w w w . r b o . o r g . b r
Original
Article
Terrible
triad
of
the
elbow:
influence
of
radial
head
treatment
夽
,
夽夽
Lucas
Braga
Jaques
Gonc¸alves
a,
Jorge
de
Almeida
e
Silva
Neto
a,
Mario
Roberto
Chaves
Correa
Filho
a,
Ronaldo
Percope
de
Andrade
a,
Marco
Antônio
Percope
de
Andrade
b,
Anderson
Humberto
Gomes
c,
José
Carlos
Souza
Vilela
c,∗aServic¸odeOmbroeCotovelo,HospitalMadreTeresa,BeloHorizonte,MG,Brazil
bServic¸odeOrtopedia,HospitaldasClínicas,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
cServic¸odeOrtopediaeMedicinadoEsporte,HospitalUnimed,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16May2013 Accepted30August2013 Availableonline11July2014
Keywords:
Dislocations Elbowjoint Radialfractures
a
b
s
t
r
a
c
t
Objective:totestthenullhypothesisthatpatientswiththeterribletriadoftheelbow
(dislo-cationtogetherwithfracturesoftheradialheadandcoronoidprocess)whoaretreatedwith openreductionandinternalfixationoftheradialheadhavefinalresultsthatarecomparable withthoseofpatientstreatedwitharthroplastyorpartialresectionoftheradialhead.
Methods:twenty-sixpatientswiththeterribletriadoftheelbowwhowereoperatedbya
singlesurgeonwereevaluatedonaverage23monthsafterthesurgery(range:16–36months). Therewere17menandninewomenofmeanage41±13.4years.Thefracturesoftheradial headweretreatedbymeansofosteosynthesis(12patients),arthroplasty(nine)orresection ofasmallfragmentornotreatment(five).Fixationofthecoronoidprocess/anteriorcapsule wasperformedin21patients.Thelateralligamentcomplex(LLC)wasrepairedinallthe patients,whilethemedialligamentcomplex(MLC)wasrepairedinthreepatientswhose elbowsremainedunstableaftertreatmentfortheradialheadandLLC,butwithoutfixation ofthecoronoidprocess.
Results:themeanfinalrangeofflexionandextensionwas112◦.Themeanpronationwas
70◦andsupination,6◦.ThemeanDASHscore(DisabilitiesoftheArm,Shoulder&Hand) was12andmeanMEPI(MayoElbowPerformanceIndex)was87.AccordingtotheMEPI scores,21patients(80%)hadgoodandexcellentresults.Therewasnostatisticallysignificant differenceintheresultsbetweenthepatientswhounderwentfixationoftheradialhead andthosewhounderwentarthroplastyorresectionofasmallfragment.
Conclusion:therewasnodifferencebetweenthepatientstreatedwitharthroplastyofthe
radialheadandthosetreatedwithothertechniques.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:Gonc¸alvesLBJ,NetoJAS,CorreaFilhoMRC,deAndradeRP,deAndradeMAP,GomesAH,etal.Tríadeterrível docotovelo:ainfluênciadotratamentodacabec¸adorádio.RevBrasOrtop.2014;49:328–333.
夽夽
WorkperformedatHospitalMadreTeresaandHospitalUnimed,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.C.S.Vilela). http://dx.doi.org/10.1016/j.rboe.2014.07.001
Tríade
terrível
do
cotovelo:
a
influência
do
tratamento
da
cabec¸a
do
rádio
Palavras-chave:
Luxac¸ões
Articulac¸ãodocotovelo Fraturasdorádio
r
e
s
u
m
o
Objetivo:testarahipótesenuladequeospacientescomatríadeterríveldocotovelo(luxac¸ão
associadaa fraturasdacabec¸adorádioedoprocessocoronoide)tratadoscomreduc¸ão abertaefixac¸ãointernadacabec¸adorádiotêmresultadofinalcomparávelaospacientes tratadoscomartroplastiaouressecc¸ãoparcialdacabec¸adorádio.
