Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Original
article
Palliative
care
in
pediatric
hematological
oncology
patients:
experience
of
a
tertiary
hospital
Maria
Thereza
Macedo
Valadares,
Joaquim
Antônio
César
Mota,
Benigna
Maria
de
Oliveira
∗UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received21January2013
Accepted25June2014
Availableonline18September2014
Keywords:
Palliativecare
Neoplasms Death
a
b
s
t
r
a
c
t
Objective:Toevaluatetheapproachtopalliativecareforhematologicaloncologypatientsin
thepediatricwardofatertiaryhospital.
Methods:Thiswasaretrospective,descriptivestudyof29hematologicaloncologypatients
whodiedbetween2009and2011.Dataregardingtheapproachandprevalenceofpain,
preva-lenceofothersymptoms,multidisciplinaryteamparticipation,communicationbetween
staffandfamilyandlimitedinvasivetherapywerecollectedfromthemedicalrecords.
Results:Twenty-seven(93.1%)patientsdisplayeddiseaseprogressionunresponsiveto
cura-tivetreatment.Themedianageatdeathwastenyearsold.Painwasthemostprevalent
symptomwithallpatientswhoreportedpainreceivinganalgesicmedications.Themajority
tookweak(55.2%)and/orstrong(65.5%)opioids.Thepatientswerefollowedbypediatricians
andapediatrichematologist/oncologist.Participationofotherprofessionalswasalso
doc-umented:86.2%werefollowedbysocialservicesand69%bypsychologists,amongothers.
Therewereexplicitdescriptionsoflimitationofinvasivetherapyinthemedicalrecordsof
26patientswhodiedwithdiseaseprogression.Allthesedecisionsweresharedwiththe
families.
Conclusion: Althoughthehospitalwherethisstudywasconducteddoesnothavea
special-izedteaminpediatricpalliativecare,itmeetsalltherequirementsfordevelopingaspecific
program.Theimportanceofapproachingpainandotherprevalentsymptomsinchildren
withcancerinvolvingacomprehensivemultidisciplinaryteamisevident.Discussionswere
hadwithmostofthefamiliesonlimitinginvasivetherapy,butnorecordofawell-defined
andcoordinatedtreatmentplanforpalliativecarewasfound.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:UniversidadeFederaldeMinasGerais(UFMG),Av.AlfredoBalena,190,sala267,30130-100BeloHorizonte,MG,
Brazil.
E-mailaddress:[email protected](B.M.deOliveira).
http://dx.doi.org/10.1016/j.bjhh.2014.09.003
1516-8484/©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Allrights
Introduction
Palliativecareinpediatricsis,accordingtotheWorldHealth
Organization,activeandtotalcaredeliveredtoachildin
rela-tiontohisorherbody,mindandsoul,withsupportprovidedto
thewholefamily.Thefocusofthisapproachisearly
identifi-cationandtreatmentofpainandothersymptomswithaview
toprovidingpatientsandtheirfamilieswiththebestquality
oflifepossible.1
There are currentlymany childreninneed ofpalliative
care2includingpatientswithneoplasms.Everyyear,200,000
childrenandadolescentsarediagnosedwithcanceraround
theworld.InBrazil,themortalityrateofchildrenand
adoles-centsagedbetweenoneand19duetocancerwas8%in2005
makingthisthesecondleadingcauseofdeathandthefirst
leadingcauseofdeathbydiseaseinthispopulation.Global
initiatives toprovide careforthesechildrenare,therefore,
necessaryandurgent.3,4
Thisstudyaimedtoevaluatetheapproachofpalliativecare
inhematologicaloncologypatientswhoprogressedtodeath
inthepediatricwardofatertiaryhospital.
It is important to state that palliative care should be
introduced at the time of diagnosis. However, as
cura-tivemeasuresdecrease,palliativecarebecomesanabsolute
necessity5and forthisreason,the studysamplewas
com-posedofpatientswhodied.
Methods
This was a retrospective, descriptive Study that included
allunder18-year-oldpatientsdiagnosedwithhematological
oncologydiseaseswhodiedinthepediatricwardofthe
Hos-pitaldas Clínicas atUniversidade Federalde Minas Gerais
(HC-UFMG)between2009and2011.
Patients withother diseases who also neededpalliative
careandprogressedtodeathwereexcludedaswerepatients
with hematological oncology diseases who died in their
homes,emergencyservices,intensivecareunitsorinother
hospitals.
