REVISTA
BRASILEIRA
DE
REUMATOLOGIA
www . r e u m a t o l o g i a . c o m . b r
Review
article
Positron
emission
tomography
with
18
F-FDG
in
the
evaluation
of
patients
with
rheumatoid
arthritis
-
a
systematic
review
Dalton
Alexandre
dos
Anjos
a,∗,
Licia
Maria
Henrique
da
Mota
baMedicineSchool,UniversidadedeBrasilia;NuclearMedicineCenter,UniversityHospitalofBrasília,ClínicaNúcleosandServiceof
PET/CT,HospitalSantaLúcia,Brasília,DF,Brazil
bDepartmentofRheumatology,MedicineSchool,UniversidadedeBrasília,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5July2012 Accepted18July2014
Availableonline25October2014
Keywords:
Positronemissiontomography(PET) Fluorine-18fluorodeoxyglucose (18F-FDG)
Rheumatoidarthritis
a
b
s
t
r
a
c
t
Introduction:Rheumatoidarthritis(RA)isadiseasecharacterizedbyinflammationofthe synovialmembrane.Severalauthorshaveinvestigatedtheroleofpositronemission tomo-graphy(PET)withfluorine-18fluorodeoxyglucose(18F-FDG)inRA.
Objectives:Tosystematicallyreviewthe currentliterature ontheroleof18F-FDGPETin
thediagnosis,determinationofdiseaseactivityandassessmentoftreatmentresponsein patientswithRA.
Methods:SearcheswereconductedinMedline,CochraneLibrary,Lilacs,PubmedandScopus inPortuguese,EnglishandSpanishlanguages,usingthekeywords«rheumatoidarthritis», «synovitis»,«FDG»,«PET»,«glycolyticmetabolism»and«diseaseactivity».
Results:Onehundredandforty-twoarticleswereinitiallyidentified,ofwhichonly40were relateddirectlytothesubject.Twelveoriginalarticlesandthreecasereportsthatmetthe inclusioncriteriawereselected.
Discussion:Thepresenceofactivatedmacrophagesandfibroblastsinpannusare respon-siblefortheintenseperiarticularuptakeof18F-FDG.Theuptakepatternsdonotallowthe
differentialdiagnosiswithotherarthritides.Theuptakeintensityandthenumberofjoints involvedaremetabolicparametersofdiseaseactivitythatcorrelatewellwiththe compos-iteindices.LongitudinalstudiesofPEThaveprovenusefulinassessingtheresponseto treatmentwithanti-TNF.Whenperformedearly,PETcanpredictthetherapeuticresponse.
Conclusion:AlthoughtheactualroleofthisnewtechniquefortheinvestigationofRAisnot yetestablished,18F-FDGPETisapromisingtoolindeterminingtheactivityandprediction
ofresponsetotreatmentofpatientswithRA.
©2014ElsevierEditoraLtda.Allrightsreserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.07.002. ∗ Correspondingauthor.
E-mail:[email protected](D.A.dosAnjos). http://dx.doi.org/10.1016/j.rbre.2014.07.003
rev bras reumatol.2014;54(6):474–482
475
Tomografia
por
emissão
de
pósitrons
com
FDG-
18F
na
avaliac¸ão
de
pacientes
com
artrite
reumatoide
–
revisão
sistemática
Palavras-chave:
Tomografiaporemissãode pósitrons(PET)
Flúor-18(FDG-18F)
Artritereumatoide
r
e
s
u
m
o
Introduc¸ão: aartritereumatoide(AR)éumadoenc¸acaracterizadapelainflamac¸ãoda mem-branasinovial.Diversosautorestêminvestigadoopapelda tomografiaporemissão de pósitrons(PET)comflúor-18(FDG-18F)naAR.
Objetivos: REVISÃOsistemáticadaliteraturaatualsobreopapeldoPETcomFDG-18Fno
diagnóstico,determinac¸ãodaatividadedadoenc¸aeavaliac¸ãodarespostaaotratamento empacientescomAR.
Métodos: ForamrealizadasbuscasnasbasesdedadosMedline,BibliotecaCochrane,Lilacs, PubmedeScopusnosidiomasportuguês,inglêseespanhol,utilizandoaspalavras-chave
«artritereumatoide»,«sinovite»,«FDG»,«PET»,«metabolismoglicolítico»e«atividadeda
doenc¸a».
Resultados: Cento equarentaedoisartigosforaminicialmenteidentificados,dosquais apenas40relacionavam-sediretamenteaotema.Foramselecionados12artigosoriginaise trêsrelatosdecasoquepreenchiamoscritériosdeinclusão.
Discussão: A presenc¸a de fibroblastos e macrófagosativados no pannus é responsável pela intensa captac¸ãoperiarticular de FDG-18F. Ospadrões de captac¸ãonãopermitem
odiagnósticodiferencialcomoutrasartrites.Aintensidadedecaptac¸ãoeonúmero de articulac¸ões envolvidas sãoparâmetros metabólicosde atividadeda doenc¸aque apre-sentamboacorrelac¸ãocomosíndicescompostos.EstudoslongitudinaisdePETtêmse mostradoúteisnaavaliac¸ãodarespostaaotratamentocomanti-TNF.Quandorealizado precocemente,PETpodepredizerarespostaterapêutica.
