w w w . r b o . o r g . b r
Update
Article
Hip
arthroscopy
夽
Henrique
Antônio
Berwanger
de
Amorim
Cabrita
a,b,∗,
Christiano
Augusto
de
Castro
Trindade
b,
Henrique
Melo
de
Campos
Gurgel
a,b,
Rafael
Demura
Leal
b,
Ricardo
da
Fonseca
de
Souza
Marques
baInstitutodeOrtopediaeTraumatologia,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil bInstitutoVita,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received8July2013 Accepted12July2013 Availableonline14May2014
Keywords: Hip/pathology Hip/surgery Arthroscopy
a
b
s
t
r
a
c
t
Hiparthroscopyisasafemethodfortreatingavarietyofpathologicalconditionsthatwere unknownuntiladecadeago.Femoroacetabularimpingementisthecommonestofthese pathologicalconditionsandtheonewiththebestresultswhentreatedearlyon.The instru-mentsandsurgicaltechniqueforhiparthroscopycontinuetoevolve.Newindicationsfor hiparthroscopyhasbeenstudiedastheligamentumteresinjuries,capsularrepairin insta-bilities,dissectionofthesciaticnerveandrepairofglutealmusclestears(injuriestothehip rotatorcuff),althoughstillwithdebatablereproducibility.Thecomplicationrateislow,and ever-betterresultswithfewercomplicationsshouldbeexpectedwiththeprogressionofthe learningcurve.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Artroscopia
de
quadril
Palavras-chave: Quadril/patologia Quadril/cirurgia Artroscopia
r
e
s
u
m
o
A artroscopiadequadriléummétodoseguroparaotratamentodediversaspatologias desconhecidasatéaúltimadécada.Oimpactofemoroacetabularéapatologiamaiscomum ecommelhoresresultadosquandotratadaprecocemente.Oinstrumentaleatécnica cirúr-gicadaartroscopiadequadrilcontinuamemevoluc¸ão.Novasindicac¸õesdeartroscopiade quadrilvemsendoestudadas,comootratamentodaslesõesdoligamentoredondo, cap-sulorrafianasinstabilidades,dissecac¸ãodonervociáticoereparodelesõesdosmúsculos glúteos(lesõesdomanguitorotadordoquadril),porémaindacomreprodutibilidade dis-cutível.Ataxadecomplicac¸õesébaixaeresultadoscadavezmelhoresecommenornúmero decomplicac¸õesdevemseresperadoscomaprogressãodacurvadeaprendizado.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
WorkperformedintheInstituteofOrthopedicsandTraumatology,HospitaldasClínicas,SchoolofMedicine,UniversidadedeSão PauloandintheHipGroup,InstitutoVita,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](H.A.B.deAmorimCabrita).
Introduction
Withinarthroscopicsurgery,approachestowardthehipjoint were shunned until recently because of the difficulty in diagnosing intra-articular pathological conditions and the technicaldifficultyofthesurgery.1
Thehipjointcapsuleisthethickestjointcapsuleinthe humanbody andislocatedindeep levelsthatcanonlybe accessedthrough voluminousmuscles suchasthe gluteus medius,andthestructuresneighboringitincludethefemoral triangleandthesciaticnerve,whichlimittheaccessportals. Thecoxofemoralspaceisverysmallandaccessibleonlywith jointtraction,andinstrumentmanipulationismadedifficult bytheconvexformatofthefemoralhead.2
Overthelasttwodecades,thedevelopmentofmagnetic resonanceimaging(MRI)hasmadeitpossibletoevaluatevery manyjointandperiarticularinjuries.Newconceptssuchas femoroacetabularimpingement(FAI)andtheperitrochanteric spacehavebeenintroduced.2,3
Specificinstruments have alsobeen developed, such as long cannulae, special optics and flexible radiofrequency shaversandprobesofsmallerdiameter.
Indications
and
contraindications
Hiparthroplastyprovidesaminimallyinvasivetechniquefor proceduresthatwillrequiresurgicaldislocationofthehip.In addition,itallowsorthopediststoaccessintra-articular alter-ationsthatpreviouslywerenotdiagnosed,letalonetreated.4
Themostcommonlytreatedpathological conditionsare FAI,labrallesions,teresligamentinjuriesandexternaland internalprominences.5
Thediagnosticindicationsinvolveevaluationofthe carti-lageinosteonecrosiscasesorinconjunctionwithosteotomy andevaluationofpainfularthroplastyandcollectionoftissue forculturing.6
Synovialdiseases(chondromatosis,pigmented villonodu-larsynovitisandrheumatoidarthritis)presentgoodsurgical indications,asalsodoestreatmentofdeepglutealpain (for-merlypiriformsyndrome).
Newindicationsforarthroscopy,suchasreconstructionof theteresligament,capsulorrhaphyincasesofinstability7and
repairofinjuriestotheglutealtendons3arebeingstudied.
The main contraindication for hip arthroscopy is the existenceofactiveinfectious processes, exceptin casesof drainageofpyoarthritisorevaluationofinfectionin prosthe-ses.Activeskininfectionsand,especially, infectionsinthe regionoftheportalsimpedesurgery.8
Technicaldifficultiesshouldbeexpected,butare notan absolutecontraindicationforsurgeryinobesepatientswith advancedosteoarthrosisorarthrofibrosis.8
Arthroscopic
hip
examination
Thearthroscopicanatomyofthehipisdividedintotwojoint compartments:centralandperipheral(Table1).