Métodos: foramavaliados,emmédiaaos23meses(16a36)apósacirurgia,26pacientes
coma tríadeterríveldocotovelooperados por umúnicocirurgião.Eram17 homense novemulheres,commédiadeidadede41anos(±13,4).Asfraturasdacabec¸adorádio foramtratadascomosteossíntese(12pacientes),ouartroplastia(nove),ouressecc¸ãodeum fragmentopequenoounenhumtratamento(cinco).Fixac¸ãodoprocessocoronoide/cápsula anteriorfoifeitaem21pacientes.Ocomplexoligamentarlateral(LCL)foireparadoem todosospacientes,enquantoqueocomplexoligamentarmedial(LCM)foireparadoemtrês pacientescujoscotovelospersistiaminstáveisapósotratamentodacabec¸adorádioedo LCL,massemfixac¸ãodoprocessocoronoide.
Resultados: oarcofinalmédiodeflexãoeextensãofoide112◦.Apronac¸ãomédiafoide
70◦easupinac¸ão,de6◦.OescoreDash(DisabilitiesofArm,Shoulder&Hand)médiofoi de12eoMepi(MayoElbowPerformanceIndex)médiofoide87.DeacordocomoMepi,21 pacientes(80%)tiverambonseexcelentesresultados.Nãohouvediferenc¸aestatisticamente significativaentreosresultadosdospacientessubmetidosafixac¸ãodacabec¸adorádioe aquelessubmetidosaartroplastiaouressecc¸ãodeumfragmentopequeno.
Conclusão: nãohádiferenc¸aentreospacientestratadoscomaartroplastiadacabec¸ado
rádiodaquelestratadoscomoutrastécnicas.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Injuriesthatinvolvedislocationoftheelbowinassociation withfracturingoftheradialheadandfracturingofthe coro-noidprocessarereferredtoastheterribletriadoftheelbow.1 Historically,theseinjurieshavebeendifficulttodealwithand theresultsfrom treatmenthavebeenunsatisfactorydueto instability,arthrosisand/orstiffnessoftheelbow.2,3The diffi-cultyintreatingthisinjurypatternhasbeenascribedtolackof knowledgeregardingtheanatomicalfactorsinvolvedinelbow stabilization andthe appropriatesurgicaltechniques. Pugh andMcKee4,5describedasystematizedapproachforsurgical treatmentoftheterribletriadofthe elbow,whichincluded osteosynthesisor arthroplasty ofthe radialhead, repairof thecoronoidwhenpossibleand/orrepairofthejointcapsule, andrepairofthelateralligamentcomplex(LLC)oftheelbow. Theyreportedthat80%oftheirpatientspresentedgoodor excellentresultsandalsothattherevisionratewas15–25%. Sincethen,severalauthorshavepresentedgoodand excel-lentresults(77–100%)fromsurgicaltreatmentoftheterrible triadoftheelbow,inaccordancewiththeprotocolpresented byPughetal.6–14
Thisstudyhadtheobjectiveofevaluatingtheclinicaland radiographicresultsfrom patientswiththeterribletriadof theelbowwho were operatedinaccordancewiththis pro-tocol.Ourhypothesiswasthatthepatientswhounderwent arthroplastyoftheradialheadwouldhaveresultsthatwere comparabletothoseoftheotherpatients.
Methods
Between March 2007and December 2009,32 patients with theterribletriadoftheelbowwerediagnosedandunderwent surgicaltreatmentperformedbythesamesurgeon(LBJG)at HospitalMadreTeresa(HMT)and“RisoletaTolentinoNeves” UniversityHospital(HURTN).Sixpatientswereexcluded:four whocouldnotbefoundandtwowhodidnotadheretothe postoperativefollow-up.Thus,26patientsremainedfor eval-uation(17menandninewomen),withameanageof41years (±13.4). Three were left-handedand 23 were right-handed. Theinjurymechanismswerefallsfromaheightin13cases, motorcycleaccidentsin10casesandbeingrunover,falling offabicycleandbeinginacaraccidentinonecaseeach.The elbowswereoperated,onaverage,ninedays(±5.93)afterthe initialtrauma.Theleftsidewasaffectedin17patients(65%) andrightsideinseven(35%).
