r e v b r a s o r t o p . 2015;50(3):266–269
w w w . r b o . o r g . b r
Original
Article
Reproducibility
of
the
AO/ASIF
and
Gartland
classifications
for
supracondylar
fractures
of
the
humerus
in
children
夽
Igor
Tadeu
Silveira
Rocha
∗,
André
de
Siqueira
Faria,
Carlos
Fontoura
Filho,
Murilo
Antônio
Rocha
UniversidadeFederaldoTriânguloMineiro(UFTM),Uberaba,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received2April2014 Accepted15May2014 Availableonline28May2015
Keywords: Fracturesofthe humerus/classification Children
Observer-dependentvariations Reproducibilityofresults
a
b
s
t
r
a
c
t
Objective:ToevaluatethereproducibilityoftheradiographicclassificationsofGartlandand theAssociationforOsteosynthesis/AssociationfortheStudyofInternalFixation(AO/ASIF) forsupracondylarfracturesofthehumerusinchildren.
Methods:Ontwooccasions,50radiographsinanteroposteriorandlateralviewswere evalu-atedbythreepediatricorthopedistsinaccordancewiththeGartlandandAO/ASIFpediatric classifications.Their responses weresubjectedto statisticalanalysisconsisting of cal-culationofthecoefficienttoassesstheintra-andinterobserverconcordance,inboth classifications.
Results:Thestrengthoftheintraobserverconcordancewashighornearperfectforthethree examinersinthetwoclassificationsystems.Thestrengthoftheinterobserverconcordance washighinthetwosystems,withcoefficientsof0.756fortheGartlandclassificationand 0.766fortheAO/ASIFclassification.
Conclusion:TheGartlandandAO/ASIFclassificationsystemsshowedsimilarreproducibility andperformance.Highstrengthofconcordancewasseenintheintra-andinterobserver analyses.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Reprodutibilidade
das
classificac¸ões
AO/ASIF
e
Gartland
para
fraturas
supracondilianas
de
úmero
em
crianc¸as
Palavras-chave:
Fraturasdoúmero/classificac¸ão Crianc¸a
r
e
s
u
m
o
Objetivo:Avaliarareprodutibilidadedasclassificac¸õesradiográficasdeGartlande Associa-tionforOsteosynthesis/AssociationfortheStudyofInternalFixation(AO/ASIF)parafraturas supracondilianasdeúmeroemcrianc¸as.
夽
WorkdevelopedintheDisciplineofOrthopedicsandTraumatology,UniversidadeFederaldoTriânguloMineiro,Uberaba,MG,Brazil. ∗ Correspondingauthor.
E-mails:[email protected],[email protected](I.T.S.Rocha). http://dx.doi.org/10.1016/j.rboe.2015.05.001
rev bras ortop.2015;50(3):266–269
267
Variac¸õesdependentesdo observador
Reprodutibilidadedosresultados
Métodos: Emduasocasiõesforamavaliadasportrêscirurgiõesortopedistaspediátricos50 radiografiasnasincidênciasanteroposterioreseperfildeacordocomasclassificac¸õesde GartlandeAO/ASIFpediátrica.Asrespostasforamsubmetidasàanáliseestatísticapelo cálculodocoeficienteparaavaliaraconcordânciaintra-einterobservador,emambasas classificac¸ões.
Resultados:Aforc¸adeconcordânciaintraobservadorfoigrandeouquaseperfeitaparaostrês examinadoresnosdoissistemasdeclassificac¸ão.Aforc¸adeconcordânciainterobservador foigrandenosdoissistemas,comcoeficientede0,756paraclassificac¸ãodeGartlandede 0,766paraclassificac¸ãoAO/ASIF.
Conclusão: Ossistemasdeclassificac¸ãodeGartlandeAO/ASIFmostraram reprodutibili-dadeedesempenhosimilar.Observou-segrandeforc¸adeconcordâncianasanálises intra-einterobservador.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Supracondylar fractures are the commonesttype of elbow fracturesinchildrenandthesecondcommonesttypeof frac-tureduringchildhood,accountingformorethan60%ofthe cases.1–4Theyoccurmostfrequentlybetweentheagesoffive andtenyears.5Thevariousclassificationsystemsproposed forthesefractureshavehad theaimsofguidingthe treat-ment,estimatingtheprognosisandenablingstandardization and comparisonamongthe many scientific studies.These classificationsneedtobesimple,easytoapplyclinicallyand reproducible, with high concordance between surgeons.6–8 TheGartlandclassificationforsupracondylarfracturesofthe humerusistheonemostused.9,10Inthisclassificationsystem, fracturesaregroupedaccordingtotheirdegreeof displace-ment.