Data were collected through analysis of the medical
records.Thesedatarefertothehospitalizationduringwhich
thepatientsdied.
The assessed data relate to the main items that
con-stitutegood assistanceinpalliativecare:approachtopain,
prevalenceofpainandothersymptoms,involvementofa
mul-tidisciplinary team, communication between medical staff
andfamily/patientonthecaseanddiseaseprogression,the
family’sdesiretogohome,patientfollow-upbythehomecare
serviceandlimitationofinvasivetherapy.
Thestudywasapprovedbythehospital’sResearchEthics
Committee,whichwaivedinformedconsent.
Results
Between2009and2011,44deathswererecordedinthe
pedi-atricwardoftheHC-UFMG.Ofthose,29(66%)werepatients
withhematologicaloncologydiseases,whowereincludedin
thestudy.
Ofthe29patientsthatdied,themedianagesatthetime
ofdiagnosisanddeathweresixandtenyears,respectively.
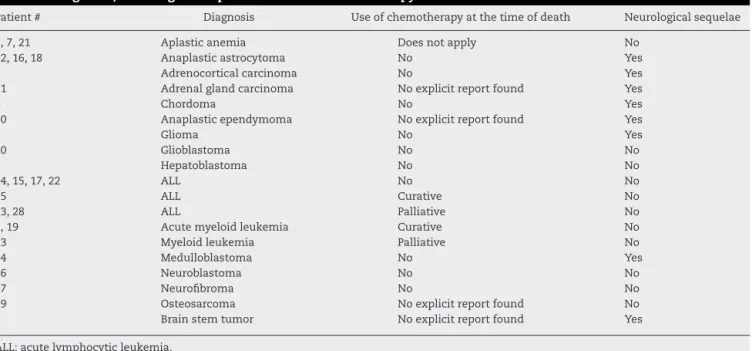
Forty-fivepercenthadhematologicaldiseases(aplastic
ane-miaor leukemia)and 55% hadsolid tumors.Twenty-seven
(93.1%)displayeddiseaseprogressionunresponsivetocurative
treatment.Ofthese,threepatientsreceivedchemotherapyas
apalliativemeasureandonlyonereceivedchemotherapywith
curativeprospects,evenwithdiseaseprogressionandlimited
invasivetherapy.
Tenpatients(34.4%)displayedneurologicalsequelae,with
varying degrees of cognitive deficit. Six patients were
tra-cheostomized(allwithneurologicalsequelae:#4,#9,#12,#16,
#18,#24),thirteenhadbeenusinganenteraltubeandonehad
agastrostomy.
Themediandurationofhospitalizationwas40days.Eight
patients(27.5%)wereadmittedintotheintensivecareunitat
leastonceduringhospitalization.
Data regarding the characterization of the sample are
showninTables1and2.
Themediannumber ofsymptomsdisplayedper patient
wasfour.Themainsymptomsandtheirprevalencesarelisted
inTable3.Painwasthemostprevalentsymptom,reportedby
almost80%ofthepatients.
All patients reporting pain took analgesic medications:
48.3% tookcommonanalgesicsbut themajoritytookweak
and/or strong opioids (55.2 and 65.5%, respectively). Three
patientswerefollowedupinthepainclinic.Therewereno
recordsofscalesornon-pharmacologicalmeasurestocontrol
painbeingused.
All patientswere followed up bygeneral pediatric
resi-dentsfullysupervisedbypreceptorsonthehospital’sclinical
staff. All patients were assisted bypediatric hematologists
oroncologistsasrequiredbytheirunderlyingdiseases.The
Table1–Characteristicsofthe29hematological oncologypatientswhoprogressedtodeath.
Characteristics
Gender(male:female) 18:11
Ageattimeofdiagnosis(years)
Median 6
Variation 1–16
Interquartilerange(25–75%) 2.5–9.5
Ageattimeofdeath(years)
Median 10
Variation 1–17
Interquartilerange(25–75%) 4.5–13
SymptomsreportedthroughoutHospitalization(n◦)
Median 4
Variation 0–8
Interquartilerange(25–75%) 3–6
Intervalbetweendiagnosisofanddeath(years)
Median 1.1
Variation 0.1–10
Interquartilerange(25–75%) 0.7–3.8
Durationofhospitalizationwhenpatientdied(days)
Median 40
Variation 3–246
Table2–Diagnosis,neurologicalsequelaeanduseofchemotherapyatthetimeofdeath.