The fractures ofthe radialhead were classified astype 4,inaccordance withMason’sclassificationasmodifiedby Johnston.15Insixfractures,onlyonefragmentwasidentified and,infourofthese,therewasananteriorfragment account-ingforlessthan20%ofthejointsurface,whichwasextremely comminuted,withoutthepossibilityoffixation.Fivefractures hadtwofragments,sevenfractureshadthreeandeight frac-tureshadmorethanthree.
Fig.1–A56-year-oldwomanwhosufferedafallfromastandingposition.(A)Lateralandanteroposteriorradiographsprior toreduction,showingposteriordislocationoftheelbowandtype2fracturingoftheradialhead,withacomminuted anteriorfragment.(B)Lateralandanteroposteriorradiographsaftersurgicaltreatment,showingconcentricreductionofthe elbow,despiteresectionoftheanteriorfragmentoftheradialhead.
intothreemaintypes.Type1consistsoffracturesofthetop ofthecoronoidprocess:1Awithfragmentsupto2mmand1B withfragmentslargerthan2mm.Type2fracturesare antero-medialandtype3are atthe baseofthe coronoidprocess. Type1Afracturesofthecoronoidprocesswereidentifiedin 19 patients, and type 1B fractures in the remaining seven patients.
Inall thepatients, injuriestothe lateral ligament com-plexdietoavulsionatitsorigininthelateral condylewere identified. Reinsertion was performed bymeans of a tran-sosseoussutureora4.0metalanchor(HexagonInd.eCom. de AparelhosOrtopédicos Ltda., Campinas, SP)using Ethi-bondno.2thread(Johnson&JohnsondoBrasilLtda.,SãoJosé dosCampos,SP).Reinsertionofthemedialligamentcomplex wasperformedinonlythreepatients,bymeansof4.0metal anchorsandEthibondno.2thread.Thesepatientspresented residualinstabilityaftertreatmentofthefractureoftheradial headandthelateralligamentcomplex.Inthesethreecases, thecoronoidprocess/anteriorcapsulewasnotfixedbecause, duringthepreoperativeassessment,thesurgeonconsidered thesetobeseparateinjuriesthatdidnotcontributetoward theelbowinstability.
Sevenpatientspresentedotherfracturesintheipsilateral upperlimb:twofractures inthe distalradius,onefracture intheulnarstyloid,onefractureinthelateralcondyle,one Stennerinjuryinthethumb,onefractureofthemetacarpal andonerotatorcuffinjuryintheshoulder.Withthe excep-tionoftherotatorcuffinjury,alltheotherswerefixedduring thesameoperation,inordertoaccelerateelbowrehabilitation duringthepostoperativeperiod.
Inall the patients, auniversal posteriorincision inthe elbowwas made,withlateral subcutaneouspushback until theelbowwascompletelyexposedlaterally.TheKocher inter-val was exploredusing the spacing alreadydefined bythe lateralligamentinjury,inordertoobtainaccesstotheelbow joint.After the joint had been exposed, the coronoid pro-cesswasdealtwithfirst.In12patients,transosseoussuturing ofpull-outtypewasperformed,whichincludedtheanterior jointcapsule andthe fragmentofthe coronoidprocess.In onepatient, thesuturingwasperformedbymeans ofa4.0 metalanchorthatwasinsertedintotheproximalulna.Ineight patientswhoallhadtype1Bfracturesofthecoronoidprocess,
osteosynthesisofthefracturedbonefragmentofthecoronoid processwasperformedusingacannulatedscrewaloneintwo cases, cannulatedscrew and Kirschnerwiresin twocases, cannulatedscrewandtransosseoussuturingofthecapsule inonecase,Kirschnerwiresandtransosseoussuturingintwo casesandKirschnerwiresaloneinonecase.Infivepatients, norepairtothecoronoidprocesswasperformed,because dur-ingthepreoperativeassessment,thesurgeonconsideredthat thesewereseparateinjuriesthatdidnotcontributetoward theelbowinstability.
