w w w . r b o . o r g . b r
Original
Article
Epidemiological
study
on
talus
fractures
夽
,
夽夽
Marcos
Hideyo
Sakaki
∗,
Guilherme
Honda
Saito,
Rafael
Garcia
de
Oliveira,
Rafael
Trevisan
Ortiz,
Jorge
dos
Santos
Silva,
Túlio
Diniz
Fernandes,
Alexandre
Leme
Godoy
dos
Santos
InstitutodeOrtopediaeTraumatologia,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(IOT-HCFMUSP),São Paulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13June2013 Accepted31July2013 Availableonline5August2014
Keywords: Talus Epidemiology Bonefractures
a
b
s
t
r
a
c
t
Objective:toanalyzethecharacteristicsofpatientswithtalusfracturesandtheinjuriesthat theypresent.
Methods:retrospectiveanalysisonpatientshospitalizedintheInstituteofOrthopedicsand Traumatology,HospitaldasClínicas,SchoolofMedicine oftheUniversityofSãoPaulo, between2006and2011,withtalusfractures.Patientprofileparameters,riskfactors,fracture characteristics,treatmentdataandacutecomplicationswereanalyzed.
Results:analysison23casesshowedthatmenweremoreaffectedthanwomen,witharatio of4.8:1.Themostfrequenttraumamechanismwastrafficaccidents,followedbyfallsfrom aheight.Themostfrequenttypeoffracturewasattheneckofthetalus,with17cases. Amongthe23cases,sevenhadperitalardislocationatthetimeofpresentation,fourhad exposedfracturesand11presentedotherassociatedfractures.Themeanlengthoftime betweenthetraumaandthedefinitivetreatmentwassixdays,whilethemeanlengthof hospitalstaywas11days.Threepatientspresentedacutepostoperativecomplications. Conclusion:talusfracturesoccurredmostcommonlyintheregionofthetalarneckandmost frequentlyinyoungmaleswhosufferedhigh-energytrauma.Inalmosthalfofthecases, therewereotherassociatedfractures.Thelengthofhospitalstaywas11days.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:SakakiMH,SaitoGH,deOliveiraRG,OrtizRT,SilvaJS,FernandesTD,etal.Estudoepidemiológicodasfraturas dotálus.RevBrasOrtop.2014;49:334–339.
夽夽
WorkdevelopedattheInstituteofOrthopedicsandTraumatology,HospitaldasClínicas,UniversityofSãoPauloMedicalSchool (IOT-HCFMUSP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.H.Sakaki). http://dx.doi.org/10.1016/j.rboe.2013.07.002
Estudo
epidemiológico
das
fraturas
do
tálus
Palavras-chave: Tálus Epidemiologia Fraturasósseas
r
e
s
u
m
o
Objetivo: Analisarascaracterísticasdosindivíduosedaslesõesencontradasempacientes comfraturasdetálus.
Métodos: AnáliseretrospectivadospacientesinternadosnoInstitutodeOrtopediae Trau-matologiadoHospitaldasClínicasdaFaculdadedeMedicinadaUniversidadedeSãoPaulo de2006a2011comfraturadetálus.Foramestudadosparâmetrosassociadosaoperfildo pacienteefatoresderisco,característicasdafratura,dadosdotratamentoecomplicac¸ões agudas.
Resultados: Aanálisedos23casosmostrouqueoshomensforammaisafetadosdoque asmulheres,comumarelac¸ãode4.8:1.Omecanismodetraumamaisfrequenteforam osacidentesdetrânsito,seguidopelasquedasdealtura.Otipodefraturamaisfrequente foiadocolodotálus,com17casos.Dos23casos,seteapresentavamluxac¸ãoperitalar nomomentodaapresentac¸ão,quatrotinhamfraturaexpostae11apresentavamoutras fraturasassociadas.Otempomédioentreotraumaeotratamentodefinitivofoideseisdias, enquantootempomédiodepermanênciahospitalarfoide11dias.Houvetrêspacientes queapresentaramcomplicac¸õespós-operatóriasagudas.
