www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Acoustic
rhinometry
in
mouth
breathing
patients:
a
systematic
review
夽
,
夽夽
Ana
Carolina
Cardoso
de
Melo
a,∗,
Adriana
de
Oliveira
de
Camargo
Gomes
b,c,
Arlene
Santos
Cavalcanti
c,
Hilton
Justino
da
Silva
caHumanCommunicationHealth,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
bHospitaldeReabilitac¸ãodeAnomaliasCraniofaciais,UniversidadedeSãoPaulo(HRAC-USP),SãoPaulo,SP,Brazil
cUniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received10May2014;accepted1August2014 Availableonline29December2014
KEYWORDS
Acousticrhinometry; Mouthbreathing; Diagnosis; Nasalcavity
Abstract
Introduction:Whenthereisachangeinthephysiologicalpatternofnasalbreathing,mouth breathingmayalreadybepresent.Thediagnosisofmouthbreathingisrelatedtonasalpatency. Onewaytoaccessnasalpatencyisbyacousticrhinometry.
Objective:Tosystematicallyreviewtheeffectivenessofacousticrhinometryforthediagnosis ofpatientswithmouthbreathing.
Methods:ElectronicdatabasesLILACS,MEDLINEviaPubMedandBireme,SciELO,Webof Sci-ence,Scopus, PsycInfo, CINAHL, and Science Direct, fromAugust to December 2013, were consulted.11,439articleswerefound:30fromLILACS,54fromMEDLINEviaBireme,5558from MEDLINEviaPubMed,11fromSciELO,2056fromWebofScience,1734fromScopus,13from PsycInfo,1108fromCINAHL,and875fromScienceDirect.Ofthese,twoarticleswereselected. Results:Theheterogeneityintheuseofequipmentandmaterialsfortheassessmentof respi-ratorymode inthesestudiesrevealsthatthereisnotyet consensusintheassessmentand diagnosisofpatientswithmouthbreathing.
Conclusion:Accordingtothearticles,acousticrhinometryhasbeenused foralmosttwenty years, but controlled studies attestingto the efficacy of measuring the geometryof nasal cavitiesforcomplementarydiagnosisofrespiratorymodearewarranted.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:deMeloAC,GomesAO,CavalcantiAS, daSilvaHJ.Acousticrhinometry inmouthbreathingpatients:a
systematicreview.BrazJOtorhinolaryngol.2015;81:212---8.
夽夽
Institution:UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil. ∗Correspondingauthor.
E-mail:[email protected](A.C.CardosodeMelo).
http://dx.doi.org/10.1016/j.bjorl.2014.12.007
PALAVRAS-CHAVE
Rinometriaacústica; Respirac¸ãobucal; Diagnóstico; Cavidadenasal
Ousodarinometriaacústicaemrespirac¸ãooral:revisãosistemática
Resumo
Introduc¸ão: Quandoháalterac¸ãonopadrãorespiratórionasalfisiológico,arespirac¸ãooralde suplênciajápodeestarpresente.Odiagnósticodarespirac¸ãooralvincula-seàpermeabilidade nasal.Umadaspossibilidadesparaavaliac¸ãodapermeabilidadenasaléarinometriaacústica. Objetivo: Revisar,deformasistemática,aeficáciadarinometriaacústicanoauxíliodiagnóstico depacientescomrespirac¸ãooral.
Método: ForamconsultadasasbasesdedadoseletrônicasLILACS,MEDLINEviaBiremeevia PUBMED,SciELO,WebofScience,Scopus,PsycInfo,CINAHLeScienceDirect,deagostoa dezem-brode2013.Foramencontrados11.439artigos,sendo30daLILACS,54daMEDLINEviaBireme, 5.558daMEDLINE viaPubmed,11daScielo,2.056daWebofScience,1.734daScopus,13da PyscInfo,1.108daCINAHLe875ScienceDirect.Desses,foramselecionadosdoisartigos. Resultados: Aheterogeneidadenousodosequipamentosemateriaisutilizadosparaaavaliac¸ão do modo respiratórionesses estudos mostra queainda não háum consenso naavaliac¸ãoe diagnósticodeindivíduoscomrespirac¸ãooral.