The radial head was dealt with next. For four patients whopresentedananteriorfragmentaccountingforlessthan 20%ofthejointsurface,whichwascomminutedanddidnot present any possibilityofreconstruction, it wasdecidedto performsimpleresectionofthefragments,sincetherewas noimpairmentofelbowstabilization(Fig.1).Insixfractures, osteosynthesisusingHerbertscrewswasperformed.Infour cases,KirschnerwireswereusedinadditiontoHerbertscrews. Intwopatients,screwsandplateswereused.Ineightpatients, uncementedarthroplastyoftheradialheadwasperformed usingamonoblockprosthesis(MetaBioIndustrialLtda.,Rio Claro,SP),withthreepossiblesizes,relatingtonecklengthsof 9,12and19mm.Inonepatient,arthroplastywasperformed usingamethylmethacrylatemoldedprosthesis,whichwas removed eight weeks later. In one patient who presented onlyslightdisplacement,thefracture wasnotsubjectedto osteosynthesis.
Lastly,thelateralligamentcomplexoftheelbowwas rein-sertedatitsisometricpoint,eitherbymeansofmetalanchors or by means oftransosseous suturing.The stabilityof the elbowwastestedthroughfullpassiveextensionoftheelbow inneutralorientation.Followingthis,assistedpassiveflexion of the elbowwas performed, with the aimof testing con-centric stability over the entirerange of motion(ROM). In threepatients,residualposteriorsubluxationwasobserved:in thesecases,themedialligamentcomplexwasrepairedusing a4.0anchorandEthibondno.2thread,andjointstabilitywas reestablishedovertheentireROM.Therewasnoneedforan articulatedexternalfixatorinanypatient.
Afterthesurgery,theelbowwasimmobilizedforoneweek at90◦offlexionandinpronation,usingaplaster-castsplint.
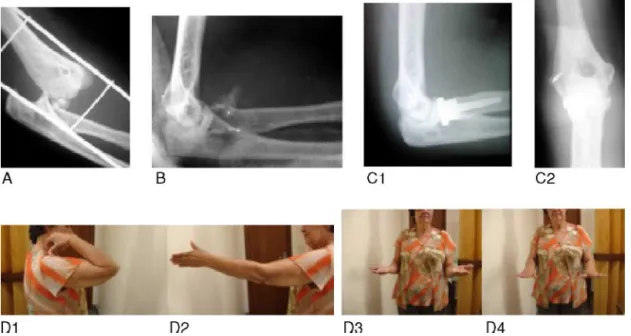
Fig.2–A54-year-oldwomanwhosufferedafallfromastandingposition.(A)Lateralradiographpriortoreduction, showingposteriordislocationoftheelbowandfracturingoftheradialhead.(B)Lateralradiographafterreduction,showing comminutivefracturingoftheradialheadandfracturingofthecoronoid.C1andC2:lateralandanteroposteriorradiographs showingconcentricreductionoftheelbow,theradialheadprosthesisandthelateralmetalanchor.D1,D2,D3andD4: clinicalresultsfromfinalfollow-up.
advised to start a home-based program for early gains in ROM,whichconsistedofactiveflexionandextensionofthe elbow(extensionwiththeelbowpronated),alongwith pas-sivepronation-supinationofthe elbowwhileflexedat90◦.
Thisprogramwascontinuedforsixweeksand,duringthis period,thepatientswereinstructednottoperformabduction oftheshouldergreaterthan60◦,orabductionwiththe
shoul-derflexedat90◦,inordertoavoidvarusstressontheligament
reconstruction, asrecommended byDuckworthet al.17 Six weekslater,thepatientswerereferredforphysiotherapyand rehabilitationoftheoperatedlimbwasstartedunder super-vision.
