SEROLOGIC
SURVEY OF HEPATITIS
A ANTIBODIES
IN MEXICAN
CHILDREN1
JesGs Kumate, 2 Ana Maria Alvizouri,3
and Armando Isibasi4
Examination of 890 sera from Mexican children has indicated high levels of exposure to hepatitis A virus. Problems relating to environmental sanitation, personal hygiene, andfecal contamination offoods and beverages could account for these exposure levels.
Introduction
Hepatitis A virus (HAV) is a cosmopolitan pathogen that strikes at all population groups regardless of age, sex, socioeconomic level, or nutritional status. It is transmitted by contact with fecally contaminated foods and beverages (1, 2).
Since the infection is clinically inapparent in a vast majority of cases, anamnesis is of no use in determining the morbidity rate; esti- mates of the ratio of icteric to anicteric cases range from 2:l to 0.08:1 (3-5).
With the development of serologic tech-
niques specific for HAV (6, 7), the epidemi- ology of the disease has been investigated and
information has been obtained concerning the
time when antibodies appear and the manner
in which immunogenic experience with HAV
is acquired. Data collected worldwide indicate that the occurrence of antibodies differs great- ly in different age groups (S), although there is also a correlation between the average socio- economic level of the subjects and the age at
which antibodies to HAV appear.
Materials and Methods
The availability of sera obtained for a na-
lAlso appearing in Spanish in the Boletin de la Oficina Sanitaria Pammricana 92(6), 1982.
2Chairmaq Department of Infectious Diseases, Hospital Infantil de M&co.
3Research Assistant, Department of Infectious Diseases, Hospital Infantil de kkkico.
%Senior Research Fellow, Department of Infectious Diseases, Hospital Infantil de M&co.
tionwide seroepidemiologic survey enabled us
to examine the incidence of antibodies to
HAV in 890 specimens from children living in six areas of central, northeast, and southeast Mexico. Sera were obtained under sterile con- ditions from children up to 15 years of age in
Mexico City (284 sera), Morelia (131 sera),
Hermosillo (132 sera), La Paz (120 sera),
Chihuahua(121 sera), andMhrida(l02 sera).
The localities chosen for sample collection all
had over 5,000 inhabitants and were repre-
sentative of urban settlements in geographi- cally similar parts of the country. Twenty- seven of the 890 subjects were infants, 190 were preschool children, and 673 were school- children.
Regarding socioeconomic status, 253 of the
Mexico City samples were obtained in three
residential areas with different socioeconomic
levels-these being Tepito, a lower middle
class area; Tlatelolco, a middle class area; and
San Angel, an upper middle class area.
Eighty-nine sera were obtained in Tepito, 74 in Tlatelolco, and 90 in San Angel.
All 890 serum samples were obtained in
1973 and were stored at -2O’C until they were tested in 1979. The serologic testing technique
used was the one developed by Bradley and
coworkers (9) and marketed commercially by
Abbot as HAVAB . It consists of an assay
based on competition between antibody in the
serum sample and IgG antibody labeled with
11z5 for HAV antigen taken from infected
chimpanzee livers and coated on polystyrene particles (9). The results recorded were ob- tained with undiluted sera.
Kumate et al. l HEPATITIS A ANTIBODIES IN MEXICAN CHILDREN 157
Results and Discussion
Table 1 compares the prevalence of serum
HAV antibodies that our study detected in
preschoolers and schoolchildren with findings for similar age groups in the United States,
Costa Rica, Australia, and Gambia (10-14).
In general, radioimmunoassay of the sort per- formed here has proved more sensitive than
the immunoadherence hemagglutination tech-
nique used in some of the other studies. In
Gambia, for example, Ajdukiewicz and
Mosley (14) obtained a 49 per cent positive
response with immunoadherence hemaggluti-
nation and a 74 per cent positive response
with the radioimmunoassay technique.
Overall, our data revealed high percentages of sera positive for HAV antibodies from the first year of life onward. For the 27 infants over six months old this figure was 33 per cent, the 95 per cent confidence limits ranging from 17 to 53 per cent; for the 190 preschool- ers the respective figures were 75 and 64-82 per cent; and for the 673 schoolchildren they were 84 and 82-86 per cent. The percentages of positive sera from children of different ages
are charted in Figure 1. These percentages
were found to conform with the plot of a loga- rithmic curve based on the formula y = 41.4
+ 50.7 log x.
