 15
2---3yr 0 1 75 0 0 76
4---6yr 0 0 0 22 0 22
7yr 0 0 0 38 3 41
≥8yr 0 0 0 27 4 31
Total(n) 12 15 75 87 7 197
using statistics( =0.53;SE=0.039,95% CI=0.45---0.60). Thestrengthofagreementwiththeweightedkappatestwas 0.74, whichshowed goodstrength of agreementbetween thetwomethods.
Blood was identified on the PLMA after removal in sevenpatientsinthepostoperativeperiod.However,other complications, such as loss of airway, stridor, and laryn-gospasm,werenotdetected.
Discussion
The auricle size-based PLMA selection method showed a good correlation with the body weight-based selection methodin pediatric patients. Auricle size-basedselection resultedinasuccessrateofinsertionofthePLMAgreater than90%atthefirstattempt.
When the patients were classified according to age groups, auricle size-based PLMAselection appeared tobe more consistent than the weight-based chart, especially in children whowere 7 years of age. The PLMA size of 3 appearedtofitchildren≥8yearsoldthebestaccordingto ourauricle-size based method,whereas theweight-based methodproposedhalfasizelargerofPLMA.However, mak-inganassumptionaboutthesuccessofweight-basedPLMA selectioninpatientsolderthan7yearsisdifficult.Because theearsizedependsonageratherthanbodysize,prediction ofthePLMAsizebasedonageappearstobemoresuitable. Supraglottic airway devices, especially the laryngeal maskairway(LMA),haveincreasinglyreplacedendotracheal intubationnotjustintheoperatingroom,butalsoin prehos-pitalandemergencycaresettings.9Becauseofanatomical
differences,LMAusemayresultindifficultinsertion,airway
obstruction,increasedventilatorpressure,and
oropharyn-gealleakinchildren.10,11Inthesecases,choosingthe
appro-priatesizeisimportantforsuccessfulinsertionandadequate
ventilation.Selectionofaninappropriately-sizedPLMAhas
been suggested asthe reason of malposition of laryngeal
masks.12,13 Selection of the appropriate size of PLMA in
childrenisnotevidence-based,andisderivedfrom
recom-mendationsoftheLMAmanufacturer.Themanufacturer
rec-ommendsthattheselectionofsizebebasedonweight.4,14
Voyagisetal. showedthatheightshould beconsideredin
selectingthesizeoftheLMA.15Anotherstudyshowedthat
usingasize2.5LMA(‘‘up-sizing’’)providedabetterfitthan size2inchildrenweighing10---20kg.16Size1.5PLMAcanbe
usedinolderchildrenweighingmorethan10kg.17
Because development of the oropharyngeal cavity and
tissues surrounding the upper airway is linearly related
to age and height independently of sex or weight of a
child, pure weight-based methods may not be the most
suitable.14Inaddition,overweightandunderweightchildren
may be excluded from the range defined by the
weight-basedtable.18 Inemergencysituations,thetrueweightof
the patientis unknown and cannotbe easily determined.
In these cases, the patient’s weight may be incorrectly
estimated,19 which could cause an inappropriate size of
PLMAtobeselected.Sometimesinthesesituations,
medi-calstaffcannotremembertherelationshipbetweenweight
andsize.
Oropharyngealleakpressureindicatesthedegreeof
air-wayprotection,thefeasibilityforpositiveventilation,and
thelikelihoodforsuccessfulplacementofaPLMA.8To
pre-vent gas leakage and aspiration of pharyngeal secretion,
oropharyngealleakpressuremayneedtoexceedthe
pres-sure of fluid at the posterior pharyngeal wall, which is
approximatelyup to10cmH2O.20 Similarto ourfindings,
Goldmannetal.foundthatoropharyngealleakpressurewith
thePLMAwas28.60±1.36cmH2O.21
In our study, the insertion time was comparable with
thatreportedpreviously.15 Insertionof thePLMAand
ven-tilationofthelungswerecompletelyunsuccessfulinthree
patients who showed anatomical positioning of grade 4.