AlthoughtheLaGrange11classificationismoredescriptive anddetailed incasesofgreaterdisplacement,it isnotthe systemmostused.
Inturn,thesystemadoptedbytheAOgroup12forfractures ofthelongbonesinchildrencombinestheclassificationof Mulleretal.13foradultswithanadditionaldescriptionfocused ontheimmatureskeleton.8Thisisanalphanumericsystem thatincludestheboneaffected,thelocationandthe sever-ity,along withthe peculiaritiesofthe growingbone.Thus, supracondylarfractureswouldbedescribedas13-/9.1withan endingofI,II,IIIorIV,accordingtowhetherthefracturewas completeorincomplete,andwithorwithoutcontactbetween thefragments.Inthismanner,onlytheexceptioncomponent (I–IV)ofthemorphologicalsegmentoftheAO/ASIF classifica-tionwastakenintoconsiderationinthepresentstudy.
Theobjectiveofthisstudywastoassessthereproducibility oftheGartlandandAO/ASIFclassificationsfor supracondy-larfracturesofthehumerusinchildren,byinvestigatingthe levelsofintra-andinterobserverconcordance.
Methods
Thisstudywasconductedinareferralhospitalthatattends orthopedictraumacases,afterreceiving approvalfrom the institution’sethicscommittee.Fiftyconventionalradiographs
(anteroposterior and lateral views) originating from initial attendance ofpatients withsupracondylar fractures ofthe humerus, produced between January and June 2013, were selectedforevaluation.
Theradiographicimagesforthe studywere obtainedby meansofhigh-resolutiondigitalphotography,with preserva-tionoftheoriginalcharacteristicsofthefilm.
Theselectiondidnottakeintoconsiderationthequality oftheradiography.Imagesfrompatientsovertheageof16 years,fromthosewhopresentedaclosedgrowthplateline andfromthosepresentingmultiplefracturesonradiographs wereexcluded.Theimageswereevaluatedbythreepediatric orthopedistswhohadhadpreviousaccesstothe classifica-tionsystems.Sevendaysoftrainingbeforetheanalysiswas permitted.
Theexaminersevaluatedthe50imagesoveramaximum time oftwo hoursandmade asecond evaluationwiththe sameduration,twoweekslater.Theorderofthe50images was variedthrough randomization.Theexaminers didnot haveaccesstotheresponsesoftheirpeersortotheirown responsesgivenonthepreviousoccasion.
Theresponsesgivenbyeachexaminertotheradiographic evaluationswerewrittenonaprintedchartthatwashanded out toeach participant, together witha freeandinformed consentstatement.
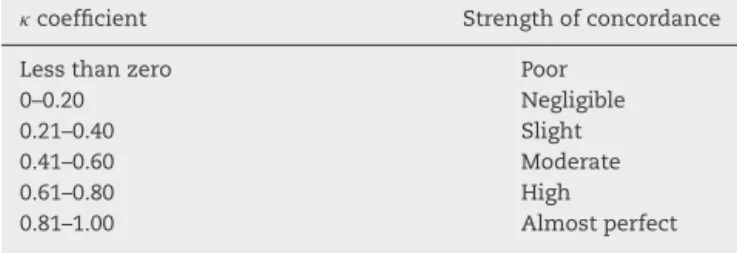
Theresultswere gatheredandanalyzedwith theaidof theSPSS® software,version12.0(Chicago,USA),inorderto determinethecoefficient,whichinferredthedegreeof con-cordancebeyondwhatwouldbeexpectedonlybychance.The strength oftheintra-andinterobserver concordanceofthe
Table1–Associationbetweenthecoefficientandthe strengthofconcordance.14
coefficient Strengthofconcordance
Lessthanzero Poor
0–0.20 Negligible
0.21–0.40 Slight
0.41–0.60 Moderate
0.61–0.80 High
268
rev bras ortop.2015;50(3):266–269Table2–Intraobserverconcordancelevelaccordingto thecoefficient,inrelationtotheGartlandandAO classificationsforsupracondylarfracturesofthe humerusinchildren.