Conclusão: Emboraorealpapeldessanovatécnicanainvestigac¸ãodaARaindanãoesteja estabelecido,PETcomFDG-18Féumaferramentapromissoranadeterminac¸ãodaatividade
enapredic¸ãoderespostaaotratamentodepacientescomAR.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isasystemicautoimmunedisease characterizedbychronicinflammationofthesynovial mem-brane.Itsprevalenceinadultsisupto1%.Whennotproperly treated,RAcanleadtoosteoarticulardestructionand func-tionallimitations,withmarkedsocioeconomicimpact.1
Rheumatoidsynovitisshowsintenseinflammatory infil-trateassociatedwithneovascularizationandproliferationof thesynovialmembrane.Thethickenedandinflamedsynovial membrane,alsoknownaspannus,isdirectlylinkedtobone andjointdestruction.2
ThediagnosisofRAinitsearlystages(upto12months aftertheonsetofthefirstsymptoms)isofparamount impor-tance for asuccessful treatment. The establishmentof an adequatetreatmentinthis period,alsoknownas“window oftherapeuticopportunity”maypreventorlimitconsiderably theconsequencesoflong-termRA.3,4However,thisdiagnosis
inanearlystagecanpresentdifficulties.Multipleconditions mayclinicallymanifestthemselvesinasimilarmannertoRA, includinginfectious diseases,systemicrheumatic diseases, spondyloarthritis,arthritis bycrystal deposition, endocrine andneoplasticdiseases.1,3,4
Laboratorytests,suchasthoseforinflammatoryactivity (erythrocytesedimentationrate[ESR]andC-reactiveprotein [CRP]) are notspecific, and rheumatoid factor (RF) may be
absentinmorethan30%ofpatientsintheearlyphaseofthe disease.5Thepreesenceofanti-proteinandanti-citrullinated
peptides(ACPA)antibodies,includinganti-citrullinatedcyclic peptide(anti-CCP)antibody,isquitespecific,butitssensitivity islimited(70-75%).[1.3]
Methodsofdiagnosticimagingsuchasconventional radio-graphy havebeenused toaidinthediagnosis ofearlyRA, but usuallythesetechniquesdetectbonyand cartilaginous structuralchangesthatoccurlateinnaturalhistoryofthe dis-ease.Ultrasonography(US)andmagneticresonanceimaging (MRI)havealsobeenemployed,andMRIshowsgreatpotential fordeterminingthethicknessofthesynovialmembraneand indetectingbonemarrowedema,beingconsideredbymany authorsasthegoldstandard(intermsofimagingprocedures) forthediagnosisofsynovitis.1,3,6
Despitemanyadvancesinunderstandingthe pathophysi-ology,diagnosisandtreatmentofRA,thecurrentprognostic anddiagnostic(clinical,laboratoryandradiographic) indica-torshavelimitedvalueforearlydiagnosisandforestablishing individualprognosis.3,7
Thedelay ofseveral weekstoestablish the diagnosisin patientswitharthritisdeprivesthosewithRAfroman ade-quate treatmentinthe therapeuticwindowofopportunity. Inthiscontext,otherdiagnosticstrategieshavebeenstudied usingnewdiagnosticimagingtechnologiesnowavailable.8
glycolyticmetabolismand,therefore,consumegreat quan-titiesofglucose.PETimagesofcancerpatientsdemonstrate intenseuptakeofradiolabeledfluorine-18fluorodeoxyglucose (18F-FDG)bymalignanttumorsandtheirmetastases.9
18F-FDG is a glucose analogue linked to a radioactive
isotope,fluorine-18.Thismoleculebehavessimilarlyto glu-cose,being avidlytaken upbycells withintenseglycolytic metabolism. It has long been known that infectious and inflammatoryprocessesalsoexhibithighuptakeof18F-FDG.
The increased expression of glucose transporter proteins (GLUTtypesIand III)bymembranesofleukocytes present ininflammatorysites,mainlyneutrophilsandmacrophages, leads to this uptake. This pathophysiological mechanism explainswhytheintensityof18F-FDGuptakeisdirectly
pro-portional to the intensity of the activity of inflammatory processes.10–12
Therefore, 18F-FDG PET is able to directly detect and
quantify articular and extra-articular sites of increased inflammatoryactivity. That puts this tool atan advantage overotherdiagnosticimagingmethods,whichdetectindirect changesofRA,suchaserosions(radiography),increasedblood flow (Doppler),increased thickening of the synovial mem-brane(ultrasonography), thepresenceofboneedema(MRI) orincreasedosteoblasticactivity(bonescan).
ThefirstreportsoftheuseofPETinRAaredatedfrom1995. Researchers at Massachusetts General Hospital in Boston reported the occurrence of strong 18F-FDG uptake in two
patientsdiagnosedwithRAandwithclinicallyactivesynovitis intheirwrists.13Sincethen,theutilityof18F-FDGPETinthe
managementofRAhasbeeninvestigatedbyseveralauthors.
Purpose
Thepurposeofthisstudywastoconductasystematicreview ofthe current literatureon the role of18F-FDGPET inthe
diagnosis,assessmentofdiseaseactivityandmonitoringthe efficacyoftreatmentwithdisease-modifyingantirrheumatic drugs(DMARDs)inpatientswithRA.