Conclusão: Afraturadotálusfoimaiscomumnaregiãodocoloemaisfrequenteemjovens dogêneromasculinoquesofreramtraumatismosdealtaenergia.Emquasemetadedos casoshouvefraturasassociadaseotempodepermanênciahospitalarfoide11dias.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Talus fractures are known to be difficult and challenging pathologicalconditions.Thereare severalfactors contribut-ingtowardsthis reputation:theincidenceofcomplications withseverefunctionallimitation,theunusualanatomyofthe talus,the greatvariabilityoffracturepatterns andthe role ofthetalusinthefunctionalityofthelowerlimb.1However,
overrecentdecades,surgicaltechniques,synthesismaterials andevenknowledgerelatingtothebiologyofbonerepairand vascularsupply ofthetalushaveevolvedgreatly and have changedthepanoramaofthistypeoffracture.
Thediagnosisismadeinitiallybymeansofradiographic evaluation, which includes a series of view of the ankle (anteroposterior, lateral and mortise) and a series of view ofthe foot (anteroposterior, lateral and oblique). Theview describedbyCanaleandKelly2,3makesitpossibletoobserve
themedialaspectofthetalarneckwell.Furthermore,thetrue lateralviewofthesubtalarjointandtheobliqueviewofthe taluscanprovideadditionalinformationaboutthefracture.4
Computedtomography playsanimportantrole in diagnos-ingtalarfractures:ithasthecapacitytodetectfracturesthat aredifficulttoviewonordinaryradiographsandprovidesa goodviewofthetalarjointcongruence,aswellascontributing towardssurgicalplanning.5Magneticresonanceimaginghas
animportantroleinviewingosteonecrosisofthetalus,which isoneofthecommonestandmostfearedcomplicationsof thistypeoffracture.6,7
Theclassificationoftalarfracturestakesintoaccountthe location(body,neck,headandprocesses),8theassociated
dis-locations(subtalar,ankle andtalonavicular)andthe degree
ofcomminution.Thetwoclassificationsmostusedare the Hawkinsclassification,9whichisusedtocategorizetalarneck
fractures,andtheAOclassification.10
The treatment should generally be aimed towards rapidlyreestablishingjointcongruenceandtowards achiev-ing anatomical reduction of the fracture, in view of the high rates ofosteonecrosis and associated fractures. Non-deviatedfracturesandthosewithoutjointincongruencecan betreatednon-surgically,whereasdeviatedfracturesusually require open reduction.Nevertheless, closed reductioncan be attempted and may be particularly useful as an initial step.11–14
Despitetheevolutionachievedoverrecentyears,the com-plicationratesremainextremelyhigh.Theosteonecrosisrate intalarneckfracturesrangesfrom21to58%,3,9whileinthe
talarbody,88%ofthepatientspresentevidenceof osteonecro-sisand/orpost-traumaticarthritis.15–19
ThereareveryfewstudiesintheBrazilianliteratureonthe epidemiologyoftalarfractures.Debieuxetal.20studied387
patientswhohadsufferedmotorcycleaccidentsinthe munic-ipalityofSãoPaulobetweenJanuary2001andJuly2002and observedthatthecommonestinjuries,inorderoffrequency, werewounds(31.8%),bruises(15.8%)andfractures(8.7%).The mostfrequentlocationforthefractureswasthefoot,in16.0% ofthepatientswithfractures,butthatstudydidnotspecify whichbonewasmostaffected.
Fonseca Filho et al.21 studied 52 cases oftalar fracture
11 to 20
Number of cases
14
12
10
8
6
4
2
0
21 to 30 31 to 40
Age
41 to 50 51 to 60
Fig.1–Agegroup.
intheneckandbodyregions.Moreover,theyfoundthat frac-turesoftheipsilateralmedialmalleoluswerethecommonest associatedinjury,presentin21.2%ofthecases.
Becauseofthescarcityofinformationregardingthe epi-demiology of talar fractures in our setting,we decided to conductthepresentstudy.
Objective
Toevaluatethecharacteristicsofpatientsandtheirinjuries, amongthose admittedtohospitalforsurgicaltreatmentof talar fractures between 2006 and 2011, at the Institute of OrthopedicsandTraumatology,HospitaldasClínicas, Univer-sityofSãoPauloMedicalSchool.
Materials
and
methods
Themedicalfilesofallthepatientsadmittedtothehospital withfracturesofthefootandanklebetween2006and2011 were surveyed.Through making adetailed reviewofthese medicalfiles,23casesoftalarfracturesthatweretreated sur-gicallywereidentified.