Patient# Diagnosis Useofchemotherapyatthetimeofdeath Neurologicalsequelae
3,7,21 Aplasticanemia Doesnotapply No
12,16,18 Anaplasticastrocytoma No Yes
9 Adrenocorticalcarcinoma No Yes
11 Adrenalglandcarcinoma Noexplicitreportfound Yes
4 Chordoma No Yes
10 Anaplasticependymoma Noexplicitreportfound Yes
5 Glioma No Yes
20 Glioblastoma No No
8 Hepatoblastoma No No
14,15,17,22 ALL No No
25 ALL Curative No
13,28 ALL Palliative No
2,19 Acutemyeloidleukemia Curative No
23 Myeloidleukemia Palliative No
24 Medulloblastoma No Yes
26 Neuroblastoma No No
27 Neurofibroma No No
29 Osteosarcoma Noexplicitreportfound No
6 Brainstemtumor Noexplicitreportfound Yes
ALL:acutelymphocyticleukemia.
Table3–Prevalenceofthesymptomsdisplayedduring thehospitalizationinwhichthepatientdied.
Symptom n %
Pain 23 79.3
Dyspnea 20 69.0
Nausea/vomiting 18 62.1
Constipation 15 51.7
Depressedmood 13 44.8
Hyporexia 10 34.5
Anxiety 7 24.1
Sleepchanges 4 13.8
Weakness 3 10.3
Irritability 3 10.3
involvementofothermedical staffisshown inTable4. Of
the patientsfollowed up bythe psychiatry department,all
wereprescribedpsychiatricmedications(antidepressantsand
anxiolytics)and onlyone wasnotsimultaneously followed
upbythepsychologydepartment.Thepsychologyapproach,
Table4–Numberofpatientswhoreceivedcarefromthe differentprofessionalsinthemultidisciplinaryteam duringthehospitalizationinwhichthepatientdied.
Professional n %
Pediatricresident/preceptor 29 100.0
Staffnurses 29 100.0
Socialworker 25 86.2
Pediatriconcologist 16 55.0
Pediatrichematologist 13 45.0
Psychologist 20 69.0
Nutritionist 16 55.0
Physicaltherapist 11 37.9
Occupationaltherapist 8 27.6
Psychiatrist 5 17.2
Painclinic 3 10.3
Religioussupport 1 3.5
in its turn, was considered for both family members and
patients.
Therewerereportsofexplicitcommunicationbetweenthe
medical teamand thefamily onthe evolution ofthe case
anditsseriousness,proposedtreatmentand/orotherissues, including limitationsofinvasivetherapywhenindicatedin 96.5%(28/29)ofthe medicalrecords.Themedicalrecordof onepatient,whodiedwithdiseasecomplications,contained
noreportsofcommunicationbetweentheteamandhis
fam-ily.Therewerenoreportsofexplicitcommunicationbetween thestaffandpatientsinonlythreecases,whowereaged14, 15and17yearsatthetimeofdeath(#1,#7and#27).
Four records described the family’s desire to take the
patienthome.Allthepatientshadbeenundergoinglimited invasivetherapy.Fourpatientswerefollowedupbythehome careteam,buttheirmedicalrecordsreportednodesireofthe familytoreturnhome.Ofthesefourpatients,thefamiliesof twowerevisitedafterdeathbythehomecareteam.According totheirrecords,25ofthe29children(92.5%)were accompa-niedbyafamilymemberatthetimeofdeath,mostly(8/25 cases)onlybythemotheralthoughinfourcasesitwasonly thefather.Thefatherandmotherweretogetherinonlytwo cases.Intheothercases,thecompanionwasanotherfamily memberorcouldnotbeidentified.
complicationssecondary to treatment, were the only ones
whoreceivedcardiopulmonaryresuscitationpriortodeath.
Three patients, who had been tracheostomized, died on
mechanicalventilation,butnoneofthemreceived
cardiopul-monaryresuscitation.
Despite the limitation of invasive therapy having been
describedexplicitlyinthemedicalrecordsof26children,these
limits were only properly described in 16 (61.5%) patients;
thatis,in38.5%thetreatingphysiciandidnotclearlyexplain
whichtherapyshouldorshouldnotbedeliveredtothepatient,
butusedvaguetermssuchas“comfortmeasures”,“palliative
care”and“limitationoftherapeuticefforts”.
