www.jped.com.br
ORIGINAL
ARTICLE
Prediction
equations
for
spirometry
in
four-to
six-year-old
children
夽
Danielle
Corrêa
Franc
¸a
a,
Paulo
Augusto
Moreira
Camargos
b,
Marcus
Herbert
Jones
c,
Jocimar
Avelar
Martins
d,
Bruna
da
Silva
Pinto
Pinheiro
Vieira
e,
Enrico
Antônio
Colosimo
f,
Karla
Morganna
Pereira
Pinto
de
Mendonc
¸a
g,
Raíssa
de
Oliveira
Borja
g,
Raquel
Rodrigues
Britto
e,
Verônica
Franco
Parreira
e,∗aRehabilitationSciencesGraduateProgram,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil bPediatricPulmonologyUnit,HospitalUniversitário,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil cPediatricRespirologyDivision,HospitalSãoLucas,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,
RS,Brazil
dHospitalArnaldoGavazza,PonteNova,MG,Brazil
ePhysiotherapyDepartment,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil fDepartmentofStatistics,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil gPhysiotherapyDepartment,UniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil
Received26March2015;accepted19October2015 Availableonline7May2016
KEYWORDS
Spirometrychildren; Child;
Predictionequations; Qualitycontrol; Preschool; Equipment
Abstract
Objective: Togeneratepredictionequationsforspirometryin4-to6-year-oldchildren. Methods: Forcedvital capacity,forcedexpiratoryvolume in0.5s,forcedexpiratoryvolume inonesecond,peakexpiratoryflow,andforcedexpiratoryflowat25---75%oftheforcedvital capacitywereassessedin195healthychildrenresidinginthetownofSeteLagoas,stateofMinas Gerais,SoutheasternBrazil.Theleastmeansquaresmethodwasusedtoderivetheprediction equations.Thelevelofsignificancewasestablishedasp<0.05.
Results: Overall, 85% of the children succeeded inperforming the spirometric maneuvers. In the prediction equation, height was the single predictor of the spirometric variables as follows: forced vital capacity=exponential [(−2.255)+(0.022×height)], forced expira-tory volume in 0.5s=exponential [(−2.288)+(0.019×height)], forced expiratory volume in onesecond=exponential [(−2.767)+(0.026×height)],peak expiratory flow=exponential
夽
Pleasecitethisarticleas:Franc¸aDC,CamargosPA,JonesMH,MartinsJA,VieiraBP,ColosimoEA,etal.Predictionequationsforspirometry infour-tosix-year-oldchildren.JPediatr(RioJ).2016;92:400---8.
∗Correspondingauthor.
E-mails:[email protected],[email protected](V.F.Parreira).
http://dx.doi.org/10.1016/j.jped.2015.10.005
0021-7557/©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
Predictionequationsforspirometricparameters 401
[(−2.908)+(0.019×height)],andforcedexpiratoryflowat25---75%oftheforcedvital capac-ity=exponential[(−1.404)+(0.016×height)].Neitheragenorweightinfluencedtheregression equations.Nosignificantdifferencesinthepredictedvaluesforboysandgirlswereobserved. Conclusion: The predicted values obtained in the present study are comparable to those reportedforpreschoolersfrombothBrazilandothercountries.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Espirometriainfantil; Crianc¸a;
Equac¸õesde predic¸ão; Controlede qualidade; Pré-escola; Equipamentos
Equac¸õesdepredic¸ãodaespirometriaemcrianc¸asdequatroaseisanos
Resumo
Objetivo: Gerarequac¸õesdepredic¸ãodaespirometriaemcrianc¸asdequatroaseisanos. Métodos: Capacidadevitalforc¸ada,volumeexpiratórioforc¸adoem0,5segundo,volume expi-ratórioforc¸adoem1segundo,picodefluxoexpiratórioefluxoexpiratórioforc¸adocom25-75% dacapacidadevitalforc¸adaforamavaliadosem195crianc¸assaudáveisqueresidemnacidade deSeteLagoas,EstadodeMinasGerais,SudestedoBrasil.Ométododosmínimosquadrados foiusadoparaderivarasequac¸õesdepredic¸ão.Oníveldesignificânciafoiestabelecidocomo p<0,05.
Resultados: Nogeral,85%dascrianc¸asforambem-sucedidasaofazerasmanobras espirométri-cas. Na equac¸ão de predic¸ão, a estatura foi a única variável preditora das variáveis espirométricas,daseguinteforma:capacidadevitalforc¸ada=exponencial[(-2,255)+(0,022 x estatura)], volume expiratório forc¸ado em 0,5 segundo = exponencial [(-2,288) +(0,019 x estatura)], volume expiratório forc¸ado em 1 segundo = exponencial [(-2,767) + (0,026 x estatura)],picodofluxoexpiratório=exponencial[(-2,908)+(0,019xestatura)]efluxo expi-ratório forc¸ado com25-75%da capacidade vital forc¸ada= exponencial [(-1,404)+(0,016 x estatura)].Nemaidadenemopesoinfluenciaramasequac¸õesderegressão.Nãofoiobservada diferenc¸asignificativanosvaloresprevistosemmeninosemeninas.
