Determination of alpha 1-antitrypsin levels and of the presence of S and Z
alleles in a population of patients with chronic respiratory symptoms*
Avaliação da concentração de alfa 1-antitripsina e da presença dos alelos S e Z em uma população de indivíduos sintomáticos respiratórios crônicos
Heliane Guerra Serra1, Carmen Sílvia Bertuzzo2, Mônica Corso Pereira3,
Cláudio Lúcio Rossi4, Walter Pinto Júnior5, Ilma Aparecida Paschoal6
Abstract
Objective: To determine the levels of alpha-1 antitrypsin (AAT) and the presence of S and Z alleles in patients with chronic respiratory
symp-toms. Methods: Patients with chronic cough and dyspnea were submitted to clinical evaluation, pulmonary function tests, high-resolution computed tomography, nephelometric determination of AAT and determination of S and Z alleles by polymerase chain reaction. Smoking and AAT levels were considered the dependent variables. Results: Of the 89 patients included in the study, 44 were female. The mean age was 51.3 ± 18.2 years. The S and Z alleles were detected in 33.3% and 5.7%, respectively, and the gene frequency was 0.16 and 0.028, respec-tively. Two patients were SZ heterozygotes (AAT levels ≤ 89 mg/dL). The patients were divided into groups based on AAT level: ≤ 89 mg/ dL (deficiency, no group); 90-140 mg/dL (intermediate, Group 1, n = 30); and ≥ 141 mg/dL (normal, Group 2, n = 57). The frequency of smokers was the same in both groups, although tobacco intake was greater in Group 2. The S allele was present in 13 and 14 patients in Groups 1 and 2, respectively, whereas the Z allele was present in 2 and 1 patient in the same groups. There was no difference in the results of pulmonary function tests or in the frequency of bronchiectasis or emphysema between the two groups. Spirometric values and AAT levels were similar in smokers and nonsmokers. Bronchiectasis was more common in nonsmokers, and emphysema was more common in smokers.
Conclusions: Thirty patients presented AAT levels lower than the mean values found in patients with the MM or MS genotype, and this fact
could not be explained by an increased frequency of S and Z alleles.
Keywords: Alpha 1-antitrypsin; Emphysema: Lung diseases; Alleles.
Resumo
Objetivo: Determinar a concentração de alfa 1-antitripsina (AAT) e a prevalência dos alelos S e Z em indivíduos sintomáticos respiratórios
crônicos. Métodos: Pacientes com tosse crônica e dispnéia foram submetidos à avaliação clínica, espirometria, tomografia computadorizada de tórax, dosagem de AAT por nefelometria e pesquisa das mutações S e Z por reação em cadeia da polimerase. Foram consideradas como variáveis dependentes a concentração de AAT e o tabagismo. Resultados: Dos 89 pacientes incluídos no estudo (44 mulheres; idade média, 51,3 ± 18,2 anos), os alelos S e Z foram detectados em 33,3% e 5,7%, respectivamente, com freqüência gênica dos alelos S e Z de 0,16 e 0,028. Dois pacientes tinham genótipo SZ (AAT ≤ 89 mg/dL). Os pacientes foram divididos em grupos segundo a concentração de AAT: ≤ 89 mg/dL (deficiência, nenhum grupo); 90-140 mg/dL (faixa intermediária, Grupo 1, n = 30); e ≥ 141 mg/dL (normal, Grupo 2, n = 57). A freqüência de fumantes foi igual nos dois grupos, com carga tabágica maior no Grupo 2. O alelo S estava presente em 13 e 14 pacientes dos Grupos 1 e 2, respectivamente, enquanto que o alelo Z estava presente em 2 e 1 paciente dos mesmos grupos. Não houve diferença nos testes de função pulmonar, nem na freqüência de bronquiectasias ou enfisema entre os dois grupos. Os valores espirométricos e as concentrações de AAT foram similares entre fumantes e não-fumantes. Bronquiectasias foram mais freqüentes entre os não fumantes, e enfisema foi mais freqüente entre os fumantes. Conclusões: Trinta pacientes apresentaram níveis de AAT abaixo da média esperada para os genótipos MM e MS, e este fato não pode ser explicado por uma freqüência maior dos alelos S e Z.