Methods
Intheperiodfrom MarchtoJune2011,searcheswere con-ductedthroughthefollowingdatabases:Medline(1980-2012), TheCochraneLibrary,Lilacs,Pubmed(1980-2012)andScopus in Portuguese, English and Spanish languages. The key-wordsusedwere“rheumatoidarthritis”(artritereumatoide), “synovitis” (sinovite), “FDG”, “PET”,“glycolytic metabolism” (metabolismoglicolítico)and“diseaseactivity”(atividadeda doenc¸a).
Inclusioncriteriawere:originalarticlesandcasereports thataddressedtheroleofPETinrheumatoidarthritisandthat containedanadequatedescriptionofthematerials,methods andresultsachieved.Reviewarticles,letterstotheeditorand editorialswereexcluded.
Thetitleandabstractofthearticlesobtainedintheinitial searchwerereviewedbytwoindependentobserversinorderto identifythosethatwererelevant.Areviewofthefullversion wasperformedonallthosepaperswhichmettheinclusion
criteria;andthereferencesofthesearticleswereanalyzedin ordertodrawattentiontoadditionalsources.Forthepurposes ofthisstudy,wereconsideredthepapersselectedaftermutual agreementofthetwoobservers.
From the manuscriptsselected, thefollowingdata were observed: typeof study,samplesize, toolsused, statistical analysisandresults.
Results
Onehundredand forty-twoarticleswereinitiallyidentified inthe databasesmentioned,ofwhichonly40were related directlytothetopicsearched.Ofthese,14wereexcludedfor beingreviewarticles,sixfornotincludingpatientswithRA, fourbecausetheydidnotcontainanadequatedescriptionof materialsandmethods,andonebecauseitdidnotuse18
F-FDGasradiotracer(Table1).The12selectedoriginalarticles wereclassifiedbytheauthorsasexperimentalstudies, diag-nosisstudies,assessmentofdiseaseactivity,andassessment oftreatmentresponse.Table2summarizesthetypesof stud-ies,thesamplesanalyzed,themaintechnicalcharacteristics, clinicalindicesandotherdiagnosticmethodsusedbythe dif-ferentarticles,aswellastheirprimaryendpoint.Threecase reportswerealsoincluded.
Experimentalstudies
Experimental studies in animals and cell cultures have investigatedthe pathophysiologicalmechanisminvolvedin periarticularuptakeof18F-FDGinpatientswithRA.Matsui
et al.14 usedan animalmodel(rats). Arthritiswas induced
byintradermal injectionofbovinecollagen. Ratswere sac-rificedimmediately afterperformingPETimages. Histology andmacroautoradiographyofjointswitharthritiswere com-paredtoPETimages.Itwasobservedthatareasofmarked uptakeof18F-FDGcorrespondedtoareasofpannusandbone
destruction;ontheotherhand,moderatelyhighuptakeareas were representedbyhyperplasiaofsynoviallayercells and bythepresenceofinflammatoryinfiltrate.Neutrophilsand macrophageswerethepredominantcellsinthesesites.
The authors also conducted an in vitro assay to deter-mine3H-FDGuptakebyneutrophils,macrophages,fibroblasts
and T cells exposed tocertain pro-inflammatory cytokines (TNF␣,IL-1andIL-6).The3H-FDGuptakebymacrophageswas
higher whenstimulatedbyTNF␣ versusIL-1 orIL-6. Fibro-blastsexhibitedamoreintenseuptakethanthatobservedin macrophages,especiallyinresponsetostimulationbyTNF␣or IL-1.Incontrast,noincreasein3H-FDGuptakewasobserved
inresponsetoinflammatorycytokinesinneutrophilsandT lymphocytes.Theseresultssuggestthattheglycolytic hyper-metabolismobservedinjointsofpatientswithRAisclosely relatedtothe presenceofpannusandtothe infiltrationof activatedmacrophagesandfibroblasts.14
Thus,thereissomepathophysiologicalsubstratetoexplain theavidityforlabeledglucosebyinflammatorycellspresent inthepannus.Suchobservationsjustifywhy18F-FDGPETis
rev bras reumatol.2014;54(6):474–482
477
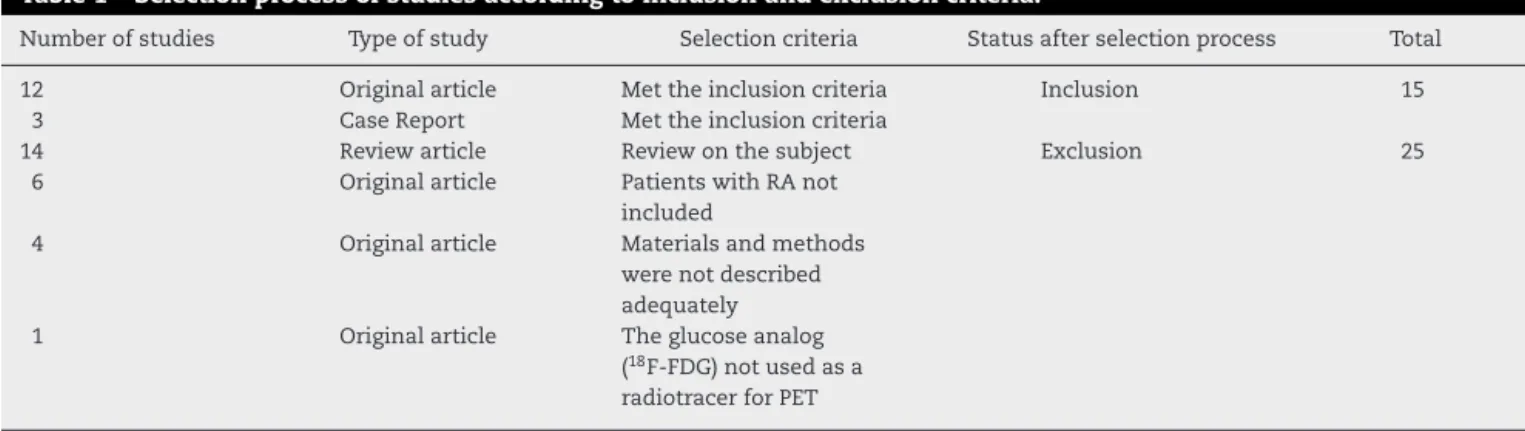
Table1–Selectionprocessofstudiesaccordingtoinclusionandexclusioncriteria.