Thecentralcompartmentisthe spacebetweenthe car-tilaginous portion of the femoral head and the acetabular
Table1–Arthroscopicexaminationofthehip. Centralcompartment–approachedundertraction
Loadsurfaceofthefemoralhead Hyalinejointcartilage
Articularportionofthefibrocartilaginouslabrum Acetabularfossaandpulvinar
Teresligament Transverseligament
Peripheralcompartment–examinedwithouttraction Surfaceofthefemoralheadthatisnotsubjectedtoloading Femoralneck
Jointcapsule
Capsularportionofthelabrum
Zonaorbicularis(transversefibersofthejointcapsule) Medialsynovialplica
Medialarticularrecess
Articularportionofthetransverseligament(incasesoflaxity)
cotyledon,withparticipationfromthearticularportionofthe labrum,thepulvinarandtheteresandtransverseligaments. Thiscompartmentcanonlybereachedthroughtractionand separationofthesejointsurfaces.
The peripheral compartment involves the joint capsule (withitsmedial,anteriorandposteriorrecessesandthe trans-verse thickening ofits fibers,named thezona orbicularis), the capsular point ofthe labrum,the transverse ligament, themedialsynovialplicaandtheanterolateralportionofthe femoralhead,wherecam-likedeformitiescommonlyoccur.
Inadditiontothese,theperiarticularstructures,suchas theglutealmusculature,iliotibialband,fascialata,piriform muscles, externalrotators,sciatic nerveand greater sciatic foramen,canbeexplored.Thisisdoneinaso-called extra-articularendoscopicprocedure.
Someauthorshavepreferredtobeginthesurgical proce-dureintheperipheralcompartment,usingtheargumentthat, inthismanner,thelabrumisnotexposedtoinadvertent perfo-ration.However,mostauthorshavestartedthesurgeryatthe centralcompartment,undertraction,andthenhaveexplored theperipheralcompartmentsecondarily.
Pathological
conditions
dealt
with
using
hip
arthroscopy
Acetabularlabraltears
Labraltearsareanimportantcauseofhippain.Thefunction ofthe labrumisbetterunderstood todayand it isbelieved thatitsactsasasealantandthat,undernegativepressure,it ensuressomestabilityforthehipandpreventsexcessive con-tactbetweenthecartilagesoftheacetabulumandthefemoral head.
Acetabularlabraltearswereinitiallycharacterizedasan isolatedpathologicalconditionwithoutmajorrepercussions, but theyhavestartedtobethoughtofasaconsequenceof bonedeformity,traumaorsupraphysiologicalmovementsof thehip,asinthecaseofballerinas,9andaredirectlyrelated
tojointdegeneration.10
Labraltearsmayhavetraumaticordegenerativeorigins11
wrenching,jointdegeneration,boneinsufficiency(dysplasia), instabilityorfemoroacetabularimpingement.12
Independentofthe etiology,labral tears are more com-monintheanterosuperiorquadrant.13 Inthislocation,the
mechanicalresistanceofthelabrumislessthaninallother regions,eitherthroughtraction(instability)orthrough com-pression(femoroacetabularimpingement),asshownininvitro mechanicaltests.14
McCarthyetal.10observedthatlabraltearsandhip
arthro-siswereprogressionsofthesamedegenerativediseaseand openedupthepossibilityofinterveningintheevolutionof thearthrosisthrougharthroscopicsurgicaltreatmentofthe labraltearanditscauses.15
Arthroscopicsurgeryhastraditionallybeenusedfor diag-nosing intra-articularlesions and for removingfreebodies fromthehip.Itsuseforlabraltearshasbeenwidely dissemi-natedoverthepastdecade.15
Arthroscopy with stabilization by means of anchors or partial resection of the labrum, together with correc-tion of the factor that triggered the lesion, is the most recommended treatment. Although the initial studies on arthroscopyreportedarelativelyhighfailurerate,16theresults
havebecomemorepromisingsincethedevelopmentofthe concepts of femoroacetabular impingement and labral re-fixationorreconstruction.
Goodresultsfrompartialresectionofthelabrumbymeans ofarthroscopywerepresentedby82%of52patientswhowere followedupfor10years,accordingtoByrdandJones.17
Studiesonsheephavedemonstratedthatthelabrumhas thecapacitytohealafterrefixation.18Likewise,arthroscopy
performedonhumancaseshasshownhealinginmorethan 88%ofreoperatedcases.18
In open treatment for femoroacetabular impingement, Espinosa et al.19 observed that the results were better in
patientsinwhom thelabrumhadbeenfixedthaninthose whounderwentresection(80%versus28%),aftertwoyearsof follow-up.
In a matched group of 74 patients who underwent arthroscopyto treatmixed orpincer-like femoroacetabular impingement, labral fixation also presented better results thanresection. Afteroneyear offollow-up, thegroup with therepairspresentedameanHarrishipscore(HHS)of94.3%, and87.9%oftheresultsweregood.Ontheotherhand,inthe groupinwhichthelabrumwasresected,themeanHHSwas 88.9%and66.7%oftheresultsweregood.20
Infollowinguptwogroups(23and25patients)withlabral tearsandfemoroacetabularimpingementthatwereoperated bymeans of arthroscopy, the group that was treated with labralstabilizationandosteochondroplastypresentedabetter functionalscoreandlowerreoperationrate.21
Incasesinwhichlabralfixationisnotpossible, reconstruc-tioncanbeperformed.Techniquesusinggraftscomingfrom theiliotibialbandorgracilistendonhavebeendescribed,with excellentresults.22,23
Evaluationoftheresultsfromtreatinglabraltearsisvery difficultbecausethereisnouniformclassification,the non-arthrotic indices forfunctional evaluationare inconsistent andthetreatmentprotocolsareveryvaried.16
Mohtadietal.24describedaceilingeffectinwhichactive
youngpatientspresentedgoodscoresdespitetheirlimitations
duetopathologicalconditionsofthehip.Thus,theycreated iHOT,whichisaspecificquestionnaireforthisactive popula-tionwithhippains.
