www.jped.com.br
ORIGINAL
ARTICLE
Nutritional
management
and
postoperative
prognosis
of
newborns
submitted
to
primary
surgical
repair
of
gastroschisis
夽
Flavia
Miranda
da
Silva
Alves
a,b,∗,
Marcelo
Eller
Miranda
b,
Marcos
José
Burle
de
Aguiar
a,
Maria
Cândida
Ferrarez
Bouzada
Viana
aaDepartmentofPediatrics,SchoolofMedicine,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil bDepartmentofSurgery,SchoolofMedicine,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received24May2015;accepted17July2015 Availableonline2February2016
KEYWORDS Gastroschisis; Nutrition; Lengthofhospital stay
Abstract
Objective: Gastroschisisisadefectoftheabdominalwall,resultingincongenitalevisceration
andrequiringneonatalintensivecare,earlysurgicalcorrection,andparenteralnutrition.This study evaluatednewbornswithgastroschisis,seeking toassociatenutritionalcharacteristics withtimeofhospitalstay.
Methods: Thiswasaretrospectivecohortstudyof49newbornsundergoingprimaryrepairof
gastroschisisbetweenJanuary1995andDecember2010.Thenewborns’characteristicswere describedwithemphasisonnutritionalaspects,correlatingthemwithlengthofhospitalstay.
Results: Thecharacteristicsthatinfluencedlengthofhospitalstaywere:(1)newbornsmallfor
gestationalage(SGA);(2)useofantibiotics;(3)dayoflifewhenenteralfeedingwasstarted;(4) dayoflifewhenfulldietwasreached.SGAinfantshadlongerlengthofhospitalstay(24.2%) thanothernewborns.The lengthofhospitalstaywas increasedby 2.1%for eachadditional daytakentointroduceenteralfeeding. However,sloweronsetoffullenteralfeedingacted asaprotectivefactor,decreasinglengthofstayby3.6%.Thevolumeofwastedrainedbythe stomach catheterinthe24hprior thestartofenteralfeedingwasnotassociated withthe timingofdietintroductionorlengthofhospitalstay.
Conclusion: Earlystartofenteralfeedingandsmall,gradualincreaseofvolumecanshorten
theuseofparenteralnutrition.Thismanagementstrategycontributestoreducetheincidence ofinfectionandlengthofhospitalstayofnewbornswithgastroschisis.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Please citethis articleas: Miranda da SilvaAlves F,Miranda ME, de Aguiar MJ,BouzadaViana MC. Nutritionalmanagement and postoperativeprognosisofnewbornssubmittedtoprimarysurgicalrepairofgastroschisis.JPediatr(RioJ).2016;92:268---75.
∗Correspondingauthor.
E-mail:[email protected](F.MirandadaSilvaAlves). http://dx.doi.org/10.1016/j.jped.2015.07.009
PALAVRAS-CHAVE Gastrosquise; Nutric¸ão; Tempode hospitalizac¸ão
Manejonutricionaleprognósticopós-operatóriodorecém-nascidosubmetido àcorrec¸ãocirúrgicaprimáriadegastrosquise
Resumo
Objetivo: agastrosquiseéumamalformac¸ãodaparedeabdominalqueresultaemeviscerac¸ão
congênita, e requer tratamento intensivo neonatal, correc¸ão cirúrgica precoce e nutric¸ão parenteral.Investigou-senesteestudoosrecém-nascidoscomgastrosquise,procurando cor-relacionarassuascaracterísticasnutricionaiscomotempodainternac¸ãohospitalar.
Métodos: estudodecoorteretrospectivode49recém-nascidossubmetidosàcorrec¸ãoprimária
de gastrosquiseno período dejaneiro de1995a dezembro de2010. Ascaracterísticas dos neonatosforamdescritascomênfasenosaspectosnutricionaisrelacionando-ascomotempo deinternac¸ãohospitalar.
Resultados: ascaracterísticas queinfluenciarama durac¸ão dainternac¸ãoforam: 1)
recém-nascidospequenos paraaidade gestacional (PIG);2) usodeantibióticos; 3) dia devidaao iniciaradietaenteral;4)diadevidaaoatingiradietaplena.Recém-nascidosPIGtiverammaior tempodeinternac¸ão(24,2%)quedemaisneonatos.Otempodeinternac¸ãofoiaumentadoem 2,1%paracadadiaamaisquesedemorouaintroduziradietaenteral.Entretanto,atingirmais lentamenteoaporteplenodadietaenteralagiucomofatorprotetor,diminuindo3,6%notempo deinternac¸ão.Ovolumederesíduodrenadopelocatetergástrico,nasúltimas24horasantes doiníciodadietaenteral,nãoapresentoucorrelac¸ãocomomomentodaintroduc¸ãodadieta, nemcomadurac¸ãodahospitalizac¸ão.