Numberofstudies Typeofstudy Selectioncriteria Statusafterselectionprocess Total
12 Originalarticle Mettheinclusioncriteria Inclusion 15
3 CaseReport Mettheinclusioncriteria
14 Reviewarticle Reviewonthesubject Exclusion 25
6 Originalarticle PatientswithRAnot
included
4 Originalarticle Materialsandmethods
werenotdescribed adequately
1 Originalarticle Theglucoseanalog
(18F-FDG)notusedasa radiotracerforPET
RA,rheumatoidarthritis;PET,positronemissiontomography.
synovial membrane. This knowledge has led several researcherstoexamine18F-FDGPETasamethodcapableof diagnoseanddemonstratetheactivityofAR.
Diagnostics
Inflammatoryarthritisandprolongedmorningstiffness, asso-ciated with the presence of rheumatoid factor and other positive serum autoantibodies, and elevated inflammatory activitytestsfavorthediagnosisofRA.1,3However,oftenthe
clinicalandlaboratorymanifestationsarenottypical.Forthis reason,RAdiagnosishasbeenbasedonpre-established clini-calandlaboratorycriteria.15SomeauthorshaveevaluatedPET
asatoolinthedifferentialdiagnosisofarthritides.
Okabeetal.16 attemptedtoestablishspecificpatternsof 18F-FDGuptakeforRAabletodifferentiatethisdiseasefrom
otherarthritides.Seventypatientswitharthritis,30withRA, were included in astudy withthe aim toestablish a pat-tern of distribution of 18F-FDG. Ninety percent ofpatients
withRAexhibitedpolyarticularhypermetabolism.However, otherdiseasesalsodemonstratedthispatternofpolyarticular hypermetabolism,suchasmixedconnectivetissuedisease, systemicsclerosisandRS3PEsyndrome(Remitting Seroneg-ativeSymmetricalSynovitiswithPittingEdemasyndrome). TheatlantoaxialinvolvementwasuniquetopatientswithRA. Somesitesofhypermetabolismwerecharacteristicofother diseases,suchassacroiliacjointuptakeinpatientswith anky-losingspondylitis;liver,spleenandbonemarrowincreased uptakeinpatientswithadultStill’sdisease;andarterial hyper-metabolisminpatientswithpolymyalgiarheumatica.
Itshouldbenotedthatsitesofextra-articularactivityofAR mayalsoexhibithypermetabolism,suchaslymphnodesand subcutaneousnodules17,18andthissubjectwasnotaddressed
byOkabeetal.;16thiscouldhavecontributedtothe
differen-tiationofarthritides(Fig.1).
Elzinga et al.19 compared PET images in patients with
RA(n=17), osteoarthritis(n=6),and fibromyalgia(n=5).As might be expected, patients with fibromyalgia showed no areas ofarticular hypermetabolism.The number of hyper-metabolic joints in patients with RA(88) was significantly higherthaninpatientswithosteoarthritis(12)(P<0.001). How-ever,uptakeintensitywasnotstatisticallydifferentbetween
thetwogroups.ThisindicatesthatPETdoesnotwork ade-quately as a tool for the differential diagnosis of these diseases.
Assessmentofdiseaseactivity
TheactivityofRAcanbemeasured byseveralclinical, lab-oratory andradiologicalparameters. Thecompositeindices ofdisease activity are the mostused and acceptedamong rheumatologists. Methodsofdiagnostic imaginghave been reservedforspecificcases.3,6
There are several studies relating the findings of PET scans with indices of disease activity and other methods of diagnostic imaging, such as ultrasonography (US) and magneticresonanceimaging(MRI).Roivainenetal.20
demon-stratedagoodcorrelationbetweenintensityof18F-FDGuptake
(standarduptakevalue[SUV])withthevolumeofthe syno-vialmembranein10patientswithclinicallyactivesynovitis. Palmer et al.21 founda good correlation betweenSUV and
thevolumeofpannuswhichwasenhancedunderthe para-magneticcontrastfat-suppressedweightedMRIin12patients witharthritis.