Conclusão:Deacordocomosartigos,arinometriaacústicaéutilizadaháquasevinteanos, porémsãonecessáriosestudoscontroladosqueatestemaeficáciadamensurac¸ãodageometria dascavidadesnasaiscomoauxíliodiagnósticodomodorespiratório.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Nasalbreathingplaysanimportantroleinvitalbody func-tions, suchas airfiltration, heating andhumidification of inspiredair,afirstdefensebarrieragainstinhaledallergens, and protection of the paranasalsinuses, earcavities and lowerairways;asitsprimaryfunction,nasalbreathing pre-parestheairforitsoptimalutilizationinthelungs.1---3When
apersonisunabletousehis/hernasalairways,changesin physiologicalnasalbreathingpatternwilloccurand, there-after,mouthbreathingensues.4
However,theliteratureexhibitsconflictindefiningwhat is considered normalbreathing through the nose, aswell asinobjectivelyidentifyingnasalobstruction.5,6Moreover,
althoughthediagnosisofmouthbreathingisrelatedtonasal obstruction,thissituationisnotalwaysthecase,especially whenoralbreathingmodehasbecomechronic.
Fordecades,specifictestsforevaluationofnasal perme-abilityhave beenusedin ordertoquantifythesubjective symptomofnasalobstruction.5
The Altman graph mirror, for example, is one of the instrumentsusedinclinicalpracticetoassessnasalpatency. Itsmetalplatehasasmoothside,andtheothersideshows millimetermarkings,allowingforaprecisemeasurementof the areamarked by thenasal exhalation,7 comparing the
condensationareabetweenthenasalcavities.8
However,acousticrhinometryisoneofthenewest meth-odsforstaticallymeasuringdifferentsegmentsofthenasal cavity, fromthenostrilstothechoanae, quicklyand non-invasively,and‘requiringlittlepatientcooperation.9,10The
technique is based on the analysis of the nasal cavity’s reflected sound from incident sound waves, taking into accountthepropertiesofthissoundinrelationtothe inten-sityandarrivaltimeoftheecho.9Therefore,thistechnique
enablesthemeasurementofthedistancescorrespondingto the cross-sectional areas, usually of the nasal valvearea andthefrontandrearareasof theconchae,andthe cal-culationofnasalvolumes,allowingtheidentificationofthe lociofconstrictionsthatcontributetonasalresistance11,12
thusprovidingtopographicalinformationontheindividual profileofthenasalandnasopharyngealairways.13
Itsreproducibilityandaccuracywereconfirmedby sev-eral authors,14---18 the procedures are standardized and
showntobereliable,11,19---22andresearchonreferencevalues
inadultsandchildrenhavealsobeenreported.12,23---27
Thetechniqueisalsousedbyseveralauthorstoestimate nasalairwayobstruction indifferentetiologies, aswell as the effectof distinct pathologies and surgical and ortho-pedicprocedures onnasal and nasopharyngeal cavities in pediatricandadultpopulations.18,28---37
Theclinicalvalueofacousticrhinometryrestsinits abil-ity to measure nasal geometry, thus being an important toolfortheclinicalrhinologicalfollow-up,9,38,39allowingfor
thediscriminationbetweenmucosalfunctionaleffectsand structuralchangesrelatedtonasalobstruction,whenused intestsbeforeandaftertreatmentwithavasoconstrictor.39
Although thetest does notprovide anetiological diag-nosis of nasal obstruction, it quantifies the magnitude of theobstructivesymptom at any giventime,and is there-foreconsideredaspecifictestintheinvestigationofnasal patency,5,21,40complementarytoclinicalexamination.
Giventheimportanceofnasalpatencyforthe establish-ment of a physiological nasal breathing and the negative impact of nasal obstruction on stomatognathic system functions,41includingspeech/articulation,thisarticleaims
Table1 Searchstrategiesfordatabase(MeSHandMeSH)survey.