Postoperativecontrolswereconductedinthe1st,2ndand 6th weeksand inthe 3rd, 6th and 12th months.Pain was assessed using a visual analog scale,ROM by means of a goniometer and stability through clinical tests (pivot shift and drawer) and radiograph imaging, in terms of concen-tricreductionsobservedinanteroposterior (AP)and lateral views.Theconsolidationofthefracturesandpresenceof het-erotopicossificationanddegenerative alterationswere also assessed.
Thefinalevaluationonthepatientswasmadebyaproperly trainedshoulderandelbowsurgeryspecialistandconsisted of application of the DASH18 and MEPI19 questionnaires, measurementoftheROM,assessmentofjointstability, inves-tigationofcomplicationsandothersurgicalproceduresinthe sameelbow,andevaluationofAPandlateral-viewradiographs inordertoinvestigatecalcificationaroundtheligament inser-tions,heterotopicossificationanddegenerativealterationsof theelbow.Thesealterationswereclassifiedinaccordancewith thecriteriaofBrobergandMorrey19:grade0(absence;i.e. nor-malelbow);grade1(mild;jointnarrowingaloneandminimal formationofosteophytes);grade2(moderate;moderatejoint
narrowingandmoderateformationofosteophytes);grade3 (severe;severenarrowingandjointdestruction).
ThevariableswereanalyzedusingFisher’stestandvalues wereconsideredtobesignificantwhenp<0.05.
Results
Thefinalevaluationwasmadeafteranaveragepostoperative periodof23months(range:12–36).Thefinalmeanflexed con-tracturewas20◦(±13.70◦),witharangefrom0◦to40◦(Fig.2).
Thefinalmeanflexionwas132◦(±13.20◦),witharangefrom
90◦to150◦.ThefinalmeanROMwas112◦(±24.29◦).Themean
pronationwas70◦(±18.34◦),witharangefrom0◦to80◦.The
meansupinationwas63◦ (±19.92◦),witharangefrom0◦ to
80◦.
Themean DASHwas12(±15.36),witharangefrom0to 44.ThemeanMEPIwas87(±14.34),witharangefrom50to 100.TheindividualMEPIanalysisshowedthattherewere12 excellent,ninegood,fourfairandonepoorresult,i.e.80%of thepatientspresentedsatisfactoryresults.Theradiographic evaluationshowedthattherewerenodegenerativealterations in14 patients(54%),whilenine patientspresentedgrade1 alterations,onegrade2andnonegrade3.Inthecasesoftwo patients,noupdatedradiographicassessmentwaspossible.
Amongtheeightpatientswhoreceivedaradialhead pros-thesis,four(50%)presentedaflexion-extensionrangeofless than100◦.Inthegroupof17patientswhoseradialheadswere
reconstructed,onlythree(17%)hadaflexion-extensionrange oflessthan100◦.However,thesevalueswerenotstatistically
osteosynthesis.However,thesevalueswerenotstatistically significant (p=0.208). In this evaluation, the patient who underwent arthroplasty ofthe radial head using a methyl methacrylate molded prosthesis, which was subsequently removed, was excluded from the comparative analysis, despitepresentingMEPIof85◦andaflexion-extensionrange
of150◦.
Complications
Noneofthepatientspresentedanyinfections,dehiscenceof theoperativewoundorneurovascularlesions.Fivepatients hadcomplicationsthatrequiredsurgicaltreatment.One pre-sented avascularnecrosis and pseudarthrosisof the radial head and underwent removal of the synthesis material togetherwiththebonefragmentsfromtheradialhead,three monthsaftertheindexsurgery.Fourpatientsdevelopedelbow jointstiffness.Ofthese,twopresentedanteriorheterotopic ossificationandthreehadundergoneradialheadarthroplasty. Allofthemunderwentsurgicalreleaseoftheelbowin asso-ciationwith removaloftheradialhead prosthesisand the heterotopic ossification, in the cases in which these were present. In one patient, two osteocapsular releases of the elbowwereperformed.Oneofthepatientsdeveloped proxi-malradioulnarsynostosisafterremovaloftheprosthesis,and subsequentlyunderwenttheKaminemi–Morreyprocedure,20 buttherewasnogaininpronation-supination,becauseofthe neoformationofsynostosis.Thispatientrefusednewsurgery.