Descritores: Alfa 1-antitripsina; Enfisema; Pneumopatias; Alelos.
* Study carried out in the Departments of Pulmonology and Medical Genetics, Universidade Estadual de Campinas – Unicamp, State University at Campinas – School of Medical Sciences, Campinas, Brazil.
1. PhD in Genetics. Universidade Estadual de Campinas – Unicamp, State University at Campinas – School of Medical Sciences, Campinas, Brazil.
2. Associate Professor. Department of Medical Genetics, Universidade Estadual de Campinas – Unicamp, State University at Campinas – School of Medical Sciences, Campinas, Brazil.
3. Professor. Pontifícia Universidade Católica de Campinas – PUC-Campinas, Pontifical Catholic University of Campinas – School of Medicine, Campinas, Brazil. 4. Associate Professor. Department of Clinical Pathology, Universidade Estadual de Campinas – Unicamp, State University at Campinas – School of Medical Sciences, Campinas, Brazil.
5. Associate Professor. Director of the Department of Forensic Genetics, Universidade Estadual de Campinas – Unicamp, State University at Campinas – School of Medical Sciences, Campinas, Brazil.
6. Associate Professor. Department of Clinical Medicine, Universidade Estadual de Campinas – Unicamp, State University at Campinas – School of Medical Sciences, Campinas, Brazil.
Correspondence to: Mônica Corso Pereira. Rua Edilberto Luis Pereira da Silva, 954, Cidade Universitária, CEP 13083-190, Campinas, SP, Brasil. Tel 55 19 3242-0255. E-mail: [email protected]
Financial support: This study received financial support from the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, Foundation for the Support of Research in the State of São Paulo; Process no. 1997/14159-7).
positivity for antineutrophil cytoplasmic antibodies with cytoplasmic pattern.(5)
The gene responsible for AAT synthesis is located on chromosome 14, and production occurs princi-pally in hepatocytes, although other cells, such as mononuclear phagocytes and epithelial cells of the lung and intestine, can contribute. The highly pleo-morphic nature of AAT indicates that the gene locus is also highly variable: approximately 100 different alleles have been identified to date. The vari-ants are inherited codominantly and are classified according to the protease inhibitor (PI) system, which is based on the electrophoretic mobility of the different proteins on acrylamide gels. The most common phenotype, the MM (medium mobility) phenotype, is present in 94% to 96% of Caucasians and is associated with serum AAT levels within the 150-350 mg/ dL range.(5)
Low serum and tissue levels of AAT occur as a result of the inheritance of two alleles (S and Z) that encode decreased levels of this protein.
The Z allele (PI*Z), when homozygous (PI*ZZ), results in serum AAT levels ranging from 15 to 50 mg/dL. In this setting, panacinar pulmonary emphysema is the most common clinical manifesta-tion, as well as being the leading cause of incapacity and death. The Z allele is the allele most commonly found in Caucasians coming from northern Europe, and accounts for 1-3% of all AAT alleles in such individuals.(2)
The S allele is more common than the Z allele, accounting for 2-4% of all AAT alleles in Caucasians from northern Europe and for 15% of all AAT alleles in individuals from the Iberian Peninsula, being especially prominent in those from northern Portugal and the region of Galicia, in Spain.(2,6)
The SZ genotype (PI*SZ) results in AAT levels ranging from 45 to 105 mg/dL, whereas the SS genotype (PI*SS) produces levels ranging from 100 to 140 mg/dL.(7) Individuals who are SZ heterozygotes are three times more likely to develop COPD.(8)
The low frequency of S and Z alleles in the popu-lation makes it difficult to obtain data on the gene frequency and the presence of AAT deficiency in the general population. In Brazil, given the level of laboratory sophistication required, there have been no studies involving epidemiological investigation in the general population.
