Universidade de Lisboa
Faculdade de Motricidade Humana
Biomechanical gait pattern changes
associated with functional fitness levels and
falls in the elderly
Dissertação elaborada com vista à obtenção do Grau de Doutor em
Motricidade Humana na Especialidade de Biomecânica
Orientador: Doutor António Prieto Veloso
Júri: Presidente
Reitor da Universidade de Lisboa Vogais
Doutor Vasilios Baltzopoulos, Professor Catedrático da Brunel University (Londres, Reino Unido) Doutor António Prieto Veloso, Professor Catedrático da Faculdade de Motricidade Humana, Universidade de Lisboa
Doutora Maria de Fátima Marcelina Baptista, Professora Associada com Agregação da Faculdade de Motricidade Humana da Universidade de Lisboa
Doutor Wolfgang Potthast, Professor Associado da Deutsche Sporthochschule Köln (Alemanha) Doutor Miguel Tavares da Silva, Professor Auxiliar do Instituto Superior Técnico da Universidade de Lisboa
Vera Moniz Pereira da Silva
2014
1
“Não faço tudo o que amo, mas amo tudo o que faço” “I do not do everything I love, but I love everything I do” (Gabriel o Pensador)
1
Para a minha avó Carlota, uma das primeiras mulheres licenciadas em Educação Física em Portugal, a melhor aluna do seu curso, uma avó maravilhosa, uma mulher extraordinária. O meu exemplo, a minha inspiração.
To my grandmother Carlota, one of the first women who graduated in Physical Education in Portugal, the best student of her course, a wonderful grandmother and an extraordinary woman. She was and is my role model and my inspiration.
1
Acknowledgments
The accomplishment of this work would not have been possible without the support of several people to whom I am very grateful.First, I would like to thank my supervisor, Professor António Prieto Veloso, who has, from the beginning, stimulated my interest in research and namely in biomechanics. António’s determination to develop biomechanics research in the University of Lisbon and throughout the country, together with his constant desire to achieve higher research standards, made possible for me to engage in different learning experiences and therefore to grow scientifically and to grow as a person. Thanks to his broad vision and networking, I spent the first semester of my PhD in the Institute for Biomedical Research into Human Movement and Health (IRM) in Manchester Metropolitan University, learning several laboratory techniques used in biomechanics. During this time, I was under the supervision of Professor Vasilios Baltzopoulos, to whom I am thankful for having dedicated his time to teach me, especially in what concerns the importance of the standardization of the laboratory procedures (from motion capture, to strength and ultrasound measures) in order to reduce the error during data collection. I am also thankful to the IRM students, particularly to Divya Sing, Linda Tersteeg and Stefano Longo, who not only have make me feel at home from the beginning, but also discussed with me constantly, and thus participated actively in my learning process. Further, António also made possible for me, several times during this process, to learn, discuss and collaborate with other scientists highly recognized in the biomechanics community. Within these, I am especially grateful to Doctor W. Scott Selbie and Tom Kepple who, despite of distance and difference in time zones, were always available to teach me and provided me with fruitfully and diverse discussions (including themes like signal filtering, modeling and induced acceleration analysis).
I am also thankful to all my co-authors, for their contributions to this work, and to other members of the Neuromechanics Research Group who were available to discuss and therefore helped me grow scientifically. Within these, I am especially grateful to Filomena Carnide, Rita Fernandes, Ruth Agostinho and Silvia Cabral. In addition of being great colleagues, they are very good friends who greatly supported and encouraged my work.
vi
Further I have to thank all the colleagues who have dared or challenged me in many different ways. They have made me a more mature, determined and resilient person.
Finally, I would like to thank to all of my friends and family that were there to make me sure that my life was and is much more than a PhD thesis. Specially, I am grateful to Marco Alves, who largely contributed for this thesis art work; to my parents, Leonor Moniz-Pereira e Francisco Silva, for being an example, for supporting me emotionally and financially, for reading my work despite of the fact that I have rarely read theirs; and to António V. Fortuna for his endless patience, daily support and unconditional love throughout this journey.
This work was also not possible without the PhD grant supported by the Portuguese Foundation for Science and Technology (PhD Grant reference: SFRH / BD / 36670 / 2007), and the congress travel grants awarded by the rectory of the Technical University of Lisbon and the International society of Biomechanics.