Conclusão: Osvaloresprevistosobtidosnesteestudosãocomparáveisàqueles relatadosem crianc¸asemidadepré-escolartantodoBrasilquantodeoutrospaíses.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Pulmonary functiontestssupplement theclinical histories and physical examinations of individuals with respiratory problems and contribute to the diagnosis, prognosis, and monitoring ofrespiratory diseases,aswell asassessments ofthetherapeuticeffectsofinterventions.1
Spirometryisauniversallyacceptedmethodforassessing pulmonaryfunction,includinglungvolumesandflows,andis themostwidelyusedmethodfordetectingfunctional alter-ations in the pulmonary functions of adults, adolescents, andschoolchildren.1,2However,spirometryhasnotyetbeen widely studied in Latin American or Brazilian preschool populations.1,3
The earliest studies that assessed spirometric maneu-versinpreschoolerswerepublishedapproximately20years ago.4,5Currently,itiswellestablishedintheliteraturethat 75---86% ofpreschoolers areabletoacceptablyand repro-duciblyperformspirometricmaneuvers1,3,6---10 asevidenced by the availability of prediction equations for preschool-ers from several countries.6,8,9,11---17 Additionally, a recent multicenterstudy16proposedpredictionequationsfor spiro-metricvariablesfrompreschoolersbasedondatacollected from the children from 11 different countries (n=3777),
including Brazil. An update was published in 2012 and included new multi-ethnic equations.18 Recently, Burity et al.19 described reference values based on 135 north-easternBrazilianpreschoolersandidentifiedheightandsex aspredictorsof lungfunctionparameters.However,these equationsarenot necessarilyrepresentative ofthe entire populationofBrazilianpreschoolers.
Duetotheimportanceofspirometryinallagegroupsand thescarcityof predictionequations for spirometric varia-blesforpreschoolersinBrazil,thepresent studyaimedto describethepredictionequationsforspirometryin4-to 6-year-oldchildrenresidinginthetownofSeteLagoas,state ofMinasGerais,southeasternBrazil.
Methods
Settingandsampling
DiseaseATS/DLD/78/C-questionnaire(i.e.,totalscoresthat are equal to or lower than 6)6,20; body mass index (BMI) betweenthe3rdand95thpercentilesforage21;birthweight greaterthan2500gatagestationalageof37---42weeks20; nofluepisodeswithintheprevioussevendays;nohistoryof maternalsmokingduringpregnancyorexposuretotobacco smokingover the years preceding the spirometric assess-ment;nopasthistoryofthoracicorabdominalsurgery;no thoracicmalformations,geneticsyndromes,metabolic dys-functions,heart diseases,neuromusculardiseases, mental disorders,orcognitivedeficits;andnouseofmedicineson aregularbasis.
The study protocol and informedconsent (providedby theparentsorlegalguardians)wereapprovedbytheEthics inResearchCommitteeoftheUniversidadeFederaldeMinas Gerais(ETICNo.0612.0.203.000-09).
Measurementinstrumentsandprocedures
The ATS-DLD-78-C questionnaire wasused torule outthe presenceof respiratorydiseases and exposureto environ-mentalpollutants.Thisquestionnaireconsistsofquestions about the symptoms, other illnesses and hospitalizations relatedtorespiratorytractdiseases,anditwascompleted bytheparentsorlegalguardians.Theoverallscoresranged from0to22, andscores greater thanor equal to7were indicativeofachronicrespiratorydisease.6Supplementary questions, for example, questions about gestational age, the neonatalperiod and concomitant diseases, were also included.
A handheld Koko spirometer (Koko®, PFT type; nSpire
HealthInc., CO, USA) wasused toassess thespirometric variablesobtainedfromthe forcedexpiratorymaneuvers. This equipment meets all of the requirements of the ATS/ERS1anddisplaysreal-timegraphsoftheflow/volume andvolume/time curves.Following the ATS recommenda-tions,adisposablemouthpieceandantibacterialfilterthat togetherresultin adeadspace oflessthan2mL/kgwere used. The accuracy of the equipment was verified daily
viacalibrationusingathree-litermanualsyringe(COSMED, PulmonaryFunctionEquipment---Italy).Thefollowing spiro-metricvariableswereanalyzed:FVC,FEV0.5,FEV1,FEF25---75,
andPEF.Thedatafortheforcedexpiratorytime(FET)and back-extrapolatedvolume(BEV)were collectedtoensure thequalitiesofthecurves.1
The data from all of the questionnaires were ana-lyzed,andthechildrenwhomettheinclusioncriteriawere invited to participate in the study. Children whose par-ents/guardiansauthorized theirparticipation inthe study andsignedaninformedconsentformwereassessedduring regularschoolactivities.