Discussion
Currently,around80%ofchildrenandadolescentsdiagnosed
withcancercanbecured.Inspiteofthehighratesofcure,
cancer-relatedmorbidityandmortalityisstillsignificant.3,4
Hence,dealingwiththisnewpatientprofileisachallenge.6
Impeccablecontrolofpainandothersymptomsisthemain
strategyinthepalliativeapproach.2Inpatientswithcancer,
painisanimportantfactorofdisease-relatedsuffering.5Asin
moststudies,painwasthemostprevalentsymptominthis
sample.7,10
Assessmentofpainshouldbedirectedduetothechild’sage
anddevelopment.2Wheneverpossible,thechild’sownreport
shouldbeesteemedandconsideredthegoldstandard.11Itis
recommendedtousescalestoassesstheintensity ofpain,
aswellastomonitortheprogressionoftreatment.1However,
theseinstrumentswerenotusedinthewardwherethestudy
wasconducted.
Lackofadequatecontrolofpainisatthecoreofthe
defi-cienciesobservedinpalliativecareindevelopingcountriesas
theavailabilityandconsumptionofopioids,consideredwide
indicatorsofcancer-relatedpainrelief,arestillrestricted.3,12
However,it wasobservedinthisstudy thatthemajorityof
patientswhoreportedpainwereprescribedopioids.
Non-pharmacologicalmeasureswerenotdescribedinthe
medical records. Such measures are part of the integral
management of pain and show synergistic effects todrug
treatment.13,14
Notonlyphysicalsymptomswereidentifiedinthisstudy.
Psychologicalsymptoms,suchasdepressionandsleep
dis-orders, were alsofound. Thesesymptoms are described in
the literature as an important cause of suffering for
chil-dren with cancer and they are often not addressed by
doctors.2,8,10
Asawayofrecognizingthecomplexityofcareneededby
patients withlife-threatening diseases, the involvementof
amultidisciplinaryteam isaprerequisitetodeliverquality
assistance.15 Itwasfound inthiscasestudy that a
signifi-cantnumberofpatientswereassistedbyamultidisciplinary
team, but the study design didnot allowanevaluation of
whetherthisfollow-upwaseffective.Itwasnotpossibleto
evaluatewhethertherewasinteractionwiththeteam,which
isessentialinmultidisciplinaryconditions,onlyby
examin-ingthemedicalrecords.Theoptimalfunctioningofthisteam
requirestraining,communicationandthesettingofrolesand
responsibilitiesofeachmember.15
The service provider where this study was conducted
hasno specialistsinpediatric palliativecare,but palliative
interventionsshouldnotbelimitedtospecialists.11 General
pediatriciansandpediatriciansfromdifferentfieldsshouldbe
abletohandlepalliativecareissues.6
Thetwopatientswho diedwithtreatment-related
com-plications were included inthis study since palliativecare
oughttobeinitiatedatthetimeofdiagnosis.6Moreover,only
fourofthepatientswhodiedwithdiseaseprogressionwere
receiving chemotherapywhen they died.In three ofthese
cases,chemotherapywasemployedasapalliativemeasure.
Researchers from differentcountrieshaveshownthat
chil-drenwhoreceiveend-of-lifechemotherapydisplayahigher
numberofsymptomsthanchildrenwhodonot,withgreater
likelihoodofinadequatecontrolofpain.8–10,16 Nevertheless,
the choice ofpalliativeor curative chemotherapyand
sus-pensionofchemotherapyisadifficultdecisionforboththe
medicalteamandthefamily.17Thisdifficultymaycause
med-icalstafftobereluctanttodiscloseanunfavorableprognosis
topatientsandtheirparents.16
Inmostofthecasesincludedinthisstudy,therewas
evi-denceofcommunicationbetweenteamsandfamilies.Three
records alsoreportedthatthere wasdirectcommunication
with thepatients, all ofwhomwere adolescents.However,
thesepatientsdidnottakepartinthedecisiontolimit
ther-apy, onlytheirparentsdid.Studiesemphasizethatdoctors
andparentsoughttotalktosickchildrenabouttheirfeelings
andanxieties.Avoidingthissortofcommunicationoverlooks
thefactthatmostofthetimetheyareawareoftheirsituation.6
Themedicalrecordsoffourfamiliesclearlyreportedthe
desiretotaketheirchildrenhome;allofthemwereawarethat
thediseasewasprogressing.Onlybyexaminingtherecords,
itisimpossibletoknowwhetherotherfamilieshadthesame
desire.Theplaceofdeathisanimportantindicatorof
end-of-lifequalityofcare.18Dyingathome,wheneverpossible,is
preferredbythemajorityoffamiliesofcancerpatients.19–21In
thisstudy,therewerereportsofafterdeathhomecarevisits
toonlytwochildren,whohadbeenfollowedupbythe
institu-tion’shomecareprogram.Afterdeathcareduringmourningis
alsoanimportantinterventioninpalliativecareandproduces
apositiveimpactonfamilies.