Allthestudiesareunanimousinstatingthatthemain fac-torforapoorprognosisisthepresenceofarthrosisorcartilage injuriesofOuterbridgetypeIVor TönnistypeIII orIV.16 If
thejointspaceislessthan2mm,progressiontoarthroplasty occurs in80% ofsuchcasesonaverage,after twoyearsof follow-up.25
Femoroacetabularimpingement
Femoroacetabularimpingement(FAI)isapurelymechanical disorderthatoccurswhenthehippresentsincongruenceand the extremes of its range of movement.It has the conse-quencesofjointpainandpredispositiontowardarthrosis.26
Itsbehaviorresemblesanabnormalityoftherotation mecha-nismofthefemoralhead,incontrastwiththeshearingforces thatoccurinvarusorvalgusnecks.
TheestimatedprevalenceofasymptomaticFAIinthe gen-eralpopulationis10–15%.27
TheclinicaltypesdescribedclinicallybyGanzetal.26are
thecamandpincerortongtypes.
In morethan 70% of the cases of dislocation operated surgically or arthroscopically, both acetabular and femoral alterationsarefound,andthesecasesaredescribed as pre-senting“mixed”impingement.28,29
Theappropriatesurgicaltreatmentinvolvescorrectionof thedeformitiesonbothsidesofthejoint,bymeansof osteo-chondroplasty.
Insomecases,theimpingementmaybedueto overload-ing, above the physiological level, ofa hip that is normal fromananatomicalpointofview,asseeninballerinas,for example.30Inthesecases,thecartilageinjurymayoccurin
atypicallocations.9
Ganzet al.26 described adirectassociation betweenFAI
andsecondaryarthrosisofthehipandrecommendedearly surgicalinterventionincasesoffemoroacetabular deformi-ties,beforeirreversiblecartilageinjuriesoccur,thuspossibly delayingtheevolutionofthehiparthrosis.Intheirpioneering evaluation,theyreportedsurgicaldislocation,whichbecame thegoldstandardatthattime.
Arthroscopyisclearlyanattractiveoption,sinceitinvolves smallerincisions,shorterrecoverytimeandpotentiallyfewer complicationsthanseeninopensurgery.Inseveralrecent arti-cles,thetwoprocedureswereseentohaveresultssimilarto thosefromarthroscopy.
The best indications for arthroscopy are cam-like tears aloneandmildacetabularretroversion.16
Mardones et al.31 compared the open and arthroscopic
surgicaltechniquesincadaversanddidnotfindany signifi-cantdifferencesintheprecisionofosteochondroplastyofthe femoralheadincasesofcam-likeimpingement.
Ilizaliturri et al.32 demonstrated improvements in the
WOMAC(WesternOntarioandMcMasterUniversities) arthri-tis score in 15 of their 19 patients. There were no severe complications.Onepatientevolvedtoarthroplastytwoyears afterthesurgery.
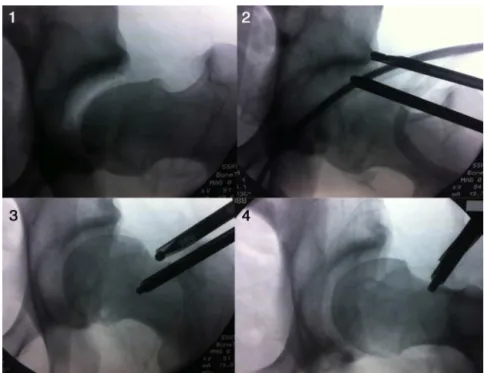
Cabrita et al.33 described 60 hiparthroscopy procedures
Fig.1–Sequenceoffluoroscopyimagesduringhiparthroscopy:(1)jointundertraction,withthepresenceofcamand pincer;(2)resectionofthepincer;(3)osteochondroplastyofthefemoralneck(cam);and(4)finalappearance.
complications and with conversion to arthroplasty in 6% (Fig.1).
Poleselloetal.34operatedon49athletes(51hips)andfound
that76%oftheathleteshadfullyreturnedtotheirsportsafter aminimumfollow-upperiodofoneyear(meanof39months). LarsonandGiveans35describedtheirearlyexperiencefrom
100hipsin96patientswithameanfollow-upof9.9months, withsignificantimprovementintheHHSandconversionto arthroplastyin3%ofthecases.
Philipponetal.36operatedon122patientswith
femoroac-etabularimpingementbymeansofarthroscopyandfollowed themupforameanof2.3years(minimumfollow-upoftwo years).ThemeanHHSwentfrom 58to84,and10patients (8.2%)underwenttotalhiparthroplasty.Thefactorsthat pre-dicted improvements were preoperative HHS>80, previous joint spacelarger than 2mmand labral repairrather than resectionduringthearthroscopyprocedure.