Discussion
Historically,publishedpapersontreatmentoftheterribletriad weresparse,presentedsmallcaseseriesandhaddifferent sur-gicalorconservativeapproaches.Allofthempresentedpoor resultsfromtreatmentsforthistypeofinjury.2,3,19
Recently,severalstudiesandinvestigationshaveprovided better understanding ofthe biomechanics and stability of theelbowandoftheinteractionsbetweenthesefactors21–28 and have contributed toward publication ofbetter surgical resultsfrom this injury. Pugh et al.4,5 described a system-atizedapproachforsurgicaltreatmentoftheterribletriadof theelbow,whichincludedosteosynthesisorarthroplastyof theradialhead,repairofthecoronoidifpossibleand/orthe jointcapsule,andrepairofthelateral ligamentcomplexof theelbow,alongwithmakingrepairstothemedialcollateral ligamentandusingexternalfixatorsfortheelbowinselected cases.Theseauthorsdemonstratedgoodandexcellentresults inmostoftheirpatientsandalsopresentedarevisionrate of15–25%.Subsequently,severalstudiespresentedconsistent andreproducibleresultsthroughusingthesamesystematized approach,withproportionsofgoodandexcellentresultsof 77–84%.6,9,13
Our study confirms the results from these morerecent studies and reinforces the reproducibility of satisfactory resultsamongpatientswhoundergotheapproachproposed byPughetal.Amongourpatients,80%presentedgoodand excellentresults,withameanMEPIof87pointsandamean DASH of 12. Nonetheless, 38% presented some degree of degenerative alterations, even though most of these were
mild,whichsupportsthenotionthatasubtledegreeofjoint instabilitypersists.Thiswouldgiverisetopoorfunctioning of the joint,witha consequent early start to degenerative alterationsinsomeoftheseelbows.Alongerfollow-upperiod wouldbeneededtoevaluatetheprogressionofthese degen-erativealterationsandtheirpossibleclinicalrepercussions.
Our null hypothesiswas corroborated.Although several papers have emphasized the importance oftrying to con-stitute the radiocapitellar joint anatomically or as closeto thisaspossible,therearenostudiesthathavecomparedthe resultsfromarthroplastyoftheradialheadwithother tech-niquesfortreatingtheterribletriad.VanGlabbeeketetal.29 describedtheimportanceofrestoringthelengthoftheradius afterarthroplastyoftheradialhead,inelbowswithinjuriesto themedialcollateralligament.Theseauthorsrecommended thatreplacementoftheradialheadshouldbedonewiththe sameaccuracyandreproducibilityregardingthepositionsof thecomponentsasinanyotherarthroplasty.Charalambouset et al.30 suggestedthatosteosynthesis oftheradialheadin patients withmedialcollateral ligament injuriespresented resultsthatweresuperiortothoseofarthroplastyand exci-sionoftheradialhead,withregardtothevarusstabilityof theelbow.Theradialheadprosthesisthatwehadavailableto uswasmodular,withjustthreesizepossibilities,allrelated tothenecklength:9mm,12mmand19mm.Therewereno variationsinthesizeoftheradialhead,thenailorthe bipo-larity.Thus,thisprosthesishastheprimaryfunctionofacting asaspacerandenablingadequatehealingofthesofttissues after the operation. We imagined that although this pros-thesiswouldbeunabletoreestablishtheradiocapitellarand proximalradioulnarjointsmoreprecisely,patients undergo-ingarthroplastyoftheradialheadwouldhaveresultssimilar tothosewhounderwentothertreatments.Incomparingthese groups, wedid notfindany statisticallysignificant results. Thus,webelievethatiftreatmentoftheradialheadis cho-sen, theresected radialhead shouldbereplacedbyarigid spacer, whichcould beametalprosthesisoraradialhead moldedfrommethylmethacrylate,aswasdoneinoneofour patients,untiladequatehealingofthesofttissueshasbeen achieved. Clearly, this isa conclusionfrom ashort follow-up andwithasmall groupofpatients, whichweakens the statisticalanalysis.Alongerfollow-upisnecessaryinorder demonstratewhetherthe“non-anatomical”reconstructionof theradialheadmighthaveconsequencesfortheelbow.