Beckersetal.22comparedthefindingsofPETscanswith
clinical,laboratoryandultrasonographicparametersofRA.A prospectivestudywasconductedincluding21patientswith clinicallyactiveRA(ACRcriteria1987)using18F-FDGPET.The
meanDAS28was7.4(5.2-8.5)andmeanSDAIwas60.2
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
4;
5
4(6)
:474–482
Table2–Typesofstudy,analyzedsamples,maintechnicalcharacteristics,clinicalindicesandotherimagingmethodsused.
Authorand reference
StudyDesign Numberof
participants
Numberof controls
Technical procedure used
Joints evaluatedby
patient
Otherclinical indicesordiagnostic
methods
Primary Outcome
Matsuietal.15 Experimental
study
5 4 PET - Macroautoradiography,
Histology
ToComparePETwith
macroautoradiographyandhistology Okabeetal.16 Retrospective
clinicalstudy
72patients (30withRA)
- PETorPET/CT 19 - Diagnosis
Elzingaetal.19 Crossover
clinicalstudy
14withRA,6 withOA
5withFM PET 22 - Diagnosis
Palmeretal.21 Prospective
clinicalstudy
12withUA - PET 1 MRI Assessmentofdiseaseactivity
Roivanenetal.20 Prospective
clinicalstudy
2withRA,6 withUA,1 withAS,1 USA
- PET 1
Contrast-enhanced MRI
Assessmentofdiseaseactivity
Beckersetal.22 Prospective
clinicalstudy
21withRA 13without arthralgia
PET 12or22 US,SDAI,DAS28 Assessmentofdiseaseactivity
Goerresetal.23 Prospective
clinicalstudy
7withRA - PET 28 DAS28,RDAI Assessmentofdiseaseactivity
Kubotaetal.24 Retrospective
clinicalstudy
18withRA - PET/CT 13 CRP,jointcount Assessmentofdiseaseactivity
Beckersetal.25 Cohortstudy 16withRA - PET 1 US,MRI,CRP,
MMP-3
Assessmentoftreatmentresponse
Okamuraetal.26 Cohortstudy 22withRA - PET/CT 12 US,MRI,DAS
28,
DAS28-CRP,ESR,
CRP,MMP-3,RF
Assessmentoftreatmentresponse
Elzingaetal.27 Exploratory
study
16withRA - PET 12 CRP,ESR,MHAQ,
VAS
Assessmentoftreatmentresponse
Satoetal.29 Prospective
clinicalstudy
6withRA - PET 2 DAS28,joint
count,ESR,CRP
Assessmentoftreatmentresponse
RA,rheumatoidarthritis;OA,osteoarthritis;UA,undifferentiatedarthritis;AS,ankylosingspondilitis;USA:undifferentiatedspondyloarthritis;FM:fibromyalgia;PET,positronemissiontomography; PET/CT,positronemissiontomographywithcomputedtomography;US,ultrasonography;MRI,magneticresonanceimaging,SDAI,simplifieddiseaseactivityindex;DAS28,diseaseactivityscore;
rev bras reumatol.2014;54(6):474–482
479
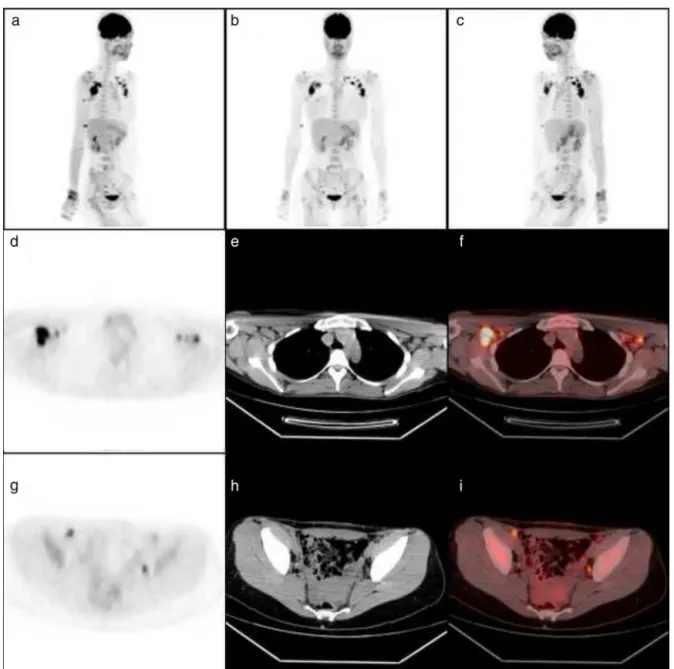
Figure1–18F-FDGPETofafemalepatient,28yearsold,complainingofsymmetricalpolyarthralgia,especiallyinvolving
handsandwristsandassociatedwithprolongedmorningstiffness.LaboratorytestsrevealedanESR=81mm,positive rheumatoidfactor(40.2IU/mL)andananticitrullinatedpeptideantibodystronglypositive(82.5IU/mL).The
three-dimensionalreconstructionimages(a,b,c)showhighuptakeinshoulders,wrists,metacarpophalangealand proximalinterphalangealjointsofthehandsandhips.TomographicimagesofPET(d,g),CTscans(e,h)andPET/CT(f,1) showingintensehypermetabolisminbilateralaxillaryandpelviclymphnodes(personalfile).
compositeindicesofthediseaseactivity(DAS28andSDAI)was
consideredsignificant(r=0.90,P<0.0001).