1
Resumo
A presente dissertação objetiva o aprofundamento do conhecimento sobre os determinantes das quedas na população idosa portuguesa, com especial enfoque nas alterações biomecânicas nos padrões de marcha associadas ao declínio funcional característico desta população. A abordagem metodológica preconizada para a análise do problema compreende duas fases complementares: uma primeira fase, que englobou dois estudos epidemiológicos com o objetivo de estabelecer os fatores determinantes de quedas na população idosa portuguesa; uma segunda fase, onde foram considerados três estudos experimentais (laboratoriais), com o propósito de determinar a influência de diferentes níveis de aptidão funcional nos padrões de marcha desta população. Os resultados demostraram que as quedas resultam da interação de diversos fatores de risco, destacando-se os seguintes: género, parâmetros de aptidão funcional e de saúde. De relevar que o fenómeno de queda se revelou independente da idade, mesmo quando analisada a sua associação com os fatores determinantes em grupos etários mais avançados (≥75 e ≥80 anos). Neste sentido, nos estudos subsequentes, foram analisados os padrões de marcha de subgrupos de idosos recrutados do grupo de participantes dos estudos anteriores e estratificados em função do seu nível de aptidão funcional. Observou-se então que os idosos com baixos níveis de aptidão funcional adotavam estratégias consistentes de redistribuição dos momentos de força articulares dos membros inferiores, aquando da execução de diferentes tarefas locomotoras (marcha, subir e descer escadas). Considerando o sucesso demonstrado das intervenções sustentadas em programas de atividade física para a prevenção de quedas e incapacidade, as alterações biomecânicas dos padrões de marcha observadas poderão constituir um importante suporte informacional para os profissionais de saúde e exercício que trabalham com a população idosa.Palavras-chave: Idosos, Quedas, Aptidão funcional, Momentos de força articulares,
1
Abstract
This thesis aimed to provide a better understanding on the determinant factors for falling in Portuguese older adults, with a special emphasis on the biomechanical changes in gait patterns associated with the functional fitness decline in this population. Our methodological approach to this problem encompassed two different levels of analysis: in the first part two epidemiological studies were conducted in order to establish the determinant factors for falling within the Portuguese older adults; in the second part three laboratory-based studies were performed in order to determine the influence of functional fitness levels on elderly gait patterns. Falls were shown to result from the interaction of many risk factors. Within these, gender, functional fitness level and health parameters were found to be the strongest fall determinants. Interestingly, age was not a determinant factor for falling, even within very old individuals (≥75 years or ≥80 years). Therefore, in the subsequent studies, the gait patterns of a subgroup of older adults, who had participated in the epidemiological studies, were characterized according with their functional fitness levels. The results showed that older subjects with a lower functional fitness level score, consistently re-distribute lower limb joint moments while performing different locomotor tasks (walking, stair ascent and stair descent). Because the success of physical activity interventions aiming at falls and disability prevention is dependent on subgroup characterization, these biomechanical gait pattern changes may yield important information for the health and exercise professionals working with the elderly.
1
Contents
Acknowledgments ... v Resumo ... vii Abstract ... ixList of Figures ... xiii
List of Tables... xv
List of Abbreviations ... xvii
Chapter 1: General Introduction ... 1
Chapter 2: Falls in Portuguese older people: procedures and preliminary results of the study biomechanics of locomotion in the elderly ... 15
Chapter 3: Using a multifactorial approach to determine fall risk profiles in Portuguese older adults ... 35
Chapter 4: Sensitivity of joint kinematics and kinetics to different pose estimation algorithms and joint constraints in the elderly ... 55
Chapter 5: Gait patterns in the elderly: the influence of functional fitness level ... 69
Chapter 6: Using induced accelerations to analyze gait in the elderly ... 87
Chapter 7: General Discussion ... 97
Thesis related outcomes ... 115
Appendix 1: Sensitivity of joint kinematics and kinetics to different pose estimation algorithms and joint constraints in the elderly (appendix data) ... 119
Appendix 2: Relevant Elderly Gait Features for Functional Fitness Level Grouping ... 129
1
List
of Figures