Thisstudypresentssomelimitations.Itwasa retrospec-tiveobservationalstudy withashortaveragefollow-up (23 months).Thisshortfollow-upmadeitimpossibletocorrectly assesstheincidence,progressionandclinicalrepercussions of secondary degenerative osteoarthrosis, which is one of themostfearedanddifficult-to-treatlatecomplications.The smallnumberofpatientsineachgroupevaluatedalso weak-enedthefinalanalysisofourhypothesis.
Conclusion
withosteosynthesisoftheradialheadandthosetreatedwith arthroplastyoftheradialheadorresectionofafragment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HotchkissRN.Fracturesanddislocationsoftheelbow.In: RockwoodCA,GreenDP,BucholzRW,HeckmanJD,editors. RockwoodandGreen’sfracturesinadults,1,4thed. Philadelphia:Lippincott-Raven;1996.
p.929–1024.
2. JosefssonPO,GentzCF,JohnellO,WendebergB.Dislocations oftheelbowandintraarticularfractures.ClinOrthopRelat Res.1989;(246):126–30.
3. RingD,JupiterJB,ZilberfarbJ.Posteriordislocationofthe elbowwithfracturesoftheradialheadandcoronoid.JBone JointSurgAm.2002;84A:547–51.
4. PughDM,McKeeMD.The“terribletriad”oftheelbow.Tech HandUpExtremSurg.2002;6(1):21–9.
5. PughDM,WildLM,SchemitschEH,KingGJ,McKeeMD. Standardsurgicalprotocoltotreatelbowdislocationswith radialheadandcoronoidfractures.JBoneJointSurg. 2004;86A:1122–30.
6. ForthmanC,HenketM,RingDC.Elbowdislocationwith intra-articularfracture:theresultsofoperativetreatment withoutrepairofthemedialcollateralligament.JHandSurg Am.2007;32(8):1200–9.
7. LindenhoviusAL,JupiterJB,RingD.Comparasionofacute versussubacutetreatmentofterribletriadinjuriesofthe elbow.JHandSurgAm.2008;33(6):920–6.
8. ZeidersGJ,PatelMK.Managementofunstableelbows followingcomplexfracture-dislocations–the“terribletriad” injury.JBoneJointSurgAm.2008;90Suppl.4:75–84. 9. WinterM,ChuinardC,CikesA,PelegriC,BronsardN,de
PerettiF.Surgicalmanagementoftheelbowdislocation associatedwithnon-reparablefracturesoftheradialhead. ChirMain.2009;28(3):158–67.
10.SeijasR,Ares-RodriguezO,OrellanaA,AlbaredaD,ColladoD, LlusaM.Terribletriadoftheelbow.JOrthopSurg(Hong Kong).2009;17(3):335–9.
11.GuittonTG,RingD.Nonsurgicallytreatedterribletriad injuriesoftheelbow:reportoffourcases.JHandSurgAm. 2010;35(3):464–7.
12.ChemamaB,BonnevialleN,PeterO,MansatP,BonnevialleP. Terribletriadinjuryoftheelbow:howtoimproveoutcomes? OrthopTraumatolSurgRes.2010;96(2):147–54.
13.Rodriguez-MartinJ,Pretell-MazziniJ,Andres-EstebanEM, Larrainzar-GarijoR.Outcomesafterterribletriadsofthe elbowtreatedwiththecurrentsurgicalprotocols:areview. IntOrthop.2011;35(6):851–60.