CrossingsinEnglish CrossingsinSpanish CrossingsinPortuguese
‘‘Acousticrhinometry’’and ‘‘mouthbreathing’’
‘‘Rinometríaacústica’’and ‘‘Respiraciónporlaboca’’
‘‘Rinometriaacústica’’and ‘‘Respirac¸ãobucal’’ ‘‘Acousticrhinometry’’and
‘‘diagnosis’’
‘‘Rinometríaacústica’’and ‘‘Diagnóstico’’
‘‘Rinometriaacústica’’and ‘‘Diagnóstico’’
‘‘Diagnosis’’and‘‘mouth breathing’’
‘‘Diagnóstico’’and ‘‘Respiraciónporlaboca’’
‘‘Diagnóstico’’and ‘‘Respirac¸ãobucal’’ ‘‘Nasalcavity’’and‘‘mouth
breathing’’
‘‘Cavidadnasal’’and ‘‘Respiraciónporlaboca’’
‘‘Cavidadenasal’’and ‘‘Respirac¸ãobucal’’ ‘‘Nasalcavity’’and
‘‘diagnosis’’
‘‘Cavidadnasal’’and ‘‘Diagnóstico’’
‘‘Cavidadenasal’’and ‘‘Diagnóstico’’ ‘‘Nasalcavity’’and
‘‘acousticrhinometry’’
‘‘Cavidadnasal’’and ‘‘Rinometríaacústica’’
‘‘Cavidadenasal’’and Rinometriaacústica’’
Methods
Asystematicliteraturereviewwasperformedfromthe fol-lowingdatabases:LILACSviaMEDLINE,MEDLINEviaBireme, MEDLINE via PubMed, SciELO, Web of Science, Scopus, PsycInfo, CINAHL, and Science Direct. The data search occurredfromAugusttoDecember2013.Tothis investiga-tion,descriptorsandcrossingsusedareshowninTable1.
The search was conducted by two researchers inde-pendently,followingcriteriaofinclusionandexclusion.As inclusioncriteria,originalarticles(whosemanuscriptswere publishedinanylanguage)addressingtheeffectivenessof theinstrumentofacousticrhinometryintheevaluationof oralbreathingwereselected.
Literaturereviewarticlesandeditorialswereexcluded, aswellasthosepaperswithnowordsreferringtothesubject discussedinthisreview,thosethatdidnotusethe instru-mentofacousticrhinometryasacomplementarydiagnostic, andstudiesonanimals.
The methodological characteristics of articles were addressed according toinclusion criteria, statistical anal-ysis and statistical comparison between selected groups (Table2).
Results
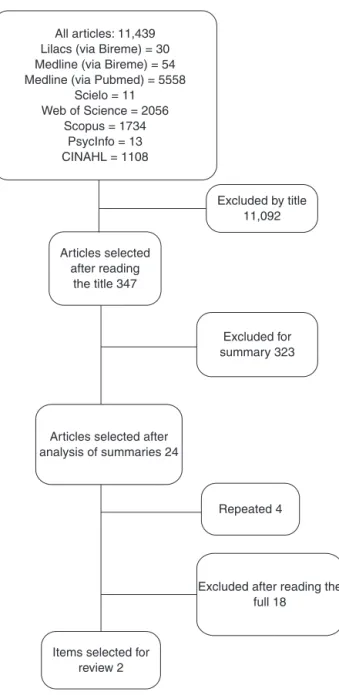
Wecanobserveintheflowchartthenumberofitemsfound andselectedafterapplyingourinclusionandexclusion crite-ria,accordingtodescriptorsanddatabases(Fig.1).
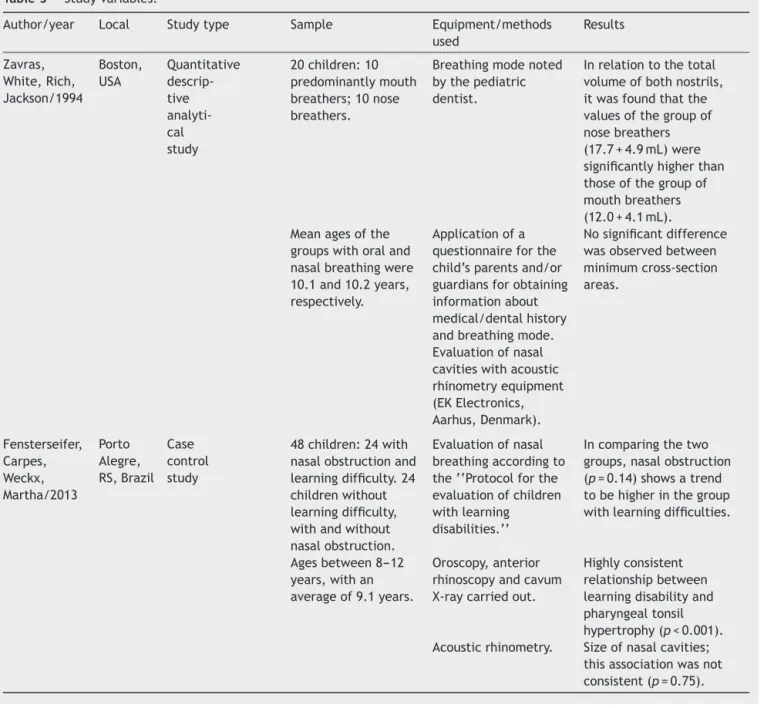
To better present the results and to cover the pro-posedobjectives,itwasdecidedtoconsiderthefollowing variables of the selected articles: author/year, location, typeofstudy,sample,equipment/methodsusedandresults (Table3).
