w w w . r b o . o r g . b r
Original
article
Analysis
of
the
characteristics
of
patients
with
open
tibial
fractures
of
Gustilo
and
Anderson
type
III
夽
Frederico
Carlos
Ja ˜na
Neto
a,b,∗,
Marina
de
Paula
Canal
b,
Bernardo
Aurélio
Fonseca
Alves
a,
Pablício
Martins
Ferreira
a,
Jefferson
Castro
Ayres
a,
Robson
Alves
caDepartmentofOrthopedicsandTraumatology,ConjuntoHospitalardoMandaqui,SãoPaulo,SP,Brazil bUniversidadeNovedeJulho,SãoPaulo,SP,Brazil
cServiceofTraumatologyandOrthopedics,InstitutoDr.JoséFrota,Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26March2015 Accepted1June2015
Availableonline29January2016
Keywords: Tibialfractures
Amputation/epidemiology Amputation/methods
a
b
s
t
r
a
c
t
Objective:ToanalyzethecharacteristicsofpatientswithGustilo–AndersonTypeIIIopen
tibialfracturestreatedatatertiarycarehospitalinSãoPaulobetweenJanuary2013and August2014.
Methods:Thiswasacross-sectionalretrospectivestudy.Thefollowingdataweregathered fromtheelectronicmedicalrecords:age;gender;diagnosis;traumamechanism; comorbidi-ties;associatedfractures;GustiloandAnderson,TscherneandAOclassifications;treatment (initialanddefinitive);presenceofcompartmentsyndrome;primaryandsecondary ampu-tations;MESS(MangledExtremitySeverityScore)index;mortalityrate;andinfectionrate. Results:116patientswereincluded:81%withfracturetypeIIIA,12%IIIBand7%IIIC;85% males;meanage32.3years;and57%victimsofmotorcycleaccidents.Tibialshaftfractures weresignificantlymoreprevalent(67%).Eightpatientsweresubjectedtoamputation:one primarycaseandsevensecondarycases.TypesIIIC(75%)andIIIB(25%)predominatedamong thepatientssubjectedtosecondaryamputation.TheMESSindexwasgreaterthan7in88% oftheamputeesandin5%ofthelimbsalvagegroup.
Conclusion: TheprofileofpatientswithopentibialfractureofGustiloandAndersonType
IIImainlyinvolvedyoungmaleindividualswhowerevictimsofmotorcycleaccidents.The
tibialshaftwasthesegmentmostaffected.Only7%ofthepatientsunderwentamputation. Given thecurrentcontroversyintheliteratureaboutamputationorsalvageofseverely injuredlowerlimbs,itbecomesnecessarytocarryoutprospectivestudiestosupportclinical decisions.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheComplexoHospitalardoMandaqui,SãoPaulo,SP,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](F.C.Ja ˜naNeto).
http://dx.doi.org/10.1016/j.rboe.2016.01.002
Análise
das
características
dos
pacientes
com
fratura
exposta
de
tíbia
grau
IIIde
Gustilo
e
Anderson
Palavras-chave: Fraturasdatíbia
Amputac¸ão/epidemiologia Amputac¸ão/métodos
r
e
s
u
m
o
Objetivo: AnalisarascaracterísticasdosindivíduoscomfraturaexpostadetíbiatipoIIIde
GustilloeAnderson,tratadosemumhospitaldenívelterciárioemSãoPaulo,entrejaneiro de2013eagostode2014.
Métodos: Estudotransversalretrospectivo.Foramcoletados dosprontuárioseletrônicos: idade, gênero, diagnóstico, mecanismo de trauma, comorbidades, fraturas associadas, classificac¸õesdeacordocomGustilloeAnderson,TscherneeAO,tratamento(iniciale defini-tivo),presenc¸adesíndromecompartimental,amputac¸õesprimáriasesecundárias,índice deMESS,índicesdemortalidadeeinfec¸ão.