Introduction
Neutrophils, which normally pass unimpeded through the pulmonary vascular system, adhere to the endothelium of capillaries and venules in response to activation by inflammatory stimuli. Neutrophil activation leads to the release of many substances, such as reactive oxygen species, cationic peptides, eicosanoids and proteo-lytic enzymes, all of which have the function of destroying aggressor agents. The activity of those substances, however, needs to be controlled by antagonists in order to prevent tissue damage and organ dysfunction.
Serine proteases, a group of neutrophil proteolytic enzymes, have various functions, such as degrading elastic and collagen fibers, producing secretory cell metaplasia in the respiratory epithelium, affecting the ciliary beat, activating the complement system, increasing interleukin-8 synthesis and increasing tumor necrosis factor-alpha synthesis, as well as activating or inactivating various cytokines.(1)
Neutrophil elastase, which is the most important serine protease, is one of the few human enzymes capable of degrading elastic fibers, which are responsible for tissue elastic recoil, including that of the alveolar walls.(2)
Clinical and experimental lines of evidence have suggested that emphysema is caused by elastase-induced destruction of elastic fibers of the lung interstitium. In 1963, two authors described five patients with alpha 1-antitrypsin (AAT) deficiency, AAT being the substance primarily responsible for neutrophil elastase inhibition; three of those patients had emphysema.(3) In 1965, one group of authors instilled papain (through the trachea) into the lung of rodents in an attempt to produce granulomas.(4) The authors discovered that papain caused emphysema.
High-resolution computed tomography (using thin slices and a high-resolution algorithm) was performed with a GE-9800 scanner (General Electric Medical Systems, Milwaukee, WI, USA) or a SOMATON AR.T scanner (Siemens Medical Solutions, Munich, Germany). The department radiologist evaluated the scans for the presence of emphysema or bron-chiectasis. No quantitative analysis of the lesions was performed, nor was the extent or severity of the lesions estimated.
The presence of S and Z alleles was determined by polymerase chain reaction, followed by enzymatic digestion of this amplified material with the restric-tion enzymes XmnI (S allele) and TaqI (Z allele).(9) After the amplification of the DNA fragment and its enzymatic digestion, the samples were submitted to electrophoresis on a 16% polyacrylamide gel.
Nephelometric determination of serum AAT levels was performed using the Array 360 System (Beckman Instruments, Inc., Fullerton, CA, USA). The normal reference range for this test is from 90 to 200 mg/dL.
The data obtained for each patient were analyzed in two ways: by using AAT levels as a dependent variable and by stratification based on the presence / absence of smoking.
The project was approved by the Ethics in Research Committee of the institution, and all patients gave written informed consent prior to their enrollment in the study.
These facts have raised interest in determining the presence of S and Z alleles in the population of patients with chronic respiratory symptoms, without asthma, treated at the outpatient clinic of the Department of Pulmonology of a regional referral hospital.
The objective of the present study was to deter-mine serum AAT levels, as well as to identify S and Z alleles, in a population of patients with chronic respiratory symptoms.
Methods
We selected patients with a clinical profile of productive cough and dyspnea treated at the outpa-tient clinic of the Department of Pulmonology. Infectious causes, such as tuberculosis and fungal infections, were ruled out by testing sputum samples, and asthma was ruled out based on clinical history and spirometry results.
Clinical data (age, gender, race, history of smoking and tobacco intake) were collected, and patients were submitted to spirometry, high-resolution computed tomography of the chest, determination of AAT levels and determination of S and Z alleles.
Pulmonary function tests were performed using a spirometer (model AM 4000 PC; Anamed, São Paulo, Brazil). Forced expiratory volume in one second (FEV1), forced vital capacity (FVC) and the ratio between the two (FEV1/FVC) were analyzed.
