rev bras ortop.2013;48(6):574–577
w w w . r b o . o r g . b r
Case
Report
Segmental
Stress
Fracture
of
Tibia
in
Recreational
Running:
A
Case
Report
夽
,
夽夽
Alexandre
de
Paiva
Luciano
a,b,∗,
Nelson
Franco
Filho
c,
Fernando
Adami
d,
Luiz
Carlos
de
Abreu
daDepartmentofMedicine,UniversityofTaubaté,Taubaté,SP,Brazil
bStudyGrouponSportsArthroscopyandTraumatology,UniversityHospitalofTaubaté,Taubaté,SP,Brazil
cOrthopedicsandTraumatologyService,UniversityHospitalofTaubaté,Taubaté,SP,Brazil
dABCSchoolofMedicine,SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13August2012
Accepted19October2012
Keywords:
Fractures,stress
Tibia Running Athletes
a
b
s
t
r
a
c
t
Oneofthefirststepstobetakeninordertoreducelesionsinsports,suchasstressfractures,
istoknowthenatureandextensionofthispathology.Whatfollowsisacasereportof
segmentalstressfractureofthetibiainrecreationalathletes,whichisconsideredsomewhat
rareintheliterature.Casereport:a40-year-oldfemalepatientwhostartedtohavefollow-up
medicalchecksduetounusualpaininherrightleg,concentratedmainlyontheproximal
regionofthekneeandankle,aftera10-kmrunforaperiodofonemonth.Segmentalstress
fractureofthetibiawasdiagnosedafterclinicalresearchandfurtherexaminations.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Fratura
por
estresse
segmentária
na
tíbia
em
corredora
recreacional
Palavraschave:
Fraturasdeestresse
Tíbia Corrida Atletas
r
e
s
u
m
o
Osprimeirospassosparasereduziremlesões,comoafraturadeestressenoesporte,é
conhecereaprofundaroestudodanaturezaeaextensãodessapatologia.Aseguir,
apre-sentamosumrelatodecasodefraturaporestressesegmentardatíbia,consideradorarona
literaturaconsultada.Descric¸ãodoquadroclínico:trata-sedepacientede40anos,feminino,
queiniciouseguimentomédicopordoresincaracterísticasnapernadireita,concentradas
principalmenteemregiãoproximaldojoelhoedotornozelodireitos,duranteapráticade
corridaderuade10kmhaviaummês.Apósinvestigac¸ãoclínicaepormeiodeexames
complementares,diagnosticou-sefraturadeestressesegmentardatíbia.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Todososdireitosreservados.
夽Pleasecitethisarticleas:dePaivaLucianoA,FilhoNF,AdamiF,deAbreuLC.Fraturaporestressesegmentárianatíbiaemcorredora
recreacional.RevBrasOrtop.2013;48:574–577.
夽夽
WorkdoneattheDepartmentofOrthopaedicsandTraumatology,DepartmentofMedicine,UniversityofTaubaté,Brazilandthe
DisciplinesMethodologyofScientificResearchandScientificWriting,SantoAndré,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.dePaivaLuciano).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
rev bras ortop.2013;48(6):574–577
575
Introduction
Withthegrowingconcernforhealthandqualityoflifethat
hasbeenseen particularlyoverthe lasttwodecades,
ever-greaternumbersofpeopleareseentobedoingexercise.This
hasledtoaconsiderableincreaseinthefrequencyof
diag-nosesofstressfractures.Theseinjurieshaveanundesirable
effect,sincetheyreducethebenefitsrelatingtosportsandact
asabarrieragainstmaintaininghealthandqualityoflife.
Thefirststeptowardsdiminishingsportsinjuriessuchas
stressfracturesistohavein-depthknowledgeofthenature
andextentofthesepathologicalconditions.
Inthefollowing,wepresent acasereportonsegmental
stressfractureofthetibia.