Decisionsonlimitationoffutiletherapyshouldbeshared
withpatientsandfamilies,22exactlyashappenedinthisstudy.
Intheonecaseinwhichtherewasadivergencebetweenthe
teamandthefamilyinspiteofprogressionofthedisease,the
patientcontinuedtoreceiveinvasiveinterventions,suchas
cardiopulmonaryresuscitation.
Tonellietal.evaluatedthecareprofiletopediatricpatients
whoprogressedtodeathinthesamehospitalasthecurrent
research.Participationofparentsindiscussionswasobserved
inonly20.8%ofthecases.23Thisfactdiffersfromtheresults
obtainedinthisstudy,whichfoundthatdiscussionswerehad
withtheparentsofallchildrenwithdiseaseprogression.Some
hypothesescanbesuggestedtoexplainthisdifference.Inthe
studybyTonellietal.,thedeathsofallpediatricpatientsat
thehospitalwereevaluated,includingpatientswithdifferent
diseasesandindifferentunits,suchasintheintensivecare
unitandoperatingrooms.23
Another factor that might have facilitated discussing
samplealreadyhadabondwiththemedicalteam,whichcan
beseenbytheintervalbetweenthediagnosisoftheunderlying
diseaseanddeath.24
Itshould also bestressed that in recent years medical
practicehasundergoneaculturalchange:the paternalistic
approachhasbeenreplacedbyanapproachthatrecognizes
theroleandimportanceofthefamilyandthepatient.25
Oneofthepossiblefactorsthataccountsforthisparadigm
shiftisthe currentBrazilianCode ofMedicalEthics,which
stressesthedutyofdoctorsto“providepalliativecareforpatients
withincurableandterminaldiseaseswithoutundertakinguseless therapeuticactionsandalwaystakingintoconsiderationthepatient’s manifestedwishor,shoulditproveimpossible,thewishofhis/her legalrepresentative”.26
Limitinginvasivetherapymeansexcludingfutile
interven-tions,whichdonothelptocontrolthe diseaseand donot
improvethepatient’squalityoflife.22Suchlimitationsshould
beindividualized.6,22Thesixtracheostomizedpatientsofthe
studycanberegardedasexamplesofthis.Allofthem
under-wentlimitation ofinvasive therapyandthreedied without
mechanicalventilatorysupport.Forthisreason,itis
impor-tantthatthephysicianrecordswhatshouldorshouldnotbe
done,afterhavinganappropriateconversationwiththe
fam-ily,ratherthanusingvaguetermssuchas“comfortmeasures”.
Itshouldbenotedthatsometermswereusedinappropriately.
Frequentlysomedoctors,whenevaluatingmedicalrecords,
consideredtheterm“palliativecaremeasures”tobesimilar
to“limitationoffutiletherapy”.
These findings reinforce the impression that there still
are heath workers who consider palliative careto be
end-of-life care.22 Some years ago,palliative and curative care
wereconsideredmutuallyexclusiveapproaches,and
pallia-tivecarewasonlyinitiatedafterallcurativepossibilitieshad
been exhausted. Currently, they are complementary forms
oftreatmentand palliativecareshouldbeimplemented at
thediagnoses oflife-threateningdiseases.Early integration
oftheseapproachesfacilitatesdiscussionofsensitiveissues
betweenmedicalstaffandfamilies,27,28inadditionto
improv-ingthequalityoflifeofpatients.29
Thelimitationsofthisstudyaremainlyrelatedtothe
rela-tivelysmallnumberofcasesandthelackofdataonthedeaths
thattookplaceathomeorinotherwards.However,
medi-calrecordswithclearandcomprehensibledescriptionswere
available.Thisisprobablyduetothefactthatthisisateaching
hospital.
