w w w . r b o . o r g . b r
Review
Article
Hip
salvage
surgery
in
cerebral
palsy
cases:
a
systematic
review
夽
Rafael
Carboni
de
Souza
∗,
Marcelo
Valentim
Mansano,
Miguel
Bovo,
Helder
Henzo
Yamada,
Daniela
Regina
Rancan,
Patricia
Maria
de
Moraes
Barros
Fucs,
Celso
Svartman,
Rodrigo
Montezuma
César
de
Assumpc¸ão
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6September2012 Accepted14May2014 Availableonline16June2015
Keywords:
Cerebralpalsy Salvage Hip Femur
a
b
s
t
r
a
c
t
Imbalanceandmusclespasticity,inassociationwithcoxa valgaandpersistentfemoral anteversion,compromiseshipdevelopmentincasesofcerebralpalsyandmayresultin chronicpainandevendislocation.Someofthesehipsundergosalvagesurgerybecauseof thesevereimpactoftheirabnormalitiesinthesepatients’qualityoflife.Weconducteda systematicreviewoftheliteraturetocomparetheresultsfromthemainhipsalvage tech-niquesappliedtotheseindividuals.Theliteraturesearchfocusedonstudiesthatevaluated resultsfromhipsalvagesurgeryincasesofcerebralpalsy,publishedfrom1970to2011, whicharepresentintheEmbase,Medline,PubMed,CochraneLibraryandSciELOdatabases. Althoughtheresultswerenotstatisticallycomparable,thissystematicreviewdemonstrates thathipsalvagesurgeryshouldbeindicatedafterindividualevaluationoneachpatient,due tothewidespectrumofpresentationsofcerebralpalsy.Therefore,itseemsthatnosurgical techniqueissuperiortoanyother.Rather,therearedifferentindications.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Cirurgias
de
salvamento
do
quadril
em
paralisia
cerebral:
revisão
sistemática
Palavras-chave:
Paralisiacerebral Salvamento Quadril Fêmur
r
e
s
u
m
o
Odesequilíbrioeaespasticidademuscular,associadosàcoxavalgaeàanteversãofemoral persistente,comprometemodesenvolvimentodoquadrilnaparalisiacerebralepodem resultaremdorcrônicaeatéluxac¸ão.Algunsdessesquadrissãosubmetidosacirurgiasde salvamentodecorrentesdograveimpactodassuasalterac¸õesnaqualidadedevida.Fizemos umarevisãosistemáticadaliteraturaparacompararosresultadosdasprincipaistécnicas aplicadasparasalvamentodoquadrilnessesindivíduos.Abuscanaliteraturatevecomo
夽
WorkperformedintheNeuromuscularDiseaseGroup,DepartmentofOrthopedicsandTraumatology,FaculdadedeCiênciasMédicas daSantaCasadeSãoPaulo,IrmandadedaSantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.C.deSouza). http://dx.doi.org/10.1016/j.rboe.2015.06.003
focoestudosqueavaliaramresultadosdecirurgiasdesalvamentodoquadrilem paral-isiacerebral,publicadosde1970a2011,presentesnasbasesdedadosEmbase,Medline, Pubmed,ScieloeCochraneLibrary.Apesardeosresultadosobtidosnãoserem estatisti-camentecomparáveis,essarevisãosistemáticademonstraqueascirurgiasdesalvamento doquadrildevemserindicadasapósavaliac¸ãoindividualdecadapaciente,decorrentedo amploespectrodeapresentac¸õesdaparalisiacerebral.Logo,aparentemente,nãoháuma técnicacirúrgicasuperioràsoutras,massimindicac¸õesdiferentes.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Hipdevelopmentisdeterminedthroughtheconstantactions ofthe musculature on this joint.Individuals withcerebral palsy(CP)arebornwithnormalhips.1However,throughthe muscleimbalancegeneratedbythespasticitypresentinthis condition, in association with coxa valga and uncorrected femoralanteversion,hipdevelopmentbecomescompromised andthisresultsindeformitiesofdifferentlevelsofseverity.1,2 Theincidenceofhipsubluxationanddislocationin spas-ticCPcasesishighlyvariable,between7%and60%.Higher prevalence,from33%to70%,isfoundamongpatientswith greaterneurologicalimpairment,quadriplegiccasesorcases presentingGMFCS(GrossMotorFunctionClassification Sys-tem) levels III, IV or V.3,4 Pain, difficulty in sitting down, pressureulcersandimpairedperinealhygienearethemain problemsresultingfromthesealterationswhenthecondition goesuntreated.5