Description
of
the
Clinical
Condition
The patient was a 40-year-old woman born and living in
Taubaté(SP).Shesaidthatshehadbeenpracticingrunningin
thestreetsforsixmonthsandshewascurrentlybeing
accom-paniedbyasportsadviser.Hertrainingwasdividedintofour
sessionsperweek,namely:a“regenerative”runonMondays;
“sprint”trainingonanathleticsrunningtrackonWednesdays,
“pace”trainingonFridays;andlongtrainingorcompetitions
atweekends.Thepatientwasdoingregularsportspractice,
butsaidthathervolumewasgraduallyincreasingandthat
shehadstartedhigh-intensitytrainingonanathleticsrunning
tracktwomonthsearlier.
Shestartedtohavemedicalfollow-upduetounusualpain
inherrightleg,concentratedmainlyintheregionoftheright
kneeandankleduring10-kmpracticerunsonemonthearlier.
Shesaidthatshehadnotbeenmaking chronicuseofany
medications,hadnothadanyprevioussurgeryandhadnot
hadanypreviouslydiagnosedchronicdiseases.
On physicalexaminationat the timeof admission, she
weighed65kg,herheightwas1.72mandherBMIwas21.97.
Shedidnothaveanypathologicalfascies.
Evaluation of the type of static and dynamic steps:
pronatedsteps.
Physicalexaminationoftheknee:
• Inspection:knees withphysiologicalvalgusinfrontview,
withoutrecurvatuminlateralview;withoutanyincreasein
volume.
• Bone palpation: medial tibial plateau painful on
palpa-tion,butwithoutpainonpalpationofthemedialfemoral
condyle.
• Palpationofsofttissues:medialcollateralligamentpainful
onpalpationatitsinsertioninthetibia.Sartorius,gracilis
and semitendinosusmusclespainfulattheirinsertionin
thetibia.
• Jointstabilitytests:negative.
• Meniscaltests:negative.
• Patellofemoraltests:negativeforpatellofemoralsyndrome.
• Degreeofmobility:extension0◦,flexion135◦,internaland
externalrotation10◦.
Physicalexaminationontheankle:
• Inspection:pronatedsteponwalkingandrunning.
• Bonepalpation:medialstructures–painonmedial
palpa-tionofthedistaltibia;lateralstructures–nopain.
• Palpation ofsoft tissues: regions of interest – Zone III –
medialmalleolus:deltoidligament,tendons:posteriortibial
tendon,longflexorofthetoesandlongflexorofthehallux
freefrompain;ZoneIV–dorsumofthefootbetweenthe
malleoli:tendons:anteriortibialtendon,longextensorof
thehalluxandlongextensorofthetoesfreefrompain.
• Anklestabilitytests:negative.
• Degreeofjointmobility:dorsiflexion20◦,plantarflexion50◦,
subtalarinversion5◦andsubtalareversion5◦.
Basedon the physicalexaminationdescribed above,we
continued the diagnostic investigation and the search for
associatedpathologicalconditionsbymeansofthefollowing
examinations:
• Radiologicalexaminations:radiographsandscanometryon
thelowerlimbs–withoutsignificantalterations;rightlower
limb:920.1mm;leftlowerlimb:920.4mm(Fig.1).
• BonedensitometryonApril23,2010(Fig.2):patternwithin
normalityfortheproximalregionofthefemur.
576
rev bras ortop.2013;48(6):574–5771.42
1.18
0.94
40 60 80 0
2 100
2.0
0.0
–2.0
–4.0 0.70
Age (years)
BMD g/cm
2
L1-L4 Comparison with references
T
value
Osteoporosis* Osteopenia* Normal*
Figure2–Bonedensitometry.
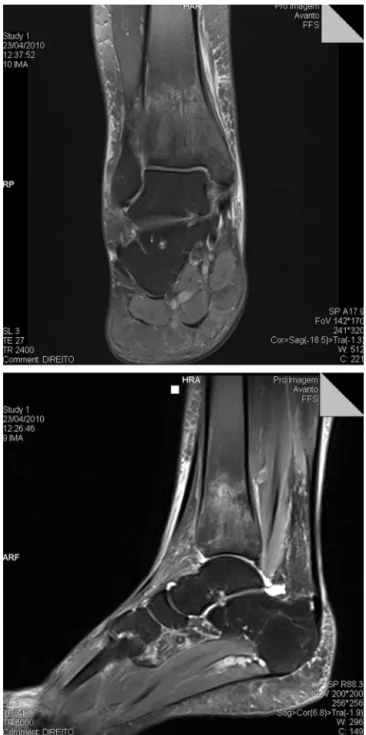
• MagneticresonanceimagingoftheankleonApril23,2010
(Fig.3).