Theresultsofthisstudyshowthatthehospitalwherethis
workwascarriedout,despitenothavingateamspecialized
inpediatricpalliativecare,meetsmostoftherequirements
forimplementingaspecificprogram.6Indevelopingcountries
suchasBrazil,therearestillcountlessdifficultiesto
follow-up children with cancer. Delays in diagnoses and limited
resources are someofthe obstacles found. Yet, suchfacts
should not hinder the development of pediatric palliative
care programs, which should be given priority in tertiary
hospitals.3,11
Theimportanceofmanagingpain andother symptoms
appropriatelyisevident.Forthisapproachtobetruly
effec-tive,involvementofworkersfromdifferentareas,withreal
integrationamongthem,isimperative.Othertoolscanalso
benefitthisapproach,suchastheuseofscales.
Despitetheinvolvementofseveralhealthworkerscaring
for thepatients included inthe study and the discussions
withmostofthemaboutlimitinginvasivetherapy,the
medi-calrecordsdidnotincludedescriptionsofawell-thought-out
treatmentplan.Thisplanconsistsofdiscussingwithpatients
andfamiliesinadvanceaboutwhatkindofassistancewillbe
delivered.Itshouldnotaddressonlymedicalaspects,butalso
socialissuessuchaswhatandwhoisimportanttothechild
andhisorherfamily.Thisplanningshouldbereassessedas
requiredbychangesintheclinicalstatus.6
Training communicationskills, developingthe abilityto
interactwithotherworkers,learningtocopewiththe
diffi-cultiesintrinsictotheprocessofdeathareamongtheitems
thatshouldbeimproved.27Inthisway,greatqualityassistance
willbedeliveredtopatientsthroughouttheprocessofdisease
regardlessofwhetherthefinaloutcomeiscureordeath.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WorldHealthOrganization.Cancerpainreliefandpalliative
careinchildren.Geneva:WHO;1998.Availablefrom:
http://whqlibdoc.who.int/publications/9241545127.pdf[cited 21.01.14].
2.HimelsteinBP.Palliativecareforinfants,children,
adolescents,andtheirfamilies.JPalliatMed.2006;9(1):163–81.
3.Rodriguez-GalindoC,FriedrichP,MorrisseyL,FrazierL.Global challengesinpediatriconcology.CurrOpinPediatr.
2013;25(1):3–15.
4.MinistériodaSaúde.InstitutoNacionaldeCâncer–INCA.
Câncerdacrianc¸aedoadolescentenoBrasil:dadosdo
registrodebasepopulacionalemortalidade;2008.Riode
Janeiro.Availablefrom:http://bvsms.saude.gov.br/bvs/
publicacoes/cancercriancaadolescentebrasil.pdf[cited 21.01.14].
5.PintoAC,CunhaAA,OtheroMB,BettebgaRT,BarbosaSM, ChibaT,etal.ManualdeCuidadosPaliativos/Academia NacionaldeCuidadosPaliativos.RiodeJaneiro:Diagraphic; 2009.
6.AmericanAcademyofPediatrics.CommitteeonBioethics andCommitteeonHospitalCare.Palliativecareforchildren. Pediatrics.2000;1062Pt1:351–7.
7.TheunissenJM,HoogerbruggePM,VanAchterbergT,PrinsJB, Vernooij-DassenMJ,VandenEndeCH.Symptomsinthe palliativephaseofchildrenwithcancer.PediatrBloodCancer. 2007;49(2):160–5.
8.CollinsJJ,ByrnesME,DunkelIJ,LapinJ,NadelT,ThalerHT, etal.Themeasurementofsymptomsinchildrenwithcancer. JPainSymptomManage.2000;19(5):363–77.
9.BerettaS,PolastriD,ClericiCA,CasanovaM,CefaloG,Ferrati A,etal.Endoflifeinchildrenwithcancer:experienceatthe PediatricOncologyDepartmentoftheIstitutoNazionale TumoriinMilan.PediatrBloodCancer.2010;54(1):88–91.
10.HeathJA,ClarkeNE,DonathSM,McCarthyM,AndersonVA, WolfeJ.Symptomsandsufferingattheendoflifeinchildren withcancer:anAustralianperspective.MedJAust.