Theaim of the treatments is to obtain a pain-free hip that allowsadequate range of motionand provides better positioningandcapacitytosit,inadditiontoimplementing hygieneandgeneralcaremeasures.6,7 Theresultsfromthe variousclosed or surgicaltreatments are directlylinked to the qualities of the joint surface, acetabular cartilage and femoral head.8 Thus, younger patients benefit more from closed reconstructionprocedures. On the other hand,hips thatpresentchronicsubluxationordislocationmayrequire salvagesurgery,suchasfemoralheadresection,arthroplasty, osteotomyorarthrodesis.9,10
Theliteratureonthissubjectissparse,particularlywith regard to presenting groups of patients that can be com-pared.Therearenocontrolledprospectivestudies,systematic reviewsormeta-analysescomparingthevarioushipsalvage surgerytechniquesappliedinCPcases.Theobjectivesofthe presentstudy were tocarryout asystematicreviewofthe literatureinordertocomparetheresultsfromthemain tech-niquesappliedforhipsalvageamongtheseindividualsand answerthe followingquestion:whichsurgicaltechnique is themosteffectivefortreatingdislocatedandpainfulhipsin CPcases,giventhesalvagesurgerymethodsavailable?
Material
and
methods
Aqualitativeandquantitativesystematicreviewofthe litera-turewascarriedout,whichhadtheaimofidentifyingallthe evidenceonhipsalvagesurgeryinCPcases.
Two reviewers separately performed a literature search focusingonstudiesthatevaluatedtheresultsfromhipsalvage surgeryinCPcases,publishedbetween1970and2012,using theEmbase,Medline,PubMed,SciELOandCochraneLibrary databases.Forthis,thefollowingdescriptorswereused: cere-bralpalsy,hip,femur,femoralandsalvage.
The studies selected complied with the inclusion and exclusioncriteriathatweestablished.Alltheinclusioncriteria hadtobemetforthestudytobeusedinthereview.Prospective clinical trials,withorwithoutrandomization, andalso ret-rospectivestudies,publishedinPortuguese,English,French, Spanish, GermanorItalianwereincluded. Sampleswithat least 10participants andlength offollow-upofatleast 12 monthswerealsoincluded.
The exclusion criteria were: case reports, editorials, descriptions of surgical techniques, studies that contained a sample of patients with neuromuscular diseases other than CP,and sampleswithmean agegreaterthan30 years (AppendixA:protocolmodel).
Thedata-gatheringprocessandinclusionandexclusionof studieswereperformedseparatelybytheauthorstwice.The efficacyofeachstudywasevaluatedregardingimprovement ofpain, easeofpersonalhygiene,functional improvement, satisfactionandpresenceorabsenceofheterotopic ossifica-tion.Theresultswerethenevaluatedand,lastly,abalanced and impartial synthesis was elaborated with due remarks relatingtoflawsintheevidence.
Results
Forty-eightpublishedpapersevaluatingpatientswithCPand painful hips who underwent salvage surgery were found. Tenobservationalretrospectivecohortstudieswereselected, while38studieswereexcluded(twodescriptionsofsurgical techniquesand36observationalstudies).Norandomizedand controlledexperimentalstudies werefound. Onlyone arti-clepresentedacontrolgroup,andthisstudycomparedthe techniquesproposedbyCastleandbyMcHale.11
The surgical techniques used and analyzed in these selected articles were: hip arthroplasty (n=1)12; Schanz femoral valgusosteotomy (n=1)13; hip arthrodesis (n=1)14; McHalevalgusosteotomy(n=2)15,16andresectionofthe prox-imal end of the femur (n=6).2,16–19 One study11 compared twosurgicaltechniques(resectionoftheproximalendofthe femurandMcHalevalgusosteotomy)(Table1).