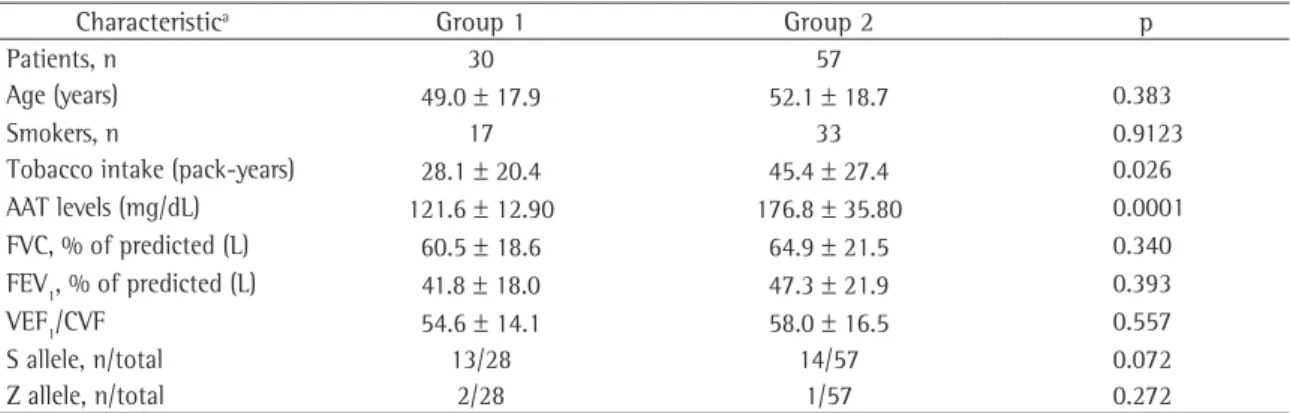
Table 1 - Clinical characteristics and spirometric parameters, as well as results of the determination of alpha-1 antitrypsin levels and of the presence of S and Z alleles, in the patients evaluated.
Characteristica Group 1 Group 2 p
Patients, n 30 57
Age (years) 49.0 ± 17.9 52.1 ± 18.7 0.383
Smokers, n 17 33 0.9123
Tobacco intake (pack-years) 28.1 ± 20.4 45.4 ± 27.4 0.026
AAT levels (mg/dL) 121.6 ± 12.90 176.8 ± 35.80 0.0001
FVC, % of predicted (L) 60.5 ± 18.6 64.9 ± 21.5 0.340
FEV1, % of predicted (L) 41.8 ± 18.0 47.3 ± 21.9 0.393
VEF1/CVF 54.6 ± 14.1 58.0 ± 16.5 0.557
S allele, n/total 13/28 14/57 0.072
Z allele, n/total 2/28 1/57 0.272
aValues expressed as mean ± standard deviation, except when specified; Group 1: alpha-1 antitrypsin (AAT) levels of 90-140 mg/ dL
The clinical characteristics, AAT levels, spirom-etry findings and tomographic findings, as well as the results of the determination of S and Z alleles, for Groups 1 and 2 are listed in Table 1.
There was no difference in terms of the percentage of smokers (57% and 58% in Groups 1 and 2, respectively), although tobacco intake was signifi-cantly different (p = 0.026), being greater in Group 2 (45 pack-years) than in Group 1 (28 pack-years).
The S allele was present in 13 and 14 patients in Groups 1 and 2, respectively, compared with 2 patients and 1 patient, respectively, for the Z allele. There was no significant difference between the two groups in terms of the presence of S or Z alleles (p = 0.072 and p = 0.272, respectively).
The comparison between Groups 1 and 2 in terms of tomographic findings revealed no differ-ences in the frequency of bronchiectasis (p = 0.324) or emphysema (p = 0.938).