The physical examinationswereinitiated by measuring theweightusingasinglescale(Filizola---SãoPaulo,Brazil) andtheheightusingaHarpenden®stadiometer(Harpenden
SkinfoldCaliper,MediflexSurgicalProducts,USA) (measure-mentrangefrom60.0cmto210.0cm,wallmounted,witha precisionof0.1cm,withthechildstanding,barefoot, pos-itionedinsuchamannerthatthehead,shoulders,buttocks, andheelslightlytouchedtheverticalsurfaceof the mea-suring device). Subsequently, blood pressure, heart rate, respiratoryrate, oxygensaturation, andlung auscultation
were assessed,and staticand dynamic inspections of the breathingpatternwereperformed toconfirm theabsence ofanyclinicalabnormality.
To perform spirometry, the recommended acceptabil-ityandreproducibilitycriteriawerefollowed.1Beforethe test, eachchild receivedage-appropriateinstructions and then performed the maneuvers. The measurements were collectedwiththesubjectseatedusingadisposable well-adjusted mouthpiece(to preventleaks), a nose clip, and computer-animation programs that provided instructions andstimulitotheparticipants.2Thesubjectswereaskedto breatheinthetidalvolumeandtheninstructedtofilltheir lungsasmuchaspossibleandblowasstrongly,rapidlyand longaspossible.Theacceptabilitycriteriawereasfollows: the flow-volume andvolume-time curves were inspected, andmaneuversthatwerevisiblyinadequatewereexcluded,
i.e.,whentheflow-volumecurvedidnotexhibitarapidrise tothepeakflowandasmoothdescendinglimbwithno evi-dence ofacough orglottic closure;theBEVwasequalor lowerthan80mLorlowerthan12.5%oftheFVC;andthe FETwasgreaterthan10%ofthePEFrate.The reproducibil-itycriteriawereasfollows:thedifferencebetweentheFVC and FEV1 was lower than 10% or 100mL for at least two
reproduciblemaneuvers.1Thetestwaslimitedto20minto ensureclinicalapplicability,andthesubjectswereallowed oneminuteofrestbetweentwoconsecutivemaneuversthat wereconductedbythesameinvestigator(DCF)in all sub-jects.
Thevolume---timeandflow---volumecurveswerevisually examinedbytwoindependentobserverswhowereblinded to the children’s past and current health status. Specifi-cally,themaximumvaluesoftheFVC,FEV0.5,FEV1,andPEF
wereobtainedusingtheappropriateandreproduciblecurve (themaximumvaluesforeachofthevariablescouldcome fromdifferentcurves).TheFEF25---75valuewasselectedfrom
thecurvethatexhibitedthelargestsumof FVCandFEV1,
andtheFEV0.5valuewasobtainedfromthecurvewiththe
greaterFEV1valueorthegreaterFEV0.5whentheFETwas
≤1s.1
Statisticalanalysis
Accordingtotheageranges(i.e.,48---59,60---71,and72---83 months)andsex(boysandgirls),180healthypreschoolers werearbitrarilypre-definedwithinthetargetagerangeas theminimumthatshouldbeassessedinthepresentstudy. Acluster randomizationwasperformed basedonthe offi-cial list of the existing public and private schools in the cityofSeteLagoas.Elevenschoolswererandomlyselected (sevenpublicandfourprivateinstitutions)while maintain-ingapublic/privateschoolratioof1.75,which wasbased ontheproportionsofregisteredstudents.Then,all4-to 6-year-oldchildrenregisteredineachschoolwereinvitedto participateinthestudy.
Predictionequationsforspirometricparameters 403
theanthropometricdataandvariablesfromthepulmonary functiontestsbetweenthe4-to6-year-oldchildren.
Togeneratethepredictionequationsforthespirometric variables,theleastmeansquaresmethodwasused.First, logarithmictransformations wereappliedtothe spiromet-ricvariableswithBox---Coxanalyses.Linearregressionswere performed betweenthespirometric(dependent) variables and the height, weight, sex, and age (exploratory varia-bles).Then,amultipleregressionanalysiswasperformed. Following the evaluation of the multiple regression anal-ysis, the normality and homoscedasticity of the residuals wereestablishedusingQ---Qplots.Theresidualassumptions weresatisfied.Theresultswereexpressedasz-scores,i.e., multiplesof the standard deviationof the mean,and the graphswiththeregressioncurvesandz-scoreswereplotted tofacilitatetheuseoftheequationsinclinicalpracticeand research.