Table1–Characteristicsaccordingtosurgicaltechnique applied.
Surgicaltechnique Meanfollow-up (months)
Samplesize Meanage
(years)
Arthroplasty 57 11 17
Arthrodesis 63 14 15.4
Castle 53.9 94 17.6
McHale 54.5 21 10.1
Schanz 98 35 13.5
Total 65.28 175 14.72
Table2–Primaryreasonsforstudyexclusion.
Primaryreasonfor exclusion
Numberofstudies
Surgicaltechnique 13
Language 6
Heterogeneouspatient sample
7
Meanage>30years Samplesize
53
Descriptionofsurgical techniques
2
Poorlydescribedresults 2
Total 38
hipsalvagesurgery,butrather,wereinterventionsfor improv-ingthepositionofthehipthroughreleasingsofttissues,along
withacetabularand femoralosteotomies.Other causes for
exclusionwere,indecreasingorder:heterogeneoussamples (n=7),language(n=6),meanagegreaterthan30years(n=5), inadequatesamplesize (n=3), descriptionofsurgical tech-niques(n=2)andpoorlydescribedresults(n=2)(Table2).
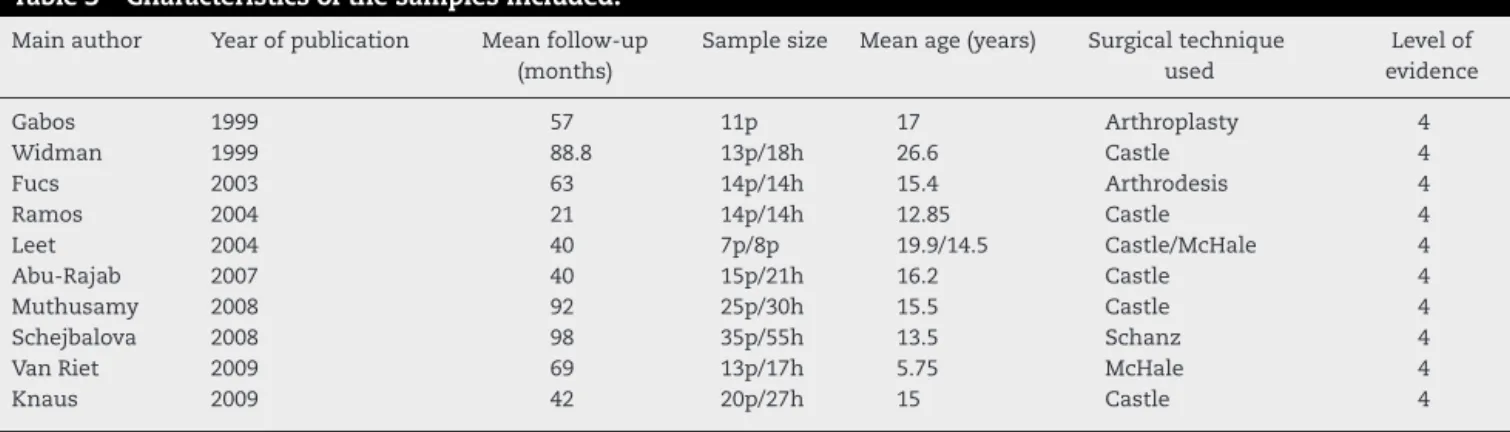
Thestudies selected were publishedbetween 1999 and 2009. The sample size ranged from 7 to 35 patients, and thesummedtotalwas175individuals.Themeanageofthe patientsintheincludedstudies was14.72years.Theolder patientsunderwentresectionoftheproximalendofthefemur (meanof17.6years),whiletheyoungeronesunderwentthe McHalevalgusosteotomytechnique(meanof10.1years).The follow-upofalltheserieswasgreaterthan21months,with
ameantotalof65.28months.Thesewereallobservational cohortstudies,withlevelIV evidence(Table3).