Resultados: Foramincluídos116pacientes,81%comfraturatipoIIIA,12%IIIBe7%IIIC, 85%dogêneromasculino,médiade32,3anose57%vítimasdeacidentedemotocicleta.A fraturadadiáfisedatíbiafoisignificativamentemaisprevalente(67%).Oitopacientesforam submetidosàamputac¸ão,umaprimáriaesetesecundárias.HouvepredomíniodostiposIIIC (75%)eIIIB(25%)entreospacientescomamputac¸ãosecundária.OíndicedeMESSobteve pontuac¸ãomaiordoque7em88%dosamputadoseem5%dospacientescomomembro salvo.
Conclusão: OperfildospacientescomfraturaexpostadetíbiadetíbiatipoIIIdeGustilo
eAndersonenvolveuprincipalmenteindivíduosjovensdogêneromasculino,vítimasde acidentesdemotocicleta.Adiáfisedatíbiafoiosegmentomaisacometido.Apenas7%dos pacientesforamsubmetidosàamputac¸ão.Diantedacontrovérsiaexistentenaliteratura sobreaamputac¸ãoouosalvamentodomembroinferiorgravementelesionado,tornam-se necessáriosmaisestudosprospectivosparaapoiaraescolhaclínica.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Exposedfractures comprise any injury pattern that causes tearing of the soft-tissue envelope and results in direct communicationbetween the boneand the environment.1,2 Epidemiological data from Europe have demonstrated that therateofoccurrenceofexposedfracturesisapproximately 4%peryear,whichissimilartotheratesinotherdeveloped countries.Itisbelievedthatthisrateisequivalenttoaround 250,000fracturesperyearintheUnitedStates.1
Thedegreeofseverityofexposedfracturesisoften classi-fiedinaccordancewiththesystemofGustiloandAnderson.2,3 Thistakesintoaccountthewoundsize,fracturepatternand degreeofsoft-tissuecontamination.TypeIIIofthis classifica-tioncorrespondstofracturesduetohigh-energytrauma,with extensiveinjurytosofttissues,andisdividedintothree sub-types:typesIIIA,IIIBandIIIC,accordingtotheseverityofthe injury.1–3
TheextensivedamageseenintypesIIIBandIIICmaybea veritablechallenge,evenforsurgeonswithgreaterexperience. Itmayrequireaclinicaldecisionbetweenattemptstosalvage thelimbandamputation.Clinicaladvanceswithin orthope-dic,plastic and vascular surgeryhave providedthe means forreconstructinginjuriestolimbsthat,around20yearsago, wouldhaveresultedprimarilyinamputation.However,some studieshavereportedthatlimbsalvageisnotalwaysthebest
solutionandthatearlyamputationwithprosthetictreatment shouldberecommendedinsomecases.4–7
Some classification scores are used to complement the detailedclinicalassessmentontheaffectedlimbandaidin makingclinicaldecisions.8,9Helfetetal.7establishedtheuse oftheMangledExtremitySeverityScore(MESS),whichgrades injuries based on the clinical findings and takes into con-sideration the characteristics ofthe injury, the duration of ischemia,theshockandthepatient’sage.Scoresgreaterthan orequaltosevenhavepredictivevalueforlimbamputation.4 AccordingtoTufescu,6evaluationscorespredictlimbsalvage, andnotamputationorthefunctioningofthesalvagedlimb. Forthisreason,theycannotbeusedastheonlytoolfor choos-ingthetreatment.Rather,theyshouldbeusedinconjunction withthe clinicalassessmentandthe gradingoflower-limb impairment.
Although muchhas been now been reported regarding exposedfractures,thereisagapintheliteratureinrelationto studiespresentingahighlevelofevidencethathavecompared outcomes betweenlimb salvage and amputation. Thisgap existsbecauseofethicalconcernsregardingrandomization ofpatientsbetweenthesetwoprocedures.10–13 Thus,many oftherecommendationsthatareincorporatedintothe treat-mentroutinesforpatientswithexposedfracturesofthetibia andfibulaarebasedonspecialists’opinions.Thus,further sci-entificstudiesareneededinordertoprovidescientificbacking forsurgeons’andpatients’choicesbeforetheoperation.The objectiveofthis studywastoanalyzethe characteristicsof individualswithexposedfracturesofthetibiathatwere clas-sifiedasGustiloandAndersontypeIII.Thesepatientswere treatedinatertiary-levelhospitalinSãoPaulo,between Jan-uary2013andAugust2014.