Conclusão: iniciaradietaenteralprecocemente,comaumentogradativoempequenosvolumes
podeabreviaradurac¸ãodanutric¸ãoparenteral.Estemanejocontribuiparaadiminuic¸ãoda incidênciadeinfecc¸õesedotempodehospitalizac¸ãoderecém-nascidoscomgastrosquise. ©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
In Brazil, in recent years, congenital abnormalities have become the second most important cause of infant mortality1 and have generated various morbidities that compromisethesechildren’sfuturequalityoflife.
Severalfactorshavecontributedtothedeclineininfant mortality rates in recent years. Among them are the advancesinperinatalcare,expansionofneonatalintensive careunits,improvedmechanicalventilationdevices,useof parenteral nutrition,advancesin pre-and postnatal diag-nosticmethods,andupdatedprotocolsfor perinatalcare. Thus, newborns with gastroschisis can currently achieve survival rates that surpass 90%, especially in developed countries.2
Nevertheless,thelengthofhospitalstayisstillamatter ofconcern.Thehighcost,thenutritionaldisability,andthe complications,inadditiontothefamilyproblemscausedby them, makecongenital malformationsimportant issuesto beidentifiedandstudied.
Newbornswithgastroschisishave adefect inthe ante-riorabdominalwall,unrelatedtotheumbilicalcord,which resultsintheexteriorizationoftheabdominalviscerafrom the time of intrauterine life. A frequency of two to five cases of gastroschisis per 10,000 livebirths is estimated, withanupwardtrendinseveralcountriesoverthelast20---30 years.3,4
The treatment of gastroschisis requires intensive care shortlyafterbirth,surgicalcorrectionwithinthefirsthours
oflife,andparenteralnutrition.Themaincomplicationsare duetointestinal dysfunction(paralyticileus, obstruction, atresia, malrotation, adhesions, resection, short bowel), thelengthofhospitalstay,andepisodesofsepticemiaand malnutrition.Depending on the viscero-abdominal dispro-portion,surgical correction can be performed in a single procedurewithprimaryclosure of theabdominalwall, or using a staged technique, with the creation of an extra-abdominalsilo,initially,tocontainandtemporarilyprotect theexternalizedviscera.5
The understanding of the nutritional aspects of these newborns and their impact on hospital stay allows the multidisciplinary team toestablish strategies todecrease morbidityandmortality,aswellastoestablishnutritional approach protocols, concentrating on the volume of the offerednutritionandthetimeofitsintroduction.
The aimof this studywastoidentifyand describethe profileof newborns withgastroschisis undergoing primary surgical correction andassociate their nutritional charac-teristicswithlengthofhospitalstay.
Methods
The diagnosis was obtained by fetal ultrasonography and/orthroughtheclinicalexaminationatbirth.
A total of 40,819 live births were identified through analysis of the Estudo Colaborativo Latino Americano de Malformac¸õesCongênitas(ECLAMC)(Latin-American Collab-orativeStudy ofCongenitalMalformations), ofwhich4111 livebirthshadmalformations;ofthese,89had gastroschi-sis.Atotal of 49patients, according tothe identification foundin themedicalrecordsandconfirmed bythe analy-siscarriedoutbythepediatricsurgeryteamofHC---UFMG, had been submitted to primary closure. Newborns with genetic syndromes, those born of multiple pregnancies, thosenot born at HC---UFMG, and thosewithgastroschisis repairedusingthestagedtechniquewereexcludedfromthe study.
