r e v b r a s r e u m a t o l . 2017;57(6):613–615
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Nephrotic
syndrome
as
the
first
manifestation
of
juvenile
systemic
scleroderma
Síndrome
nefrótica
como
a
primeira
manifestac¸ão
da
esclerodermia
sistêmica
juvenil
Saulo
B.
Couto
a,
Adriana
M.
Sallum
a,
Luciana
S.
Henriques
a,
Denise
M.
Malheiros
b,
Clovis
A.
Silva
b,
Maria
H.
Vaisbich
a,∗aUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,HospitaldasClínicas,InstitutodaCrianc¸a,UnidadedeNefrologiaPediátrica,
SãoPaulo,SP,Brazil
bUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,HospitaldasClínicas,DepartamentodePatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27February2014 Accepted17August2014
Availableonline12December2014
Introduction
Juvenilesystemicsclerosis(JSSc)isanautoimmunedisease, characterizedbydisorderedcollagen accumulation,leading todisseminatedvascularlesionsinskinandinternalorgans fibrosis,includingthekidneys.1–3
Worthyofnote,renalinvolvementisararemanifestation and occurs in 1–12%of JSSc patients, mainly with arterial hypertensionand/orproteinuria.1,3–5Sclerodermarenalcrisis
wasalsorarelyreported5,6 andtoourknowledge,nephrotic
syndrome(NS)wasdescribedinonlyoneJSScpatientwith membranousnephropathy.7
WereporthereinapatientwhopresentedNSasthefirst manifestationofJSScwithfocalsegmentalglomerulosclerosis (FSGS).
∗ Correspondingauthor.
E-mail:[email protected](M.H.Vaisbich).
Case
report
Afemale patientpresentedvomiting,malaiseand general-izededemaattheageof12years.Shehadsystemicarterial hypertension,hypoalbuminemia(<2.5mg/dL)andproteinuria (urineprotein/creatinineratio≥2.0mg/g).Shewasdiagnosed
withNSandtreatedwithprednisone(60mg/m2/day)with
pro-gressivereduction.Duringfollow-upshehadseveralrelapses ofNS,oneofthemassociatedtotheupperrespiratorytract infectionsandanotheronewithspontaneousbacterial peri-tonitis,andwasreferredtoourUniversityHospitalattheage of14.On the first admissionatourservice, shepresented orbital and lowerlimbsedema, systemicarterial hyperten-sion, sclerodactyly and proximal skin sclerosis.No muscle weaknessand vasculitiswereobserved.Laboratoryfindings
http://dx.doi.org/10.1016/j.rbre.2014.08.004
614
rev bras reumatol.2 0 1 7;57(6):613–615A
B
A
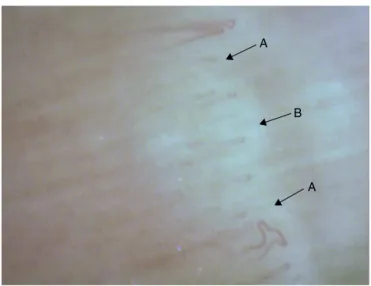
Fig.1–Nailfoldcapillaroscopyshowingmoderatecapillary dilation(arrowA)andmildfocaldevascularization(arrow B)inpatientwithjuvenilesystemicsclerosis.
revealedserumalbumin0.9g/dL(normallevels3.8–5.6),total cholesterol637mg/dL(normal<199),lowdensitylipoprotein (LDL) 439mg/dL (normal <110), serum urea 18mg/dL (nor-mal 15–45), serum creatinine 0.53mg/dL (normal 0.6–0.9), 25-hydroxyvitamin D 5ng/mL (normal 30–100ng/mL) and proteinuria7.8g/day. HandsX-rayrevealed no bone abnor-malities. Antinuclear antibodies (ANA), rheumatoid factor, andanti-Scl-70(anti-topoisomeraseI),anti-Sm,Anti-SS-A/Ro, Anti-SS-B/Laandanti-smoothmuscle(anti-SMA)antibodies werenegative.C3andC4fractionsofthecomplement sys-temwerenormal.SerologyforhepatitisA,BandC,human immunodeficiencyvirus(HIV),cytomegalovirus,Epstein–Barr virusandsyphiliswerenegative.Echocardiogramwasnormal. Moderatecapillarydilationandmildfocaldevascularization were observed in nailfold capillaroscopy, compatible with early stage of scleroderma (scleroderma pattern) (Fig. 1). Percutaneous renal biopsy guided by ultrasound revealed focalsegmentalglomerulosclerosisand direct immunofluo-rescencewerenegative(Fig.2AandB).Therefore,shefullfilled the provisional classification criteriafor JSSc.6 Thepatient
was treated with oral 25-hydroxyvitamin D (800IU/day),
methotrexate (0.5mg/kg/week) and amlodipin (0.15mg/kg). Prednisone (60mg/m2/day) was administered for 4
consec-utive weeks, followed by alternate-day (40mg/m2) for 2
consecutive months,with tapering for4months and then stoppingthismedication.Currently,sheisbeingtreatedwith methotrexate15mg/week,withoutedemaandproteinuria.
Discussion
Toourknowledge,thiswasthefirstcasereportedwith steroid-sensitiveNSandFSGSasthefirstmanifestationofJSSc.