Alltestswereassessedatanalphaof0.05withno adjust-ments for multiple comparisons. The data were analyzed usingtheRstatisticallanguage(FreeSoftwareFoundation --- Boston,MA,USA)andSPSS(SPSSInc.Released2009.SPSS forWindows,Version15.0,IL,USA).
Results
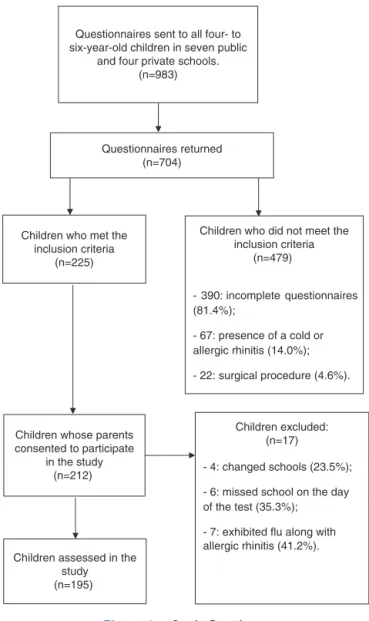
Fig. 1 depictsthe study flowchart and indicates that 195 children were initiallyassessed andthat 131 (67%) public schooland64(33%)privateschoolstudentswereenrolledin thestudyfromJune2010toAugust2011.
Table 1 presents the coefficients of determination (r2)
of the regression equations for the spirometric variables withtheindependentvariables ofheight, height+weight, height+age,andheight+weight+age.Ther2values
exhib-ited little variation (approximately 1%) when height was used as the single predictor of the spirometric variables withheight+weight+age as the independentvariables in theregressionequations.Table1alsopresentsthe regres-sion equations and the lower normal limits (i.e., −1.64
z-scores) for the spirometric variables withheight as the singlepredictor.
The linear regression between the spirometric param-eters (dependent variables) and height, weight, and age (independentvariables)exhibitedastatisticallysignificant association. However, the spirometric variables did not presentastatisticallysignificantassociationwithsex.
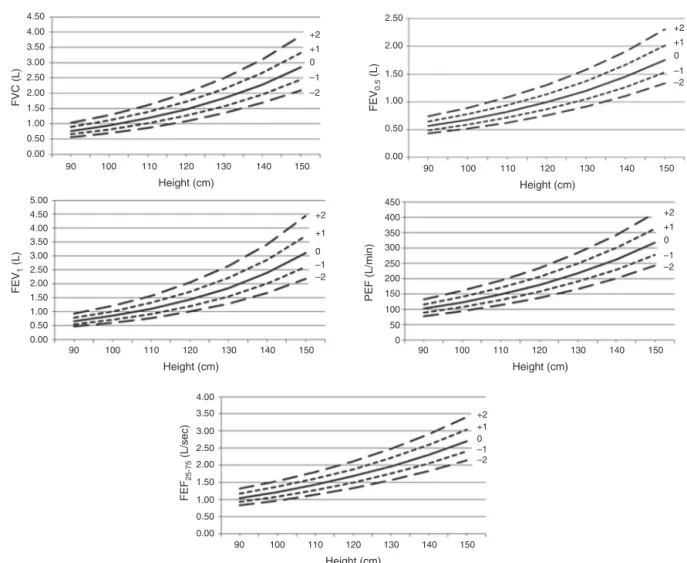
The graphs of the spirometric variables according to height in which the z-scores are plotted and shown in Fig. 2. As illustrated, shorter heights were associated withless variabilityin eachofthespirometricparameters studied.
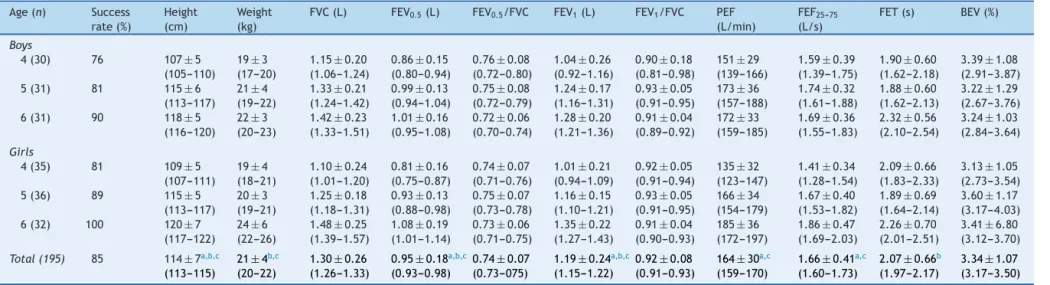
Table 2 presents the proportion of children who suc-cessfully performed spirometry, the anthropometric data, and the spirometric parameters by age of the 195 chil-dren. Overall, 85% of thechildren successfully performed the spirometricmaneuvers,and thesuccess rate progres-sivelyincreasedwithage.Thesamplefromwhichthecurves weregenerated and theequations were derived was pre-dominantlyofmixedethnicity(134outof166,i.e.,80.7%), white(27outof166,i.e.,16.3%),andthoseAsian/African descendants(onlyfiveoutof166,i.e.,3.0%).This informa-tionwasobtainedfromparents’report.Thecomparisonsof
Questionnaires sent to all four- to six-year-old children in seven public
and four private schools. (n=983)
Questionnaires returned (n=704)
Children who met the inclusion criteria
(n=225)
Children whose parents consented to participate
in the study (n=212)
Children who did not meet the inclusion criteria
(n=479)
- 390: incomplete questionnaires (81.4%);
- 67: presence of a cold or allergic rhinitis (14.0%);
- 22: surgical procedure (4.6%).