Variables relatedtothenewborn wereidentified,such asgender,gestationalage,classificationinrelationto ges-tationalageandbirthweight,Apgar scoreat1and5min, presenceof othermalformations,locationof the anatom-ical defect in relation to the umbilical cord, aspect of theexternalizedbowelloops(simple:noalterations; com-plex:necrosis,ischemia,perforation,stenosisandatresia), contentofexternalizedviscera(onlyintestineorassociated withotherorgans),thesizeoftheabdominalwalldefect, timeuntil the surgery, whetherbowel resection was per-formedinthefirstsurgery,theneedforfurtherinterventions duringhospitalization,timeofmechanicalventilation, num-berofantibiotictherapycycles,useofmusclerelaxant,and occurrenceofhemodynamicinstability(shock).Nutritional approachdata were assessed, such astime of parenteral nutrition,dayoflifewhenthedietwasinitiated,volumeof gastricresiduein 24hbeforethestart ofthe diet,dayof lifewhenfulldietwasreached,sodiumandserumalbumin measurement,whetheror notenteralnutritionwas inter-ruptedafter itsstart, weightat discharge, and weightat discharge/birthweightratio.
Adescriptiveanalysiswasperformed of newborn char-acteristics and nutritional aspects. The variables were submitted to univariate and multivariate analysis consid-eringthe timeof thefirsthospitalizationanditsoutcome (dischargeordeath).
Rsoftware®,version3.0.3forWindows(Microsoft®,WA, USA),wasusedfor the univariateand multivariate analy-sis.Thestepwise6methodwasusedtoselectthesignificant variablesinvolvedwithlengthofhospitalstayofnewborns, whereas the forward method was used in the univari-ate analysis, considering a significance level of 25%. The Mann---Whitney test was used for the univariate analysis, andtime wasstratified untildischarge over the categori-calvariables,whereasSpearman’scorrelationtestwasused to associate time until discharge with other quantitative variables.
The selected variableswere usedin the multiple Pois-sonregression,applyingthebackwardmethod,withalevel ofsignificanceof 5%.Thefinal regression,afterthe back-wardandforwardprocedures,wastermedstepwisePoisson regression.Thequasi-likelihoodmethod7,8wasusedforthe phenomenaofover-orunder-dispersionformodel estima-tion,allowing the estimation of robust variance tothese phenomena.Nagelkerke9pseudoR2wascalculatedfor
logis-ticregression,whileR2adjustedtolog-linearmodels10 was calculatedforPoissonregression.
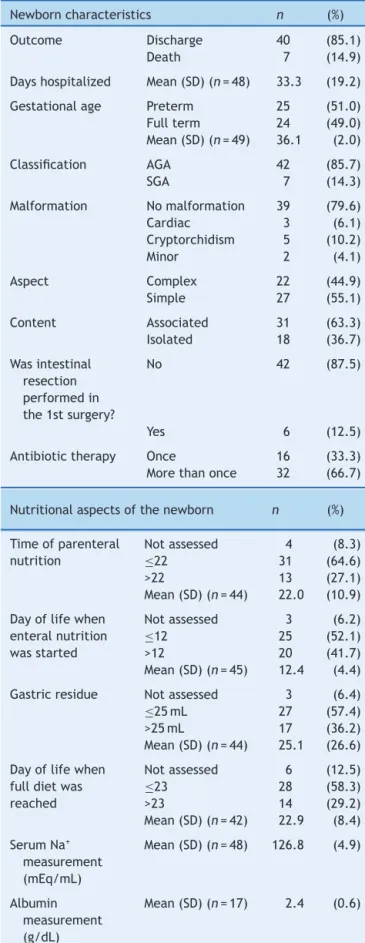
Table1 Frequencyanddescriptivemeasuresofthe char-acteristic variables of neonates with gastroschisis and nutritionalaspects,fromJanuary1995toDecember2010.
Newborncharacteristics n (%)
Outcome Discharge 40 (85.1)
Death 7 (14.9)
Dayshospitalized Mean(SD)(n=48) 33.3 (19.2)
Gestationalage Preterm 25 (51.0) Fullterm 24 (49.0) Mean(SD)(n=49) 36.1 (2.0)
Classification AGA 42 (85.7)
SGA 7 (14.3)
Malformation Nomalformation 39 (79.6) Cardiac 3 (6.1) Cryptorchidism 5 (10.2)
Minor 2 (4.1)
Aspect Complex 22 (44.9) Simple 27 (55.1)
Content Associated 31 (63.3) Isolated 18 (36.7)
Wasintestinal resection performedin the1stsurgery?