The parameters analyzed were: age; gender; laterality; exposure; smoking; trauma mechanism; type of fracture; classification;associatedinjuries;treatmentadministeredat theemergency service;definitivetreatment; lengthoftime betweenthe traumaandthe definitivetreatment;lengthof hospitalstay;andacutepostoperativecomplications.
Results
Amongthe23patientsevaluated,therationofmentowomen was4.8:1(19menandfourwomen).Theirmeanagewas30.4 years,rangingfrom18to49years(Fig.1).Therightsidewas affectedin13patientsandtheleftsidein10.Amongthese23 patients,threeweresmokers(incidenceof13%).
Themostfrequenttraumamechanismwasfallingfroma height,witheightcases,followedbymotorcycleandcar acci-dents,withfiveeach.Theothermechanismsweretorsional trauma,withthreecases,andsportstrauma,withtwo(Fig.2). Inrelationtothetypeoffracture,talarneckfractureswere themostprevalenttype,with17cases.Therewerealsothree casesoffracturesofthebody,twoofthetalarprocessesand
Motorcycle accident
Car accident Torsional trauma
Sports trauma
Number of cases
8
4
2 6
0
Falling from height
Fig.2–Traumamechanism.
20
15
10
5
0
Talar neck Talar body
Number of cases
Talar processes Talar head
Fig.3–Fracturelocation.
oneofthehead(Fig.3).Outofthe17fracturesofthetalarbody, 16wereclassifiedasHawkins2andoneasHawkins3.
Fourpatientssufferedanexposedfracture(17.4%),ofwhich twowereclassifiedasGustilotypeII,oneastypeIIIAandone astypeIIIB.
Outofthe23casesanalyzed,seven(30.4%)hadperitalar dislocationatthetimeofpresentation.
Inrelationtotreatmentattheemergencyservice,16cases wereimmobilizedbymeansofaplastercastsplintcovering thefootandlowerleg.Amongthesevencaseswith associ-ateddislocation,itwaspossibletoreducethedislocationby meansofclosedmaneuversinfivecases,whiletheothertwo casesunderwentsurgicalreductionfollowedbyplacementof anexternalfixator.
Thedefinitivetreatmentconsistedofosteosynthesisin20 casesandresectionoftheintra-articularbonefragmentsin theotherthreepatients.
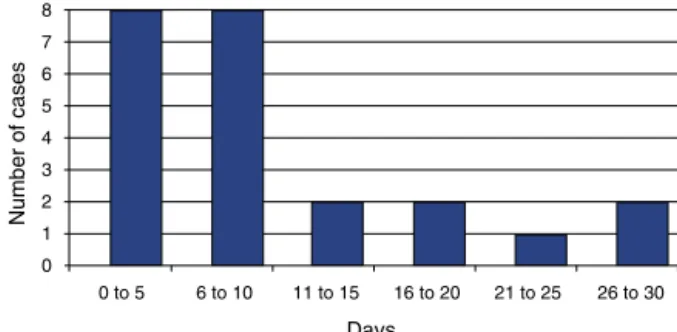
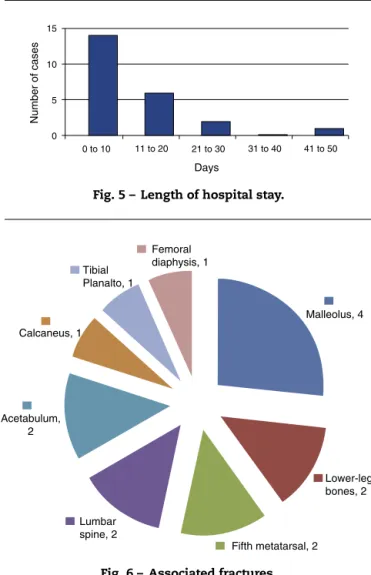
The mean lengthof time between the trauma and the definitivetreatmentwassixdays,rangingfrom0to29(Fig.4). Themeanlengthofhospitalstaywas11days,rangingfrom2 to44(Fig.5).
Associatedinjurieswerepresentin11patients(47.8%):four withmalleolarfractures,twowithfracturesoflegbones,two withfractures ofthe baseofthe fifthmetatarsal,twowith fracturesofthelumbarspine,twowithacetabularfractures,
0 to 5 8 7
6 5
4 3
2 1 0
6 to 10 11 to 15 16 to 20 21 to 25 26 to 30
Days
Number of cases
0 to 10 15
10
5
0
11 to 20 21 to 30 31 to 40 41 to 50
Days
Number of cases
Fig.5–Lengthofhospitalstay.