Figure 1.1: Risk factor model for falls in older age (World Health Organization, 2007) ... 4 Figure 1.2: Disability conceptual model (Spirduso et al., 2005) ... 5 Figure 1.3: A functional ability framework(Rikli & Jones, 1997, 1999) ... 6 Figure 4.1: Joint angles root mean square (RMS) (A) and normalized RMS (RMSN) (B) differences between methods for the walking task (Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion). Maximum and minimum intersubject variability (INTER_VAR) is represented by the gray shadow, while maximum and minimum intrasubject variability (INTRA_VAR) is represented by the black shadow. ... 61 Figure 4.2: Joint moments root mean square (RMS) (A) and normalized RMS (RMSN) (B) differences between methods for the walking task (Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion). Maximum and minimum intersubject variability (INTER_VAR) is represented by the gray shadow, while maximum and minimum intrasubject variability (INTRA_VAR) is represented by the black shadow. ... 62 Figure 4.3: Joint angular displacements, of one of the subjects, for the 3 different methods during a walking stride cycle (from right foot off to right foot off). Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion. ... 63 Figure 4.4: Joint moments, of one of the subjects, for the 3 different methods during a walking stride cycle (from right foot off to right foot off). Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion. ... 64
Figure 5.1: Joint moment profiles in the sagittal plane during stance for all tasks. LFFL stands for low functional fitness level group and HFFL stands for high functional fitness level group. The vertical line distinguishes braking and propulsive impulses (impulse 1 and 2, respectively). Positive values represent plantarflexion/extension moments. ... 77 Figure 5.2: Joint moment profiles in the frontal plane during stance for all tasks. LFFL stands for low functional fitness level group and HFFL stands for high functional fitness level group. The vertical line distinguishes braking and propulsive impulses (impulse 1 and 2, respectively). Positive values represent abduction moments... 79 Figure 6.1: Mean (n=3) lower limb joint moments in sagittal plane as a % of gait cycle (GC) time. Forward acceleration interval is in grey ... 92 Figure 6.2: (A) Mean (n=3) induced horizontal acceleration on CoM during forward acceleration interval (~35-55% of total GC); (B) Mean (n=3) induced vertical acceleration on CoM during gait cycle (data computed only after right toe off ~10% GC; double support phase is in grey) ... 93 Figure 7.1: Marker set ... 106 Figure 7.2: Diagram showing the custom-built staircase ... 108
xiv
Figure 9.1: Joint angles root mean square (RMS) (A) and normalized RMS (RMSN) (B) differences between methods for the stair ascent task (Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion). Maximum and minimum intersubject variability (INTER_VAR) is represented by the gray shadow, while maximum and minimum intrasubject variability (INTRA_VAR) is represented by the black shadow. ... 121 Figure 9.2: Joint moments root mean square (RMS) (A) and normalized RMS (RMSN) (B) differences between methods for the stair ascent task (Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion). Maximum and minimum intersubject variability (INTER_VAR) is represented by the gray shadow, while maximum and minimum intrasubject variability (INTRA_VAR) is represented by the black shadow. ... 122 Figure 9.3: Joint angular displacements, of one of the subjects, for the 3 different methods during a stair ascent stride cycle (from right foot contact to right foot contact). Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion. ... 123 Figure 9.4: Joint moments, of one of the subjects, for the 3 different methods during a stair ascent stride cycle (from right foot contact to right foot contact). Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion. ... 124 Figure 9.5: Joint angles root mean square (RMS) (A) and normalized RMS (RMSN) (B) differences between methods for the stair descent task (Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion). Maximum and minimum intersubject variability (INTER_VAR) is represented by the gray shadow, while maximum and minimum intrasubject variability (INTRA_VAR) is represented by the black shadow. ... 125 Figure 9.6: Joint moments root mean square (RMS) (A) and normalized RMS (RMSN) (B) differences between methods for the stair descent task (Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion). Maximum and minimum intersubject variability (INTER_VAR) is represented by the gray shadow, while maximum and minimum intrasubject variability (INTRA_VAR) is represented by the black shadow. ... 126 Figure 9.7: Joint angular displacements, of one of the subjects, for the 3 different methods during a stair descent stride cycle (from right foot off to right foot off). Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion. ... 127 Figure 9.8: Joint moments, of one of the subjects, for the 3 different methods during a stair descent stride cycle (from right foot off to right foot off). Fl/Ex, Ab/Ad, Ex/In and Pf/Df stand for flexion/extension, abduction/adduction, external/internal rotations and plantar/dorsiflexion. ... 128