No 42 (87.5)
Yes 6 (12.5)
Antibiotictherapy Once 16 (33.3) Morethanonce 32 (66.7)
Nutritionalaspectsofthenewborn n (%)
Timeofparenteral nutrition
Notassessed 4 (8.3)
≤22 31 (64.6)
>22 13 (27.1) Mean(SD)(n=44) 22.0 (10.9)
Dayoflifewhen enteralnutrition wasstarted
Notassessed 3 (6.2)
≤12 25 (52.1)
>12 20 (41.7) Mean(SD)(n=45) 12.4 (4.4)
Gastricresidue Notassessed 3 (6.4)
≤25mL 27 (57.4)
>25mL 17 (36.2) Mean(SD)(n=44) 25.1 (26.6)
Dayoflifewhen fulldietwas reached
Notassessed 6 (12.5)
≤23 28 (58.3)
>23 14 (29.2) Mean(SD)(n=42) 22.9 (8.4)
SerumNa+
measurement (mEq/mL)
Mean(SD)(n=48) 126.8 (4.9)
Albumin measurement (g/dL)
Table1 (Continued)
Nutritionalaspectsofthenewborn n (%)
Interruptedthe dietafteritwas started
No 35 (72.9)
Yes 13 (27.1)
Weight Mean(SD)(n=49) 2,414.0 (552.1)
Weightat discharge
Mean(SD)(n=46) 2,790.9 (571.1)
Discharge weight/birth weightratio
Gained 39 (84.8)
Lost 7 (15.2)
Mean(SD)(n=46) 1.18 (0.19)
This study was approved by the Ethics Committee of UFMG.
Results
The characteristicsof newbornswithgastroschisis submit-ted to primary closure and the variables related to their nutritionalstatusareshowninTable1.
Sevennewbornswhodiedwereidentified,corresponding to14.9%ofthenewborns.Themeanlengthofhospitalstay was33.3days.
Regardingtheclassificationofweightinrelationto gesta-tionalage,14.3%ofthenewbornswereclassifiedassmallfor gestationalage(SGA)and85.7%wereclassifiedasadequate forgestationalage(AGA).
Consideringthatallneonates withgastroschisisreceive atleastoneinitialcourseofantibioticsduring hospitaliza-tion,66.7%ofinfantsinthisstudyreceivedmorethanone antibiotictherapycycle.
The parenteralnutritiontimeof64.6%ofthenewborns was≤22days.Gastricresiduewas≤25mLinthelast24h beforethestartofenteralnutritionin57.4%ofnewborns. Asfortheageofstartofenteralfeeding,52.1%ofnewborns startedenteraldietuntilthe12thdayoflife,and58.3%of thenewbornsreachedfulldietwithinanaverageof23days. ThemeanvaluefoundforserumNa+was126.8mEq/mL,
whereas the mean value for serum albumin levels was 2.4g/dL.
In27.1%oftheinfants,enteralnutritionwasinterrupted afteritsstartduetoabdominaldistension,biliousvomiting, or bowel movement interruption. Regarding the weight, 15.2%ofnewbornshadweightlossfrombirthuntildischarge ordeath.
Newborns whodied veryearly,evenbeforethe period ofparenteralandenteralnutritionintroduction,couldnot have their nutritional characteristics assessed and were excluded fromtheanalysis.At13 daysoflife, 90%of the newborns werealive,whereasat 30 days,atleast 50%of theinfantswerestillhospitalized.
At thehospitalstay analysis,theresultswerearranged according to the newborn and nutritional characteristics (Table2).
Forthegeneralcharacteristics relatedtonewborns,no significantvariablecouldbeassociatedtohospitallengthof stay.
Regardingtheassessednutritionalaspects,itwas possi-bletoidentifythefollowingvariables(withsignificantvalue,
p<0.05)toexplainthelengthofhospitalstay:‘‘Interrupted theenteraldietafteritsstart,’’‘‘Weightatdischarge/birth weightratio,’’‘‘Parenteralnutritiontime,’’and‘‘Dayoflife whenthenewbornreachedfulldiet’’(Table3).
Subsequently,these variables wereapplied in multiple Poissonregression;theregressionmodelisshowninTable4. Using pseudo R2 (multiple regression), it wasobserved
that 82.7% of the total variability of length of hos-pital stay until discharge was explained by the varia-bles: ‘‘Classification,’’ ‘‘Antibiotic therapy,’’ ‘‘Discharge weight/birthweight ratio,’’ ‘‘Parenteral nutrition time,’’ ‘‘Dayoflifewhenneonatestartedenteralnutrition,’’and ‘‘Dayoflifewhenneonatereachedfulldiet.’’