Discussion
In the twentieth XIX, specifically in 1977, Jackson et al. developed studies on the acoustic reflex technique with theaimtocalculatecross-sectionalareasoftrachea, phar-ynxandsupraglotticregion.42 Onlyin1989,Hilbergetal.9
introducedthemethodofrhinometryasanacoustic reflec-tionmethod,adaptedtonasalcavities.Suchamethodcan bedefinedasanobjectiveassessmentofnasalpatency(or permeability),basedonthereflectionofasoundwaveand offering information on the dimensions and geometry of nasalcavity.11,12,27,43
The use of this technique in the evaluation of mouth breathers has been maturing over the last twenty years. Inthisinvestigation,wefoundtwoarticlesthataddressed theproposedthemeandperceivedheterogeneitybetween these papers, with respect to the authors and publica-tion periods. In the manuscripts included in our study, the beginning of the use of acousticreflection technique for breathing-mode evaluation and characterization was observed,followinganintervalofalmosttwodecadestothe applicabilityofthissame technique.Fromthepaper pub-lishedin1994totheyear2013,44,45nostudiesdepictingthe
useof acousticrhinometryasa complementaryprocedure forthediagnosisofmouthbreathingwerepublished.
Table2 Methodologicalclassificationofselectedarticles.
Articlesand criteria
Zavrasetal. (1994)
Fensterseifer etal.(2013)
1.Specified inclusion criteria
Yes Yes
2.Controlgroup Yes Yes 3.Random
allocation
No No
4.Confidentiality inallocation
No No
5.‘‘Blind’’ subjects
No No
6.‘‘Blind’’ therapists
No No
7.Statistical analysis
Yes Yes
8.Statistical comparison betweengroups
Table3 Studyvariables.
Author/year Local Studytype Sample Equipment/methods used
Results
Zavras, White,Rich, Jackson/1994
Boston, USA
Quantitative descrip-tive analyti-cal study
20children:10 predominantlymouth breathers;10nose breathers.
Breathingmodenoted bythepediatric dentist.
Inrelationtothetotal volumeofbothnostrils, itwasfoundthatthe valuesofthegroupof nosebreathers (17.7+4.9mL)were significantlyhigherthan thoseofthegroupof mouthbreathers (12.0+4.1mL). Meanagesofthe
groupswithoraland nasalbreathingwere 10.1and10.2years, respectively.
Applicationofa questionnaireforthe child’sparentsand/or guardiansforobtaining informationabout medical/dentalhistory andbreathingmode.
Nosignificantdifference wasobservedbetween minimumcross-section areas.
Evaluationofnasal cavitieswithacoustic rhinometryequipment (EKElectronics, Aarhus,Denmark).
Fensterseifer, Carpes, Weckx, Martha/2013
Porto Alegre, RS,Brazil
Case control study
48children:24with nasalobstructionand learningdifficulty.24 childrenwithout learningdifficulty, withandwithout nasalobstruction.
Evaluationofnasal breathingaccordingto the‘‘Protocolforthe evaluationofchildren withlearning disabilities.’’
Incomparingthetwo groups,nasalobstruction (p=0.14)showsatrend tobehigherinthegroup withlearningdifficulties.
Agesbetween8---12 years,withan averageof9.1years.
Oroscopy,anterior rhinoscopyandcavum X-raycarriedout.