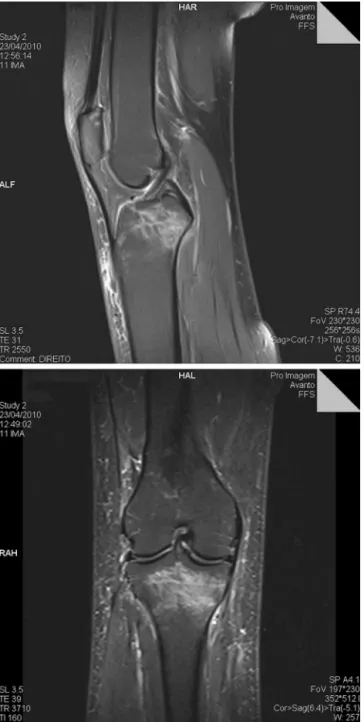
• MagneticresonanceimagingofthekneeonApril23,2010
(Fig.4).
Discussion
Insportspractice,stressfracturesareclinicalentitiesthatalso
fitintothewell-knownoverusesyndrome.1,2
The etiology of stress fractures can be best described
asacceleratedboneremodelinginresponsetosubmaximal
repetitivestress.Thebonerespondsandformsnewperiosteal
boneasanextrareinforcement.However,iftheosteoclastic
activitycontinuestoexceedthemeannumberofosteoblasts
fornewboneformation,afractureinthecorticalbonemay
eventuallyoccur.3
Therisksoffractureduetostressareinfluencedbyvarious
factorsandaredividedintointrinsicfactors(sex,age,ethnicity
andmusclestrength),extrinsicfactors(trainingregimen,type
offootwearused,trainingsurfaceandtypeofsport),
biome-chanicalfactors(bonemineraldensityandbonegeometry),
anatomicalfactors(footmorphology,leglengthdiscrepancy
andknee alignment), hormonalfactors(delayedmenarche,
menstrualdisordersandcontraceptives)andnutritional
fac-tors(calciumandvitaminDdeficiencies,fooddisordersand
thefemaleathletetriad).2,3
Studieshaveshownthatfemaleathletespresentgreater
numbersofstressfracturesthanshownbymen.3,4
Stressfracturesgenerallyoccuringroupsofyoung
indi-vidualswhoaresubjectedtointensephysicalactivities,such
asmilitaryrecruits,dancers,runnersandathletesingeneral.
This typeof fracture occurs mainly inbones of the lower
extremities,such asthe metatarsus,fibula, calcaneus and,
mostfrequently,thetibia.5
Thetibiaisthecommonestsiteforstressfracturestooccur
inathletes.Thelocationofthefracturesvariesaccordingto
thetypeofsportpracticed.Inrunners,fracturesarefoundat
thetransitionfromthemiddletodistalthird.5
Thedifferentialdiagnosisshouldincludebothmiddletibial
stress syndrome (MTSS) and chronic compartmental
syn-drome(CCS).6
Magneticresonanceimagingmayalsodiagnosestress
frac-turesatanearlystage.Thesignsareboneedema,whichmay
Figure3–Radiologicalexaminationsshowinganareaof hypersignalonT2weightedimage,inthedistalregionof therighttibia,withsolutionofcontinuityintheposterior corticalbone,whichmaycorrespondtoastressfracture.
befoundintheregionanteriortothetibialcorticalbone,inthe
bonemarrow,orevenafractureline,asinthecasedescribed.7
Intheinitialphaseofthetreatment,itisrecommended
thatspecificphysiotherapeuticmeasuresshouldbeusedto
reducethepainfulcondition,suchascryotherapy,TENS,
ultra-sound toaccelerate bone tissue productionand laser as a
healing method. In addition, anti-inflammatory drugs are
used to reduce prostaglandin synthesis, which is
respon-sible for activating the free nerve ends that take sensory
informationtothebrainandincreasetheperceptionofpain.8
rev bras ortop.2013;48(6):574–577
577
Figure4–AreaofhypersignalonT2weightedimage,inthe proximalregionoftherighttibia,withsolutionof
continuityintheposteriorcorticalbone,whichmay correspondtoastressfracture.
includedassoonasthepainfulconditionhasbeenreduced.