Children excluded: (n=17)
- 4: changed schools (23.5%);
- 6: missed school on the day of the test (35.3%);
- 7: exhibited flu along with allergic rhinitis (41.2%). Children assessed in the
study (n=195)
Figure1 Studyflowchart.
theanthropometricdataandspirometricvariablesbetween the boys and girls did not reveal significant differences (p>0.05,independentt-tests).Nonetheless,theageranges indicatedthatweight,height,and mostofthe pulmonary functionparametersexhibitedprogressiveandstatistically significantincreaseswithage. RegardingtheFET,a signif-icantincreasewasobservedonlyamongthechildren aged 4---6 years. Only the BEV, FVC, FEV0.5/FVC, and FEV1/FVC amongall of theinvestigatedage rangesfailedtoexhibit statistically significant differences according to Hochberg test.
Discussion
Tothebestoftheauthors’knowledge,thepresentreportis thesecondstudydesignedtodescribepredictionequations for spirometricvariables exclusively for Brazilian 4- to 6-year-oldpreschoolers.
Franc
¸a
DC
et
al.
Table1 Coefficientofdeterminationofthemultipleregressionanalyzesforspirometricvariables,consideringtheexplanatoryvariables:height,height+weight,height+age, andheight+weight+age;aswellasthelowerlimitofnormalandpredictionequationsforspirometricvariablesaccordingtoheight.
Spirometricvariables Coefficientofdetermination(r2) Predictionequations Lowerlimitofnormal
H H+W H+A H+W+A
FVC 0.56a 0.57a 0.56a 0.57a Exp[(−2.255)+(0.022×height)] Exp(predictedvalue−0.253)
FEV0.5 0.51a 0.51a 0.51a 0.52a Exp[(−2.288)+(0.019×height)] Exp(predictedvalue−0.225)
FEV1 0.45a 0.44a 0.44a 0.44a Exp[(−2.767)+(0.026×height)] Exp(predictedvalue−0.294)
PEF 0.35a 0.34a 0.35a 0.35a Exp[(−2.908)+(0.019×height)] Exp(predictedvalue−0.220)
FEF25---75 0.24a 0.24a 0.24a 0.25a Exp[(−1.404)+(0.016×height)] Exp(predictedvalue−0.191)
H,height(cm);W,weight(kg);A,age(months);Exp,exponential;FVC,forcedvitalcapacity(L);FEV0.5,forcedexpiratoryvolumein0.5s(L);FEV1,forcedexpiratoryvolumeinone
P rediction equations for spirometric parameters 405
Table2 Anthropometricdata,successrates,andobservedvaluesofthespirometricvariablesaccordingtoage,amongthe195assessedchildren.