The findings of this and similar surveys
must be interpreted in the light of sample
Figure 1. Percentages of 800 sera from children 1-15 years of age in six Mexican cities showing
antibodies to hepatitis A virus, by age group. The data from the 90 San Angel schoolchildren tested have been excluded because no preschool-
ers were included in this subgroup.
-I
sizes, sampling methods, socioeconomic
levels, and serologic techniques. In the
present case the total number of sera tested was large enough to be considered acceptable,
Table 1. Percentages of wra from children 1-15 years of age in various countries showing antibodies to hepatitis A virus.
Children, by age group Country and
year of survey
l-5 years 6-10 years 11-15 years
NO. % NO. % NO. %
Mexico, 1973a 190 75.0 291= 89.3 292c 92.8
Australia, 1975a 94 10.6 101 22.5 81 28.4
Costa Rica, 1976h 60 36.7 120 71.7 20 95.0 United States, 197713 34 8.8 33 24.2 39 30.8
Gambia, 1979b 50 24.0 32 56.0 53 62.0
‘Radioimmunoassay.
bImmunoadherence hemagglutination.
but very few infant sera (27) were examined because it was hard to obtain serum samples from this age group.
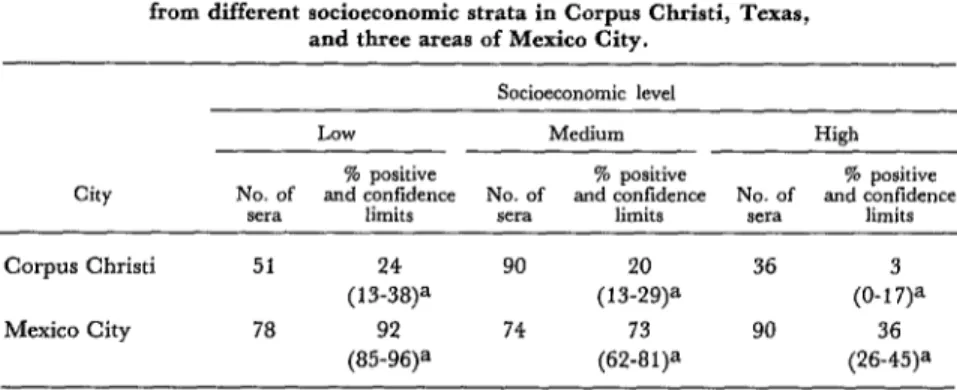
An inverse relationship observed between
socioeconomic levels and the presence of
HAV antibodies is an almost universal find- ing. For example, as Table 2 shows, a survey
in Corpus Christi, Texas, found that sera
from subjects with low, middle, and high so-
cioeconomic status yielded positive responses
in 24, 20, and 3 per cent of the cases, respec- tively. In our own study, 35.5 per cent of the sera from the upper middle class area of San
Angel were positive, as compared to 73 per
cent of the sera from Tlatelolco (middle class) and 96 per cent of the sera from Tepito (lower middle class).
In most developed countries, the percent- ages of positive serologic responses to hepatitis A virus rise gradually with age and by adult- hood are still under 50 per cent. Two excep- tions to this rule have been found, these being
Belgium and Israel, where positive responses
have been obtained from 87 and 94 per cent of the respective sera tested (15). It seems un- likely that poor environmental sanitation, the factor commonly responsible for high rates of
exposure, could account for these results.
However, the practice of caring for preschool- ers in day-care centers during their parents’ working hours is a factor of growing impor-
tance in the developed countries, and this
could account for exposure at early ages even
where environmental sanitation is satisfactory (16).