Discussion
There isgreat debate in the literatureconcerning surgical treatment for painful hips in CP cases, especially in rela-tiontothosewithsomelevelofdislocation,becausethereis no consensusregardingwhether thisfactor iswhatcauses the painful condition.10 Treatment decisions need to be basedoncarefulindividualizedclinicalobservationsoneach patient.14,20
Thisreviewoftheliteratureconsistedofqualitative anal-ysis on the results from the selected studies. Quantitative analysis,i.e.meta-analysis,wasnotpossiblebecauseofthe heterogeneity ofthe variables evaluated and the interpre-tation of the outcomes obtained from the studies, which thereforemadetheresultsnotstatisticallycomparable.
In many situations,thereare no controlledrandomized studies in the literature,and only datafrom observational studiesareavailable.Althoughtheinitialpreferencefor sys-tematicreviewsistorestrictthemtorandomizedprospective studies,thenumberofreviewsandmeta-analysespublished involving observational studies has increasedsubstantially overthepastfourdecades,withtheaimoffillingthisgap.21
Themainobstaclerelatingtoreviewswithobservational studies is the impossibility of controlling the sample and thevariablesevaluatedbecauseoftheirretrospectivenature. Therefore,it isnotalwayspossibletocomparetheselected studiesthroughmeta-analysis.21
Totalandpartialhiparthroplasty
Onlyonestudyevaluatedtheuseofpartialarthroplastyasa hipsalvagetechniqueinCPcases.12Gabosetal.12usedthe humeralcomponentofashoulderprosthesisafterresectionof theproximalendofthefemur.Overaperiodoffouryearsand ninemonths,11patientsofmeanage17yearswhopresented quadriplegic cerebral palsy and were unable towalk were evaluated.Paincriteriaandimprovementofperinealhygiene wereevaluatedbymeansofquestionnairesappliedoverthe telephone.In onlyonecasewas theevolutionunfavorable,
Table3–Characteristicsofthesamplesincluded.
Mainauthor Yearofpublication Meanfollow-up
(months)
Samplesize Meanage(years) Surgicaltechnique used
Levelof evidence
Gabos 1999 57 11p 17 Arthroplasty 4
Widman 1999 88.8 13p/18h 26.6 Castle 4
Fucs 2003 63 14p/14h 15.4 Arthrodesis 4
Ramos 2004 21 14p/14h 12.85 Castle 4
Leet 2004 40 7p/8p 19.9/14.5 Castle/McHale 4
Abu-Rajab 2007 40 15p/21h 16.2 Castle 4
Muthusamy 2008 92 25p/30h 15.5 Castle 4
Schejbalova 2008 98 35p/55h 13.5 Schanz 4
VanRiet 2009 69 13p/17h 5.75 McHale 4
Knaus 2009 42 20p/27h 15 Castle 4
andthis patientcontinued tohavehygiene difficultiesand hippain.
Totalhiparthroplastyincerebralpalsycasesisfrequently recommendedforolder,skeletallymaturepatients.22–26These individuals,giventheirgreaterage,mostlypresentlesssevere conditionswithregardtospasticityandcognitiveandmotor deficit.Thisobservationcorroboratesthefindingthatpatients whoseconditionsaremoreseverecasesdieearlier.8Thus,the successoftotalhiparthroplastyseemstobedirectly propor-tionaltothe severityoftheclinical conditionofCP,among otherfactors.
Arthrodesis
Onlyoneofthestudiesusedhiparthrodesisasanoptionfor salvagesurgery.14Fucsetal.14evaluatedtheevolution(mean follow-upoffiveyearsandthreemonths)of14patientswho underwentunilateralarthrodesis.Thissamplewascomposed offour diplegicindividuals,eightquadriplegicpatientsand twowithamixedpattern (diplegiaand dyskinesia),with a meanageof15yearsandfivemonths.Functionally,fourwere abletowalk(oneofthemonlyathome),threewereonlyable tositupandsevenwerepermanentlybedridden.Allofthese individualspresentedcomplaintsofsevereunilateralhippain. The postoperative functional evaluation demonstrated absence of pain and better positioning (flexion-abduction) amongalltheindividuals.Amongthebedriddenpatients,five becameabletoremainseatedandtwostartedtowalk.Despite theresultsobtained,thelimitsandcontraindicationsofthis techniqueincludesituationsofthecontralateralhipatriskor alreadycompromised,andalsothepresenceofspinal defor-mity.