Age(n) Success
rate(%)
Height (cm)
Weight (kg)
FVC(L) FEV0.5(L) FEV0.5/FVC FEV1(L) FEV1/FVC PEF
(L/min)
FEF25---75
(L/s)
FET(s) BEV(%)
Boys
4(30) 76 107±5
(105---110)
19±3 (17---20)
1.15±0.20 (1.06---1.24)
0.86±0.15 (0.80---0.94)
0.76±0.08 (0.72---0.80)
1.04±0.26 (0.92---1.16)
0.90±0.18 (0.81---0.98)
151±29 (139---166)
1.59±0.39 (1.39---1.75)
1.90±0.60 (1.62---2.18)
3.39±1.08 (2.91---3.87)
5(31) 81 115±6
(113---117)
21±4 (19---22)
1.33±0.21 (1.24---1.42)
0.99±0.13 (0.94---1.04)
0.75±0.08 (0.72---0.79)
1.24±0.17 (1.16---1.31)
0.93±0.05 (0.91---0.95)
173±36 (157---188)
1.74±0.32 (1.61---1.88)
1.88±0.60 (1.62---2.13)
3.22±1.29 (2.67---3.76)
6(31) 90 118±5
(116---120)
22±3 (20---23)
1.42±0.23 (1.33---1.51)
1.01±0.16 (0.95---1.08)
0.72±0.06 (0.70---0.74)
1.28±0.20 (1.21---1.36)
0.91±0.04 (0.89---0.92)
172±33 (159---185)
1.69±0.36 (1.55---1.83)
2.32±0.56 (2.10---2.54)
3.24±1.03 (2.84---3.64)
Girls
4(35) 81 109±5
(107---111)
19±4 (18---21)
1.10±0.24 (1.01---1.20)
0.81±0.16 (0.75---0.87)
0.74±0.07 (0.71---0.76)
1.01±0.21 (0.94---1.09)
0.92±0.05 (0.91---0.94)
135±32 (123---147)
1.41±0.34 (1.28---1.54)
2.09±0.66 (1.83---2.33)
3.13±1.05 (2.73---3.54)
5(36) 89 115±5
(113---117)
20±3 (19---21)
1.25±0.18 (1.18---1.31)
0.93±0.13 (0.88---0.98)
0.75±0.07 (0.73---0.78)
1.16±0.15 (1.10---1.21)
0.93±0.05 (0.91---0.95)
166±34 (154---179)
1.67±0.40 (1.53---1.82)
1.89±0.69 (1.64---2.14)
3.60±1.17 (3.17---4.03)
6(32) 100 120±7
(117---122)
24±6 (22---26)
1.48±0.25 (1.39---1.57)
1.08±0.19 (1.01---1.14)
0.73±0.06 (0.71---0.75)
1.35±0.22 (1.27---1.43)
0.91±0.04 (0.90---0.93)
185±36 (172---197)
1.86±0.47 (1.69---2.03)
2.26±0.70 (2.01---2.51)
3.41±6.80 (3.12---3.70)
Total(195) 85 114±7a,b,c
(113---115)
21±4b,c
(20---22)
1.30±0.26
(1.26---1.33)
0.95±0.18a,b,c
(0.93---0.98)
0.74±0.07
(0.73---075)
1.19±0.24a,b,c
(1.15---1.22)
0.92±0.08
(0.91---0.93)
164±30a,c
(159---170)
1.66±0.41a,c
(1.60---1.73)
2.07±0.66b
(1.97---2.17)
3.34±1.07
(3.17---3.50)
FVC,forcedvitalcapacity;FEV0.5,forcedexpiratoryvolumein0.5s;FEV0.5/FVC,ratiobetweenFEV0.5andFVC;FEV1,forcedexpiratoryvolumeinonesecond;FEV1/FVC,ratiobetween
FEV1andFVC;PEF,peakexpiratoryflow;FEF25---75,forcedexpiratoryflowat25---75%oftheFVC;FET,forcedexpiratorytime;BEV,back-extrapolatedvolume.
Thedataarepresentedasthemeans±thestandarddeviationswiththe95%confidenceintervals(inparentheses).
a p<0.05betweenthe4-and5-year-oldchildren. b p<0.05betweenthe5-and6-year-olds.
4.50 2.50 2.00 1.50 1.00 0.50 0.00 450 400 350 300 250 200 150 100 50 0 4.00 3.50 3.00 2.50 2.00 1.50 1.00 0.50 0.00 5.00 4.50 4.00 3.50 3.00 2.50 2.00 1.50 1.00 0.50 0.00 4.00 3.50 3.00 2.50 2.00 1.50 1.00 0.50 0.00
90 100 110 120
Height (cm) FVC (L) FEV 1 (L) FEV 0.5 (L) PEF (L/min) FEF 25-75 (L/sec)
130 140 150
+2 +1 0 –1 –2 +2 +1 0 –1 –2 +2 +1 0 –1 –2 +2 +1 0 –1 –2 +2 +1 0 –1 –2
90 100 110 120
Height (cm)
130 140 150 90 100 110 120
Height (cm)
130 140 150
90 100 110 120
Height (cm)
130 140 150
90 100 110 120
Height (cm)
130 140 150
Figure2 Graphs ofthez-scoresfor thespirometricvariablesaccording toheight. FVC,forcedvital capacity;FEV0.5,forced expiratoryvolumein0.5s;FEV1,forcedexpiratoryvolumeinonesecond;PEF,peakexpiratoryflow;FEF25---75,forcedexpiratory flowat25---75%oftheFVC.
maneuvers.In contrast to the present study, the statisti-calanalysesincludedlogarithmicandlinearregressionsand didnotincludetheleastmeansquaresmethod.Thelatter methodallowsfortheconstructionoffunnel-shapedcurves thatbetterreflect thecorrelationsbetween physical lung growthacrosstheanalyzedages(4,5,and6yearsoflife) andfunctionalparameters.