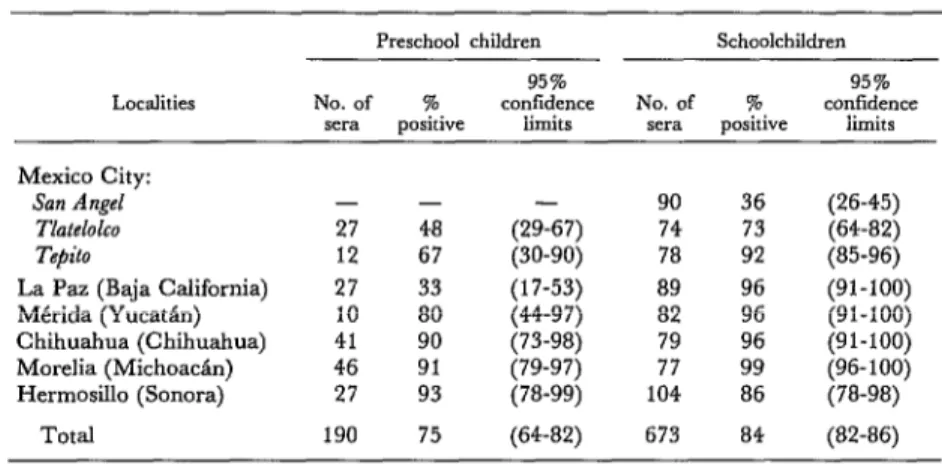
Our data for preschoolers were highly
variable, ranging from 33 per cent positive results in La Paz and 48 per cent in Tlatelolco to 80 per cent in MCrida and 90, 91, and 93
per cent in Chihuahua, Morelia, and Hermo-
sill0 (Table 3). These disparities cannot be ex- plained on the basis of socioeconomic differ-
ences, because average living standards in
Hermosillo and Chihuahua were at least as
high as those in La Paz and Tlatelolco (17). In contrast to the data on preschoolers’ sera, no significant differences were found be-
tween the percentages of positive responses
obtained from schoolchildren in the five areas
outside Mexico City, these percentages ex-
ceeding 90 per cent of the sera tested in most cases.
The most probable interpretation of our
overall findings showing high percentages of
positive sera is that the infant population was exposed very early to HAV as a result of poor
environmental sanitation, uncertain personal
hygiene, and substantial fecal contamination of foods and beverages. This situation is very similar to that found with regard to poliovirus, where children have generally been immuno- genitally exposed before reaching two years of
age, and where subsequent exposures have
yielded small subsequent increases in anti-
body levels, so that few individuals remain susceptible by the time they are adults.
Table 2. Prevalencea of liepatitis A serum antibodies in whoolchildren from different socioeconomic strata in Corpus Cbristi, Texas,
and three areas of Mexico City.
Socioeconomic level
LOW Medium High
City No. of and confidence % positive No. of and confidence % positive No. of and confidence % positive sera limits sera limits sera limits
Corpus Christi 51 90 36 (O-l&
Mexico City 78 (85?6)a 74 (6&a 90 (26?5)=
Kumate et al. l HEPATITIS A ANTIBODIES IN MEXICAN CHILDREN 159
Table 3. Prevalences of hepatitis A serum antibodies in preschoolers and schoolchildren from six Mexican cities.
Localities
Preschool children Schoolchildren
95% 95%
No. of % confidence No. of % confidence set-a positive limits sera. positive limits Mexico City:
San Angel Tl&+JkO Tepito
La Paz (Baja California) Mtrida (Yucatsn) Chihuahua (Chihuahua) Morelia (Michoadn) Hermosillo (Sonora)
- - (29-67) 90 36
27 48 74 73
12 67 (30-90) 78 92
27 33 (17-53) 89 96
10 80 (44-97) 82 96
41 90 (73-98) 79 96
46 91 (79-97) 77 99
27 93 (78-99) 104 86
(26-45) (64-82) (85-96) (91-100) (91-100) (91-100) (96- 100) (78-98)
Total 190 75 (64-82) 673 84 (82-86)
SUMMARY
Sera from a 1973 epidemiologic survey in Mexico were examined in an effort to determine levels of childhood exposure to hepatitis A virus. In all, 890 sera from subjects up to 15 years of age in six cities were examined. The examination detected anti- bodies to hepatitis A virus in sera from 33 per cent of 27 infants, 75 per cent of 190 preschool children, and 84 per cent of 673 school-age children. It also found that sera from some areas of Mexico City with relatively low socioeconomic levels were more
apt to yield positive results than sera from areas with higher socioeconomic levels.