Calcaneus, 1
Fifth metatarsal, 2 Lumbar
spine, 2
Lower-leg bones, 2 Malleolus, 4 Femoral
diaphysis, 1
Acetabulum, 2
Tibial Planalto, 1
Fig.6–Associatedfractures.
onewithacalcanealfracture,onewithatibialplateaufracture andonewithafemoraldiaphysisfracture(Fig.6).
Inrelationtoacutecomplications,therewerethreecasesof postoperativeinfection:oneassociatedwithcompartmental syndromeofthefootconsequenttoaclosedfractureofthe talarneck;oneresultingfromaGustiloIIIBexposedfracture thatevolvedwithlossofthemicrosurgicalflapthathadbeen constructedtocoverit;andoneduetoaGustiloIIfracture associatedwithalumbarspinefracture.
Discussion
Overthisfive-yearperiod,23patientswithtalarfractureswere operatedatourservice,i.e.,anincidenceof4.6casesperyear, whileFonsecaFilho etal.21 treated 52casesover 23 years,
whichwasameanof2.3peryear.Sincebothofthesestudies wereconductedinlarge-sizedhospitalsthatprovide tertiary-levelorthopedictraumatologycare,itisevidentthatthistype offracturehaslowfrequencyofoccurrencewithinthetotal numberoffracturesthatare treatedsurgically.Thismeans thatfororthopedistswhoprovidefracturetreatmentcarein thevariouscentersinBrazil,alongtimeisneededforthemto acquireexperienceintherapeuticmanagementfortalus frac-tures.Medicalcentersofsmallersizewillprobablyhavegreat difficultyintrainingtraumatologistswiththeskillstooperate
onthistypeoffracture.ThestudybyFonsecaFilhoetal.21
cov-eredatimeperiod(from1972to1995)duringwhichthecity ofSãoPaulohadnotyetfelttheeffectsofthegrowing num-bersofmotorcycleaccidentsthathavebeenseenoverthelast decade.Thepresentstudythusservestoupdatethe epidemi-ologyoftalusfractures,withdatarelatingtoamorerecent period(from2006to2011).
Thegreaterprevalenceofmalepatients(4.8:1)andyoung patients(meanof30.4years)showstheimportanceofcorrect treatmentforthistypeoffracture,whichpresentshighrates oflatecomplications,withsequelaethatareoften incapacitat-ingandmayrequirearthrodesisoftheankleandhindfootto controltheseconditions.Comparingourfindingswiththose ofFonsecaFilhoetal.21themeanageintheirstudy(31years
and4months)wasverysimilar,buttherewasgreater predom-inanceofmalegenderinourstudy(4.8menforeachwoman versus2.9menforeachwomanintheearlierstudy).This find-ingmayhavebeenrelatedtothegreaterexposureoftheyoung malepopulationtotrafficaccidents.
In18 cases(78.3%), high-energytraumawas responsible forthefracture.Tenfracturecases(43.8%ofthetotal)resulted fromtraffic-relatedaccidents,whichwassimilartothe find-ingsofFonsecaFilhoetal.21(42.3%).Likewise,fallingfroma
heightwasthesecondmostfrequentmechanism,andthis, togetherwiththetrafficaccidents,accountedfor78.3%ofour casesand71.2%ofthoseofFonsecaFilhoetal.21Thesedata
servetoguidethechoiceofpreventivemeasuresagainsttalus fractures,suchasstiffbootsthatlimitdorsalflexion move-mentsofthefoot,whichisthemechanismrelatingtothese fractures.Suchboots, formotorcyclistsandpeopleworking atheights, wouldneed tobesturdy and havehigh impact absorptioncapacity.