The analysis of AAT levels of the patients in Groups 1 and 2, taken together, in the presence or absence of the S allele (Table 2), revealed a signifi-cant difference in the medians (p = 0.0089), with greater values in the group without the S allele.
A second analysis, considering all of the patients studied, compared smokers and nonsmokers in terms of AAT levels and spirometry results. No differences were found in any of the parameters (AAT levels, p = 0.585; FVC, p = 0.157; FEV1, p = 0.870; and FEV1/FVC, p = 0.134). However, smoking was found to be associated with presence of bronchiectasis and emphysema, in opposite ways: bronchiectasis was more common in nonsmokers (p = 0.008) and emphysema was more common in smokers (p = 0.032).
Discussion
Since this was a cross-sectional cohort study involving a population of patients with respiratory symptoms, the data obtained cannot be extrapo-lated to the general population. The present study Statistical analysis of continuous data was
performed using the parametric Student’s t-test or the nonparametric Wilcoxon test, when necessary. The correlations among categorical variables were studied using a parametric chi-square test or the nonparametric Fisher’s exact test, depending on the distribution of frequencies in a two-by-two table. The correlations among continuous variables were analyzed using Pearson and Spearman correlation tests. The SAS® (Statistical Analysis System, Cary, NC, USA) and the Minitab® (Minitab Inc., State College, PA, USA) statistical software were used for all tests. The level of statistical significance was set at 5%.
Results
A total of 89 patients (44 females and 45 males) were evaluated. The mean age was 51.3 ± 18.2 years. Of those, 87 were submitted to determination of S and Z alleles. The S allele was detected in 29 (33.3%) of the 87 patients evaluated, whereas the Z allele was detected in 5 (5.7%). The gene frequency of S and Z alleles was 0.160 and 0.028, respectively. The sample is in Hardy-Weinberg equilibrium (χ2 = 2.69; p = 0.61), which indicates that it is not subject to selection pressure and that the migration flow and the mutation rate are not significant to the point of affecting the interpretations of the analyses performed.
For the analysis of the results, the patients were divided into groups based on AAT levels, according to the cut-off values suggested in the guidelines for the diagnosis and management of individuals with AAT deficiency established by the American Thoracic Society (ATS) in collaboration with the European Respiratory Society (ERS)(5): ≤ 89 mg/ dL (deficiency); 90-140 mg/dL (intermediate); and ≥ 141 mg/dL (normal).
Only 2 patients presented AAT levels ≤ 89 mg/ dL, a number that is insufficient for statistical analysis. Both of those patients were SZ heterozygotes, were heavy smokers (18 and 20 pack-years) and had COPD. One of the two patients had chronic respiratory insufficiency and used home oxygen therapy, whereas the other had a history of frequent exacerbations and presented bronchiectasis on the tomography scan. Among the 89 patients, AAT levels were 90-140 mg/dL in 30 and ≥ 141 mg/dL in 57. These were designated Group 1 and Group 2, respectively.
Table 2 - Alpha-1 antitrypsin levels in the presence or absence of the S allele.
Variable S allele Level, median (minimum-maximum)
p AAT (mg/dL) Present 143 (105-181) 0.0089
Absent 166 (97-371)
In addition, the two groups presented equal degrees of abnormality in the spirometry findings (p > 0.05). In Group 1, FVC (% of predicted) was 60.5 ± 18.6 L, FEV1 (% of predicted) was 41.8 ± 18.0 L and the FEV1/FVC ratio was 54.6 ± 14.1, compared with 64.9 ± 21.5 L, 47.3 ± 21.9 L and 58.0 ± 16.5, respectively, in Group 2 (Table 1).