Theanalysisoftheseresultssuggeststhatthemetabolic activityofsynovitisdemonstratedby18F-FDGPETcanreflect
diseaseactivitywithagoodcorrelationwithDAS28andSDAI.
However,thesmallnumberospatientsandtheprevalenceof RApatientswithhighdiseaseactivityinthisstudylimitits conclusions.
Goerresetal.23proposedavisualscoretoquantify
metabol-ically active joints with PET. Seven patients with DAS28 ≥
4.2wereincluded.Anindexofzeroto4(zerofornouptake
and 4 for a marked uptake) was assigned to each of the 28 joints usually assessedby compositeindices of disease activity.TheSpearmantestshowedasignificantcorrelation betweenvisualscoringbyPETandDAS28.PETalsorevealed
sites of extra-articular (tendons and bursae) uptakein six ofsevenpatients.However,onceagainthesmallnumberof patients included didnot allowany extrapolation ofthese findings.
Kubotaetal.24usedPETscanwithafocusonlargejoints.
Eighteen RA patients underwent 18F-FDG PET/CT to study
wrists,carpals,hipsandknees).PET/CTisacombinationof functionalpositron emissiontomographyequipment and a computedtomography.Fourpatientswereinclinical remis-sionand14presentedwithclinicallyactiveRA.Amodified Goerres et al.23 score was used. The number of affected
joints and the total score of PET were significantly differ-entamongpatientsinremissionand withactiveRA.There wasalsoapositivelinearcorrelationbetweenthetotalscore withPET and serum levels ofCRP(r=0.658, P=0.003). Five patients(28%)showedhypermetabolismintheatlantoaxial joint.Thepresenceofhypermetabolicaxillarylymphnodes wascorrelatedwiththesuperiorlimbsjointsuptake(r=0.731, P=0.000004).
Monitoringtreatmentresponse
Thetreatmentwithsynthetic DMARDshaslowcost. How-ever,biologicalDMARDshavehighcostandcausenumerous adverseeffects.Inthiscontext,18F-FDGPEThasbeenusedas
anattempttodiscriminatewhosepatientscanbenefitfrom thistypeoftreatment.Beckersetal.25compared18F-FDGPET
withcontrast-enhancedMRIandUSinthetreatmentresponse evaluation.SixteenpatientswithactiveRAunderwent whole-body PET,contrast-enhancedMRIand US ofoneknee (i.e., the joint referred to by patients as that with moresevere pain) before and after four weeks oftreatment with anti-TNF(drugnotspecifiedbytheauthors).Metabolicallypositive kneesshowedgreatersynovialthicknessandamoreintense paramagneticcontrastenhancement.Therewasgood correla-tionbetweentheintensityof18F-FDGuptake(SUV),synovial
thicknesswithUSandenhancementbyparamagnetic con-trastwithMRI.Afterfourweeksoftreatmentwithanti-TNF, asignificantdecreaseinSUVandinparamagneticcontrast enhancementoccurred,butwithoutasignificantreductionin synovialthickness.Thesedatashowthattheresponseto bio-logicaltreatmentscanbedemonstratedbyPETimageswith respecttothemetabolicaspect,beforetheobservationofa significantreductioninsynovialthicknessby ultrasonogra-phyor MRIstudies.However,ofallpossibly affectedjoints inthese16 patients,the study onlyevaluatedalargejoint (knee).Thisoccurredduetoatechnicallimitationof contrast-enhancedMRI,whichisamethodthatstudiesonlyonejoint areaatatime,spending30-40minutesforeach region.PET shows great advantage in this regard, since it can assess alljoints ofthebody inasingleexamination,withsimilar duration.
Okamuraetal.26 studied22patientswithpoorresponse
tosyntheticDMARDs,includingmethotrexate,andwith indi-cationfortreatmentwithbiologicDMARDs(etanerceptin16 andinfliximabin6).Allpatientsunderwent18F-FDGPET/CTat
baselineandsixmonthsaftertheinitiationoftherapy.DAS28,
DAS28-CRP,ESR,CRP,matrixmetalloproteinase-3(MMP-3)and
RF were determined on the same days ofPET/CT. Patients had moderatetohigh RAactivity (meanDAS28:5.29±1.01; minimum:3.47andmaximum: 6.95).Allclinical,laboratory andmetabolicparametersshowedsignificantdecreaseafter sixmonthsoftreatment(meanDAS28:3.81±0.86,minimum:
2.21andmaximum:5.33).Therewasgoodcorrelationamong valuesofSUV,DAS28 and DAS28-CRP. Thedecrease in SUV
also correlated with the decrease in values of DAS28 and
DAS28-CRP.TheseresultsshowthatPETcanbeanalternative
methodforobjectivelymeasuringdiseaseactivityand deter-miningtheresponsetotherapywithanti-TNFinarelatively simpleandstraightforwardmannerandwithgoodcorrelation withtheindicesmorecommonlyusedbyrheumatologistsfor suchpurposes.