Althoughsmokinghasbeencorrelatedwithcomplications intheevolutionoffracturesandsurgicalproceduresonfeet, the three patients who were smokersdid notpresent any postoperativecomplicationsuptothetimeofdischargefrom hospital.Webelievethatifalargernumberofpatientswere tobestudied,thenegativeinfluenceofsmokingonsurgical treatmentoftalusfracturesmightbecomeevident.22
Central fractures (of the neck and body) were much more frequent than other types and accounted for 87.0% of the 23 cases studied, which is similar to what was described byFonseca Filhoet al.21 (78.8%).Thisprevalence
may haveresultedfrom the factthat alargeproportionof peripheralfracturesofthetalus(includingthoseofthe pos-terior and lateral processes)often go unnoticed and,even when correctly diagnosed, frequently can be treated non-operatively.1,11
The high incidenceofHawkins type2 fractures (16out of 17 cases) and the absence oftype 1fractures contrasts withwhatwasfoundbyFonsecaFilhoetal.21whohadnine
casesofHawkins2fracturesandfiveofHawkins1fractures amongtheirtotalof21casesoftalarneckfractures.This dif-ferencewasprobablyduetoouruseofmultislicecomputed tomographyforfractureinvestigation,forallofourpatients. Thistechnologywasintroducedattheendofthe1990sand enablesdetailedevaluationoffracturesandsmall displace-ments,butit wasnotavailableatthe timeofthe studyby Fonseca Filho et al.21 Moreover, intheir study, although it
wheneverpossible”,thetotalnumberofpatientswho under-wentthisexaminationwasnotstated.
Theincidenceofexposedfractureswas17.4%,andthisrate waspracticallyidenticaltowhatwasfoundbyFonsecaFilho etal.21whichwas17.3%.Itshouldbehighlightedthat,inour
survey,twoofthefourcasesofexposedfractureevolvedwith acuteinfection:onewithGustiloIIandtheotherwithIIIB.
Among the seven cases of fractures associated with dislocation,two(28.6%)requiredsurgicalreductionofthe dis-locationattheemergencyservice,oneofthesewasthecaseof Hawkinstype3,andthisalsopresentedGustiloIIIBexposure. Exceptforthesetwocasesoperatedattheemergencyservice, alloftheotherswereimmobilizedattheemergencyservice usingplastercastsplintsandnoneofthemevolvedwith for-mationofphlyctenaebeforethedefinitivesurgicaltreatment. Althoughhigh-energytraumacausedthe majorityofthese fractures,nonuse ofexternalfixationasameansof immo-bilizationbeforetheoperationdidnotgiverisetosoft-tissue complications,incomparisonwithwhatoccursincasesofthe fracturesofthetibialpilon.Ifacentralfractureofthetalusis intracapsular,thismaycontributetowardsnon-infiltrationof bleedinginto thesurroundingtissuesandmaythusleadto lesselevationoftheadjacentpressurelevels.
Themeanwaitingtimeforthedefinitivesurgicaltreatment wassixdaysandmeanlengthofhospitalstaywas11days. Thefactthat47.8%ofthepatientspresentedassociated frac-turescontributedtowardsmakingtheseperiodslongandhad adirectinfluenceonthecostoftreatment.Althoughblood irrigationofthetalusiscriticalincasesoftalarneckfractures withdisplacement,thewaitforthedefinitivesurgical treat-mentseemednottoincreasetheriskofavascularnecrosis ofthetalarbody.Thiscomplicationismuchmoreconnected withthelengthoftimebetweentheaccidentandthe reduc-tionofthedislocation,whenthelatterispresent.19,23Inany
event,measuresthatmightreducethelengthofthe preoper-ativeperiodshouldbesoughtinthistypeofpatient.
Fifteen associated fractures (Fig. 6) were found in 11 patients (47.8%),which showed the high-energy trauma to whichthese patientswere subjected.This ratewas practi-callyidenticaltowhatwasfoundinthestudybyFonsecaFilho etal.21(46.2%).
Fromcombinedanalysisonalltheseresults,wecansay that althoughtalus fractures epidemiologically represent a smallproportionofthetotalnumberoffracturestreatedin orthopedichospitals,theirimportanceliesinthefactthatthey affectyoungindividualsatthepeakoftheirworkactivities, oftenwithassociatedinjuries,thusnecessitatinglong hospi-talstays.Thepatternoftalusfracturesissevere,withahigh riskofcomplicationssuchasavascularnecrosis.Preventive measuresshouldbecreatedbasedonthecommonest mech-anismsthathavebeenidentified:trafficaccidentsandfalling fromaheight.
Conclusions
Patientswithtalusfractureswhowereattendedandoperated inatertiary-levelhospitalinthecityofSãoPaulowereyoung, withameanageof30.4years.Mostofthemweremale(4.8:1) andtheyhadsufferedtrafficaccidentsorfallsfromaheight.