Based on the data presented above, we can conclude that, in the population studied, interme-diate AAT levels were more common among patients who smoked less heavily. However, the intermediate AAT levels cannot be explained by a greater presence of S and Z alleles, since there was no statistically significant difference between the two groups in terms of the frequency of S and Z heterozygotes, which was 13/28 and 14/57 for S heterozygotes in Groups 1 and 2, respectively, compared with 2/28 and 1/57, respectively, for Z heterozygotes (Table 1; p = 0.072 and p = 0.272, respectively). Nevertheless, it should be noted that the frequency of the S allele was greater in Group 1 than in Group 2, and the level of significance found in the comparison of the two groups (p = 0.072) seems to suggest a tendency that would eventually be confirmed if we had evalu-ated a greater number of patients.
In a meta-analysis published in 2005,(8) the role of the S allele in the risk of COPD was investigated. The authors found that SZ heterozygotes were three times more likely to develop the disease. Regarding individuals with the MS genotype, cross-sectional and case-control studies have revealed a small but significant increase in the risk of COPD.
In addition, the median AAT levels were signifi-cantly lower in patients with a single S allele (p = 0.0089) than in patients without the S or the Z allele (Table 2). In the present study, lower AAT levels, whether caused by the presence of a deficient allele or not, seemed to be associated with higher susceptibility to respiratory diseases. Since only S and Z alleles were investigated, we cannot rule out the possibility that patients with intermediate AAT levels have some known rare allele or even genetic alterations yet to be described, which could be detected only by gene sequencing.
There are nongenetic causes of AAT deficiency, such as liver diseases or other pathological conditions that lead to protein loss. However, those comorbidi-was carried out in an institution that serves a region
with approximately 4 million inhabitants, and, since this institution is a referral hospital for severe cases, the population treated represents the characteristic miscegenation of the Brazilian population, espe-cially that of the state of São Paulo.
In the analysis of the results, we opted for using three serum AAT level ranges to define three groups: the first with AAT levels ≤ 89 mg/ dL (deficiency); the second with AAT levels of 90-140 mg / dL (intermediate); and the third with AAT levels ≥ 141 mg/dL (normal). According to the ATS/ERS document,(5) even patients with intermediate AAT levels should be submitted to a qualitative test, such as phenotyping or geno-typing, as was done in the present study, although AAT levels > 50 mg/dL are considered protective against the development of emphysema.
Decreased serum AAT levels should not have, a priori, any relationship with the smoking habit. In fact, since AAT is an acute phase protein, the expected effect of smoking on AAT levels would be that of an increase, due to the inflammatory process triggered by the substances present in tobacco smoke. There is evidence that, although not decreasing AAT levels in the blood and tissues, smoking can decrease AAT activity due to methio-nine oxidation at the protein active site.(5) In the patients studied here, greater tobacco intake was associated with higher AAT levels (p = 0.026).
In summary, the S allele was detected in 33.3% of the 89 patients studied, whereas the Z allele was detected in 5.7%. The quantitative analysis of AAT levels revealed that 30 patients presented serum AAT levels lower than the mean values found in patients with the MM or MS genotype, who account for most of the population (94-96% of Caucasians).(5)
In Brazil, there are no data on the frequency of S and Z alleles or on the quantitative analysis of AAT levels in the general population. It can be said, however, that the AAT levels found, which were classified as intermediate, cannot be explained by an increased frequency of S and Z alleles in those patients. More comprehensive studies, preferably multicenter studies, are needed in order to deter-mine the frequency of the principal alleles associated with AAT deficiency in Brazil.
References
1. Tetley TD. Antiprotease Therapy. In: Cazzola M, Celli B, Dahl R, Rennard S, editors. Therapeutic Strategies in COPD. Oxford: Clinical Publishing; 2005. p. 233-245.
2. Crystal RG, Brantly ML, Hubbard RC, Curiel DT, States DJ, Holmes MD. The alpha 1-antitrypsin gene and its mutations. Clinical consequences and strategies for therapy. Chest. 1989;95(1):196-208.
3. Laurell CB, Eriksson S. The electrophoretic alpha-1 globulin pattern of serum in alpha-1 antitrypsin deficiency. Scan J Clin Lab Invest. 1963;15(2):132-140.