Highlyconsistent relationshipbetween learningdisabilityand pharyngealtonsil hypertrophy(p<0.001). Acousticrhinometry. Sizeofnasalcavities;
thisassociationwasnot consistent(p=0.75).
The objective assessment of nasal permeability in patients with nasal obstruction has been developed with theuseoftheacousticreflectionmethod,through investi-gationsinpopulationswithallergicrhinitis,hypertrophyof palatine tonsilsand recurrent respiratoryinfections.1,46---48
Mouthbreathinghasbeen underlinedinpublicationsusing acousticrhinometry,asaconsequenceofnasalobstruction. Duetothisfact,wefound largegapsbetweenthestudies hereevaluated.
With respect to the origin, the manuscripts included in this review are from North America (Boston, United States)andSouthAmerica(PortoAlegre,Brazil).44,45
How-ever,thelastUSpublicationontheproposedissueoccurred in1994,showingthattheuseofacousticrhinometry equip-ment in Brazil continues in its update process in a wide range of populations, including the assessment and diag-nosis of oral breathing. In the included manuscripts, we
observesimilarities regarding the type of study, in which theypresentspecifiedinclusioncriteria,presenceofa con-trol group, statistical analysis and statistical comparison between groups. These manuscripts are characterized as quantitative,descriptiveanalyticalstudy,43andascase
con-trolstudy.45
Thesamplingprocedureisarelevantaspectunderlinedin themanuscripts,andrevealedasimilarityinthesmall num-berofsubjectsinthefirstarticle(20;10in eachgroup)44
versusaslightlymorethantwice(48;24ineachgroup)the numberof subjects in the second article.45 It is assumed
that the small numbers of individuals presented in these studiesmaycompromisethereproducibilityofthefindings forthegeneralpopulation.Inthemanuscripts,the partic-ipants’age is alsosimilar: children between eightand12 yearswithanapproximatemeansof9.145and10.1years.44
All articles: 11,439 Lilacs (via Bireme) = 30 Medline (via Bireme) = 54 Medline (via Pubmed) = 5558
Scielo = 11 Web of Science = 2056
Scopus = 1734 PsycInfo = 13 CINAHL = 1108
Excluded by title 11,092
Articles selected after reading
the title 347
Excluded for summary 323
Articles selected after analysis of summaries 24
Repeated 4
Excluded after reading the full 18
Items selected for review 2
Figure1 Flowchart:numberofarticlesfound.
withpediatricpopulations,bothformeanageandnumber ofparticipants.31,48,49
In studies evaluating surgical procedures for nasal obstruction,acousticrhinometryisusedtoquantifythe suc-cessof thesesurgeries. Consideringthat this is amethod availablewhichprovidesthegeometricmeasureofthenasal cavitybymeansofareflectedacousticsignal,itsresultis awavecalled rhinogram, which hasthetypical formofa ‘‘W’’.Thus, this methodprovidessome parameters,such astheminimumcross-sectionalarea(regionofhigher resis-tancetoairflow)andvolumeatspecificsegments.31,49,50
Anotherimportantaspect ishowthesampleisdivided. Inbotharticlesincludedinthisreviewthereisadivisionof twosamplegroups:agroupofmouthbreathersandanother predominantlywithnosebreathers.Thestatistical compar-isonbetween groups44,45 shows the homogeneity of these
variablesinourselectedstudies.Thisisconsistentwith stud-iesusing the samemethodology tocompare groups, with
predominanceofpublicationsstudyingallergicrhinitis popu-lationsandcontrolgroups.41,48
Inbothmanuscriptsincludedinthisreview,themethod ofacousticrhinometrytoevaluateoralbreathingwasused. Zavras et al.44 used an EK Electronics (Aarhus, Denmark)
acoustic rhinometer. This was an observational clinical evaluationof respiratorymodebyapediatric dentist, fol-lowed by a questionnaire given to relatives/carers. On the other hand, the Fenterseifer et al.45 did not specify
whichrhinometricequipmentwasused;ontheotherhand, these authors performed ENT tests of oroscopy, anterior rhinoscopyandcavumX-ray,inadditiontotheclinical eval-uation of respiratory mode through the Protocol for the AssessmentofChildrenwithLearningDisabilities.