Materials
and
methods
This retrospective cross-sectional study was conducted in the Mandaqui HospitalComplex inSão Paulo, Brazil.After approval had been granted by the institution’s Research EthicsCommittee(no.745.737),theelectronicfilesofpatients with a diagnosis of exposed fractures of the tibia that were classified as Gustiloand Anderson typeIII, and who were treated at this service between January 2013 and August 2014, were identified. The data were gathered by means of the HospGestor software, which is available at
https://www.hgresidencia.com.br.Thedatainthissystemare
updatedevery daybythetraumatologyteamofthis hospi-tal.Thefollowingcharacteristicswereanalyzed:number of amputations(primaryandsecondary)andnumberofsalvage procedures on the limbaffected; degree ofseverity ofthe exposedfractures,classifiedinaccordancewithGustiloand Anderson,2,3classificationofOesternandTscherne13for eval-uatingthe condition ofthe soft tissue;MESS index,(x) age; gender;diagnosis(typeoffractureandclassificationin accor-dancewith AO/OTA)14; injury mechanism;multipletrauma (morethanoneorganaffected);associatedfractures;presence ofcomplications(compartmentsyndromeandinfection)and mortalityrate.
Thedatawere analyzedstatisticallyand the mean was calculated (with minimum and maximum values) for the continuousoutcomes;andfrequencyandpercentageforthe dichotomousdata(95%confidenceinterval).
Patientswithincompletemedicalfilesand/orlackof radio-graphicexaminations,andthosewhohadtransferredtoother services,wereexcluded.Thestatisticalanalysisonthedata consistedofdescriptiveanalysisonthecontinuousdata,with calculationofmeans,standarddeviationsand95%confidence intervals.Student’sttestandanalysisonrelativefrequencies witha95%confidenceintervalwereusedforthedichotomous data.
Results
Theinitialselectionincluded 126patientswhofulfilledthe inclusioncriteria.However,tenwereexcludedbecausetheir treatment was transferred to another service. Thus, the
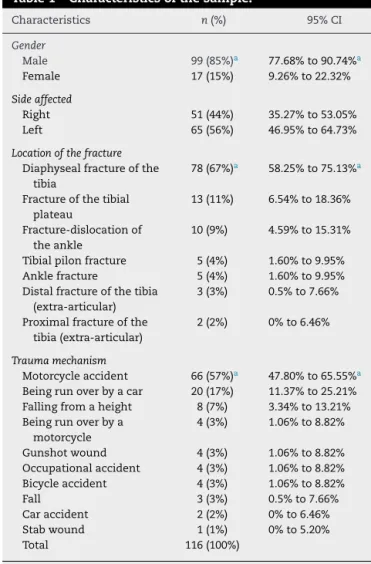
Table1–Characteristicsofthesample.
Characteristics n(%) 95%CI
Gender
Male 99(85%)a 77.68%to90.74%a
Female 17(15%) 9.26%to22.32%
Sideaffected
Right 51(44%) 35.27%to53.05%
Left 65(56%) 46.95%to64.73%
Locationofthefracture Diaphysealfractureofthe
tibia
78(67%)a 58.25%to75.13%a
Fractureofthetibial plateau
13(11%) 6.54%to18.36%
Fracture-dislocationof theankle
10(9%) 4.59%to15.31%
Tibialpilonfracture 5(4%) 1.60%to9.95%
Anklefracture 5(4%) 1.60%to9.95%
Distalfractureofthetibia (extra-articular)
3(3%) 0.5%to7.66%
Proximalfractureofthe tibia(extra-articular)
2(2%) 0%to6.46%
Traumamechanism
Motorcycleaccident 66(57%)a 47.80%to65.55%a Beingrunoverbyacar 20(17%) 11.37%to25.21% Fallingfromaheight 8(7%) 3.34%to13.21% Beingrunoverbya
motorcycle
4(3%) 1.06%to8.82%
Gunshotwound 4(3%) 1.06%to8.82%
Occupationalaccident 4(3%) 1.06%to8.82% Bicycleaccident 4(3%) 1.06%to8.82%
Fall 3(3%) 0.5%to7.66%
Caraccident 2(2%) 0%to6.46%
Stabwound 1(1%) 0%to5.20%
Total 116(100%)
a Statisticallysignificantdifference.
sample was composed of116 patients witha diagnosis of exposedfractureofthetibiaofGustiloandAndersontypeIII. Amongthese,81%presentedtypeIIIA(95%CI,73%to87%), 12%IIIB(95%CI,7%to19%)and7%IIIC(95%CI,3%to13%). Therewassignificantpredominanceofthemalegender(85%; 95%CI,78%to91%)andthemeanageofthesamplewas32.3 years (± 15.70).Theleft sidewasaffected morefrequently, but withoutasignificantdifference(56%; 95%CI,46.95%to 64.73%).Trafficaccidentsweretheinjurymechanismin84%of thecases,withasignificantdifferenceinrelationtoaccidents involvingmotorcycles:57%;95%CI,47.80%to65.55%). Frac-turesofthetibialdiaphysisweresignificantlymoreprevalent and were diagnosed in 78 patients (67% of the total sam-ple;95%CI,58.25%to75.13%),followedby13patientswith fracturesofthetibialplateau(11%;95%CI,6.54%to18.36%)
(Table1).InrelationtotheAO/OTAclassification,20%ofall
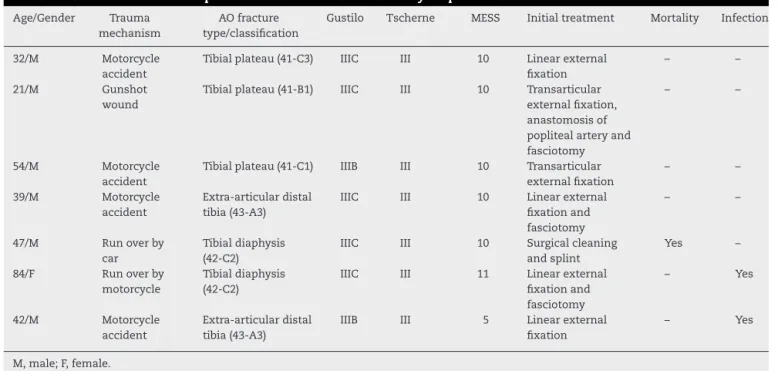
Table2–Characteristicsofthepatientswhounderwentsecondaryamputation.
Age/Gender Trauma mechanism
AOfracture type/classification
Gustilo Tscherne MESS Initialtreatment Mortality Infection
32/M Motorcycle
accident
Tibialplateau(41-C3) IIIC III 10 Linearexternal fixation
– –
21/M Gunshot
wound
Tibialplateau(41-B1) IIIC III 10 Transarticular externalfixation, anastomosisof poplitealarteryand fasciotomy
– –
54/M Motorcycle
accident
Tibialplateau(41-C1) IIIB III 10 Transarticular externalfixation
– –
39/M Motorcycle
accident
Extra-articulardistal tibia(43-A3)
IIIC III 10 Linearexternal
fixationand fasciotomy
– –
47/M Runoverby
car
Tibialdiaphysis (42-C2)
IIIC III 10 Surgicalcleaning
andsplint
Yes –
84/F Runoverby
motorcycle
Tibialdiaphysis (42-C2)
IIIC III 11 Linearexternal
fixationand fasciotomy
– Yes
42/M Motorcycle
accident
Extra-articulardistal tibia(43-A3)
IIIB III 5 Linearexternal
fixation
– Yes
M,male;F,female.
20%
1%
1% 2%
5% 3%
1% 6%
3% 8%
13%
9% 8%
2%
2% 3%2%2%2%
1% 5%
3%
41-A1 41-A2 41-B1 41-C1 41-C2 41-C3 42-A2 42-A3 42-B1 42-B2 42-B3 42-C1 42-C2 42-C3 43-A3 43-C1 43-C2 44-A1 44-A2 44-A3 44-B1 44-B3 44-C2 1%
Fig.1–SampledistributionaccordingtotheAO/OTA classificationsystem.
IIIC,TschernetypeIIIandMESSindex11,andwhopresented irreversibleinjurytothepoplitealartery.
Amongthesevenpatientswhorequiredsecondary ampu-tation,threepresentedfracturingofthetibialplateau,twoof thetibialdiaphysis,oneoftheproximaltibia(extra-articular) andoneofthedistaltibia(extra-articular).Inrelationtothe Gustiloand Andersonclassification,typeIIICfractures pre-dominated(fivepatients),whiletwopatientspresentedtype IIIB.ThescoresintheMESS indexweresimilar amongthe patients(meanof9.5).Themeantimethatelapsedbetween theinitialtreatmentandthesecondaryamputationwas17.5 days(range:5–40).Themainreasonsforreachingthisdecision wereproblemswithreperfusion(fourpatients)andinfection ofsofttissueswithpurulent secretionand extensiveareas ofnecrosis(threepatients). Amongthesevenpatientswho underwent secondary amputation, two presentedinfection thatwastreatedandonediedduetocomplicationsrelating toreperfusionandmultipleorganfailure(Table2).
The 108 patients whose affected limb was salvaged presented characteristics that differed from those of the
amputees. Asignificant majority oftheseindividuals (87%; 95%CI,79%to92%)presentedtheGustilotypeIIIA classifica-tion,whileinthegroupofamputeestherewereonlyfractures oftypeIIIB(25%;95%CI,6%to60%)andtypeIIIC(75%;95% CI,40%to94%)and nosignificantdifferencecouldbeseen. Themeanageamongtheamputeeswas42.62(±22.26)years anditwas31.57(±14.96)yearsintheothergroup(P=0.0543). Therewasalsoadifferencebetweentheamputeesandthe patientswhoselimbsweresalvagedinrelationtotheMESS index,suchthat88%oftheamputeeshadscoresgreaterthan seven(95%CI,51%to99%),comparedwith5%inthe other group(95%CI,2%to11%).Thesamewasobservedregarding the numberofmultipletraumapatients, suchthatthe fre-quencyofthisconditionwas50%amongtheamputees(95% CI,22%to78%),whereasitwas9%amongthosewhoselimb wassalvaged(95%CI,4%to15%);regardingassociated frac-tures, 50%(95%CI,22%to78%)versus19%(95%CI,13%to 28%),respectively;andregardingdiagnosesofcompartment syndrome,38%(95%CI,13%to70%)versus6%(95%CI,3%to 13%),respectively.Theinfectionratewassignificantly differ-ent,comprising62%amongtheamputees(95%CI,30%to87%) and17%amongthosewhoselimbwassalvaged(95%CI,11%
to25%)(Table3).
Discussion
Table3–Distributionofthecharacteristicsofamputatedpatientscomparedwiththosewhoselimbwassalvaged.
Amputation%(95%CI) Salvagedlimb%(95%CI) Total%(95%CI)
Male(%) 88%(51%to99%)a 85%(77%to91%)a 85%(78%to91%)a
GustiloandAnderson(%)
IIIA 0%(0%to37%) 87%(79%to92%)a 81%(73%to87%)a
IIIB 25%(6%to60%) 11%(6%to19%) 12%(7%to19%)
IIIC 75%(40%to94%) 2%(0%to7%) 7%(3%to13%)
Tscherneclassification(%)
I 0%(0%to37%) 2%(0%to8%) 3%(1%to8%)
II 0%(0%to37%) 80%(71%to86%)a 74%(65%to81%)a
III 100%(63%to100%)a 18%(11%to26%) 23%(16%to32%)
MESS(%)
<7 12%(0%to49%) 95%(89%to98%)a 90%(83%to94%)a
≥7 88%(51%to99%)a 5%(2%to11%) 10%(6%to17%)
Multipletrauma(%) 50%(22%to78%) 9%(4%to15%) 11%(6%to18%)
Associatedfractures(%) 50%(22%to78%) 19%(13%to28%) 22%(15%to30%)
Compartmentsyndrome(%) 38%(13%to70%) 6%(3%to13%) 9%(5%to15%)
Infection(%) 62%(30%to87%) 17%(11%to25%) 20%(13%to28%)
Mortality(%) 12%(0%to49%) 1%(0%to6%) 2%(0%to6%)
Total(n) 8 108 116
a Statisticallysignificantdifference.
higherincidenceamongyoungmenofproductiveagethat wasdemonstratedinthepresentstudycorrelatesdirectlywith thesefactors,especiallywithregardtotheinjurymechanism. Themaininjurymechanismsforexposedtibialfractures aretrafficaccidents,violence,occupationalaccidentsand seri-ousgunshotwounds.15Theanalysisonthedatagatheredin thisstudycorroboratesthisdescription:84%oftheexposed fractures were causedby trafficaccidents, especiallythose involvingmotorcycles(57%).
Severalscoringsystemsforassistinginmakingdecisions regardingamputationorsalvageofthewoundedlimbhave been described.5 TheMESSindex isperhapsthe onemost used,bothinclinicalpracticeandinscientificcircles,although controversystillexistsinrelationtoitssensitivityand speci-ficity.
Inthe presentstudy,MESS scoresgreater thanor equal tosevenwereobservedin88%oftheamputationcases,but inonly5% ofthe limbsalvage cases. Furthermore,among thepatientssubjectedtoamputation,75%oftheirfractures wereclassifiedastypeIIICand25%astypeIIIBofGustiloand Anderson.Fagelmanetal.16evaluatedthecorrelationbetween fracturesofGustiloandAndersontypesIIIBandIIICandthe MESSindexforexposedfracturesofthelowerlimbsandfound resultsthatsignificantlypredictedtreatment,for93%.Onthe otherhand,Sheeanetal.17didnotfindanysignificant differ-enceinMESSvaluesbetweenamputeesandpatientswhose limbswere salvaged.Both oftheseauthors highlightedthe importanceofthe presence ofvascular lesions asa factor predictiveofamputation. Slauterbecket al.18 reportedthat earlyuseofascoringsystemsuchasMESSwould possibly reducethemorbidityassociatedwithprolongedhospitalstay andwiththevarioussurgicalproceduresperformedinthese cases.
Dua et al.19 conducted a retrospective cross-sectional study and demonstrated that better control over harm to patients,evolutionofsurgicaltechniquesandshorterduration
ofischemiawerebenefitsthatcontributed towardreducing the morbidity and mortalityrates. However,evenwith the advances in these techniques, deciding whether to recon-structandsalvagealimbortoamputateitremainsamatterof controversyincasesofcomplexexposedfractureswith asso-ciatedinjuriestoadjacenttissues.
Sgarbi et al.20 emphasized that it was important that patientswithexposed tibialfracturesofGustiloand Ander-sontypeIIIshouldbetreatedathospitalservicesthathave fullresourcesavailableforensuringthatsalvageofthelimb affectedmightbepossible.However,salvageoflowerlimbs affected by crushing and extensive soft-tissue injuries, in multipletraumavictims,mayresultinseveremetabolic alter-ationsandtheriskofsepsisthroughsystemicdissemination ofinfection.Thus,suchinjuriesneedtobecarefullyassessed bytheteam.
According toSlauterbecket al.,18 preservationofalimb withseveralattemptstosalvageitmaybeshowntobe unvi-able,giventhatthelimbbecomesinsensitiveandincapableof functionalrecoveryandthereisgreaterriskofmorbidityand mortalitydue tothe prolongedhospitalization and various surgicalprocedures.
It isalso importantto take into consideration the high costsandthefinancial,personalandsocialexpensethatmay resultfromamputationsthataretheoretically“unavoidable” butwhichareoftenpostponed.Theabsoluteindicationsfor primaryamputationofthelowerlimbsincludecomplete avul-sionofthelimb,injurytothepoplitealartery,ischemialasting morethansixhours,neurologicalinjuries,gaseousgangrene andimpossibilityofrestoringthecirculatoryflow.20
casesrequiredsecondaryinterventionbecausetheattempts tosalvagethelimbfailed.Amongthemainreasonsthatled tosecondaryamputationweresoft-tissueinfection,presence ofextensiveareasofnecrosisandvascularand reperfusion-relatedcomplications.
Duaetal.19 reportedthathistorically,the highmortality rates relating to the need forrevascularization of severely injuredlimbsmadeitmoreacceptabletomakethedecision toamputatetheinjuredsegment.Inthepresentstudy,two cases ofdeath relating to severe deficit of perfusion were recorded(2.4%ofthetotalsample):onepatientwho under-went secondary amputation (47-year-old man who was a victimofbeingrunover,withanexposedfractureofthe tib-ialdiaphysisoftypeIIICandMESSindexof10points);and another,forwhomthetreatmentdecisionwaslimbsalvage (88-year-oldwomanwhowasavictimoffallingdownstairs, withanexposedtibialpilonfractureoftypeIIICandMESS indexof7).
Thefinaldecisionregardingthetreatmentforpatientswith adiagnosisofanexposedfractureofthetibianeedstotake intoaccountfuturefunctionality,availabilityofrecovery,the patient’sprofileandthesurgeon’sexpertise.Thecriteriafor indicatorssuchastheMESSscoreandthefracture classifica-tionneedtobecarefullyanalyzedsothatthelimbsalvagecan bedoneinaneffectivemannerandsothatamputationisdone inpreciselyselectedcases.15,16
Theretrospectivedata-gatheringofthisstudycanbe con-sideredtobealimitation.Thus,thereisanevidentneedfor prospectivestudies, especially giventhe lackof studies of goodmethodologicalquality.Theinformedconsentstatement foramputationsthatisused inhospitalservices attending traumapatientsneedstoincludethedetailedorthopedicand vascularevaluation,alongwithpredictivefactorssuchasthe MESSindex,theGustiloandAndersonclassificationandthe Tscherneclassification.Itshouldalsoincludetheevolution ofthetreatmentandqualityscientificevidence,sothatsuch studiescancontributetowardbettertreatmentforpatients whoarevictimsofseveretraumatothelowerlimbs.
Conclusion
Asshownbythesampleanalyzedinthisstudy,thepatient profileamongtheseindividualswithexposedtibialfractures ofGustiloandAndersontypeIIImainlyinvolvedyoungmales ofproductiveagewhoweretrafficaccidentvictims,especially relatingtomotorcycles.Asignificantmajority(81%)presented fracturesofthetibialdiaphysisoftypeIIIA.Only7%ofthese patientsunderwentamputation:75%withGustiloand Ander-sontypeIIICand25%withtypeIIIB.AMESSindexwithscores greaterthanorequaltosevenwasobservedin88%ofthecases ofamputation, comparedwith5%ofthecasesoflimb sal-vage.Inthelightofthescarcityofstudiesandthecontroversy thatexistsintheliteratureregardingamputationversus sal-vageforseverelyinjuredlowerlimbs,prospectivestudiesthat providegood-qualityscientificevidenceregardingthe crite-riaformakingtreatmentchoicesincasesofcomplexexposed tibialfracturesbecomenecessary.Throughthis,better func-tionalprognosesandreductionsinmorbidityandmortality ratesmaybeachieved.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KamathAF,HorneffJG,EsterhaiJL,LackeyWG,JerayKJ,
BroderickJS.Openfractures.In:BhandariM,editor.
Evidence-basedorthopedics.Oxford:BlackwellPublishing;
2012.p.617–26.
2.GustiloRB,AndersonJT.Preventionofinfectioninthe
treatmentofonethousandandtwenty-fiveopenfracturesof
longbones:retrospectiveandprospectiveanalyses.JBone
JointSurgAm.1976;58(4):453–8.
3.GustiloRB,MendozaRM,WilliamsDN.Problemsinthe
managementoftypeIII(severe)openfractures:anew
classificationoftypeIIIopenfractures.JTrauma.
1984;24(8):742–6.
4.BusseJW,JacobsCL,SwiontkowskiMF,BosseMJ,BhandariM.
Complexlimbsalvageorearlyamputationforsevere
lower-limbinjury:ameta-analysisofobservationalstudies.J
OrthopTrauma.2007;21(1):70–6.
5.FochtmannA,MittlböckM,BinderH,KöttstorferJ,HajduS.
Potentialprognosticfactorspredictingsecondaryamputation
inthird-degreeopenlowerlimbfractures.JTraumaAcute
CareSurg.2014;76(4):1076–81.
6.TufescuTV.Mangledextremity.In:BhandariM,editor.
Evidence-basedorthopedics.1sted.Oxford:Blackwell
Publishing;2012.p.655–60.
7.HelfetDL,HoweyT,SandersR,JohansenK.Limbsalvage
versusamputation.PreliminaryresultsoftheMangled
ExtremitySeverityScore.ClinOrthopRelatRes.
1990;(256):80–6.
8.JohansenK,DainesM,HoweyT,HelfetD,HansenSTJr.
Objectivecriteriaaccuratelypredictamputationfollowing
lowerextremitytrauma.JTrauma.1990;30(5):568–72,
discussion572–3.
9.RobertsonPA.Predictionofamputationafterseverelower
limbtrauma.JBoneJointSurgBr.1991;73(5):816–8.
10.McNamaraMG,HeckmanJD,CorleyFG.Severeopenfractures
ofthelowerextremity:aretrospectiveevaluationofthe
MangledExtremitySeverityScore(MESS).JOrthopTrauma.
1994;8(2):81–7.
11.GeorgiadisGM,BehrensFF,JoyceMJ,EarleAS,SimmonsAL.
Opentibialfractureswithseveresoft-tissueloss.Limb
salvagecomparedwithbelow-the-kneeamputation.JBone
JointSurgAm.1993;75(10):1431–41.
12.Saddawi-KonefkaD,KimHM,ChungKC.Asystematicreview
ofoutcomesandcomplicationsofreconstructionand
amputationfortypeIIIBandIIICfracturesofthetibia.Plast
ReconstrSurg.2008;122(6):1796–805.
13.OesternH-J,TscherneH.Pathophysiologyandclassification
ofsofttissueinjuriesassociatedwithfractures.In:Tscherne
H,GotzenL,editors.Fractureswithsofttissueinjuries.Berlin:
Springer-Verlag;1984.p.1–8.
14.MarshJL,SlongoTF,AgelJ,BroderickJS,CreeveyW,DeCoster
TA,etal.Fractureanddislocationclassificationcompendium
–OrthopaedicTraumaAssociationclassification,database
andoutcomescommittee.JOrthopTrauma.2007;2110
Suppl.:S1–133.
15.FodorL,SobecR,Sita-AlbL,FodorM,CiuceC.Mangledlower
extremity:canwetrusttheamputationscores?IntJBurns
Trauma.2012;2(1):51–8.
16.FagelmanMF,EppsHR,RangM.Mangledextremityseverity
scoreinchildren.JPediatrOrthop.2002;22(2):182–4.
17.SheeanAJ,KruegerCA,NapieralaMA,StinnerDJ,HsuJR.
Evaluationofthemangledextremityseverityscorein
combat-relatedtypeIIIopentibiafracture.JOrthopTrauma.
2014;28(9):523–6.
18.SlauterbeckJR,BrittonC,MoneimMS,ClevengerFW.Mangled
extremityseverityscore:anaccurateguidetotreatmentof
theseverelyinjuredupperextremity.JOrthopTrauma.
1994;8(4):282–5.
19.DuaA,DesaiSS,ShahJO,LaskyRE,Charlton-OuwKM,
AzizzadehA,etal.Outcomepredictorsoflimbsalvagein
traumaticpoplitealarteryinjury.AnnVascSurg.
2014;28(1):108–14.
20.SgarbiMWM,GotfrydAO.Amputac¸ãooureconstruc¸ãoda
extremidadeesmagada:utilizac¸ãodoÍndicedaSíndrome
daExtremidadeEsmagada.ActaOrtopBras.2006;14(5):
264–7.
21.DurhamRM,MistryBM,MazuskiJE,ShapiroM,JacobsD.
Outcomeandutilityofscoringsystemsinthemanagement