4. Gross P, Pfitzer EA, Tolker E, Babyak MA, Kaschak M. Experimental emphysema: its production with papain in normal and silicotic rats. Arch Environ Health. 1965;11:50-8.
5. American Thoracic Society/European Respiratory Society Statement. Standards for the Diagnosis and Management of Individuals with Alpha-1 Antitrypsin Deficiency. Am J Respir Crit Care Med. 2003;168(7):818-900.
6. Hutchison DC. Alpha 1-antitrypsin deficiency in Europe: geographical distribution of Pi types S and Z. Respir Med. 1998;92(3):367-77.
7. Ogushi F, Hubbard RC, Fells GA, Casolaro MA, Curiel DT, Brantly ML, et al. Evaluation of the S-type of alpha-1-antitrypsin as an in vivo and in vitro inhibitor of neutrophil elastase. Am Rev Respir Dis. 1988;137(2):364-70.
8. Dahl M, Hersh CP, Ly NP, Berkey CS, Silverman EK, Nordestgaard BG. The protease inhibitor PI*S allele and COPD: a meta-analysis. Eur Respir J. 2005;26(1):67-76. 9. Andresen BS, Knudsen I, Jensen PK, Rasmussen K, Gregersen
N. Two novel nonradioactive polymerase chain reaction-based assays of dried blood spots, genomic DNA, or whole cells for fast, reliable detection of Z and S mutations in the alpha 1-antitrypsin gene. Clin Chem. 1992;38(10):2100-7. 10. Brantly ML, Wittes JT, Vogelmeier CF, Hubbard RC, Fells
GA, Crystal RG. Use of a highly purified alpha 1-antitrypsin standard to establish ranges for the common normal
ties were not present in the patients included in the present study.
The frequency of bronchiectasis was the same in Groups 1 and 2, as it was in patients with and without the S allele. Although there is substantial evidence that the presence of bronchiectasis is common in patients with severe AAT deficiency,(11) the genesis of bronchiectasis is certainly multifactorial.
Considering smokers and nonsmokers, tomo-graphic findings of bronchiectasis were significantly more common in nonsmokers, probably because this disease was the cause of chronic respiratory symp-toms that motivated the inclusion of those patients in the study.
As expected, tomographic findings of emphy-sema were much more common in smokers than in nonsmokers, although there was no statisti-cally significant difference between Groups 1 and 2 in terms of the frequency of a diagnosis of emphysema.
Low AAT levels can worsen emphysema lesions due to the lack of protease inhibition, as well as to the absence of inhibition of alveolar epithelial cell apoptosis. In an experimental study involving a model of noninflammatory emphysema,(12) in which the alterations were produced by the inhibi-tion of vascular endothelial growth factor receptors, the authors provided additional evidence of this new role of AAT (reducing alveolar epithelial cell apoptosis in emphysema). In mice more susceptible to tobacco-induced emphysema, which present a 50% reduction in AAT levels in the bronchoalveolar lavage fluid, the increase in the AAT levels available decreased the emphysema produced by the vascular endothelial growth factor receptor inhibitors.
the prevention of pulmonary emphysema. Am J Respir Crit Care Med. 2006;173(11):1222-8.
13. Sandford AJ, Chagani T, Weir TD, Connett JE, Anthonisen NR, Paré PD. Susceptibility genes for rapid decline of lung function in the lung health study. Am J Respir Crit Care Med. 2001;163(2):469-73.
and deficient alpha 1-antitrypsin phenotypes. Chest. 1991;100(3):703-8.
11. Parr DG, Guest PG, Reynolds JH, Dowson LJ, Stockley RA. Prevalence and impact of bronchiectasis in alpha1-antitrypsin deficiency. Am J Respir Crit Care Med. 2007;176(12):1215-21. 12. Petrache I, Fijalkowska I, Zhen L, Medler TR, Brown E, Cruz