Valgusproximalosteotomyofthefemur
Regardingvalgusproximalosteotomyofthefemur,two stud-ieswereincluded.Inone,Schanzosteotomywasapplied,13,27 whileinthe other,thetechniquedescribed byMcHalewas used.15,28
ThesepatientspresentedspasticquadriplegicCP,andtheir meanageswere13.5and21years,inthegroupsthat under-wenttheMcHaleandSchanzsurgeries,respectively.Themean minimum follow-up was 69 months.15 Among the criteria evaluated,bothoftheseauthorsdescribedimprovementsof paininover80%oftheirpatients,althoughthepainful condi-tionpersistedin7.3%13and15.3%.15
Bothofthesetechniquesresultedinimprovementofhip functionandallowedbetterhygienecare,althoughthegain ofmobilitywasonlyquantified(indegrees)inthegroupthat underwentthe McHalesurgery: 90◦ offlexion ormorewas
achievedby76.9%ofthepatientsandatleast35◦ofabduction
in69.2%.Thereweresomecomplicationssuchasheterotopic ossification,implantfailure,postoperativeinfectionand per-sistenceofpain,buttheseoccurredinaminimalnumberof cases.13,15
Schejbalovaetal.13justifiedthechoiceoftheirprocedure (Schantzvalgusosteotomy)asbeinglessinvasiveinrelation toothersurgicalmethodsfortheproximalfemur,andstated thatthisshouldbeappliedtoolderchildrenwithdislocated hipsforwhomreconstructivesurgeryisnotrecommended.
Therefore,thismethodisanoptionforpatientswithsevere quadriplegia,inrelationtothetechniqueofresectionofthe proximalendofthefemur.
Resectionoftheproximalendofthefemur
The mostwidelydisseminated resection techniquefor the proximalendofthefemurthatisusedashipsalvagesurgery inCPcaseswasdescribedbyCastleandSchneiderin1978.29 Thismethodconsistsofinterpositionarthroplasty,i.e. sub-trochantericosteotomy,andinvolvesremovalofthefemoral neckandhead(whichhavebeencompromisedby cartilagi-nousdegeneration)andinterpositionofthemusculatureof thequadricepsbetweenthestumpandtheacetabulum.
There are divergencesregardingthe postoperative man-agement of patients who undergo the Castle surgery. The measuresadoptedhavesoughtmainlytoavoidascensionof thefemoralstumpand,therefore,recurrenceofthepainful condition.29 To achieve this, methods such as cutaneous traction,skeletaltraction,externalfixatorsandpelvic immo-bilizationwithplastercastshavebeenused,dependingonthe author.Thetimeofuseofthesemethodshasusuallynotbeen mentioned.11,27,29
Sixstudies thatusedthistechnique,withits variations, suchastreatmentofthepainfuldislocatedhipatdifferent levels,wereselectedforthissystematicreview.2,11,16–19Most ofthesampleswerecomposedofpatientswithtetraparetic spasticCPwhowereunabletowork,asseeninthestudyby Abu-Rajabetal.,18inwhichalltheindividualswereclassified atGMFCSlevelV.
The patients with CP who underwent resection of the proximal end of the femur were younger than those that underwenttotalhiparthroplasty.Theirmeanageswere17.6 years and 38.1 years, respectively. These individuals were similarregardingclinicalconditiontothosewhounderwent valgusosteotomy,andbothgroupsonceagaindifferedfrom patients who undergo total hip arthroplasty, who are fre-quentlyabletowalkandhavebetterfunctionallevels.
The postoperative results obtained with this technique weresatisfactoryinallthestudiesselected.Whatmost dif-ferentiatedthestudiesweretheevaluationmethodsfor pre-andpostoperativepain,giventhatthisisasubjective crite-rionandmanyofthesepatientspresentedcognitivedeficit. Widmanetal.16usedthequantityofanalgesicpillsthatthe patientwasconsumingperday.Anotherauthormeasuredthe evolutionofpainbymeansofananalogscale(1–10),which wasappliedoverthetelephone.11
Regarding function and perineal hygiene, this surgical treatment was also shown to lead to an improvement in rangeofmotionandconsequentlyinperinealcare. Evalua-tion ofperineal hygienewas foundinall thestudies,with improvementsof62%16to100%,17,18fromassessmentofthe ease of perineal cleaning afterthe procedure.16–19 In turn, the evolutionofthe rangeofmotionwasassessedinmost studiesthroughmeasurementandcomparisonofabduction amplitudesbeforeandaftertheoperation.16,17Allthestudies presentedgainsinrangeofmotion.