Thetalarneckwastheregionmostaffectedand,atthetime whenthecaseswerefirstattended,peritalardislocationwas presentin30.4%andthetalusfractureswereexposedin17.4%. Almosthalfofthesepatientspresentedassociatedfractures andthemeanlengthofhospitalstaywas11days.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MurphyGA.Talarfractures.In:Campbell’s.,editor.Operative orthopaedics.Philadelphia:MosbyElsevier;2007.p.4851–66. 2.CanaleST.Fracturesoftheneckofthetalus.Orthopedics.
1990;13(10):1105–15.
3.CanaleST,KellyJrFB.Fracturesoftheneckofthetalus long-termevaluationofseventy-onecases.JBoneJointSurg Am.1978;60(2):143–56.
4.EbraheimNA,PatilV,FrischNC,LiuX.Diagnosisofmedial tuberclefracturesofthetalarposteriorprocessusingoblique views.Injury.2007;38(11):1313–7.
5.ChanG,SandersDW,YuanX,JenkinsonRJ,WillitsK.Clinical accuracyofimagingtechniquesfortalarneckmalunion.J OrthopTrauma.2008;22(6):415–8.
6.KerrR,ForresterDM,KingstonS.Magneticresonanceimaging offootandankletrauma.OrthopClinNAm.
1990;21(3):591–601.
7.MunkPL,VelletAD,LevinMF,HelmsCA.Currentstatusof magneticresonanceimagingoftheankleandthehindfoot. CanAssocRadiolJ.1992;43(1):19–30.
8.InokuchiS,OgawaK,UsamiN.Classificationoffracturesof thetalus:cleardifferentiationbetweenneckandbody fractures.FootAnkleInt.1996;17(12):748–50.
9.HawkinsLG.Fracturesoftheneckofthetalus.JBoneJoint SurgAm.1970;52(5):991–1002.
10.FractureanddislocationcompendiumOrthopaedicTrauma AssociationCommitteeforCodingandClassification.J OrthopTrauma.1996;10Suppl.1:1–154.
11.SandersDW.Talusfractures.In:RockwoodCA,GreenDP, editors.Fracturesinadults.Piladelphia:LippincottWilliams &Wilkins;2010.p.2022–63.
12.AdelaarRS.Thetreatmentofcomplexfracturesofthetalus. OrthopClinNAm.1989;20(4):691–707.
13.SangeorzanBJ,WagnerUA,HarringtonRM,TencerAF. Contactcharacteristicsofthesubtalarjoint:theeffectoftalar neckmisalignment.JOrthopRes.1992;10(4):
544–51.
14.DanielsTR,SmithJW,RossTI.Varusmalalignmentofthe talarneckitseffectonthepositionofthefootandonsubtalar motion.JBoneJointSurgAm.1996;78(10):1559–67.
15.VallierHA,NorkSE,BenirschkeSK,SangeorzanBJ.Surgical treatmentoftalarbodyfractures.JBoneJointSurgAm. 2003;85(9):1716–24.
16.LindvallE,HaidukewychG,DiPasqualeT,HerscoviciJrD, SandersR.Opennreductionandstablefixationofisolated, displacedtalarneckandbodyfractures.JBoneJointSurgAm. 2004;86(10):2229–34.
18.VallierHA,NorkSE,BareiDP,BenirschkeSK,SangeorzanBJ. Talarneckfractures:resultsandoutcomes.JBoneJointSurg Am.2004;86(8):1616–24.
19.ElgafyH,EbraheimNA,TileM,StephenD,KaseJ.Fracturesof thetalus:experienceoftwolevel1traumacenters.Foot AnkleInt.2000;21(12):1023–9.
20.DebieuxP,ChertmanC,MansurNSB,DobashiE,Fernandes JA.Musculoskeletalinjuriesinmotorcycleaccidents.Acta OrtopBras.2010;18(6):353–6.
21.FonsecaFilhoFF,SantinRAL,FerreiraRC,SanmartinM, GuerraA.Epidemiologicalaspectsoffracturesofthetalus. RevBrasOrtop.1996;31(6):481–4.
22.KwiatkowskiTC,HanleyJrEN,RampWK.Cigarettesmoking anditsorthopedicconsequences.AmJOrthop(BelleMead NJ).1996;25(9):590–7.