Thus,lower-limbexercisesareinitiallydoneinaclosedkinetic
chainandtheninanopenkineticchain.9
Stressfractures thatare consideredtopresent highrisk
shouldbetreatedsurgically,giventhatthechancesofsuccess
withconservativetreatmentarelow.10
Intheliteratureinvestigated,wefoundcasesofbilateral
stressfracturesinthelowerlimbs.11However,wedidnotfind
casesofsegmentalfractures ofthetibia, which provesthe
rarity ofthe casereportedhere.Likethe majorityofstress
fractures,thefracturesdiagnosedinthiscasewereconsidered
tobelow-riskcasesandweretreatedassuch.Thiscasewas
conductedinaccordancewithaprotocoldescribedinthe
liter-ature,withtwophasesoftreatment.10Phase1ischaracterized
bypaincontrolthrough medicalprescriptionofanalgesics;
reductionorcessationofsportsmovementsthatcause
symp-toms;andintroductionofphysiotherapeuticmethods.Phase
2ischaracterizedbythemeasuresofPhase1plusagradual
returntosport;inthisphase,correctionofpredisposing
fac-torsisimportant(typeoffloor,typeofsteps,biomechanics
ofrunningandregularrenewaloffootwear).Phase2begins
whentheathleteisfreefrompainandpresentsnormal
nobil-ity,around10–14daysafterthestartofsymptoms.Thetime
takentoreturntosportsmovementsdependsonmany
fac-tors,includingtheseverityandchronicityoftheinjuryand
theathlete’sfunctionalmorbiditylevel.10
Conflicts
of
Interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WardenSJ,HurstJA,SandersMS,TurnerCH,BurrDB,LiJ.
Boneadaptationtoamechanicalloadingprogram
significantlyincreasesskeletalfatigueresistance.JBone
MinerRes.2005;20(5):809–16.
2.NattivA,PufferJC,CasperJ.Stressfractureriskfactors,
incidence,anddistribution:a3yearprospectivestudyin
collegiaterunners.MedSciSportsExerc.2000;32Suppl5:S347.
3.LavienjaAJ,BraamLM,MarjoHJ,KnapenGeusensP,BrounsF,
VermeerC.Factorsaffectingbonelossinfemaleendurance
athletes.Atwo-yearfollow-upstudy.AmJSportsMed.
2003;31(6):889–95.
4.WarrenMP,PerlrothNE.Theeffectsofintenseexerciseonthe
femalereproductivesystem.JEndocrinol.2001;170(1):3–11.
5.JensenA,DahlS.Stressfractureofthedistaltibiaandfibula
throughheavylifting.AmJIndMed.2005;47(2):181–3.
6.YatesB,WhiteS.Theincidenceandriskfactorsinthe
developmentofmedialtibialstresssyndromeamongnaval
recruits.AmJSportsMed.2004;32(3):772–80.
7.ProvencherMT,BaldwinAJ,GormanJD,GouldMT,ShinAY.
Atypicaltensile-sidedfemoralneckstressfractures:thevalue
ofmagneticresonanceimaging.AmJSportsMed.
2004;32(6):1528–34.
8.MollonB,daSilvaV,BusseJW,EinhornTA,BhandariM.
Electricalstimulationforlongbonefracture-healing:a
meta-analysisofrandomizedcontrolledtrials.JBoneJoint
SurgAm.2008;90(11):2322–30.
9.BodenBP,OsbahrDC,JimenezC.Low-riskstressfractures.
AmJSportsMed.2001;29(1):100–11.
10.BodenBP,OsbahrDC.High-riskstressfractures:evaluation
andtreatment.AmAcadOrthopSurg.2000;8(6):344–53.
11.SciberrasN,TaylorC,TrimbleK.Bilateraldistaltibialstress
fracturesinamilitaryrecruit.BMJCaseReports.2012,