Diagnostic
indications
Painfulhiparthroplasty
Evaluationofpainfulhiparthroplastybymeansofarthroscopy isthecommonestdiagnosticindication.Collectionofsynovial and jointcapsulefluidsamplesprovides agood sourcefor cultures.Othersourcesofpaincanalsobeobservedin pros-theses,suchastendinitisoftheiliopsoasduetofriction,36
interpositionofforeignbodies,jointinstability,aseptic loos-ening,impingementbetweencomponentsandadherences.37
Osteonecrosis
Evaluation of the joint cartilage in osteonecrosis cases is possible using hip arthroscopy, which can be done
together withdecompression (forage) ofthe femoral head, in Ficat stages I or IIa of osteonecrosis, without risk of worsening the circulation of the femoral head. Ellenrieder etal.38usedarthroscopytodeterminehowtomanagethese
cases. In patients with Steinberg stages II and III, with-out head collapseor chondral lesions, decompression was performed in association with grafting using autologous graft cylinders. In cases of collapse (Steinberg IV), reduc-tionofthecollapsedportionwasattemptedwiththeaidof fluoroscopy.38
Inaddition, indicationofarthroscopyhasbecome inter-estingbecausedamagetothecartilageofthefemoralhead can be better assessed.In 52 cases ofosteonecrosis, Rush etal.39 founddamagetothefemoralcartilagethathadnot
beendetectedthroughmagneticresonanceimagingin36%of thepatients.
Hiparthroscopyintraumacases
Hip arthroscopy is indicated inpost-traumatic cases, with goodresultsachievedsafely.40
Cabritaetal.41 performed32hiparthroscopyprocedures
Synovialdiseasesofthehip
Pigmented villonodular synovitis may present diffusely or focally.Bothconditionscanbetreatedusingarthroscopy,but theprognosisisverydifferentandpoorerindiffusecases,with earlyprogressiontoarthritis.43
BoyerandDorfmann44treated111patientswithsynovial
chondromatosisarthroscopically,withamean follow-up of sixyears.Halfofthepatientsevolvedwellandwithoutany needforother treatments. There were indicationsfornew arthroscopyin20%ofthecases,opensurgeryin37%andtotal hiparthroplastyin19%.
Otherauthorshavereportedthatarthroplastyisan effec-tivemethodforremovingfreechondromatousbodies,butthat theremightbedifficultiesinaccessingposteromedialand pos-terolateralareasintheperipheralcompartment,whichcould leadtorecurrences.45,46
Inaretrospectivestudy,Zhouetal.47inspected40hipsin
36patients withautoimmunediseases (17with ankylosing spondylitis,11withrheumatoidarthritisandeightwith pso-riaticarthritis),bymeansofirrigationanddebridementofthe inflammatorytissue.Allofthepatientspresentedimproved rangeofmotionanddiminishedsynovitisonmagnetic reso-nanceimaging,and75%ofthepatientsweresatisfiedwiththe results.
Arthroscopy
in
cases
of
sequelae
of
childhood
diseases
Hipdysplasia
There is some controversy regarding indications for arthroscopy in cases of dysplasia, and its use should be consideredtobetheexception.
ByrdandJones48reportedgoodresultsin38casesthatwere
dysplasticoronthethresholdofdysplasia,withprogressionof themeanHHSfrom57pointsto83,andtherewereonlythree unsatisfactoryresultsafterameanfollow-upof27months.
Parvizietal.49reportedthatpainfulsymptomspersistedin
24casesoutof34casesthatwerefollowedup.Fourteencases evolvedtoservearthrosisandtherewere13casesoflateral migrationofthefemoralhead.Theseauthorscontraindicated hiparthroscopyincasesofdysplasiabecauseofthepossibility ofaccelerationofthedegenerativeprocess.
Recently,arthroscopyhasbeenperformedinsuchpatients together withor afterperiacetabularosteotomy, withgood results.Onehypothesisforexplainingthisisthatthe acetab-ular reorientation provides a better environment for the repairedlabrumtohealin.50
SlippedcapitalfemoralepiphysisandPerthessequelae
Slippedcapitalfemoralepiphysisand Perthessequelaeare twocausesofcam-likefemoroacetabularimpingementthat canbedealtwithusingarthroscopy.51
Deformitiesduetoslippedcapitalfemoralepiphysisshould beevaluated bymeans oflateral radiographsor computed tomography.Incasesofalterationofthefemoraloffset,i.e. sig-nificantposteriorslippage,osteochondroplastytocorrectthe
femoroacetabularimpingementwillnotwork.Rather,there needstoberealignmentoftheproximalfemurbymeansof intra-articularorsubtrochanteric.
AlthoughFreemanetal.52affirmedthatarthroscopywould
notaffectthenaturalhistoryofPerthesdisease,theyindicated thatthisprocedurewouldimprovequalityoflifeandscores, overaminimumfollow-upoftwoyears.
Teresligamentinjuriesandcapsulerepairincasesof instability
Thefunctionoftheteresligamenthasstillnotbeenwell estab-lished,but it seemstoplacelimitson combinedextension and externalrotationmovements.Itbecomestensed when thismovementistestedinphysicalexaminations,orwiththe Faberemovement(flexion,abductionandexternalrotation).
Rao et al.53 classified teres ligament injuries into three
groups: I – partialtraumatic; II –total traumatic; and III – degenerative.
Inaninitialseriesof271hiparthroscopyprocedures,Byrd andJones54found41casesofteresligamentinjuries,ofwhich
23weretraumaticand18weredegenerative.
Philipponetal.55reportedthatreconstructionoftheteres
ligamentcouldbeperformedinaselectgroupofpatientswith complaintsofinstabilityandsupraphysiologicalmovements, afterattemptingtheusual arthroscopicmanagement,asin treatmentsforfemoroacetabularimpingement,labralrepair andcapsuleplication.