Elzinga et al.27 investigated the potential of 18F-FDG
PET to predict the therapeuticresponse toinfliximab. Six-teen patients with at least two swollen or painful joints (metacarpophalangealand/orwrists)wereenrolledfor treat-mentwithsubcutaneousinjectionsofinfliximabatweeks0, 2,6,14and22.ThedeterminationofthevaluesofCRPand ESR,aswellasthecountingof28painfulorswollenjoints, wasperformedatthesameintervals.TheEuropeanLeague AgainstRheumatism(EULAR)criteria15wereusedtoclassify
theresponsetotreatmentasgood(n=5),moderate(n=8)and non-responders (n=3).PETstudies ofmetacarpophalangeal jointsand wristswereperformedbeforethetreatmentand aftertwoweeks.TheresultsshowedthatthechangeinSUV betweenzeroandtwoweekscorrelatedwithDAS28atweeks
14and22(r=0.62,P<0.05;r=0.65,P<0.01,respectively).The changeofthecomponentsofDAS28(ESR,CRP,jointcounting,
visual analoguescale) intheinterval oftwo weeksdidnot correlatewithDAS28atweeks14and22.Alogisticregression
analysisshowedthatSUVreductionwastheonlysignificant predictive factorfordeterminingDAS28 atweeks14and 22
(=0.62,P<0.05;=0.65,P<0.01,respectively).Theresults obtained in this small group ofpatients suggest that 18
F-FDGPETofwristsandmetacarpophalangealjoints,performed withonlytwoweeksoftreatment,canpredictthesystemic response to infliximabafter 14 and 22 weeks.Considering the highcostofthis treatment,this studyencouragesnew researchprojectsusing 18F-FDGPETasatooltodetermine
whichpatientsmaybenefitfromthelong-termtreatmentwith infliximab,savingalotofmoneyforhealthsystems, consider-ingsuchacostlytreatment.Thisstrategyalsocouldprovideto non-responderstoinfliximabthechanceofatreatmentwith otherbiologicalDMARDs.
Thetherapeuticeffectsofacupuncture inthetreatment ofpatientswithRAhavealsobeenunderinvestigation.Sato etal.28includedonlysixpatientsintheirresearch.Allofthem
reportedimprovementinpain,functionalcapacityand qual-ityoflifeaftertwomonthsoftreatmentwithacupuncture. However, 18F-FDG PETshowed no change inthe metabolic
activity of the affected joints. The inflammatory activity tests(CRPandESR) didnotshowsignificant variationafter acupuncture.Theseresultssuggestthatacupuncturehasno anti-inflammatoryeffectinpatientswithRA.
Conclusions
Althoughthenumberofstudiesontheroleof18F-FDGPETin
RAislimited,andconsideringthesmallnumberofpatients enrolled bymost studies published with this purpose, the datapresentedinthisreviewallowsustomakesome con-siderations.18F-FDGPETisanon-invasiveimagingmethodof
rev bras reumatol.2014;54(6):474–482
481
Itshighcostcanbeevaluatedinarelativemanner,whenwe considerthatthisisanassessmentofthewholebody, allow-ing the study ofall joints at once.Its abilitytodetermine andpredict earlierthe responsetotreatmentwithbiologic DMARDsconstitutesafactorthatdeservesamoreprofound analysisinfutureinvestigations.Newprospective longitudi-nalrandomizedstudiesareneededtoconsolidatethismethod ofdiagnosticimaging.
Although the actual role of this new technique in the investigationofRAisnotyetestablished,18F-FDGPETisa
promisingtoolforthedeterminationofdiseaseactivityand intheassessmentandprediction oftreatment responsein patients with RA. It might be that in the future, 18F-FDG
PET will playa moreimportant role in the diagnosis and assessmentofdiseaseactivity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ScottDL,WolfeF,HuizingaTW.Rheumatoidarthritis.Lancet. 2010;376:1094–108.
2. McInnesIB,SchettG.Thepathogenesisofrheumatoid arthritis.NEnglJMed.2011;365:2205–19.
3. daMotaLM,CruzBA,BrenolCV,PereiraIA,FronzaLS,Bertolo MB,etal.ConsensusoftheBrazilianSocietyofRheumatology fordiagnosisandearlyassessmentofrheumatoidarthritis. RevBrasReumatol.2011;51:199–219.
4. daMotaLM,CruzBA,BrenolCV,PereiraIA,Rezende-Fronza LS,BertoloMB,etal.2012BrazilianSocietyofRheumatology Consensusforthetreatmentofrheumatoidarthritis.Rev BrasReumatol.2012;52:152–74.
5. daMotaLM,dosSantosNetoLL,BurlingameR,MénardHA, LaurindoIM.Laboratorycharacteristicsofacohortofpatients withearlyrheumatoidarthritis.BrazJRheumatol.
2010;50:375–88.
6. daMotaLMH,LaurindoIMM,Santos-NetoLL,LimaFAC, VianaSL,MendlovitzPS,etal.Imagingdiagnosisofearly rheumatoidarthritis.RevBrasReumatol.2012;52:757–66. 7. AndersonJ,CaplanL,YazdanyJ,RobbinsML,NeogiT,
MichaudK,etal.Rheumatoidarthritisdiseaseactivity measures:AmericanCollegeofRheumatology
recommendationsforuseinclinicalpractice.ArthritisCare Res(Hoboken).2012;64:640–7.