recommended radiotherapy (RT), with 700cGy, to prevent heterotopicossification.Inthatstudy,usingBrooker’s classifi-cation,meansof2.7amongpatientswithoutRTand0.8among thosewhounderwentRTwereobtained.16
Finally,theonlycomparativestudyonhipsalvagesurgery techniqueswasconductedbyLeetetal.11 in2004.The evo-lution(mean follow-up of 3.4years) of15 individuals who hadundergonetheCastleandSchneider29(n=7)andMcHale etal.28(n=8)techniqueswerecomparedbymeansofa ques-tionnaireappliedoverthetelephone,toassesssatisfaction, mobility,perinealhygieneandpain,onascalefrom0to10. Thegroup that underwent the Castle and Schneider tech-niquepresentedapreoperativescoreof8.2,whichdecreased to2.9aftersurgery.Thegroup thatunderwent the McHale techniquehadapreoperativescoreof8.0,whichdecreased to4.8aftersurgery.Thesatisfactionscoreamongthe individ-ualswhounderwenttheCastleandSchneidertechniquewas 9,whilethosewhounderwenttheMcHaletechniquehad a scoreof7.7.Thedifferencesobtainedinbothtechniqueswere notstatisticallysignificant.
Final
remarks
Althoughtheresultsobtainedwerenotstatistically compa-rable,thissystematicreviewdemonstratedthathipsalvage surgeryshould beindicated afterindividual assessmentof eachpatient,becauseofthebroadspectrumofpresentationof CP.Thus,theredoesnotseemtobeanysurgicaltechniquethat issuperiortoanyother:rather,therearedifferentindications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Anexo
1.
Protocol
for
inclusion/exclusion
of
studies
1-Surgicaltechnique: 2-Samplesize(n): Malesex:femalesex: 3-Meanlengthoffollow-up: 4-Meanage:
5-Evolutioncriteria:()pain()hygiene()mobility() satisfaction()heterotopicossification
()others:–––––––––––––––––
r
e
f
e
r
e
n
c
e
s
1. ValenciaFG.Managementofhipdeformitiesincerebralpalsy. OrthopClinNAm.2010;41(4):549–59.
2. MuthusamyK,ChuHY,FriesenRM,ChouPC,EilertRE,Chang FM.Femoralheadresectionasasalvageprocedureforthe severelydysplastichipinnonambulatorychildrenwith cerebralpalsy.JPediatrOrthop.2008;28(8):884–9.
3.AckerlyS,VitztumC,RockleyB,OlneyB.Proximalfemoral resectionforsubluxationordislocationofthehipinspastic quadriplegia.DevMedChildNeurol.2003;45(7):436–40. 4.SooB,HowardJJ,BoydRN,ReidSM,LaniganA,WolfeR,etal.
Hipdisplacementincerebralpalsy.JBoneJointSurgAm. 2006;88(1):121–9.
5.TerjesenT.Developmentofthehipjointsinunoperated childrenwithcerebralpalsy:aradiographicstudyof76 patients.ActaOrthop.2006;77(1):125–31.
6.BleckEE.Hipdeformitiesincerebralpalsy.InstrCourseLect. 1971;67:530–2.
7.SamilsonRL,TsouP,AamothG,GreenWM.Dislocationand subluxationofthehipincerebralpalsypathogenesis,natural historyandmanagement.JBoneJointSurgAm.
1972;54(4):863–73.
8.HodgkinsonI,JindrichML,DuhautP,VadotJP,MettonG, BérardC.Hippainin234non-ambulatoryadolescentsand youngadultswithcerebralpalsy:across-sectional multicentrestudy.DevMedChildNeurol.2001;43(12):806–8. 9.SpiegelDA,FlynnJM.Evaluationandtreatmentofhip
dysplasiaincerebralpalsy.OrthopClinNAm. 2006;37(2):185–96.