Thecapsule-ligamentstabilizersofthehiparecontinuing tobestudiedandtheirrolehasstillnotbeendefined.Some authorshavedevelopedtechniquesforcapsulerepair,butthe effectsofthissurgicalprocedureoverthelongtermremain unknownandprospectivestudiesarestillbeingconducted.7,56
Hippyoarthritis
Kim et al.57 performed arthroscopy on eight cases of hip
pyoarthritisinchildrenandtwocasesinadultsandachieved therapeuticsuccessinallofthem.
El-Sayed58 compared arthroscopic treatment with open
drainageincasesofhippyoarthritisin20children:70%ofthe resultsfromtheopentechniqueweregoodand90%fromthe arthroscopictechnique.
Yamamotoetal.59successfullytreatedfouradultswithhip
pyoarthritis,andNusemetal.60sixadults,usingarthroscopy.
Resectionofosteoidosteoma
Resectionofosteoidosteomainthehiphasbeendescribedin childrenandadultsinisolatedcases.Thesymptomsinthese patients may simulatethose offemoroacetabular impinge-ment,withgoodindicationsonlyinsubchondraloranterior femoralneckcases.60
Extra-articular
arthroscopy
(endoscopic
treatment
of
pathological
conditions
of
the
hip)
Fig.2–Imageofendoscopicreleaseofthesciaticnerve:(1)nerve(representedby*)withthepiriformmuscle,showing adherencesand(2)finalappearanceoftheprocedurefollowingtenotomyofthepiriformmuscleandneurolysisofthe sciaticnerve.
tendinopathy of the gluteus minimus and gluteus max-imus, which together cover the concept of the painful syndromeofthegreatertrochanter,61internalprojectionand
piriformsyndrome(deepglutealpain).
Externalprojection
Externalprojectionisproducedbythickening ofthe poste-riorportionoftheiliotibialbandoranteriorthickeningofthe fibersofthegluteusmaximus.Itisreproducedthroughfriction betweenthesestructuresandthegreatertrochanterduring flexionorextension,anditmayormaynotbepainful.62Many
ofthesymptomaticcasescanberesolvedbymeansof physio-therapyandstretching.Releasecanbeperformedasanopen oran arthroscopic procedure.63 Thiscan bedone withthe
patientinlateraldecubitus.
Poleselloetal.63describedatechniquethatdiminishedthe
tensionintheiliotibialbandbymeansofhalf-releasingthe glutealtendonatitsfemoralinsertion, onthe lineaaspera, withgoodresults.
Trochantericbursitisandinjuriesoftheglutealmuscles
Therearemanytherapeuticpossibilitiesfortrochanteric bur-sitis.Casesthatarerefractorytoconservativetreatmentcan betreatedsurgicallybymeansofendoscopy,efficientlyand safely.62
Tendontearsoftheglutealmuscleshavebeencompared withrotatorcufftearsintheshoulder. Incompleteor com-pletetearsare correlated withchronictrochantericbursitis withapositiveTrendelenburgsign.Itisverylikelythatthese injuries are underdiagnosed. There is little published data onthistopicandnewtechniquesareemerging.However,it remainsuncleartowhatpointthemuscleinjuryisreversible, orwhatitslong-termprognosisis.
Internalprojection
Internal projection generally occurs when the tendon of theiliopsoasrubsagainstthe iliopectinealeminenceorthe femoralhead.
Ilizariturrietal.64treated19patientswithinternal
projec-tion causedbytheiliopsoasmuscle, withgoodresultsand
without anydifferenceregardingwhethertenotomyshould beperformedatthelevelofthelessertrochanterorinthe anteriorcapsularregionofthehip.
Inareviewarticle,Khanetal.65reportedthatarthroscopic
releasehadalowercomplicationrateandlesspostoperative painthanshownwiththeopentechnique.
Deepglutealpain
Deepglutealpain,formerlyknownaspiriformsyndrome,is apathologicalconditiondiagnosedbyrulingoutalternatives anditstreatmentiseminentlyconservative.Surgeryis indi-catedinrefractorycases.66
Itmanifestsaspainintheglutealregion,withorwithout accompanyingsciaticpain.Itworsenswithlocalcompression andgenerallycontinuesforyearsuntilitisidentified.
Theclassicalsurgicaltreatmentconsistsofanopen tech-nique, but the esthetic result from this approach and the potential forsciatic nerve injuriesofteninhibit use ofthis surgery.
Martinetal.67performedendoscopicreleaseofthesciatic
nervein35patients.Theydissecteditfromstructuressuchas the piriformmuscle,fibrous bands,vascular malformations andadherencestotheobturatormusclesandthequadratus femorismuscle,therebyachievingimprovementofthemean HHSfrom54.4beforetheoperationto78aftertheoperation, withafollow-upof1.5years.Thesciaticpainthatthepatients hadcomplainedofwhentheywereseateddisappearedin83% ofthecases.
Cabritaetal.68 describedexplorationofthesciaticnerve
(Fig.2)accompaniedbytenotomyofthepiriformand neurol-ysisofthesciaticnerve,withintraoperativeneuralmonitoring (evoked potential and electroneuromyography), with good resultsintheirinitialtencases,withoutrecurrencesand with-outneurologicalinjuries.
Complications
Inasystematicreviewoftheliterature69thatincluded92
6.3%.Thecommonestcauseofcomplicationswasconversion toatotalhipprosthesis.
Thecommonestcomplication isiatrogenicinjurytothe cartilageorlabrumduringpositioningoftheportals.