Differencesintheuseofequipmentandinmaterialsfor breathingmodeevaluationbetweenstudieswereobserved, showing that there has not yet been consensus on the assessmentanddiagnosisofmouthbreathers.Moreover,our analysisshows thelimitednumber ofpublications demon-stratingtheuseofadevicethataimstomeasurethenasal cavityarea---averyimportantresourceasacomplementary procedureforthediagnosisofpatients’respiratorymode.
The articles in this review were statistically analyzed usingthesamestatisticaltestforindependentsamples.In thestudy publishedin 1994,44 a dataanalysiswascarried
outwiththepairedt-testforindependentsamples;withthis test,intheanalysisofthetotalvolumeofbothnostrils,it wasfoundthatthevaluesofgroupB---predominantlywith nasal breathers (17.7+4.9mL) --- were significantly higher than those obtained for Group A --- with mouth breathers (12.0+4.1mL).Ontheotherhand,theSpearmancorrelation testusedfortheanalysisbetweennasalcavitiesshowed sig-nificantcorrelationsbetweenminimumareaofeachnostril andthecorrespondingvolumeofthenostrilbeinganalyzed. However,thestudypublishedin201345reportedthatinthe
evaluation of nasalcavity volumeby acousticrhinometry, theresultsshowednoconsistentrelationshipinthe compar-isonbetweenthetwogroupsstudiedwithrespecttothesum ofthemeanvolumeofnasalcavities(p=0.75).Ingeneral, theselectedstudiesshowthatadecreaseinnasalgeometry occursinmouth breathingchildren. Wecaninferthatthe absenceofmoresignificantstatisticdatacouldberelated tothesmallnumberofsubjectsinthesestudies.
Despitenotbeingdirectedtooralbreathing,astudyof 101 subjectsdemonstratedsignificant differencesin nasal geometry,volumeandminimalcross-sectionalareabetween groupswithdifferentdegrees(mild,moderateandsevere) ofnasalobstruction.47 Thisfindingshowsthatthestudyof
a greater number of subjects results in better significant differences.
Theseresultsindicatetheneedformoredetailedstudies inthepopulation ofmouthbreathers,withinvestments in objectiveandquantitativemethods,aswellasin standard-izedtests.
Conclusion
breathers,ithasnotyetbeenpossibletodemonstrate sci-entifically and clinically this decrease, compared tonose breathers.Accordingtothearticlesinvestigated,this tech-nique has already been applied for almost twenty years, butcontrolledstudiesattestingtotheefficacyofmeasuring the areaof nasalcavities for complementarydiagnosis of respiratorymodeareneeded.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TrindadeIEK,ConegliamPCP,TrindadeSHK,DiasNH, Sampaio-TeixeiraACM. Internal nasal dimensionsof adultswithnasal obstruction.BrazJOtorhinolaryngol.2013;79:575---81. 2.Ferreira ML. A incidência de respiradores bucais em
indi-víduos com oclusão classe II. J Bras Ortodon Ortop Facial. 1999;4:223---40.
3.DiFrancescoRC.Respiradorbucal:avisãodo otorrinolaringol-ogista.JBrasOrtodonOrtopFacial.1999;4:241---7.
4.CópioFC[dissertac¸ão]Acapacidadefuncionaldacrianc¸a respi-radoraoralavaliadapelotestedecaminhadadeseisminutos. BeloHorizonte, MG:Faculdadede Medicina da Universidade FederaldeMinasGerais;2008.
5.RoithmannR.Testesespecíficosdapermeabilidadenasal.Braz JOtorhinolaryngol.2007;73:2.
6.BaraniukJ.Subjectivenasalfullnessandobjectivecongestion. ProcAmThoracSoc.2011;8:62---9.
7.Cunha DA, Silva HJ, Moraes KJR, Cunha RA, Régis RMFL, SilvaEGF. Aerac¸ão nasal em crianc¸as asmáticas. RevCEFAC. 2011;13:783---9.
8.BrecvoviciS,RoithmannR.Areprodutibilidadedoespelhode glatzelmodificadonaaferic¸ãodapermeabilidadenasal.BrazJ Otorhinolaryngol.2008;74:215---22.
9.HilbergO,JacksonAC,SwiftDL,PedersenOF.Acoustic rhinom-etry:evaluationofnasalcavitygeometrybyacousticreflection. JApplPhycol.1989;66:295---303.