The main results of the present study are the follow-ing:progressiveandstatisticallysignificantincreasesinthe majorityofthespirometricparameterswereobservedwith increasing height, and the resulting prediction equations incorporated height as a single predictor. These results agreewithpreviouslyreportedresults.6,9,15 Thus,the pre-dictionequationsforspirometricvariablesdescribedinthe presentstudyweregeneratedbyconsideringheightasthe single independent variable. This choice of a single pre-dictorwasbasedonthefollowingfactors:thestatistically non-significant variation in the coefficients of determina-tion withthe addition of the other possible independent variables (i.e.,age, weight, and sex), the ease of use of theequationswithsinglepredictorsinclinicalpractice,and the previous use of height as a single independent vari-ablebyseveral authorstoderivepredictionequations for
spirometricparametersamongpreschoolers.6,8,11,13,15 Addi-tionally,thevaluesforthecoefficientofdetermination(r2)
thatwerefoundinthepresentstudy(Table1)aresimilarto thosepreviouslydescribed,9,12,15 includingthoseofastudy thatenrollednortheasternBrazilianpreschoolers.19Overall, ther2valuesreportedintheliteratureforFVCrangedfrom
0.76to0.53;forFEV0.5,from0.73to0.42;for FEV1,from
0.78 to0.55; for PEF,from0.78to0.38; andfor FEF25---75,
from0.37to0.17.9,12,15,19
The graphs of the spirometric variables according to heightinwhichthez-scoreswereplottedreflectthedirect correlations between the spirometric variables and the increaseinheight.Therefore,withaprogressiveincreasein height,thevariablesthatwereassessedinthepresentstudy presentedwidevariability.Thegraphsfrompreviousstudies resembledthoseofthepresentstudyinappearance.16,17
Predictionequationsforspirometricparameters 407
differencesbetweenpreschoolmalesandfemalesandthe smallsamplesize.
Additionally, strong agreements (i.e.,z-scores closeto zero)wereobservedinthecomparisonsofthespirometric valuesgeneratedfromourpredictionequationsandthe val-uesthatwererecentlyreportedbyQuanjerandcoworkers basedon97,759recordsofhealthynonsmokersaged2.5---95 years from around the world.18 For example, the mean
z-scores for the FVC, FEV1, FEV1/FVC ratio, and FEF25---75
obtainedinthepresentstudywere−0.8,−0.00,+0.1,and +0.05,respectively; i.e.,all oftheparametersfell within theacceptedrangeof±0.5z-scores.Inotherwords,these valueswerelowerthanapproximately1---2%ofthepredicted values reported by Quanjer et al.,18 which are clinically irrelevant. However,thepredictionequations proposedin thepresentstudyappeartobemoreapplicableto popula-tions similartothat of thepresent study,simplybecause theseequationsweregeneratedfromsuchapopulation.
ComparedtothereferencevaluesdescribedbyRosenthal etal.4 andBurityetal.19 andaccountingfor thechildren with heights of 110cm, the present predicted values are closetothosethathavebeenpreviouslyreported,i.e.,FVC of 1.20L, 1.10L,and 1.18L,respectively, FEV1 of 1.10L,
1.05L,and1.10L,respectively,andFEV1/FVCof0.90,0.95,
and0.93,respectively.
Oneofthelimitationsofthepresentstudywasthatitdid notinclude3-year-oldchildren,althoughthepreschoolage rangeisconsidered tobeginat thatage.However,access to these children would have been restricted due to the smallnumber of schools in Sete Lagoas, particularly pub-licschools,for childrenyoungerthan4yearsold.Another limitationistherelativelysmallsamplesizeofthisstudy.
In summary,predictionequationsfor spirometric varia-blesweregeneratedfor4-to6-year-oldBrazilianchildren residinginthestateofMinasGerais.Theseresultsmaybe of importance tothe field of pediatric respiratory health becausethesevaluescanbeusedtooptimizethe diagno-sisandclinicalmanagementofchildren withsuspectedor confirmedrespiratorydiseases.Pulmonaryfunctiontestsare importanttoelucidatediagnostic hypothesesandimprove clinical management. Reflecting the importance of their use, these tests are increasingly being used among the preschoolpopulation.Theresultsofthepresentstudymay helptobroadentheuseofspirometryamongpreschoolers, astheseresultscorroboratethefindingsofpreviousstudies thathavereportedhighsuccessratesintheperformanceof spirometricmaneuversby preschoolersandan increasein thesuccessratewithage.3,6,7,9,10,15,22
Given the continental characteristics of Brazil, further studies on this topic across the five macroregions of the countryshouldbeencouraged,andthesestudiesshouldaim to obtain lung function data from a more representative populationofBrazilianchildren.