NewbornsclassifiedasSGAhadameanlengthofhospital stay 24.2% longerthan the infants whowere classified as AGA.Those whoreceived more than one antibiotic cycle showedameanlengthofstay16.5%longerthannewborns thatunderwentonlyonecycle.
Foreach extraday beforestarting enteralfeeding,the meanlengthofstayincreasedby2.1%.
Foreachextradaybeforereachingfulldiet,themean hospitalstaydecreasedby3.6%.
Foreachextradayreceivingparenteral nutritiontime, the mean timefrom admission to discharge increased by 5.4%.
Discussion
Inthis study,the most relevant characteristics that influ-enced the length of hospital stay of newborns were: (1) weight classification for gestational age (SGA newborns); (2)useoftwoormoreantibioticcyclesduring hospitaliza-tion;(3)theassociation betweenthenewborn’sweightat dischargeandthenewborn’sbirthweight;(4)timeof par-enteralnutrition administration; (5) day of life when the newbornstartedenteralnutrition;(6)dayoflifewhenthe newbornreached fulldiet; (7)the interruptionof enteral diet.
Adequate fetal growth, especially in late pregnancy, dependsonthenormalfunctionofthegastrointestinaltract, which may not occur in gastroschisis.11 In this study, the meanlengthofhospitalstay ofnewborns classifiedasSGA washigherthaninAGAnewborns.
It is known that one of the common complications amongnewborns withgastroschisis is intrauterinegrowth restriction (IUGR),12 which manifests as low birth weight (≤2500g).11 The lower fetalgrowth can beinfluenced by lossofnutrientsandproteinsthroughtheintestinalexposure toamnioticfluid,withasecondarynutritionaldeprivation13 causingalowertolerancetotheprogressionofenteral feed-ing,requiringlongertimeofparenteralnutritionandthus, longerhospitalstays.
Table2 Univariateanalysisofthecharacteristicsofnewbornswithgastroschisis,fromJanuary1995toDecember2010.
Newborncharacteristics n 2ndQ 1stQ 3rdQ p-value
Gender Female 25 31.0 25.0 38.0
0.502
Male 15 27.0 23.0 36.0
Gestationalage Preterm 20 30.5 24.0 48.5
0.465
Fullterm 20 30.5 24.0 35.5
Coefficientofcorrelation 40 r=−0.009 0.956
Liquid Absent 2 22.5 19.0 26.0
0.320
Clear 15 31.0 23.5 38.5
Meconial 21 31.0 24.0 38.0
Apgar--- 1strange <4 8 28.0 22.0 41.5
0.748
>4 32 30.5 2.5 38.0
Coefficientofcorrelation 40 r=−0.020 0.902
Apgar---5thrange <6 1 25.0 25.0 25.0
0.544
>6 39 31.0 24.0 38.0
Coefficientofcorrelation 40 r=−0.152 0.347
Classification AGA 35 27.0 24.0 36.5
0.072
SGA 5 38.0 36.0 38.0
Malformation Without 32 28.0 24.0 38.0
0.352
With 8 31.5 29.0 50.0
Paraumbilicallocation Right 37 31.0 24.0 38.0
0.483
Left 2 25.5 25.0 26.0
Aspect Complex 16 30.0 26.0 38.0
0.507
Simple 24 30.5 23.5 38.5
Content Associated 26 31.5 25.0 38.0
0.132
Isolated 14 25.5 22.0 32.0
Defectsize(cm) Coefficientofcorrelation 36 r=0.033 0.847
Timetothe1stintervention(hours) Coefficientofcorrelation 40 r=−0.197 0.224
Wasintestinalresectionperformedin the1stsurgery?
No 37 30.0 24.0 38.0
0.425
Yes 3 39.0 30.5 68.0
Wasanotherinterventionperformed duringfollow-up?
No 37 30.0 24.0 38.0
0.250
Yes 3 90.0 56.0 93.5
Mechanicalventilation Coefficientofcorrelation 40 r=0.124 0.444
Antibiotictherapy Once 11 25.0 23.0 27.0
0.076 Morethanonce 29 32.0 25.0 39.0
Musclerelaxant No 9 39.0 22.0 45.0
0.559
Yes 31 30.0 24.5 35.5
Shock No 17 26.0 24.0 38.0
0.294
Yes 22 31.5 26.0 38.0
AGA,adequateforgestationalage;SGA,smallforgestationalage.