8. ØstergaardM,PedersenSJ,DøhnUM.Imaginginrheumatoid arthritis-statusandrecentadvancesformagneticresonance imaging,ultrasonography,computedtomographyand conventionalradiography.BestPractResClinRheumatol. 2008;22:1019–44.
9. FletcherJW,DjulbegovicB,SoaresHP,SiegelBA,LoweVJ, LymanGH,etal.RecommendationsontheUseofF-18FDG PETinOncology.JNuclMed.2008;49:480–508.
10.MochizukiT,TsukamotoE,KugeY,KanegaeK,ZhaoS, HikosakaK,etal.FDGuptakeandglucosetransporter subtypeexpressionsinexperimentaltumorand inflammationmodels.JNuclMed.2001;42:1551–5.
11.ZhaoS,KugeY,TsukamotoE,MochizukiT,KatoT,Hikosaka K,etal.EffectsofinsulinandglucoseloadingonFDGuptake inexperimentalmalignanttumoursandinflammatory lesions.EurJNuclMed.2001;28:730–5.
12.YamadaS,KubotaK,KubotaR,IdoT,TamahashiN.High accumulationoffluorine-18-fluorodeoxyglucosein turpentine-inducedinflammatorytissue.JNuclMed. 1995;36:1301–6.
13.PolissonRP,SchoenbergOI,FischmanA,RubinR,SimonLS, RosenthalD,etal.Useofmagneticresonanceimagingand positronemissiontomographyintheassessmentofsynovial volumeandglucosemetabolisminpatientswithrheumatoid arthritis.ArthritisRheum.1995;38:819–25.
14.MatsuiT,NakataN,NagaiS,NakataniA,TakahashiM, MomoseT,etal.Inflammatorycytokinesandhypoxia contributeto18F-FDGuptakebycellsinvolvedinpannus formationinrheumatoidarthritis.JNuclMed.2009;50: 920–6.
15.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO,3rd,etal.2010Rheumatoidarthritisclassificationcriteria: anAmericanCollegeofRheumatology/EuropeanLeague AgainstRheumatismcollaborativeinitiative.Arthritis Rheum.2010;62:2569–81.
16.OkabeT,ShibataH,ShizukuishiK,YoneyamaT,InoueT, TateishiU.F-18FDGuptakepatternsanddiseaseactivityof collagenvasculardiseases-associatedarthritis.ClinNucl Med.2011;36:350–4.
17.SeldinDW,HabibI,SoudryG.Axillarylymphnode visualizationonF-18FDGPETbodyscansinpatientswith rheumatoidarthritis.ClinNuclMed.2007;32:
524–6.
18.dosAnjosDA,doValeGF,CamposCM,doPradoLF,Sobrinho AB,daCunhaAL,etal.Extra-articularinflammatorysites detectedbyF-18FDGPET/CTinapatientwithrheumatoid arthritis.ClinNuclMed.2010;35:540–1.
19.ElzingaEH,vanderLakenCJ,ComansEF,LammertsmaAA, DijkmansBA,VoskuylAE.2-Deoxy-2-[F-18]fluoro-D-glucose jointuptakeonpositronemissiontomographyimages: rheumatoidarthritisversusosteoarthritis.MolImagingBiol. 2007;9:357–60.
20.RoivainenA,ParkkolaR,Yli-KerttulaT,LehikoinenP,Viljanen T,MöttönenT,etal.Useofpositronemissiontomography withmethyl-11C-cholineand2-18F-fluoro-2-deoxy-D-glucose incomparisonwithmagneticresonanceimagingforthe assessmentofinflammatoryproliferationofsynovium. ArthritisRheum.2003;48:3077–84.
21.PalmerWE,RosenthalDI,SchoenbergOI,FischmanAJ,Simon LS,RubinRH,etal.Quantificationofinflammationinthe wristwithgadolinium-enhancedMRimagingandPETwith 2-[F-18]-fluoro-2-deoxy-D-glucose.Radiology.
1995;196:647–55.
22.BeckersC,RibbensC,AndréB,MarcelisS,KayeO,MathyL, etal.Assessmentofdiseaseactivityinrheumatoidarthritis with(18)F-FDGPET.JNuclMed.2004;45:956–64.
23.GoerresGW,ForsterA,UebelhartD,SeifertB,TreyerV,Michel B,etal.F-18FDGwhole-bodyPETfortheassessmentof diseaseactivityinpatientswithrheumatoidarthritis.Clin NuclMed.2006;31:386–90.
24.KubotaK,ItoK,MorookaM,MitsumotoT,KuriharaK, YamashitaH,etal.Whole-bodyFDG-PET/CTonrheumatoid arthritisoflargejoints.AnnNuclMed.2009;23:
783–91.
25.BeckersC,JeukensX,RibbensC,AndréB,MarcelisS,Leclercq P,etal.(18)F-FDGPETimagingofrheumatoidkneesynovitis correlateswithdynamicmagneticresonanceand
sonographicassessmentsaswellaswiththeserumlevelof metalloproteinase-3.EurJNuclMedMolImaging.
2006;33:275–80.
27.ElzingaEH,vanderLakenCJ,ComansEF,BoellaardR, HoekstraOS,DijkmansBA,etal.18F-FDGPETasatoolto predicttheclinicaloutcomeofinfliximabtreatmentof rheumatoidarthritis:anexplorativestudy.JNuclMed. 2011;52:77–80.