Thesepatients hadtobeintubated. The anatomical
posi-tion was assessed by fiberoptic broncoscopy and graded:
1=vocal cords (visual obstruction of epiglottis to
lar-ynx<50%);2=arytenoidsorposteriorpartofthelaryngeal inlet;3=epiglottis(visual obstruction of epiglottis to lar-ynx>50%);and4=noglottalview;orviewofepiglottis.22
Similartoourfindings,Goldmannetal.showedthatthe
successrateofinsertionatthefirstattemptwas87%.Our
studyshowedthattheproposedauricle-basedsizingmethod
waseffectivein determiningtheappropriatesizeofPLMA
inchildren.
Inourstudy,wealsoincludedpatientswhowerelessthan
6monthsof age,differentfromthestudydone byZahoor
etal.whichisoneofthelimitationsoftheirstudy.6Another
differencewithZahoor’sstudyisthatweperformedtwo
dif-ferentevaluationstodeterminethedifferenceswhen30kg
patientswerecategorizedtoeitherthe2.5or3sizePLMA
groups.Furthermore,wealsoexaminedwhetherdifferent
agegroupscorrelatedwellwithweight-orauriclesize-based
PLMAselection.Anotherstudyusedthewidthoftheindex,
middle,andringfingersofthepatientstodeterminethesize oftheLMA.23Inthatpreviousstudy,themeanbodyweightof
thepatientsinthelaryngealmask3groupwas44±11.4kg.
The standard deviation in the data of these patients was
high.Thiswiderangeofbodyweightwithinthesamegroup
mayhavedistortedevaluationofthedata.
AllofthePLMAswereinsertedbyexperienced
anesthe-siologists,andourdatamaynotbeapplicabletothosewith
lessexperience.Thisisalimitationofourstudy.Future
stud-iesneed to determine the viability of the earsize based
PLMAselectionforchildrenwhoareoverweightandwhether
theuseofthismethodisadequateforadults.
Summary
We conclude that the proposed auricle-based method for
determiningtheappropriatesizeofthePLMAisuseful
com-paredwiththemanufacturer’sweight-basedformula.Inthis
case,theauricle-basedsizedeterminationmethodcanbe
appliedinclinicalpracticeasanalternativemethodtothe
weight-basedformula.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
WethankEmiMaedawhoprovidedmedicalwritingservices
waysizeforoverweightandunderweightchildren.Anaesthesia. 2010;65:50---3.
6.ZahoorA,AhmadN,SerecheG,etal.Anovelmethodfor laryn-geal maskairway size selectioninpaediatricpatients. EurJ Anaesthesiol.2012;29:386---90.
7.LMAProsealTMInstructionManual.1sted.SanDiego,CA,USA; 2000.
8.KellerC,Brimacombe JR,KellerK,etal.Comparisonoffour methodsforassessingairwaysealingpressurewiththelaryngeal maskairwayinadultpatients.BrJAnaesth.1999;82:286---7.
9.Jolliffe L, Jackson I. Airway management in the outpatient setting:newdevicesandtechniques.CurrOpinAnaesthesiol. 2008;21:719---22.
10.ParkC,BahkJH,AhnWS,etal.Thelaryngealmaskairwayin infantsandchildren.CanJAnaesth.2001;48:413---7.
11.MasonDG,BinghamRM.Thelaryngealmaskairwayinchildren. Anaesthesia.1990;45:760---3.
12.CookTM,LeeG,NolanJP.TheProSeallaryngealmaskairway: areviewoftheliterature.CanJAnaesth.2005;52:739---60.
algorithm.Anesthesiology.1996;84:686---99.
18.Johnston DF, Wrigley SR, Robb PJ, et al. The laryngeal maskairwayinpaediatricanaesthesia.Anaesthesia.1990;45: 924---7.
19.GreigA,RyanJ,GlucksmanE.Howgoodaredoctorsat estimat-ingchildren’sweight?JAccidEmergMed.1997;14:101---3.
20.BrimacombeJ,BerryA, BrainAI.Optimalintracuffpressures withthelaryngealmask.BrJAnaesth.1996;77:295---6.
21.Goldmann K, Roettger C, Wulf H. The size 1(1/2) ProSeal laryngealmaskairwayininfants:arandomized,crossover inves-tigationwiththeClassiclaryngealmaskairway.AnesthAnalg. 2006;102:405---10.
22.CookTM,McKinstryC,Hardy R,etal. Randomizedcrossover comparisonoftheProSeallaryngealmaskairwaywiththe Laryn-gealTubeduringanaesthesiawithcontrolledventilation.BrJ Anaesth.2003;91:678---83.