Gartland AO
Examiner1 0.781 0.767
Examiner2 0.859 1
Examiner3 0.719 0.782
Table3–Interobserveranalysisoncoefficientfor Gartlandclassification.
GartlandI GartlandII GartlandIII
0.945 0.535 0.677
p-Valueof <0.001 <0.001 <0.001
95%confidence intervalof
Upper:1.0 Upper:0.695 Upper:0.837
Lower:0.785 Lower:0.375 Lower:0.517
twoclassificationsystemswasthendetermined,asdetained inTable1.14
Results
The intraobserver concordance according to the coeffi-cient,relatingtotheGartlandclassificationforsupracondylar fracturesofthehumerusinchildrenandtheAO/ASIF clas-sificationforfractures inchildren,aspresentedinTable2, washighoralmostperfectforalltheexaminersinrelation tobothclassifications.For twoofthethree examiners,the concordancefortheAO/ASIFsystemwasslightlyhigher.
Tables3and4presenttheinterobserveranalysesforthe GartlandandAOclassifications,respectively.Itcanbeseen thattheinterobserverconcordancedecreasedwithregardto categoryII,inbothclassificationsystems.
AsshowninTable5,theinterobserverevaluationshowed of0.756 for the Gartland classification and 0.766 forthe
AO/ASIFclassification,whichthusshows highconcordance betweenthetwosystems.
Discussion
Thediversityofclassificationsystemsforagroupoffractures thatispublishedoverthecourseoftimemaygiveriseto inter-pretationalconflicts.
Thus,thevalidity,reproducibilityandcorrelationsof well-established classifications need to be verified, given that comparisonsbetweendifferentevaluations,withexclusionof causalityandpersonalbias,candemonstratethequalitiesor weaknessesofagivensystemunderexamination.According toAudigéetal.,6fortheseobjectivetobeattained,the clas-sificationsystemneedstogothroughthreeresearchphases beforeitisvalidatedforclinicaluse.6,14
Toknowwhetheragivencharacterizationorclassification foranobjectisreliable,thisobjectneedstobeevaluated sev-eraltimes,bymorethanoneexaminer.Forthis,inthepresent study,thecoefficientwasused.Thisinfersthedegreeof con-cordancebeyondwhatwouldbeexpectedpurelybychance. Itisbasedonthenumberofconcordantresponses,i.e.the numberofcasesforwhichtheresultisthesameamongthe examiners.15,16
In thepresent study,the examinersseemed tobe“well calibrated”,bothwithinthemselvesandwiththeothers.The interobserverconcordancevalueswerewithinthe95% con-fidenceinterval,withp<0.001inbothclassificationsystems. Therefore,thesevaluespresentedstatisticalsignificance.As alsofoundbyBrandãoetal.,14ourinterobserverconcordance indexwasnogreaterthan0.8,eventhoughtheobserverswere allpediatricorthopedists.
TheconcordancefoundbetweentheGartlandandAO/ASIF classificationsystemswas satisfactory(high oralmost per-fect). These systems had similar performance, despite the greatercomplexityoftheAO/ASIFsystemandtheexaminers’ lowerdegreeoffamiliaritywiththissystem.
Inthepresentstudy,theloweststrengthofconcordance (moderate)intheinterobserveranalysiswasfoundintypeIIof theGartlandandAO/ASIFclassifications.However,according toHealetal.,10thelowestlevelofinterobserverconcordance fortheGartlandclassificationoccurredintypeI.
Itwasobservedthatvariationsinthedegreeof concord-anceintheinterobserveranalysisofdifferentstudies10,14did
Table4–InterobserveranalysisoncoefficientforAOclassification.
AOI AOII AOIII AOIV
0.865 0.435 0.75 1.0
p-Valueof <0.001 <0.001 <0.001 <0.001
95%confidenceintervalof Upper:1.0 Upper:0.595 Upper:0.91 Upper:1.0
Lower:0.705 Lower:0.275 Lower:0.59 Lower:0.84
Table5–Generalcoefficientforinterobserverevaluation,accordingtoclassificationsystem.