The most probable explanations for the high general exposure levels found were poor environ- mental sanitation, uncertain personal hygiene, and substantial fecal contamination of foods and bever- ages. This situation is similar to that regarding poliovirus, where children have generally been im- munologically exposed before they are two years old.
REFERENCES
(1) Rowland, A. J., and J. F. Skone. Epidemi- gamma globulin and on the incidence of inapparent olo,,q-y of infectious hepatitis. Br Med Bull 28:149, infection../.. 174:823, 1960.
197X
(2) Mosley, J. W. The epidemiology of viral hepatitis: An overview. Am J Med Sci 270:253, 1975.
(3) Matthew, E. B., D. E. Dietzman, D. L. Madden, S. J. Newman, J. L. Sever, B. Nagler, S. M. Bouton, and M. Rostafinski. A major epidemic of infectious hepatitis in an institution for the men- tally retarded. AmJ Epidemiol98: 199, 1973.
(4) Decker, R. H., L. R. Overby, C. M. Ling, G. Frijsner, F. Deinhardt, and J. Beggs. Serologic studies of transmission of hepatitis A in humans. J Infect Dis 139:74, 1979.
(5) Krugman, S., R. Ward, J. Giles, and A. M. Jacobs. Infectious hepatitis: Studies on the effect of
(6) Miller, W. J., P. J. Provost, W. J. M&leer, 0. L. Ittensohn, V. M. Villarejos, and M. R. Hilleman. Specific immune adherence assay for human hepatitis A antibody: Application to diag- nostic and epidemiologic investigations. Proc Sot Exp Biol Med 149:254, 1975.
(7) Provost, P. J., 0. L. Ittensohn, V. M. Villa- rejos, and M. R. Hilleman. A specific complement- fxation test for human hepatitis A employing CR 326 virus antigen: Diagnosis and epidemiology. Proc Sot Exp Biol Med 148:962, 1975.
(8) Dienstag, J. L. The pathobiology of hepatitis A virus. Int Rev Exp Pathol 20: 1, 1979.
Whittington, and L. R. Overby. Serodiagnosis of viral hepatitis A by a modified competitive binding radioimmunoassay for immunoglobulin M anti- hepatitis A virus. J Clin Microbial 9: 120, 1979.
(10) Maynard, J. E., D. W. Bradley, C. L. Hornbeck, R. M. Fields, and I. L. Doto. Prelimi- nary serologic studies of antibody to hepatitis A virus in populations in the United States. J Infect Dis 134:528, 1976.
(11) Villarejos, V. M., P. J. Provost, 0. L. Ittensohn, A. A. Mclean, and M. R. Hilleman. Seroepidemiologic investigations of human hepati- tis caused by A, B, and a possible third virus. Proc SOG Exp Biol Med 152:524, 1976.
(12) Zacarfas, J., J. Rakela, L. Macho, and J. Mosley. Estudio de anticuerpos de hepatitis A en
niiios. Bol Med Ho@ Infant Mex 36:571, 1979. (13) Gust, I. D., N.I.Z. Lehmann, C. R.
Lucas, A. A. Ferris, and S. A. Locarnini. Studies on the Epidemiology of Hepatitis A in Melbourne. In G. N. Vyas, S. N. Cohen, and R. Schmid. Viral Hepatitis. The Franklin Institute Press, Philadel- phia, 1978, p. 105.
(14) Ajdukiewicz, A., and J. W. Mosley. Hepa- titis A antibody in West Africa. Lancet 2:695, 1980.
(15) Szmuness, W., J. L. Dienstag, R. H. Purcell, C. E. Stevens, D. C. Wong, H. &ram, S. Bar-Shany, R. P. Beasley, J. Desmyter, and J. A. Gaon. The prevalence of antibody to hepatitis A antigen in various parts of the world: A pilot study. Am J Epidemiol 106:392, 1977.
(16) Hadler, S. C., H. M. Webster, J. J. Erben, J. E. Swanson, and J. E. Maynard. Hepatitis A in