Funding
Pró-Reitoria de Pesquisa da Universidade Federal de Minas Gerais, Brazil; Brazilian Research Agencies, Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico (CNPq,GrantNo.309494/2013-3[toVFP]and 303396/2012-1[toPAMC]),andFundac¸ãodeAmparoàPesquisadoEstado
de Minas Gerais (FAPEMIG, Grant No. PPM-00065-14 [to PAMC]andPPM-00287-15[toVFP]).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors wish to thank Maria Ângela Gonc¸alves de OliveiraRibeiroandElianeViana Mancuzoforreviewing a preliminaryversionofthemanuscriptandfortheir invalu-ableinput.
References
1.BeydonN,DavisSD,LombardiE,AllenJL,AretsHG,AuroraP, etal.AnofficialAmericanThoracicSociety/European Respira-torySocietystatement:pulmonaryfunctiontestinginpreschool children.AmJRespirCritCareMed.2007;175:1304---45.
2.BeydonN.Pulmonaryfunctiontestinginyoungchildren. Paedi-atrRespirRev.2009;10:208---13.
3.VerasTN,PintoLA.Feasibilityofspirometryinpreschool chil-dren.JBrasPneumol.2011;37:69---74.
4.RosenthalM,BainSH,CramerD,HelmsP,DenisonD,BushA, et al. Lung function in white childrenaged 4---19years: I ---spirometry.Thorax.1993;48:794---802.
5.KanengiserS,DozorAJ.Forcedexpiratorymaneuversin chil-drenaged3---5years.PediatrPulmonol.1994;18:144---9.
6.EigenH,BielerH,GrantD,ChristophK,TerrillD,HeilmanDK, etal.Spirometricpulmonaryfunctioninhealthypreschool chil-dren.AmJRespirCritCareMed.2001;163:619---23.
7.MarosticaPJ,WeistAD,EigenH,AngelicchioC,ChristophK, SavageJ,et al.Spirometryin3-to6-year-old childrenwith cysticfibrosis.AmJRespirCritCareMed.2002;166:67---71.
8.Vilozni D, BarakA, Efrati O, Augarten A, Springer C, Yahav Y, et al. The role of computer gamesin measuring spirom-etry in healthy and asthmatic preschool children. Chest. 2005;128:1146---55.
9.NystadW,SamuelsenSO,NafstadP,EdvardsenE,StensrudT, JaakkolaJJ.Feasibilityofmeasuringlungfunctioninpreschool children.Thorax.2002;57:1021---7.
10.AuroraP,StocksJ,OliverC,SaundersC,CastleR,Chaziparasidis G,et al.Qualitycontrolfor spirometryinpreschoolchildren with and without lungdisease. Am J RespirCrit Care Med. 2004;169:1152---9.
11.Pesant C, Santschi M, Praud JP, Geoffroy M, Niyonsenga T, Vlachos-MayerH. Spirometricpulmonary function in3-to 5-year-oldchildren.PediatrPulmonol.2007;42:263---71.
12.PiccioniP,BorraccinoA,FornerisMP,MiglioreE,CarenaC, Big-naminiE,etal.Referencevaluesofforcedexpiratoryvolumes and pulmonary flows in 3---6year children: a cross-sectional study.RespirRes.2007;8:14.
13.Zapletal A, Chalupová J. Forced expiratory parameters in healthypreschoolchildren(3---6yearsofage).PediatrPulmonol. 2003;35:200---7.
14.American Thoracic Society/European Respiratory Society. ATS/ERSStatementonrespiratorymuscletesting.AmJRespir CritCareMed.2002;166:518---624.
15.JengMJ,ChangHL,TsaiMC,TsaoPC,YangCF,LeeYS,etal. Spirometric pulmonary function parameters of healthy Chi-nese children aged 3---6 years in Taiwan. Pediatr Pulmonol. 2009;44:676---82.
theAsthmaUKCollaborativeInitiative.AmJRespirCritCare Med.2009;180:547---52.
17.QuanjerPH,StanojevicS,StocksJ,HallGL,PrasadKV,Cole TJ, et al. Changes in the FEV1/FVC ratio during childhood and adolescence: an intercontinental study. Eur Respir J. 2010;36:1391---9.
18.QuanjerPH,StanojevicS,ColeTJ,BaurX,HallGL,CulverBH, etal.Multi-ethnicreferencevaluesforspirometryforthe 3---95-yragerange:thegloballungfunction2012equations.EurRespir J.2012;40:1324---43.
19.BurityEF,PereiraCA,RizzoJA,BritoMC,SarinhoES.Reference valuesforspirometryinpreschoolchildren.JPediatr(RioJ). 2013;89:374---80.
20.BurityEF, PereiraCA,Rizzo JÂ,SarinhoES,Jones MH.Early termination of exhalation: effect on spirometric parame-tersinhealthypreschool children.JBrasPneumol.2011;37: 464---70.
21.World Health Organization (WHO). Multicentre Growth References Study Group. WHO Child Growth Standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-heightandbodymassindex-for-age:methodsand development.Geneva:WHO;2006.