Numberofradiographs General Generalp-value 95%confidenceintervalof
Gartland 50 0.756 <0.001 Upper:0.874
Lower:0.637
AO/ASIF 50 0.766 <0.001 Upper:0.868
rev bras ortop.2015;50(3):266–269
269
notinvalidatetheconstantobservationthatthetwo classifi-cationshavegoodreproducibility.
Evaluationofthereproducibilityoftheseclassificationsis ofimportanceinsofarastheyguidethetypeoftreatment insti-tutedforthesefractures(conservativeversussurgical).They alsoenablestandardization ofthe orthopediclanguage for comparingstudiesfromdifferentcenters.
Nowthatthereproducibilityoftheseclassificationsystems hasbeen verified,it becomesnecessary toconduct further studiestoascertainwhetheroneofthemmightbesuperior totheotherandthustodetermineastandardsystem.
Conclusion
TheGartlandandAO/ASIFclassificationsystemsshowed sim-ilarreproducibilityandtheintra-andinterobserveranalyses showed high strength of concordance,even though use of theAO/ASIFsystemremainslimitedamongorthopedistsand, consequently,theirfamiliaritywiththismethodislower.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. LinsRE,SimovitchRW,WatersPM.Pediatricelbowtrauma. OrthopClinNorthAm.1999;30(1):119–32.
2. ChengJC,ShenWY.Limbfracturepatternindifferent pediatricagegroups:astudyof3350children.JOrthop Trauma.1993;7(1):15–22.
3. BlountWP.Fracturesinchildren.Baltimore:Williamsand Wilkins;1955.
4.SmithFM.Children’selbowinjuries:fracturesand dislocations.ClinOrthopRelatRes.1967;(50):7–30. 5.KasserJR,BeatyJH.Supracondylarfracturesofthedistal
humerus.In:BeatyJH,KasserJR,editors.Rockwoodand Wilkins’fracturesinchildren.5thed.Philadelphia:Lippincott Williams&Wilkins;2001.p.577.
6.AudigéL,BhandariM,KellamJ.Howreliablearereliability sudiesoffractureclassifications?Asystematicreviewoftheir methodologies.ActaOrthopScand.2004;75(3):184–94. 7.GarbuzDS,MarsiBA,EsdaileJ,DuncanCP.Classification
systemsinorthopaedics.JAmAcadOrthopSurg. 2002;10(4):290–7.
8.SlongoT,AudigéL,SchlickeweiW,ClavertJ,HunterJ. DevelopmentandvalidationoftheAOpaediatric
comprehensiveclassificationoflong-bonefractures.JPediatr Orthop.2006;26(1):43–9.
9.GartlandJJ.Managementofsupracondylarfracturesofthe humerusinchildren.SurgGynecolObstet.1959;109(2):145–54. 10.HealJ,BoudM,LivingstoneJ,BlewittN,BlomAW.
ReproducibilityoftheGartlandclassificationfor
supracondylarhumeralfracturesinchildren.JOrthopSurg (HongKong).2007;15(1):12–4.
11.LaGrangeJRP.Fracturessupracondyleennes.RevChirOrthop. 1962;48:337–414.
12.SlongoT,AudigéL,ClavertJM,LutzN,FrickS,HunterJ.AO comprehensiveclassificationofpediatriclong-bonefractures: aweb-basedmulticenteragreementstudy.JPediatrOrthop. 2007;27(2):171–80.
13.MüllerME,NazarianS,KochP.Thecomprehensive classificationoffracturesoflongbones.Berlin: Springer-Verlag;1990.
14.BrandãoG,TeixeiraL,AméricoL,SoaresC,CaldasL,Azevedo A,etal.Reprodutibilidadedaclassificac¸ãodaAO/Asifpara fraturasdosossoslongosnacrianc¸a.RevBrasOrtop.2010;45 Suppl.:37–9.
15.SiegelS,CastellanN.Nonparametricstatisticsforthe behavioralsciences.NewYork:McGraw-Hill;1988. 16.FleissJL.Themeasurementofinterrateragreement.In: