www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Effect
of
cigarette
smoke
on
counts
of
immunoreactive
cells
to
eotaxin-1
and
eosinophils
on
the
nasal
mucosa
in
young
patients
with
perennial
allergic
rhinitis
夽
Bertha
Beatriz
Monta˜
no-Velázquez
a,
Eulalia
Beatriz
Flores-Rojas
a,
Francisco
Javier
García-Vázquez
b,
Silvio
Jurado-Hernandez
a,
Marco
Antonio
Venancio
Hernández
c,
Angélica
Kathya
Alanis
Flores
c,
Kathrine
Jáuregui-Renaud
d,∗aInstitutoMexicanodelSeguroSocial,CentroMédicoNacionalLaRaza,ServiceofOtorhinolaryngology,MexicoCity,Mexico bInstitutoNacionaldePediatría,MolecularPathologyLaboratory,DepartmentofPathologyAnatomy,MexicoCity,Mexico cInstitutoMexicanodelSeguroSocial,CMNLaRaza,HospitaldeEspecialidades,ServiceofImmunologyandAllergy,MexicoCity,
Mexico
dInstitutoMexicanodelSeguroSocial,CentroMédicoNacionalsXXI,P.B.EdificioCSaludenelTrabajo,MedicalResearchUnitin
Otoneurology,MexicoCity,Mexico
Received11January2016;accepted27April2016 Availableonline19May2016
KEYWORDS Rhinitis; Allergic; Tobacco;
ChemokineCCL11;
Eosinophils
Abstract
Introduction:Inteenagerswithperennialallergicrhinitis,exposuretotobaccocigarettesmoke increasesthecountofeosinophilsinthenasalmucosa;therecruitmentofeosinophilsarises fromthecombinedactionofanumberofcellularandmolecularsignals,includingeotaxin.
Objective:To assess the effect of exposure to tobacco cigarette smoke on the count of immunoreactivecellstoeotaxin-1andeosinophilsonthenasalmucosaofchildrenandteenagers withperennialallergicrhinitis.
Methods:Inacross-sectionalstudy,forty-fourpatientswereevaluated(aged7---19yearsold): 22withand22withnoexposuretotobaccocigarettesmoke.Afterreplyingto2validated ques-tionnaires,onAsthmaandAllergiesinChildhoodandontheseverityofnasalsymptoms,nasal mucosalsamples wereobtainedby scrapingthemiddleone-thirdoftheinferiorturbinates. Thencountsofimmunoreactivecellstoeotaxin-1andeosinophilswereassessedby immuno-histochemistry.
夽 Pleasecitethisarticleas:Monta˜no-VelázquezBB,Flores-RojasEB,García-VázquezFJ,Jurado-HernandezS,VenancioHernándezMA,
AlanisFloresAK,etal.Effectofcigarettesmokeoncountsofimmunoreactivecellstoeotaxin-1andeosinophilsonthenasalmucosain youngpatientswithperennialallergicrhinitis.BrazJOtorhinolaryngol.2017;83:420---5.
∗Correspondingauthor.
E-mail:[email protected](K.Jáuregui-Renaud).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.011
Results:Patientswithexposuretotobaccocigarettesmokeshowedhighercellcountsofboth eotaxin-1andeosinophilsthanpatients withnoexposuretothesmoke, withnocorrelation betweenthetwovariables.However,bothcounts,ofeotaxin-1andeosinophils,wererelated tothecotinine/creatinineratio.
Conclusions: Exposureto tobaccocigarette smokecan increase eotaxin-1and thecount of eosinophilsinthenasalmucosaofyoungpatientswithperennialallergicrhinitis.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Rinite;
Alérgico; Tabaco;
QuimiocinaCCL11;
Eosinófilos
Efeitodotabagismonascontagensdecélulasimunorreativasaeotaxina-1 eeosinófilosnamucosanasalempacientesjovenscomrinitealérgicaperene
Resumo
Introduc¸ão: Emadolescentescomrinitealérgicaperene,aexposic¸ãoàfumac¸adocigarrode tabacoaumentaacontagemde eosinófilosnamucosa nasal.Orecrutamento deeosinófilos surgedaac¸ãocombinadadealgunssinaiscelularesemoleculares,incluindoaeotaxina.
Objetivo: Avaliaroefeitodaexposic¸ãoàfumac¸adocigarrodetabaconacontagemdecélulas imunorreativasaeotaxina-1eeosinófilosnamucosanasaldecrianc¸aseadolescentescomrinite alérgicaperene.
Método: Emumestudotransversal,44pacientesforamavaliados(entresetee19anos):22com e22semexposic¸ãoàfumac¸adocigarrodetabaco.Depoisderesponderadoisquestionários validados,sobreasmaealergiasnainfânciaesobreagravidadedossintomasnasais,asamostras demucosanasalforamobtidaspormeioderaspagemdoterc¸omédiodasconchasinferiores.Em seguida,ascontagensdecélulasimunorreativasparaeotaxina-1eeosinófilosforamavaliadas porimuno-histoquímica.
Resultados: Ospacientescomexposic¸ãoàfumac¸adocigarrodetabacoapresentaramcontagens decélulasmaiselevadastantoparaeotaxina-1comoparaeosinófilosemcomparac¸ãocomos pacientessemexposic¸ãoàfumac¸a,semcorrelac¸ãoentreasduasvariáveis.Noentanto,ambas ascontagens,deeotaxina-1eeosinófilos,foramrelacionadascomarazãocotinina/creatinina.
Conclusões: Aexposic¸ãoàfumac¸adocigarrodetabacopodeaumentaraeotaxina-1ea con-tagemdeeosinófilosnamucosanasaldepacientesjovenscomrinitealérgicaperene. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Allergicdiseases, such asallergicasthma, allergicrhinitis and atopic dermatitis are characterized by an increased numberofeosinophilsinthecirculatingblood,and degranu-lationinthetargettissueisconsideredthemajorpathogenic event.1Therecruitmentofeosinophilsarisesfromthe
com-binedactionofanumberofcellularandmolecularsignals, includingeotaxin.2,3Eotaxin-1bindswithhighaffinitytoCC
chemokine receptor3,which is expressed bya varietyof inflammatory cells.4---6 Blocking eotaxin or CCR3 has been
proposedas anew approachtoallergyimmunotherapy.7,8
However,moreinformationabouttheinteractionbetween theligandsandtheirreceptorsisrequired.
Allergic rhinitis is a common condition affecting peo-pleofallages,withpeaklifetimeprevalenceoccurringin teenagers.9 Ithasbeenshownthat,in adultpatientswith
allergicrhinitis,nasalallergenchallengemayledtoparallel increasesofthecountofeosinophils andeotaxinlevelsin nasallavagefluid,withastrongcorrelationbetweenthetwo
variables.10 Innaturalconditionsofdisease,withoutnasal
challenge,comparedwithcontrols,eotaxin-1concentration innasal lavagefluid frompatients withallergicrhinitis is increasedinboth,theperennialandseasonalforms,andit isrelatedtothepercentageof lavageeosinophilsandthe severityofsymptomexpression.11
Childrenexposedtoenvironmentaltobaccosmokehave anincreasedrisk of developingrespiratory-tractillnesses. Experiments in murine models show that tobacco smoke can elicit a rapid and prolonged exaggerated immune response.12,13 In humans,theeffectsof tobaccosmoke on
theupperrespiratoryairwaysincludetherecruitmentand activationofinflammatorycells.14Inteenagerswith
peren-nialallergicrhinitis,patientsexposedtotobaccocigarette smoke,comparedwiththosewithnoexposure, mayhave anincreasedcountofeosinophilsinthenasalmucosa.15 In
patientswithasthmasmokingincreaseseotaxinlevels.16
nasalmucosaofchildrenandteenagerswithperennial aller-gicrhinitis.
Methods
Ethicalconsiderations
TheprotocolwasapprovedbytheLocalResearchandEthics Committee, and informed consent was obtained from all patientsandtheirparents.
Participants
Forty-fourpatients withperennial allergicrhinitis partici-patedinthe study,allliving withinthe samecity areaof MexicoCity.Inclusioninthestudy wasconsidered consec-utively when perennialallergic rhinitis was diagnosed for the first timeand patients had noevidence of infection, sinusitis,otitismedia,nasalpolyps,anatomicalabnormality, systemicdisease,lungdisease,asthma, atopicdermatitis, seasonal allergic rhinitis or pregnancy; neither they have used immunotherapy, corticosteroids (nasal or systemic), cromolin,anti-inflammatorytreatment orantileukotrienes within3monthspriortoparticipatinginthestudy.
Accordingtotheexposure totobaccocigarettesmoke, they were classified in two groups, with a similar age, weight, body mass index and time of clinical evolution
(Table1):
Group I --- 22 patients exposed to tobacco cigarette smoke.Theywereaged7---19years(mean±standard devi-ation12±3years),12weremalesand10werefemales.
GroupII---22patientsnotexposedtotobaccocigarette smoke.They were aged7---17 years (11.9±3.2 years),15 weremalesand7werefemales.
Procedures
Exposure or noexposure to tobacco cigarettesmoke was determinedbymeansofTheGlobalYouthTobaccoSurvey,17
and by urinary cotinine/creatinine ratio.18 On the same
day that participants replied to the questionnaire, their urinewascollectedtoassesstheircotinine/creatinineratio. Only when the twoevaluations were consistent, patients were included in the study.The cotinine/creatinine ratio wasassessedbysolid-phasecompetitivechemiluminescent immunoassay for cotinine (Metabolites of Nicotine, DPC France; Immulite 1000, DPC, NJ, USA) and colorimetric Jaffé method for creatinine (ClinicalChemistry ILTestTM,
Spinreac, Saint Esteve deBas, Spain; ExpressPlus, Bayer, Tarrytown, NY, USA). A cut-off value of 21.8ng/mg of cotinine/creatinine ratiowasusedtoidentifyexposureto tobaccosmoke.18
After a clinical evaluation was performed, patients replied to the short version of the questionnaire from the‘‘InternationalStudy ofAsthmaandAllergiesin Child-hood’’9 and a validated questionnaire of the severity of
nasalsymptomsinchildrenwithperennialallergicrhinitis.19
Thesymptomsevaluatedwere:congestion,sneezing, itch-ingandrhinorrhea.Theseverityofeachsymptomwasrated by the patient as absent (0), mild (1), moderate (2) or severe(3).Totalsymptomscorewascalculatedasthesum of each symptom score(maximum=12).19 In children and
teenagerswithperennialallergicrhinitis,thisquestionnaire hasshown aconsistency of0.89 andrepeatabilityof 96%, witharepeatabilitycoefficientof2.20
Nasal mucosal samples were obtained by scraping the middle one-third of the inferior turbinates (Rhinoprobe Arlington Scientific Inc., Arlington, TX, USA) and were stainedwithWright-Giemsastain.Allsampleswereanalyzed
Table1 Characteristicsof44patientswithperennialallergicrhinitis:22withand22withnoexposuretocigarettetobacco smoke.
Variables(mean±SD) Passiveexposure(n=22) Noexposure(n=22) p≤0.05
Age(years) 12.09±3.0 11.9±3.2
---Weight(kg) 47.09±14.99 44.46±15.48
---Height(m) 1.48±0.13 1.45±0.16
---Bodymassindex 20.98(4.6) 20.44(3.43)
---Timeofclinicalevolution(years) 3.6±2.1 4.4±3.3
---Urinecotinine/creatinineratio(ng/mg) 25.98±3.7 11.21±2.47 ≤0.01
Eotaxin-1(immunoreactivecellspersquaremillimeter) 194±178 4±7 ≤0.01
Eosinophilscount(immunoreactivecellspersquaremillimeter) 198±264 18±40 ≤0.01
Allergens Frequency(n) Frequency(n)
Dermatophagoidessp. 40%(9) 50%(11)
---Housemites 45%(10) 36%(8)
---Cockroach 32%(7) 36%(8)
---Nasalsymptoms Frequency(n) Frequency(n)
Obstruction 90%(20) 86.36%(19)
---Rhinorrhea 95.45%(21) 95.45%(21)
---Itching 81.81%(18) 81.81%(18)
---Sneezing 86.36%(19) 68.18%(15)
---by immunohistochemistry, by two independentreviewers,
on the slides of ten calibrated fields that were
ran-domly selected (Leica, DM750, 40×), to determine the
countsofimmunoreactivecellstoeotaxin-1andeosinophils per squared millimeter, usingrabbit monoclonal antibody
chemokine(C Cmotif)ligand11(EotaxinEPR5825;
Gene-Tex Irving, CA, USA) and mouse monoclonal antibodies
(mouse mayorbasic proteinBMK13, 1:25;Chemicon
Inter-national,Temecula,CA,USA)respectively.
Statisticalanalysis
AfterKolmogorovSmirnovtest,statisticalanalysiswas per-formedaccordingtodatadistributionusingttest,Pearson’s correlationcoefficientandAnalysisofCovariance,valuesof p≤0.05wereconsideredsignificant.
Results
Clinicalcharacteristicsofthepatients
Thegeneralcharacteristicsofthepatientsaredescribedin
Table1.Amongthepatientswithexposuretotobaccosmoke
(Group I),21patients reportedonly passiveexposure and onepatientreportedboth,passiveandactiveexposure.In thetwogroups,thenumberofpositiveallergensduringprick testing(AllerStand,MexicoCity;IRCguidelines,1994)was from1to13(median3)andthemostfrequentallergenwas
Dermatophagoidessp.(40%inGroupIvs.50%inGroupII). The frequency and severity of the nasal symptoms is described in Table 1. There was no difference between groups either on the frequency of each symptom or the totalscore(median6,inthe2Groups).Themostfrequent symptomwasrhinorrhea,whichwasreportedby95%ofthe patientsinthetwogroups.
Immunoreactivecellcountsofeotaxin-1andeosinophils
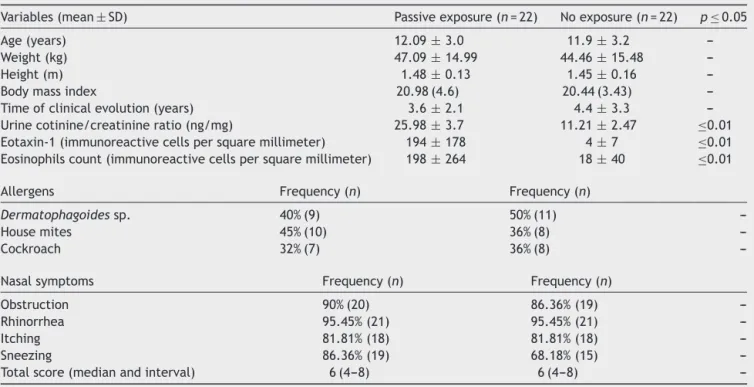
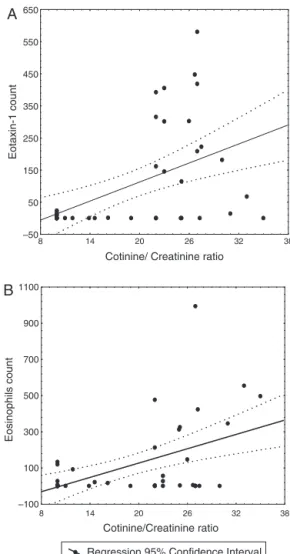
Patients with exposure to tobacco cigarette smoke had highercounts ofimmunoreactive cellsinthenasalmucosa for both eotaxin-1 and eosinophils than patients with no exposure(tStudent,p<0.05) (Table1).Although thetwo variables showednolinear relationship between them,in the whole group, the cell counts of both eotaxine-1 and eosinophils were related to the urine cotinine/creatinine ratio (Pearson’s r=0.51 and 0.50 respectively, p<0.001) (Fig.1).
Analysis of Covariance showed that the relationship between the cell count of eotaxin-1 and the urine coti-nine/creatinine ratio was independent fromthe age, the genderandthebodymassindexofthepatients(p>0.05), whiletherelationshipbetweenthecellcountofeosinophils andtheurinecotinine/creatinine ratiowasrelatedtothe age(ˇ=−0.6,95%CI0.89---0.31)andtothebodymassindex
(ˇ=0.44,95%CI0.15---0.74)(wholemodelR=0.7,p<0.001).
Discussion
The results of this study show evidence that compared to children and teenagers with no exposure to tobacco cigarette smoke, those with perennial allergic rhinitis
A
Cotinine/ Creatinine ratio
Eotaxin-1 count
–50 50 150 250 350 450 550 650
38 32 26 20 14 8
Regression 95% Confidence Interval
B
Cotinine/Creatinine ratio
Eosinophils count
–100 100 300 500 700 900 1100
38 32 26 20 14 8
Figure 1 Linear relationship between the urine coti-nine/creatinineratioand(A)thecountofimmunoreactivecells to eotaxin-1 and (B) the count of eosinophils, in the nasal mucosaof44patientswithperennialallergicrhinitis.
whowere exposedto tobaccosmoke mayhave increased immunoreactivecell counts intheir nasalmucosa toboth eotaxin-1andeosinophils,whicharerelatedtotheirurine cotinine/creatinineratio.
Inanimal modelsandhumans,several effectsof
expo-sure to tobacco smoke on the immune response have
been described,21---24 including modified blood counts of
eosinophils and monocytes.25 However, thereis a lack of
studies assessing the effect of tobacco smoke exposure on eotaxin-1 in patients with allergic rhinitis. This study shows that even passive exposure totobacco smoke may increase immunoreactive cell counts to eotaxin-1 in the nasalmucosa,whicharelinearly relatedtotheexposure. Then,inpatientswithallergicrhinitis,assessmentand con-trolof the exposure totobaccosmoke may contribute to preventfurtherdamagetothenasalmucosa.
T helper type 2 lymphocytes.4---6 Then, CCR3-eotaxin are
expressednotonlyincellsimplicatedinactivationor migra-tionofeosinophilsbutalsoinvariousothercellsinvolvedin allergicinflammation.26,27
The relationship between the countof eosinophils and the body mass index, observed in the whole group of patients,is in agreementwithprevious reports showinga proportionalrelationshipbetweenthebodymassindexand allergicdiseasesoftheairways.15,28,29Althoughfurther
stud-iesareneededtounderstanditsmeaning.
Thefindingofasimilarfrequency/severityofnasal symp-toms in patients with allergic rhinitis exposed or not to tobaccosmoke,mighthavebeenrelatedtotheageofthe participants.Evidencesupportthatchildrenandteenagers withperennialrhinitis frequentlyunder-reporttheirnasal symptoms.30,31Additionally,thestudysettingmayhavebeen
a confounder; all participants were living in one of the most polluted cities in the world. Since the two groups weresimilarlyexposedtopollution,theywerecomparable, butenvironmental factors mayhave interfered withtheir symptoms. Several between- and within-country associa-tionsbetweenenvironmentalfactorsandpersistentrhinitis symptomprevalencehavebeenreported.32,33InPeru34and
in Brazil,35 higher current asthma and rhinitis symptoms
havebeenobservedinurbanteenagersascomparedtothose livinginruralvillages.
Evidencesupportsthat sexhormonesarelikelytoplay animportantroleinthedevelopmentandoutcomeofthe allergic immune response.36 Although, this study wasnot
designed to explore it, the similar age and male/female ratioofthetwogroupsallowedcomparisonsbetweenthem, whilecontrollingforapossibleinfluenceofthesefactorson theresults.
Themainlimitationsofthisstudyarethedesignandthe samplesize.Thecross-sectionaldesignpreventustodiscuss anycausalrelationship;andthesamplesizeallowedusto identifyonly themost evident differences, without deny-ingotherpossiblerelationshipsamongthevariablesofthe study.Although, theselectioncriteriawereusefulto con-troltheinfluenceofthemainconfounders(likeconcurrent inflammatorydiseasesandimmunotherapy),apossible influ-enceontheresultsofotherpotentialconfounders,likefood intake and the respiratory exposure to other substances, cannotbeexcluded.
Conclusion
Exposuretotobaccocigarettesmokecanincreaseeotaxin-1 andthecountofeosinophils inthenasalmucosaofyoung patientswithperennialallergicrhinitis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KariyawasamHH,RobinsonDS.Theeosinophil:thecellandits weapons,thecytokines,itslocations.SeminRespirCritCare Med.2006;27:117---27.
2.TeranLM,Rojas-RamosE,AvalosAF,Perez-FernandezL,Cuevas F. The chemokines RANTES, MCP-3, MCP-4, eotaxin-1 and eotaxin-2 are associated with eosinophil recruitment into the airways of asthmatic children. J Allergy Clin Immunol. 2002;109:S36.
3.Semik-Orzech A, Barczyk A, Wiaderkiewicz R, Pierzchała W. Eotaxin,butnotIL-8,isincreasedinupperandlowerairwaysof allergicrhinitissubjectsafternasalallergenchallenge.Allergy AsthmaProc.2011;32:230---8.
4.SallustoF,MackayCR,LanzavecchiaA.Selectiveexpressionof theeotaxinreceptorCCR3byhumanThelper2cells.Science. 1997;277:2005---7.
5.Heinemann A, HartnellA, Stubbs VE, MurakamiK, Soler D, LaRosaG, et al.Basophil responsestochemokinesare regu-latedbybothsequentialandcooperativereceptorsignaling.J Immunol.2000;165:7224---33.
6.JuremalmM,NilssonG.Chemokinereceptorexpressionbymast cells.ChemImmunolAllergy.2005;87:130---44.
7.LusterAD.Antichemokineimmunotherapyforallergicdiseases. CurrOpinAllergyClinImmunol.2001;1:561---7.
8.ElsnerJ,EscherSE,ForssmannU.Chemokinereceptor antago-nists:anoveltherapeuticapproachinallergicdiseases.Allergy. 2004;59:1243---58.
9.AsherMI,MontefortS,BjörksténB,LaiCK,StrachanDP, Wei-land SK, et al. Worldwide time trends inthe prevalence of symptomsofasthma,allergicrhinoconjunctivitis,andeczema inchildhood:ISAACPhasesOneandThreerepeatmulticountry cross-sectionalsurveys.Lancet.2006;368:733---43.
10.TeradaN,HamanoN,KimWJ,HiraiK,NakajimaT,YamadaH, etal.The kineticsofallergen-inducedeotaxinlevelinnasal lavage fluid: its key role in eosinophil recruitment in nasal mucosa.AmJRespirCritCareMed.2001;164:575---9.
11.Salib RJ, Lau LC, Howarth PH. Nasal lavage fluid concen-trations of eotaxin-1 (CCL11) in naturally occurring allergic rhinitis:relationshiptodiseaseactivity,nasalluminaleosinophil influx,andplasmaproteinexudation.ClinExpAllergy.2005;35: 995---1002.
12.Seymour BWP, Pinkerton KE, Friebertshauser KE, Coffman RL, Gershwin LJ. Second-hand smoke is an adjuvant for T-helper-2responsesina murinemodel ofallergy.JImmunol. 1997;159:6169---75.
13.RumoldR,JyralaM,Diaz-SanchezD.Secondhandsmokeinduces allergicsensitizationinmice.JImmunol.2001;167:4765---70. 14.Vinke JG, KleinJan A, Severijnen WFM, Fokkens WJ.
Pas-sivesmoking causesan‘‘allergic’’cell infiltrateinthenasal mucosaofnon-atopicchildren.IntJPediatrOtorhinolaryngol. 1999;51:73---81.
15.Monta˜no-VelázquezBB,CampilloNavarreteR,GarciaF,Mogica MartínezMD,Becerril-ÁngelesM,Jáuregui-RenaudK.Influence ofexposuretotobaccocigarettesmokeontheeosinophilcount onthenasalmucosainyoungpatientswithperennialallergic rhinitis.Rhinology.2013;51:253---8.
16.Krisiukeniene A, Babusyte A, Stravinskaite K, Lotvall J, SakalauskasR,SitkauskieneB.Smokingaffectseotaxinlevels inasthmapatients.JAsthma.2009;46:470---6.
17.WarrenCW,JonesNR,PerugaA,ChauvinJ,BaptisteJP,Costa deSilvaV,etal. CentresforDiseaseControl and Prevention (CDC). Global youth tobacco surveillance, 2000---2007. Morb MortalWklyRepSurveillSumm.2008;57:1---28.
18.OlivieriM,BodiniA,PeroniDG,CostellaS,PacificiR, Piacen-tiniGL, et al.Passive smoking inasthmatic children.Effect ofa‘‘smoke-freehouse’’measuredbyurinarycotininelevels. AllergyAsthmaProc.2006;27:350---3.
20.Monta˜no-VelazquezBB,Jáuregui-RenaudK,CampilloNavarrete MR,MojicaMartinezM, RuizHinojosaA, BecerrilAngeles M. Evaluationofaquestionnaireformeasuringnasalsymptomsin subjectswithallergicrhinitis.RevAlergMex.2003;50:17---21. 21.KalraR,SinghSP,SavageSM,FinchGL,SoporiML.Effectsof
cigarettesmokeontheimmuneresponse:chronicexposureto cigarettesmokeimpairsantigen-mediatedsignalinginTcells anddepletesIP3-sensitivecalciumstores.JPharmacolExpTher. 2000;293:166---71.
22.MatsumotoK,AizawaH,InoueH,KotoH,TakataS,ShigyoM, etal. Eosinophilic airway inflammationinduced byrepeated exposuretocigarettesmoke.EurRespirJ.1998;12:387---94. 23.MioT,RombergerDJ,ThompsonAB,RobbinsRA,HeiresA,
Ren-nard SI. Cigarette smoke induces interleukin-8 release from humanbronchialepithelial cells.AmJRespirCritCareMed. 1997;155:1770---6.
24.SoporiML,KozakW,SavageSM,GengY,KlugerMJ. Nicotine-induced modulation of T cell function. Implications for inflammation and infection. Adv Exp Med Biol. 1998;437: 279---89.
25.JensenEJ,PedersenB,NarvestadtE,DahlR.Bloodeosinophil andmonocytecountsarerelatedtosmokingandlungfunction. RespirMed.1998;92:63---9.
26.OyamadaH,KamadaY,KuwasakiT,YamadaY,KobayashiY,Cui C,etal.CCR3mRNAexpressioninbronchialepithelialcellsand variouscellsinallergicinflammation.IntArchAllergyImmunol. 1999;120Suppl.1:45---7.
27.GerberBO,Zanni MP,UguccioniM,Loetscher M,MackayCR, PichlerWJ,etal.Functionalexpressionoftheeotaxinreceptor CCR3inTlymphocytesco-localizingwitheosinophils.CurrBiol. 1997;7:836---43.
28.BråbäckL, Hjern A, Rasmussen F.Body mass index, asthma andallergicrhinoconjunctivitisinSwedishconscripts-anational cohortstudyoverthreedecades.RespirMed.2005;99:1010---4.
29.WeinmayrG,ForastiereF,BücheleG,JaenschA,StrachanDP, NagelG,etal.Overweight/obesityandrespiratoryandallergic diseaseinchildren:internationalstudyofasthmaandallergies inchildhood(ISAAC)phasetwo.PLOSONE.2014;9:e113996. 30.Priftisa KN, Drigopoulosb K, Sakalidoua A, Trigaa M, Kallisb
V, Nicolaidouc P. Subjective and objective nasal obstruction assessmentinchildrenwithchronicrhinitis.IntJPediatr Otorhi-nolaryngol.2006;70:501---5.
31.Monta˜no-Velázquez BB, Navarrete RC, Mogica Martínez MD, Becerril-Ángeles M, Jáuregui-Renaud K. Rhinomanom-etry in young patients with perennial allergic rhinitis with/without recent exposure to tobacco smoke. Clin Otolaryngol.2011;36:320---4.
32.FuertesE,ButlandBK,RossAndersonH,CarlstenC,Strachan DP,BrauerM,etal.Childhoodintermittentandpersistent rhini-tisprevalenceand climate andvegetation: aglobal ecologic analysis.AnnAllergyAsthmaImmunol.2014;113:386---92. 33.D’AmatoG,HolgateST,PawankarR,LedfordDK,CecchiL,
Al-AhmadM,etal.Meteorologicalconditions,climatechange,new emergingfactors,andasthmaand relatedallergicdisorders. AstatementoftheWorldAllergyOrganization.WorldAllergy Organ.2015;14,8:25.eCollection2015.
34.RobinsonCL,BaumannLM,GilmanRH,RomeroK,CombeJM, CabreraL,etal.Effectofurbanisationonasthma,allergyand airwaysinflammationinadevelopingcountrysetting.Thorax. 2011;66:1051---7.
35.Solé D, Cassol VE, Silva AR, Teche SP, Rizzato TM, Bandim LC, et al. Prevalence of symptoms of asthma, rhinitis, and atopiceczemaamongadolescentslivinginurbanandruralareas indifferent regions ofBrazil.Allergol Immunopathol(Madr). 2007;35:248---53.