Themeanlengthofstayofnewbornswhoreceivedmore thanonecycleofantibiotictherapywaslongerthanthose who received only one in the present study. The use of antibiotics in infants with gastroschisis is aimed toward reducingthecontaminationoftheexternalizedbowel.5The useofmorethanonecycle ofantibioticsisrelatedtothe higher number of infections affecting the newborn. The occurrence of infectionin theneonatal period is directly relatedtothedelayindietintroduction,andtheprolonged timeoftotalparenteralnutritionandcentralvenousaccess devices.
Also,thehighertheratiobetweenthedischargeweight andbirthweight,thelongerthelengthofhospitalstay.This occursbecausetheneonatewithlongerhospitalizationgains moreweightwhileundergoinghospitalcare,reflectingthe adequacyofnutritionalsupportduringhospitalization.
Table3 Univariateanalysisofvariablesrelatedtothenutritionalaspectsofneonateswithgastroschisis,fromJanuary1995 toDecember2010.
Nutritionalaspectsofnewborns n 2ndQ 1stQ 3rdQ p-value
Interruptedthedietafteritsstart
No 30 26.5 23.0 32.0 0.001
Yes 10 48.5 38.0 66.0
Birthweight
<2500g 24 33.0 25.5 42.5 0.094
>2500g 16 26.0 24.0 31.5
Coefficientofcorrelation 40 r=−0.297 0.063
Weightatdischarge
Coefficientofcorrelation 40 r=0.113 0.486
Dischargeweight/birthweightratio
Gainedweight 35 31.0 25.0 38.5 0.054
Lostweight 5 21.0 19.0 31.0
Coefficientofcorrelation 40 r=0.626 0.000
Timeofparenteralnutrition
Coefficientofcorrelation 40 r=0.641 0.000
Dayoflifewhenenteralnutritionwasstarted
Coefficientofcorrelation 40 r=0.294 0.065
Gastricresidue
Coefficientofcorrelation 40 r=0.174 0.290
Dayoflifewhenfulldietwasreached
Coefficientofcorrelation 40 r=0.609 0.000
SerumNa+measurement(mEq/mL)
Coefficientofcorrelation 40 r=−0.179 0.272
Albuminmeasurement(g/dL)
Coefficientofcorrelation 13 r=−0.196 0.522
Table4 StepwisePoissonregressionanalysiswithrobustvarianceforhospitalstayofnewbornswithgastroschisis,fromJanuary 1995toDecember2010.
StepwisePoissonregression p-value Exp(ˇ) 95%CI
Classification=AGA
Classification=SGA 0.033 1.242 1.026;1.505
Antibiotictherapy=once
Antibiotictherapy=morethanonce 0.045 1.165 1.009;1.345 (Dischargeweight/birthweightratio)×100 0.015 1.006 1.001;1.011
Timeofparenteralnutrition 0.000 1.054 1.034;1.075 Dayoflifewhenenteralnutritionwasstarted 0.015 1.021 1.005;1.037 Dayoflifewhenfulldietwasreached 0.000 0.964 [0.947;0.982]
PseudoR2=82.67%.
AGA,adequateforgestationalage;SGA,smallforgestationalage.
24and67days.4 Inthepresentstudy,themeanlengthof stay was33 days andthe timeto reachfull diet was, on average,22daysoflife.
In thisstudy,newborns whohadintolerancetoenteral nutrition after its start, (manifested by abdominal dis-tention, vomiting, massive bilious gastric stasis, and interruption/decreaseof gasesandfeceselimination) had
longerhospital stays, comparedto newborns that had no interruptionoftheenteraldietadministration.
A longer length of hospital stay is observed in gas-troschisisduetocomplicationsandassociatedmorbidities, increasinghospitalmedicalcosts andaffecting the family lifeoftheseneonates.
Itisnoteworthythatdelayintheintroductionofenteral feedingbecomesafactorthatincreasesthelengthof hospi-talstayoftheseneonates;however,afterdietintroduction, thesupplyofthetotalrequiredvolumeshouldnotbe accel-erated.Aslowincreaseinthedietvolumeissuggestedeach day,asrapidincreasesinvolumearenotfavorable.Thishas alsobeendemonstratedbythestudiesperformedby Walter-Nicoletetal.18 Theseauthorsstatedthattheintroduction ofearlyminimal enteraldiet(lowvolumeprovidedatthe samerate for at least fivedays)can promote thegrowth of intestinal mucosa, optimize the maturation of intesti-nalmusclefunction,increasethereleaseofhormonesand localpeptides,andaltertheintestinalflora.Thus,enteral nutritionmanagementhelpstoreducecomplicationsof par-enteralnutrition and accelerate the tolerance to enteral nutrition.