Neuropraxiaofthepudendumnerveandlateralcutaneous nerveofthethighwasthecommonestneurovascular compli-cationandwasdirectly relatedtothetractionmechanisms andtoskinlesionsintheperinealregion.
Hipdislocationdue toexcessive removalofthe acetab-ular rim, intra-abdominal and intrathoracic extravasation, hypothermia,infection, thromboembolicphenomena, avas-cular necrosis, heterotopic ossification and fracturing of the neckare complicationsthat are reported from time to time.
Cabritaetal.41reportedthatamong450consecutivecases,
thecomplicationratediminishedwiththeevolutionofthe learningcurve.
However,Souzaetal.70statedthatamong194casesthat
theyfollowedup,thecomplicationrateremainedunchanged with the learning curve, although the nature of the com-plicationschanged, accompanyingindicationsand surgical techniquesthatwereincreasinglycomplex.
Final
remarks
1. Hiparthroscopyisasafetreatmentmethodforamyriadof pathologicalconditionsofthehipthatwereunknownuntil adecadeago.
2. Femoroacetabularimpingementisthecommonest arthro-scopicpathologicalconditionandtheonethatpresentsthe bestresultsfromearlytreatment.
3. Theinstrumentsandthesurgicaltechniquesforhip arthro-plastyarecontinuingtoevolve.
4. New indications forhip arthroplasty are being studied, such asrepairsforteres ligament injuries, capsulorrha-phy incasesoftraumaticandnon-traumatic instability; dissection of the sciatic nerve; and repairs to injuries of the gluteus medius and minimus muscles. Despite the enthusiasm, these indications are technically dif-ficult, with debatable reproducibility, and there is a lack of long-term prospective studies for proving their efficacy.
5. Ever-betterresultsandever-fewercomplicationsshouldbe expected,inaccordancewiththelearningcurve.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GlickJM.Hiparthroscopybythelateralapproach.Instr CourseLect.2006;55:317–23.
2. ByrdJW.Hiparthroscopyutilizingthesupineposition. Arthroscopy.1994;10(3):275–80.
3. BediA,KellyBT,KhandujaV.Arthroscopichippreservation surgery:currentconceptsandperspective.BoneJointJ. 2013;95(1):10–9.
4.CabritaHA,GurgelHM,LealRD,OksmanD.Hiparthroscopy inthesupineposition:follow-upof400consecutivecases. Arthroscopy.2011;27(10):e108–9.
5.LynchTS,TerryMA,BediA,KellyBT.Hiparthroscopic surgery:patientevaluation,currentindications,and outcomes.AmJSportsMed.2013;41(5):1174–89. 6.ByrdJW.Hiparthroscopy:patientassessmentand
indications.InstrCourseLect.2003;52:711–9.
7.SlikkerW3rd,VanThielGS,ChahalJ,NhoSJ.Theuseof double-loadedsutureanchorsforlabralrepairandcapsular repairduringhiparthroscopy.ArthroscTech.2012;1(2):e213–7. 8.McCarthyJC,LeeJA.Hiparthroscopy:indications,outcomes,
andcomplications.InstrCourseLect.2006;55:301–8. 9.KoloFC,CharbonnierC,PfirrmannCW,DucSR,LubbekeA,
DuthonVB,etal.Extremehipmotioninprofessionalballet dancers:dynamicandmorphologicalevaluationbasedon magneticresonanceimaging.SkeletalRadiol.
2013;42(5):689–98.
10.McCarthyJC,NoblePC,SchuckMR,WrightJ,LeeJ,TheOttoE. AufrancAward:theroleoflabrallesionstodevelopmentof earlydegenerativehipdisease.ClinOrthopRelatRes. 2001;(393):25–37.
11.LeunigM,SledgeJB,GillTJ,GanzR.Traumaticlabralavulsion fromthestablerim:aconstantpathologyindisplaced transverseacetabularfractures.ArchOrthopTraumaSurg. 2003;123(8):392–5.
12.KellyBT,WeilandDE,SchenkerML,PhilipponMJ.
Arthroscopiclabralrepairinthehip:surgicaltechniqueand reviewoftheliterature.Arthroscopy.2005;21(12):1496–504. 13.LeunigM,PodeszwaD,BeckM,WerlenS,GanzR.Magnetic
resonancearthrographyoflabraldisordersinhipswith dysplasiaandimpingement.ClinOrthopRelatRes. 2004;(418):74–80.
14.SmithCD,MasourosS,HillAM,AmisAA,BullAM.A biomechanicalbasisfortearsofthehumanacetabular labrum.BrJSportsMed.2009;43(8):574–8.
15.McCarthyJC.Hiparthroscopy:whenitisandwhenitisnot indicated.InstrCourseLect.2004;53:615–21.
16.McCarthyJC.Thediagnosisandtreatmentoflabraland chondralinjuries.InstrCourseLect.2004;53:573–7. 17.ByrdJW,JonesKS.Hiparthroscopyforlabralpathology:
prospectiveanalysiswith10-yearfollow-up.Arthroscopy. 2009;25(4):365–8.
18.PhilipponMJ,SchenkerML,BriggsKK,KuppersmithDA, MaxwellRB,StubbsAJ.Revisionhiparthroscopy.AmJSports Med.2007;35(11):1918–21.
19.EspinosaN,RothenfluhDA,BeckM,GanzR,LeunigM. Treatmentoffemoro-acetabularimpingement:preliminary resultsoflabralrefixation.JBoneJointSurgAm.
2006;88(5):925–35.