14.JeongWK,OhJK,HwangJH,HwangSM,LeeWS.Resultsof terribletriadsintheelbow:theadvantageofprimary restorationofmedialstructure.JOrthopSci.2010;15(5):612–9.
15.JohnstonGW.Afollow-upofonehundredcasesoffractureof theheadoftheradiuswithareviewoftheliterature.Ulster MedJ.1962;31:51–6.
16.O’DriscollSW,JupiterJB,CohenMS,RingD,McKeeMD. Difficultelbowfractures:pearlsandpitfalls.InstrCourseLect. 2003;52:113–34.
17.DuckworthAD,KulijdianA,McKeeMD,RingD.Residual subluxationoftheelbowafterdislocationor
fracture-dislocation:treatmentwithactiveelbowexercises andavoidanceofvarusstress.JShoulderElbowSurg. 2008;17(2):276–80.
18.HudakPL,AmadioPC,BombardierC.Developmentofan upperextremityoutcomemeasure:theDash(disabilitiesof thearm,shoulderandhand)[corrected].TheUpperExtremity CollaborativeGroup(UECG).AmJIndMed.1996;29(6):602–8. 19.BrobergMA,MorreyBF.Resultsofdelayedexcisionofthe
radialheadafterfracture.JBoneJointSurgAm. 1986;68(5):669–74.
20.KamineniS,MaritzNG,MorreyBF.Proximalradialresection forposttraumaticradioulnarsynostosis:anewtechniqueto improveforearmrotation.JBoneJointSurgAm.
2002;84-A(5):745–51.
21.MorreyBF,AnKN.Articularandligamentouscontributionsto thestabilityoftheelbowjoint.AmJSportsMed.
1983;11(5):315–9.
22.O’DriscollSW,BellDF,MorreyBF.Posterolateralrotatory instabilityoftheelbow.JBoneJointSurgAm.1991;73(3):440–6. 23.DunningCE,ZarzourZD,PattersonSD,JohnsonJA,KingGJ.
Ligamentousstabilizersagainstposterolateralrotatory instabilityoftheelbow.JBoneJointSurgAm.
2001;83-A(12):1823–8.
24.McKeeMD,SchemitschEH,SalaMJ,O’DriscollSW. Thepathoanatomyoflateralligamentousdisruptionin complexelbowinstability.JShoulderElbowSurg. 2003;12(4):391–6.
25.SchneebergerAG,SadowskiMM,JacobHA.Coronoidprocess andradialheadasposterolateralrotatorystabilizerofthe elbow.JBoneJointSurgAm.2004;86-A(5):975–82. 26.OkazakiM,TakayamaS,SekiA,IkegamiH,NakamuraT.
Posterolateralrotatoryinstabilityoftheelbowwith insufficientcoronoidprocessoftheulna:areportof3 patients.JHandSurgAm.2007;32(2):236–9.
27.HullJR,OwenJR,FernSE,WayneJS,BoardmanIIIND.Roleof thecoronoidprocessinvarusosteoarticularstabilityofthe elbow.JShoulderElbowSurg.2005;14(4):441–6.
28.TeradaN,YamadaH,SekiT,UrabeMD,TakayamaTS.The importanceofreducingsmallfracturesofthecoronoid processinthetreatmentofunstableelbowdislocation.J ShoulderElbowSurg.2000;9(4):344–6.
29.VanGlabbeekF,VanRieRP,BumfeldJA,NealePG,O’Driscol SW,MorreyBF,etal.Detrimentaleffectsofoverstuffingor understuffingwitharadialheadreplacementinthemedial collateral-ligamentdeficientelbow.JBoneJointSurgAm. 2004;86-A(12):2629–35.
30.CharalambousCP,StanleyJK,SiddiqueI,PowellE,
RamamurthyC,GageyO.Radialheadfractureinthemedial collateralligamentdeficientelbow;biomechanical