Thisstudyshowedthatnewbornsstartedtheenteraldiet withvaryingamountsofgastricresidue;thisvariablewasnot significantfortheoutcome.Therefore,thestartofenteral dietshouldnotbe delayedbased solelyonthe volumeor biliousaspectofgastricdrainage.
Other authors have also studied the impact of early enteralnutritioninthepostoperativeoutcomeofnewborns withgastroschisis.19,20 Aljahdalietal.19 observed abetter evolution when diets were initiated seven days after the abdominalwallclosure.Sharpetal.20 foundthatforevery dayofdelayofthestartofenteralnutrition,therewasan increaseinthelengthofstay of1.05daysandanincrease inthedurationofenteralnutritionof1.06days.
In this study, the best outcomes were obtained in neonateswhostartedenteralnutritionwithin12daysoflife. Arnonetal.21statedthatSGAnewbornsbenefitedfromearly enteral nutrition (beginning within the first 24h of life), resultinginlowerhospital staywhen comparedtoinfants whostartedthedietlater.
Severalstudieshave aimedtoevaluate theimportance ofhydrationstatusandserumsodiummeasurementandits management,aswellasthedegreeofmalnutrition (hypoal-buminemia)inpatientswithgastroschisiswiththeoutcome observedinthesepatients.17,22,23 Inthepresentstudy,the occurrenceof hyponatremiaandhypoalbuminemia related totheseverityandthedegreeofinitialhypercatabolismof thenewborndid notcorrelate withhospitalstay. Dataon albuminmeasurementwasfoundforonly17infants, show-ingthatintheHC---UFMG,until2010,theevaluationofthis parameterwasnotpartofroutinecarefornewborns with gastroschisis.Thefailuretocompletethemedicalrecords withthisinformationisalimitingfactor,makingitdifficult toattainabetterevaluation.
Althoughthisstudywasconductedwitha16-yearcohort, thenumberof patientsinvolved wassmall,whichhinders theextensionoftheresultstootherpopulations. Further-more,theinvolvementofasinglestudycentercontributes tothesmallsample,evenconsideringtheincreasing preva-lenceofgastroschisisinrecentyears.
An important bias to be considered is the fact that data collection was obtained from non-electronic and non-standardizedmedicalrecords.Inthistypeofcollection,
theinformationisscatteredinthefileandabsentinsome cases,asitdependsontheexaminer’snotesatthetimethe eventsoccurred.
Thedecisiontostudypatientswithgastroschisis submit-tedonlytoprimarysurgicalclosurewasmadeinanattempt toidentifyfactorsrelatedtothelengthofstayspecificfor thisgroupofinfants,whoaremorelikelytoreceive early enteral feeding,as theydo not requirea second surgical procedure,characteristicofthestagedcorrection.
Themortalityrateofnewbornswithgastroschisisislow, between5%and10%,asshownbySnyder24andDriveetal.25 However,inthis study,mortality washigher(14.9%) when compared with the results from developed countries.24,25 In the seven newborns who died, this outcome occurred veryearly,beforetheseventhdayoflife,andthus,there wasnotenoughtimetoassesstheimplementednutritional measures.
Inconclusion, this study demonstratesthat the earlier enteraldietisstarted(≤12days)andtheslowerfullenteral feedingis reached (>23days),thebettertheprognosis of thenewbornandtheshorterthehospitallengthofstay.The authors emphasize the importance of small, gradual vol-ume increasestoimprovethe newborn’s tolerance tothe diet.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Franc¸aE,LanskyS,RêgoMA,CamposD,AbreuDM, Vasconce-losAM.Mudanc¸anoperfildecausasdemortalidadeinfantilno Brasilentre1996e2011:porqueavaliarlistasdeclassificac¸ão dascausasperinatais.Montevideo,Uruguay:VCongresoda Aso-ciaciónLatinoamericanadePoblación-ALAP;2012.
2.CurryJI,MckinneyP,ThorntonJG,StringerMD.Theaetiology ofgastroschisis.BJOG.2000;107:1339---46.