20.LarsonCM,GiveansMR.Arthroscopicdebridementversus refixationoftheacetabularlabrumassociatedwith femoroacetabularimpingement.Arthroscopy. 2009;25(4):369–76.
21.NeppleJJ,ZebalaLP,ClohisyJC.Labraldiseaseassociatedwith femoroacetabularimpingement:doweneedtocorrectthe structuraldeformity?JArthroplasty.2009;24(6Suppl):114–9. 22.EjnismanL,PhilipponMJ,LertwanichP.Acetabularlabral
tears:diagnosis,repair,andamethodforlabral reconstruction.ClinSportsMed.2011;30(2):317–29. 23.MatsudaDK,BurchetteRJ.Arthroscopichiplabral
reconstructionwithagracilisautograftversuslabral refixation:2-yearminimumoutcomes.AmJSportsMed. 2013;41(5):980–7.
InternationalHipOutcomeTool(iHOT-33).Arthroscopy. 2012;28(5):595–605.
25.PhilipponMJ,BriggsKK,CarlisleJC,PattersonDC.Jointspace predictsTHAafterhiparthroscopyinpatients50yearsand older.ClinOrthopRelatRes.2013;471(8):2492–6.
26.GanzR,ParviziJ,BeckM,LeunigM,NötzliH,SiebenrockKA. Femoroacetabularimpingement:acauseforosteoarthritisof thehip.ClinOrthopRelatRes.2003;(417):112–20.
27.LeunigM,GanzR.Femoroacetabularimpingement.A commoncauseofhipcomplaintsleadingtoarthrosis. Unfallchirurg.2005;108(1):9–10.
28.BeckM,KalhorM,LeunigM,GanzR.Hipmorphology influencesthepatternofdamagetotheacetabularcartilage: femoroacetabularimpingementasacauseofearly
osteoarthritisofthehip.JBoneJointSurgBr. 2005;87(7):1012–8.
29.PhilipponM,SchenkerM,BriggsK,KuppersmithD. Femoroacetabularimpingementin45professionalathletes: associatedpathologiesandreturntosportfollowing arthroscopicdecompression.KneeSurgSportsTraumatol Arthrosc.2007;15(7):908–14.
30.DuthonVB,CharbonnierC,KoloFC,Magnenat-ThalmannN, BeckerCD,BouvetC,etal.Correlationofclinicaland magneticresonanceimagingfindingsinhipsofelitefemale balletdancers.Arthroscopy.2013;29(3):411–9.
31.MardonesR,LaraJ,DonndorffA,BarnesS,StuartMJ,GlickJ, etal.Surgicalcorrectionof“cam-type”femoroacetabular impingement:acadavericcomparisonofopenversus arthroscopicdebridement.Arthroscopy.2009;25(2):175–82. 32.IlizaliturriJrVM,Orozco-RodriguezL,Acosta-RodríguezE, Camacho-GalindoJ.Arthroscopictreatmentofcam-type femoroacetabularimpingement:preliminaryreportat2years minimumfollow-up.JArthroplasty.2008;23(2):226–34. 33.CabritaHA,CastropilLF.Hipathroscopy–anevaluationof60
consecutivecases.JBoneJointSurgBr.2006;88(Suppl1):76. 34.PoleselloGC,OnoNK,BellanDG,HondaEK,GuimarãesRP,
JuniorWR,SellaGD.Artroscopiadoquadrilematletas.Rev BrasOrtop.2009;44(1):26–31.
35.LarsonCM,GiveansMR.Arthroscopicmanagementof femoroacetabularimpingement:earlyoutcomesmeasures. Arthroscopy.2008;24(5):540–6.
36.PhilipponMJ,BriggsKK,YenYM,KuppersmithDA.Outcomes followinghiparthroscopyforfemoroacetabularimpingement withassociatedchondrolabraldysfunction:minimum two-yearfollow-up.JBoneJointSurgBr.2009;91(1):16–23. 37.McCarthyJC,JibodhSR,LeeJA.Theroleofarthroscopyin
evaluationofpainfulhiparthroplasty.ClinOrthopRelatRes. 2009;467(1):174–80.
38.EllenriederM,TischerT,KreuzPC,FröhlichS,FritscheA, MittelmeierW.Arthroscopicallyassistedtherapyofavascular necrosisofthefemoralhead.OperOrthopTraumatol. 2013;25(1):85–94.
39.RuchDS,SekiyaJ,DicksonSchaeferW,KomanLA,PopeTL, PoehlingGG.Theroleofhiparthroscopyintheevaluationof avascularnecrosis.Orthopedics.2001;24(4):339–43.
40.YamamotoY,IdeT,OnoT,HamadaY.Usefulnessof arthroscopicsurgeryinhiptraumacases.Arthroscopy. 2003;19(3):269–73.
41.CabritaHBA.Artroscopiadequadril.In:BarrosFilhoTEP, CamargoOP,CamanhoGL,organizadores.ClínicaOrtopédica. SãoPaulo:Manole;2011.p.966-89.
42.IlizaliturriJrVM,Gonzalez-GutierrezB,Gonzalez-UgaldeH, Camacho-GalindoJ.Hiparthroscopyaftertraumatichip dislocation.AmJSportsMed.2011;39(Suppl):50S–7S. 43.WardSrWG,BolesCA,BallJD,ClineMT.Diffusepigmented
villonodularsynovitis:preliminaryresultswithintralesional resectionandp32synoviorthesis.ClinOrthopRelatRes. 2007;454:186–91.