The mostimportantsystemic manifestationof JSSc are cutaneouslesions,speciallyindurationproximalto metacar-pophalangealjoints,sclerodactlyandedema,1,3,4asobserved
inthepresentcase.Thecapillaroscopycanbeusedto eval-uate changes of microcirculation in the capillaries of the nailbed.8Thesefindingsstronglysuggestsystemicsclerosis
diagnosis,8asevidencedherein,andnotfoundincutaneous
scleroderma.9
Kidneyinvolvementwasrarelydescribedinpediatric scle-rodermapopulation.Themostfrequentrenalmanifestations were arterial hypertension and proteinuria. Renal crisis in JSSc patients ranges from 0.7% to 4%.1,3–5 This is a
life-threatening complication with abrupt onset of malignant arterialhypertension,proteinuriaand/orhematuria, throm-boticmicroangiopathyandpotentiallycanresulttoendstage kidneydisease.6,10,11
AdultsclerodermaNShasagreatspectrumvaryingfrom minimal changes disease and secondary amyloidosis to rapidly progressive renal failure and proliferative changes lesions with crescents,and membranous nephropathy. NS wasonlyreportedinone12-year-oldfemalepatientwho pre-sentedwithsclerodermafiveyearsaftertheonsetofthisrenal involvementwithmembranousnephropathy.7
Importantly,ourpatienthad steroidsensitive NSwitha severehistologicalpatternofFSGS.Thisglomerulopathyisan importantcauseofproteinuriaandchronicrenaldiseasein childrenandadolescents,accountingin5–15%ofallcasesof idiopathicNS.12,13
ThetreatmentofJSCc isperformedaccording toorgans andsystemsinvolvement.Methotrexatehasbeenshownto improveskinscoresinearlydiffuseSSc.14Additionally,renal
rev bras reumatol.2 0 1 7;57(6):613–615
615
treatmentofFSGSincludesglucocorticoidand antihyperten-sivedrugs,asusedinourpatient.12Interestingly,theabsence
ofproteinuriawithcompleteremissionaftertreatment sug-gestsadequaterenallong-termoutcome.13
Inconclusion,wereportedararecaseofNSwithFSGSas thefirstmanifestationofscleroderma.Therefore,renalbiopsy ismandatoryinJSScpatientswithsustainedproteinuriaorNS.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ThisstudywassupportedbyFundac¸ãodeAmparoàPesquisa doEstadodeSãoPaulo–FAPESP(grant#08/58238-4toCAS), Conselho Nacional de Desenvolvimento Científico e Tec-nológico–CNPq(302724/2011-7toCAS),FedericoFoundation toCASandNúcleodeApoioàPesquisa“SaúdedaCrianc¸ae doAdolescente”daUSP(NAP-CriAdtoCAS).
r
e
f
e
r
e
n
c
e
s
1. MartiniG,FoeldvariI,RussoR,CutticaR,EberhardA,Ravelli A,etal.Systemicsclerosisinchildhood:clinicaland immunologicfeaturesof153patientsinaninternational database.ArthritisRheum.2006;54:3971–8.
2. ZulianF,CuffaroG,SperottoF.Sclerodermainchildren:an update.CurrOpinRheumatol.2013;25:643–50.
3. FoeldvariI,TyndallA,ZulianF,Müller-LadnerU,CzirjakL, DentonC,etal.Juvenileandyoungadult-onsetsystemic sclerosissharethesameorganinvolvementinadulthood: datafromtheEustardatabase.Rheumatology(Oxford). 2012;51:1832–7.
4.ScalapinoK,ArkachaisriT,LucasM,FertigN,HelfrichDJ, LondinoAVJr,etal.Childhoodonsetsystemicsclerosis: classification,clinicalandserologicfeatures,andsurvivalin comparisonwithadultonsetdisease.JRheumatol.
2006;33:1004–13.
5.AoyamaK,NagaiY,EndoY,IshikawaO.Juvenilesystemic sclerosis:reportofthreecasesandreviewofJapanese publishedwork.JDermatol.2007;34:658–61.
6.ZulianF,WooP,AthreyaBH,LaxerRM,MedsgerTAJr,Lehman TJ,etal.ThePediatricRheumatologyEuropean
Society/AmericanCollegeofRheumatology/EuropeanLeague againstRheumatismProvisionalClassificationCriteriafor JuvenileSystemicSclerosis.ArthritisRheum.2007;57:203–12.
7.SarkarD,SircarG,WaikhomR,RaychowdhuryA,PandeyR, GhoshA.Severesystemicsclerosisdevelopinginapatientof membranousnephropathy.Rheumatology(Oxford).
2011;50:1522–3.
8.SatoLT,KayserC,AndradeLE.Nailfoldcapillaroscopy abnormalitiescorrelatewithcutaneousandvisceral involvementinsystemicsclerosispatients.ActaReumatol Port.2009;34:219–27.
9.ZulianF,AthreyaBH,LaxerR,NelsonAM,FeitosadeOliveira SK,PunaroMG,etal.Juvenilelocalizedscleroderma:clinical andepidemiologicalfeaturesin750children.An
internationalstudy.Rheumatology(Oxford).2006;45: 614–20.
10.KronbichlerA,MayerG.Renalinvolvementinautoimmune connectivetissuediseases.BMCMed.2013;11:95.
11.SabirO,YounasH,TanvirI,TarifN.Sclerodermarenalcrises: casereportandreviewofliterature.JPakMedAssoc. 2013;63:916–8.
12.D’AgatiVD,KaskelFJ,FalkRJ.Focalsegmental glomerulosclerosis.NEnglJMed.2011;365:2398–411.
13.LombelRM,GipsonDS,HodsonEM.Kidneydisease: improvingglobaloutcomestreatmentofsteroid-sensitive nephroticsyndrome:newguidelinesfromKDIGO.Pediatr Nephrol.2013;28:415–26.
14.RabinovichCE.Challengesinthediagnosisandtreatmentof juvenilesystemicsclerosis.NatRevRheumatol.