10.DjupeslandP,PedersenOF.Acousticrhinometryininfantsand children.RhinolSuppl.2000;16:52---8.
11.HilbergO.Objectivemeasurementofnasalairwaydimensions usingacousticrhinometry:methodologicalandclinicalaspects. Allergy.2002;57Suppl.70:5---39.
12.TrindadeIEK,GomesAOC,Sampaio-TeixeiraACM,TrindadeSHK. Adultnasal volumesassessed byacousticrhinometry. Braz J Otorhinolaryngol(EnglEd).2007;73:32---9.
13.KunkelM,WahlmannU,WagnerW.Nasalairwayincleft-palate patients: acoustic rhinometric data. J Cranio-Max Fac Surg. 1997;25:270---4.
14.Wilson AM, Fowler SJ, Martin SW, White PS, Gardiner Q, Lipworth BJ. Evaluation of the importance of head and probestabilisationinacousticrhinometry.Rhinology.2001;39: 93---7.
15.FonsecaMJ,GotoEY,NigroCEN,RochaFM, Mello JuniorJF, VoegelsRL. Reprodutibilidade erepetibilidadedarinometria acústica.ArqOtorrinolaringol.2003;7:213---8.
16.OuriquesDM,CarliniD,FujitaR,Pignatari SSNP,Weckx LLM. Correlationbetween fiberopticnasal endoscopyand acoustic rhinometryin adultswithoutnasal complaints.Am JRhinol. 2006;20:375---8.
17.CastanoR,ThériaoultG,GautrinD,GhezzoH,TrudeauC,Malo J.Reproducibilityofacousticrhinometryintheinvestigationof occupationalrhinitis.AmJRhinol.2007;21:474---7.
18.DorukC,SöcüküO,Bic¸akc¸iAA,YilmazU,TasF.Comparisonof nasal volumechangesduringrapidmaxillaryexpansion using acousticrhinometryandcomputedtomography.EurJOrthod. 2007;29:251---5.
19.HilbergO,PedersenOF.Acousticrhinometry:recommendations fortechnicalspecificationsandstandardoperatingprocedures. RhinolSuppl.2000;16:3---17.
20.ClementPAR,GordtsF.Consensusreportonacousticrhinometry andrhinomanometry.Rhinology.2005;43:169---79.
21.CoreyJP.Acousticrhinometry:shouldwebeusingit?CurrOpin OtolaryngolHeadNeckSurg.2006;14:29---34.
22.ClementPA,HalewyckS,GordtsF,MichelO.Criticalevaluation ofdifferentobjectivetechniquesofnasalairwayassessment:a clinicalreview.EurArchOtorhinolaryngol.2014[Epubaheadof print].
23.Zancanella E, Anselmo-Lima WT. Uso da rinometria acús-tica como método diagnóstico. Braz J Otorhinolaryngol. 2004;70:500---3.
24.MillqvistE,BendeM.Two-yearfollow-upwithacoustic rhinom-etryinchildren.AmJRhinol.2006;20:203---5.
25.Qian W, Chen W, Chen JM, Haight J. Acoustic rhinom-etry in preschool children. Otolaryngol Head Neck Surg. 2007;137:39---42.
26.Samolinski BK, GrzankaA, GotlibT. Changes in nasal cavity dimensionsinchildrenand adultsbygenderand age. Laryn-goscope.2007;117:1429---33.
27.Gomes AOC,Sampaio-Teixeira AC,Trindade SH, Trindade IE. Nasalcavitygeometryofhealthyadultsassessedusingacoustic rhinometry.BrazJOtorhinolaryngol.2008;74:746---54. 28.MamikogluB,HouserSM,AkbarINGB, CoreyJP.Acoustic
rhi-nometryandcomputedtomographyscansforthediagnosisof nasal septal deviation, withclinical correlation. Otolaryngol HeadNeckSurg.2000;123:61---8.
29.MamikogluB,HouserSM,CoreyJP.Aninterpretationmethod forobjectiveassessmentofnasalcongestionwithacoustic rhi-nometry.Laryngoscope.2002;112:926---9.
30.Carlini D, Ouriques DM, Weckx LLM, Fujitaet RR. Mod-ified method of acoustic rhinometry. Acta Otolaryngol. 2002;122:298---301.