3.IslamS.Clinicalcareoutcomesinabdominalwalldefects.Curr OpinPediatr.2008;20:305---10.
4.ReigstadI,ReigstadH,KiserudT, BerstadT.Pretermelective caesareansection and earlyenteral feedingin gastroschisis. ActaPaediatr.2011;100:71---4.
5.MirandaME,TatsuoES,GuimarãesJT,PaixãoRM,LannaJCBD. Use ofa plastic hemoderivate bag in thetreatment of gas-troschisis.PediatrSurgInt.1999;15:442---4.
6.Efroymson MA. Multiple regression analysis. Mathematical methodsfordigitalcomputers,vol.1.NewYork:Wiley;1960. 7.Wedderbun RW. Quasilikelihood functions, generalized
lin-ear models and the Gauss-Newton method. Biometrika. 1974;61:439---47.
8.McCullagh P,Nelder JA. Generalized linear models. London: ChapmanandHall;1989.
9.NagelkerkeN.Anoteonageneraldefinitionofthecoefficient ofdetermination.Biometrika.1991;78:691---2.
10.Cameron AC, Windmeijer FA. R2 measures for count data regressionmodelswithapplications.JBusEconStat.1996;14: 209---20.
12.Puligandla PS, Janvier A, Flageole H, Bouchard S, Mok E, LabergeJM.Thesignificanceofintrauterinegrowthrestriction isdifferentfromprematurityfortheoutcomeofinfantswith gastroschisis.JPediatrSurg.2004;39:1200---4.
13.Hunter AG, Stevenson RE. Gastroschisis: clinical presenta-tion and associations. Am J Med Genet CSemin Med Genet. 2008;148c:219---30.
14.SkarsgardED,ClaydonJ,BouchardS,KimPC,LeeSK,Laberge JM,etal.CanadianPediatricSurgicalNetwork:aanalyzing sur-gicalbirthdefects.Thefirst100casesofgastroschisis.JPediatr Surg.2008;43:30---4.
15.Murphy FL, Mazlan GC, Tarheen F, Corbally MT, Puri P. Gastroschisis and exomphalos in Ireland 1998---2004. Does antenatal diagnosis impact on outcome? Pediatr Surg Int. 2007;23:1059---63.
16.LoggeHL,MasonGC,ThorntonJG,StringerMD.Arandomized controlledtrial ofelective pretermdelivery of fetuses with gastroschisis.JPediatrSurg.2005;40:1726---31.
17.TannuriAC,SilvaLM,LealJG,MoraesAC,TannuriU.Does admin-isteringalbumintopostoperativegastroschisispatientsimprove outcome?Clin(SãoPaulo).2012;67:107---11.
18.Walter-NicoletE,RousseauV,KiefferF,FusaroF,BourdaudN, OucherifS,etal.Neonataloutcomeofgastroschisisismainly influencedbynutritionalmanagement.JPediatrGastroenterol Nutr.2009;48:612---7.
19.AljahdaliA, Mohajerani N,Skarsgard ED. Effect oftimingof enteral feedingon outcome ingastroschisis. J Pediatr Surg. 2013;48:971---6.
20.SharpM,BulsaraM,GollowI,PembertonP.Gastroschisis:early enteralfeedsmayimproveoutcome.JPaediatrChildHealth. 2000;36:472---6.
21.Arnon S,SulamD,Konikoff F,RegevR, Litmanovitz I,Timna N. Very early feeding in stable small for gestational age preterminfants:arandomizedclinicaltrial.JPediatr(RioJ). 2013;89:388---93.
22.Tannuri AC, Silva LM, Leal JJ, Ricardi RR, Tannuri U. Qual éa melhor soluc¸ãode hidratac¸ão parenteral a ser utilizada no tratamento pós-operatório de recém-nascidos com gas-trosquise?ExperiênciadoInstitutodaCrianc¸adoHospitaldas CLínicasdaFaculdadedeMedicinadaUSP.Pediatr(SãoPaulo). 2010;32:84---9.
23.Snyder CW, Biggio JR, Bartle DT,Georgeson KE, Muensterer OJ.Earlyseverehypoalbuminemiaisanindependentrisk fac-tor for intestinal failure in gastroschisis. Pediatr Surg Int. 2011;27:1155---8.
24.SnyderCI.Outocomeanalysisforgastroschisis.JPediatrSurg. 1999;34:1253---6.