2010;192(2):71–5.
12.DelgadoE,BarfielRC,BakerJN,HindsPS,YangJ,NambayanA, etal.Availabilityofpalliativecareservicesforchildrenwith cancerineconomicallydiverseregionsoftheworld.EurJ Cancer.2010;46(12):2260–6.
13.Vargas-SchafferG.IstheWHOanalgesicladderstillvalid? Twenty-fouryearsofexperience.CanFamPhys.
2010;56(6):514–7.
14.AraujoCM,OliveiraBM,PereiraYS.Avaliac¸ãoetratamentoda doremoncologiapediátrica.RevMédMinasGerais(Belo Horizonte).2012;22Suppl.7:S22–31.
15.VissersKCP,VanDenBranMWM,JacobsJ,GrootM,
VeldhovenC,VerhagenC,etal.Palliativemedicineupdate:a multidisciplinaryapproach.PainPract.2013;13(7):576–88.
16.TangST,HungYN,LiuTW,LinDT,ChenYC,WuSC,etal.
PediatricendoflifecareforTaiwanesechildrenwhodiedasa resultofcancerfrom2001through2006.JClinOncol. 2011;29(7):890–4.
17.TomlisonD,BartelsU,GammonJ,HindsPS,VolpeJ,BouffetE, etal.Chemotherapyversussupportivecarealoneinpediatric palliativecareforcancer:comparingthepreferencesof parentsandhealthcareprofessionals.CMAJ.
2011;183(17):E1252–8.
18.HouttekierD,CohenJ,SurkynJ,DeliensL.Studyofrecentand futuretrendsinplaceofdeathinBelgiumusingdeath certificatedata:ashiftfromhospitalstocarehomes.BMC PublicHealth.2011;11:228.
19.VickersJ,ThompsonA,CollinsGS,ChildsM,HainR.Place andprovisionofpalliativecareforchildrenwithprogressive cancer:astudybythepaediatriconcologynurses’
Forum/UnitedKingdomChildren’sCancerStudyGroup PalliativeCareWorkingGroup.JClinOncol.
2007;25(28):4472–6.
20.WidgerK,DaviesD,DrouinDJ,BeauneL,DaoustL,FarranRP, etal.PediatricpatientsreceivingpalliativecareinCanada: resultsofamulticenterreview.ArchPediatrAdolescMed. 2007;161(6):597–602.
21.KurashimaAY,LatorreMR,TeixeiraSA,CamargoB.Factors associatedwithlocationofdeathofchildrenwithcancerin palliativecare.PalliatSupportCare.2005;3(2):115–9.
22.PivaJP,GarciaPCR,LagoPM.Dilemasedificuldades envolvendodecisõesdefinaldevidaeofertadecuidados paliativosempediatria.RevBrasTerIntens.2011;23(1):78–86.
23.TonelliHA,MotaJA,OliveiraJS.Perfildascondutasmédicas queantecedemaoóbitodecrianc¸asemumhospitalterciário. JPediatr(RioJ).2005;81(2):118–25.
24.HellerKS,SolomonMZ.Continuityofcareandcaring:what matterstoparentsofchildrenwithlife-threatening conditions.JPediatrNurs.2005;20(5):335–46.
25.WeidnerNJ.PediatricpalliativeCare.CurrOncolRep. 2007;9(6):437–9.
26.ConselhoFederaldeMedicina.CódigodeÉticaMédica.
Availablefrom:www.portalmedico.org.br/novocodigo/
integra1.asp[cited21.01.14].
27.MoritzRD,DeicasA,CapalboM,ForteDN,KretzerLP,LagoP, etal.IIFórumdo“GrupodeEstudosdoFimdaVidadoCone Sul”:definic¸ões,recomendac¸õeseac¸õesintegradaspara cuidadospaliativosnaunidadedeterapiaintensivade adultosepediátrica.RevBrasTerIntens.2011;23(1):24–9.
28.MichelsonKN,SteinhornDM.PediatricEnd-of-Lifeissuesand palliativecare.ClinPediatrEmergMed.2007;8(3):212–9.
29.TemelJS,GreerJA,MusikanskyA,GallagherER,AdmaneS, JacksonVA,etal.Earlypalliativecareforpatientswith metastaticnon-small-celllungcancer.NEJM.