31.NigroCEN,GotoE,NigroJFA,JuniorJM,MionO,VoegelsRL. Acousticrhinometry evaluation ofnasal cavity and nasopha-rynxbeforeandafteradenoidectomy.BrazJOtorhinolaryngol. 2003;69:333---6.
32.Marques VC, Anselmo-Lima WT. Pre and postoperative eval-uation by acoustic rhinometry of children submitted to adenoidectomyoradenotonsillectomy.IntJPediatr Otorhino-laryngol.2004;68:311---6.
33.CanIH,CeylanK,BayizU,OlmezA,SamimE.Acoustic rhinom-etryintheobjectiveevaluationofchildhoodseptoplasties.Int JPediatrOtorhinolaryngol.2005;69:445---8.
34.Trindade IEK, Castilho RL, Sampaio-Texeira ACM, Suedam-TrindadeIK,SilvaFilhoOG.Effectsoforthopedicrapidmaxillary expansiononinternalnasaldimensionsinchildrenwithcleftlip andpalateassessedbyacousticrhinometry.JCraniofacSurg. 2010;21:306---11.
35.CompadrettiGC,TascaT,Alessandri-BonettiPeriS,D´Addario A. Acoustic rhinometric measurements in children undergo-ingrapidmaxillary expansion.IntJPediatrOtorhinolaryngol. 2006;70:27---34.
36.EnokiC,ValeraFC,LessaFC,EliasAM,MatsumotoMA, Anselmo-LimaWT.Effectofrapidmaxillaryexpansiononthedimension ofthenasal cavityand onnasal airresistance.IntJPediatr Otorhinolaryngol.2006;70:1225---30.
37.TrindadeIEK,PradoPC,TrindadeSHK,DiasNH,Sampaio-Texeira ACM.Internalnasalmeasurementsofadultswithnasal obstruc-tion.BrazJOtorhinolaryngol.2013;79:1---7.
39.GomesAOC.Dimensõesinternasnasaisdecrianc¸ascomfissuras delábio epalatounilateralaferidasporrinometriaacústica. Bauru.Tese,HRAC-USP;2007.
40.LalD,CoreyJP.Acousticrhinometryanditsusesinrhinology anddiagnosisofnasalobstruction.FacialPlastSurgClinNorth Am.2004;12:397---405.
41.LemosCM,WilhelmsenNSW,MionOG,JúniorJFM.Alterac¸ões funcionais do sistema estomatognático em pacientes com rinitealérgica:estudocaso-controle.BrazJOtorhinolaryngol. 2009;75:268---74.
42.Connell JT. Rhinometry:measurement ofnasal patency. Ann Allergy.1982;49:179---85.
43.GrymerLF,HilbergO,PedersenOF.Predictionofnasal obstruc-tion based on clinical examination and acoustic rhinometry. Rhinology.1997;35:53---7.
44.ZavrasGE,WhiteA,RichI,JacksonAC.Acousticrhinometryn theevaluationofchildrenwithnasalororalrespiration.JClin PediatrDent.1994;18:203---10.
45.Fensterseifer GS, Carpes O, Weckx LLM, Martha VF. Mouth breathinginchildrenwithlearningdisorders.BrazJ Otorhino-laryngol.2013;79:620---4.
46.MendesAI,WandalsenGF,SoléD.Objective,subjective assess-mentsof nasal obstructionin children and adolescentswith allergicrhinitis.JPediatr.2012;88:389---95.
47.Teik-Ying NG, Chen YF, Tsai MH, Huang KH, Tai CJ. Objec-tivemeasurementsdifferforperceptionofleftandrightnasal obstruction.AurisNasusLarynx.2012;40:81---4.
48.Wandalsen GF, Mendes AI, Solé D. Correlation between nasal resistance and different acoustic rhinometry parameters in children and adolescents with and with-out allergic rhinitis. Braz J Otorhinolaryngol. 2012;78: 81---6.
49.Voegels RL, Goto EY, Lessa MM, Romano FR, Neves MC, TavaresR,et al.Avaliac¸ãoPré ePós-operatória por Rinome-tria Acústica de Pacientes Submetidos à Cirurgia de Septo NasaleConchasInferiores.IntArchOtorhinolaryngol.2002;6: 172.