10.RootL.Surgicaltreatmentforhippainintheadultcerebral palsypatient.DevMedChildNeurol.2009;51Suppl.4:84–91. 11.LeetAI,ChhorK,LaunayF,Kier-YorkJ,SponsellerPD.Femoral
headresectionforpainfulhipsubluxationincerebralpalsy:is valgusosteotomyinconjunctionwithfemoralheadresection preferabletoproximalfemoralheadresectionandtraction?J PediatrOrthop.2005;25(1):70–3.
12.GabosPG,MillerF,GalbanMA,GuptaGG,DabneyK.Prosthetic interpositionarthroplastyforthepalliativetreatmentof end-stagespastichipdiseaseinnonambulatorypatientswith cerebralpalsy.JPediatrOrthop.1999;19(6):796–804.
13.SchejbalovaA,HavlasV,TrcT.Irreducibledislocationofthe hipincerebralpalsypatientstreatedbySchanzproximal femoralvalgusosteotomy.IntOrthop.2009;33(6):1713–7. 14.FucsPM,SvartmanC,deAssumpc¸ãoRM,KertzmanPF.
Treatmentofthepainfulchronicallydislocatedand subluxatedhipincerebralpalsywithhiparthrodesis.J PediatrOrthop.2003;23(4):529.
15.VanRietA,MoensP.TheMcHaleprocedureinthetreatment ofthepainfulchronicallydislocatedhipinadolescentsand adultswithcerebralpalsy.ActaOrthopBelg.2009;75(2): 181–8.
16.WidmannRF,DoTT,DoyleSM,BurkeSW,RootL.Resection arthroplastyofthehipforpatientswithcerebralpalsy:an outcomestudy.JPediatrOrthop.1999;19(6):805–10.
17.RamosASN,CrestaniMV,MoschenGM,NetoLM.Ressecc¸ão dofêmurproximalemquadrisdolorososedeslocadosna paralisiacerebral.RevBrasOrthop.2004;39(5):245–52. 18.Abu-RajabRB,BennetGC.Proximalfemoral
resection-interpositionarthroplastyincerebralpalsy.J PediatrOrthopB.2007;16(3):181–4.
19.KnausA,TerjesenT.Proximalfemoralresectionarthroplasty forpatientswithcerebralpalsyanddislocatedhips:20 patientsfollowedfor1-6years.ActaOrthop.2009;80(1): 32–6.
20.TerjesenT.Thenaturalhistoryofhipdevelopmentincerebral palsy.DevMedChildNeurol.2012;54(10):951–7.
21.StroupDF,BerlinJA,MortonSC,OlkinI,WilliamsonGD, RennieD,etal.Meta-analysisofobservationalstudiesin epidemiology:aproposalforreporting.JAMA.
2000;283(15):2008–12.
22.BulyRL,HuoM,RootL,BinzerT,WilsonPDJr.Totalhip arthroplastyincerebralpalsy.Long-termfollow-upresults. ClinOrthopRelatRes.1993;296:148–53.
24.RaphaelBS,DinesJS,AkermanM,RootL.Long-termfollowup oftotalhiparthroplastyinpatientswithcerebralpalsy.Clin OrthopRelatRes.2010;468(7):1845–54.
25.SchroederK,HauckC,WiedenhöferB,BraatzF,AldingerPR. Long-termresultsofhiparthroplastyinambulatorypatients withcerebralpalsy.IntOrthop.2010;34(3):335–9.
26.WeberM,CabanelaME.Totalhiparthroplastyinpatients withcerebralpalsy.Orthopedics.1999;22(4):
425–7.
27.ShanzA.ZurBehandlungderveraltetenangeborenen Hüfvtverrenkung.ZOrthop.1921;42:442–4.
28.McHaleKA,BaggM,NasonSS.Treatmentofthechronically dislocatedhipinadolescentswithcerebralpalsywith femoralheadresectionandsubtrochantericvalgus osteotomy.JPediatrOrthop.1990;10(4):504–9. 29.CastleME,SchneiderC.Proximalfemoral