44.BoyerT,DorfmannH.Arthroscopyinprimarysynovial chondromatosisofthehip:descriptionandoutcomeof treatment.JBoneJointSurgBr.2008;90(3):314–8. 45.LeeJB,KangC,LeeCH,KimPS,HwangDS.Arthroscopic
treatmentofsynovialchondromatosisofthehip.AmJSports Med.2012;40(6):1412–8.
46.ZiniR,LongoUG,deBenedettoM,LoppiniM,CarraroA, MaffulliN,etal.Arthroscopicmanagementofprimary synovialchondromatosisofthehip.Arthroscopy. 2013;29(3):420–6.
47.ZhouM,LiZL,WangY,LiuYJ,ZhangSM,FuJ,etal. Arthroscopicdebridementandsynoviumresectionfor inflammatoryhiparthritis.ChinMedSciJ.2013;28(1):39–43. 48.ByrdJW,JonesKS.Hiparthroscopyinthepresenceof
dysplasia.Arthroscopy.2003;19(10):1055–60.
49.ParviziJ,BicanO,BenderB,MortazaviSM,PurtillJJ,EricksonJ, etal.Arthroscopyforlabraltearsinpatientswith
developmentaldysplasiaofthehip:acautionarynote.J Arthroplasty.2009;24(Suppl6):110–3.
50.MatsudaDK,SafranMR.Arthroscopicinternalfixationof osteochondritisdissecansofthefemoralhead.Orthopedics. 2013;36(5):e683–6.
51.JayakumarP,RamachandranM,YoumT,AchanP.Arthroscopy ofthehipforpaediatricandadolescentdisorders:current concepts.JBoneJointSurgBr.2012;94(3):290–6.
52.FreemanCR,JonesK,ByrdJW.Hiparthroscopyfor Legg–Calvè–Perthesdisease:minimum2-yearfollow-up. Arthroscopy.2013;29(4):666–74.
53.RaoJ,ZhouYX,VillarRN.Injurytotheligamentumteres. Mechanism,findings,andresultsoftreatment.ClinSports Med.2001;20(4):791–9.
54.ByrdJW,JonesKS.Traumaticruptureoftheligamentumteres asasourceofhippain.Arthroscopy.2004;20(4):385–91. 55.PhilipponMJ,PennockA,GaskillTR.Arthroscopic
reconstructionoftheligamentumteres:techniqueandearly outcomes.JBoneJointSurgBr.2012;94(11):1494–8.
56.DombBG,PhilipponMJ,GiordanoBD.Arthroscopic capsulotomy,capsularrepair,andcapsularplicationofthe hip:relationtoatraumaticinstability.Arthroscopy. 2013;29(1):162–73.
57.KimSJ,ChoiNH,KoSH,LintonJA,ParkHW.Arthroscopic treatmentofsepticarthritisofthehip.ClinOrthopRelatRes. 2003;(407):211–4.
58.El-SayedAM.Treatmentofearlysepticarthritisofthehipin children:comparisonofresultsofopenarthrotomyversus arthroscopicdrainage.JChildOrthop.2008;2(3):
–37.
59.YamamotoY,IdeT,HachisukaN,MaekawaS,AkamatsuN. Arthroscopicsurgeryforsepticarthritisofthehipjointin4 adults.Arthroscopy.2001;17(3):290–7.
60.NusemI,JaburMK,PlayfordEG.Arthroscopictreatmentof septicarthritisofthehip.Arthroscopy.2006;22(8),902.e1-3. 61.IlizaliturriJrVM,Camacho-GalindoJ.Endoscopictreatmentof
snappinghips,iliotibialband,andiliopsoastendon.Sports MedArthrosc.2010;18(2):120–7.
62.CabritaHABA,GurgelHMC,LealRD,EmilioL,OksmanD. Externalsnappinghip:anewdiagnosticmaneuverand arthroscopictreatmentof15cases.Arthroscopy. 2011;27(10):e95–6.
63.PoleselloGC,QueirozMC,DombBG,OnoNK,HondaEK. Surgicaltechnique:endoscopicgluteusmaximustendon releaseforexternalsnappinghipsyndrome.ClinOrthop RelatRes.2013;471(8):2471–6.
65.KhanM,AdamichJ,SimunovicN,PhilipponMJ,BhandariM, AyeniOR.Surgicalmanagementofinternalsnappinghip syndrome:asystematicreviewevaluatingopenand arthroscopicapproaches.Arthroscopy.2013;29(5):942–8. 66.FishmanLM,DombiGW,MichaelsenC,RingelS,RozbruchJ,
RosnerB,etal.Piriformissyndrome:diagnosis,treatment, andoutcome–a10-yearstudy.ArchPhysMedRehabil. 2002;83(3):295–301.
67.MartinHD,ShearsSA,JohnsonJC,SmathersAM,PalmerIJ. Theendoscopictreatmentofsciaticnerveentrapment/deep glutealsyndrome.Arthroscopy.2011;27(2):172–81.
68.CabritaHABA,GurgelHMC,LealRD,OksmanD,FerreiraR. Arthroscopicreleaseofthepiriformistendonwith intra-operativeneuromuscularmonitoring.Arthroscopy. 2011;27(10):e94–5.
69.HarrisJD,McCormickFM,AbramsGD,GuptaAK,EllisTJ,Bach JrBR,etal.Complicationsandreoperationsduringandafter hiparthroscopy:asystematicreviewof92studiesandmore than6,000patients.Arthroscopy.2013;29(3):589–95. 70.SouzaBG,DaniWS,HondaEK,RicioliW,GuimaraesRP,Ono