1
List of Tables
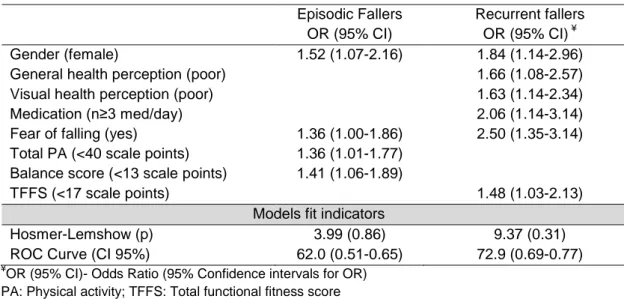
Table 2.1: Sample characterization: main demographic parameters and their associations among groups non-fallers (NF), fallers (F) and recurrent fallers (RF). ... 24 Table 2.2: Health parameters and its association among groups of Non-fallers(NF), fallers (F) and recurrent fallers (RF) ... 26 Table 2.3: Physical Activity parameters and their association among between groups non-fallers (NF), fallers (F) and recurrent fallers (RF) ... 27 Table 2.4: Functional Fitness parameters and their association among groups non-fallers (NF), fallers (F) and recurrent fallers (RF) ... 28 Table 3.1: Sample characterization: Demographic, health, PA and FF parameters (absolute and valid frequency) and their associations among groups (non-fallers (NF), episodic fallers (EF) and recurrent fallers (RF)) ... 44 Table 3.2: Bivariate logistic regression models for episodic and recurrent fallers ... 45 Table 3.3: Multivariate logistic regression models for episodic and recurrent fallers... 46 Table 5.1: Group Means (M) ± SD and effect sizes (ES) for temporal distance parameters during walking, stair ascent and stair descent. ... 76 Table 5.2: Means ± SD for joint moments and rotational impulses for each task: within subjects effects. ... 78 Table 5.3: Means ± SD and effect sizes (ES) for joint moments and rotational impulses for each task: between groups effects. ... 80 Table 6.1: Kinematic and kinetic gait variables ... 92
1
List of Abbreviations
ADLs Activities of daily living CD Chronic diseases CoM Centre of mass CS Chair stand test (SFT) ES Effect size
F/EF Episodic fallers
FAB Fullerton advanced balance scale FAB4 Step up and over a bench (FAB) FAB5 Tandem walk along a line (FAB) FAB6 Stand on one leg from (FAB)
FAB7 Stand on a foam with eyes closed (FAB) FF Functional fitness
FOF Fear of falling GC Gait cycle
GO Global optimization
GOR Global optimization restricted GRF Ground reaction force HHP Hearing health perception
HFFL High functional fitness level group HP Health perception
IAA Induced acceleration analysis
LFFL Low functional fitness level group MI Moving index (YPAS)
NF Non fallers PA Physical activity
Pose Segments’ position and orientation RF Recurrent fallers
RMS Root mean square ROM Range of motion SA Stair ascent SD Stair descent SFT Senior fitness test SI Standing index (YPAS) SO Segment optimization STA Soft tissue artifact STI Sitting index (YPAS) UG 8 foot and go test (SFT) VHP Visual health perception VI Vigorous index (YPAS) WI Walking index (YPAS) YPAS Yale physical activity survey
1
Cha
pter
1
1.1 Background
Thirty to forty percent of the community dwelling older adults over 65 years fall at least once each year (Todd & Skelton, 2004; Lord, Sherrington, Menz, & Close, 2007a; World Health Organization, 2007). Further, fall rates are reported to increase with ageing, reaching approximately 50% in elderly who are over 80 years of age (Todd & Skelton, 2004). More than an incidence issue, falling is a serious problem among older adults, who are more susceptible to injury due to the higher prevalence of clinical conditions like osteoporosis and reduced bone density. Thus, within this population, even a mild fall may have very serious consequences. Falls have been related to the increase of morbidity and mortality within the older subjects, and may also be the first indicator of an undetected illness (Todd & Skelton, 2004; World Health Organization, 2007). Furthermore, even non-injurious falls appear to be determinant for functional decline, social withdrawal, anxiety and depression, and long term placement in a skilled-nursing facility (Todd & Skelton, 2004; Tinetti & Williams, 1997, 1998; Stel, Smit, Pluijm, & Lips, 2003; Voermans, Snijders, Schoon, & Bloem, 2007).The burden induced by falls not only affects the elderly and their families’ quality of life, but has also associated costs for the health care system, which are reported to be increasing throughout the world, due to the increase of life expectancy (World Health Organization, 2007). As so, fall prevention became a primary public health concern, and many studies have been done to determine the main risk factors for falling (e.g. Graafmans et al., 1996; Pluijm et al., 2006; Stalenhoef, Diederiks, Knottnerus, Kester, & Crebolder, 2002; Tromp et al., 2001; Yamashita, Noe, & Bailer, 2012).
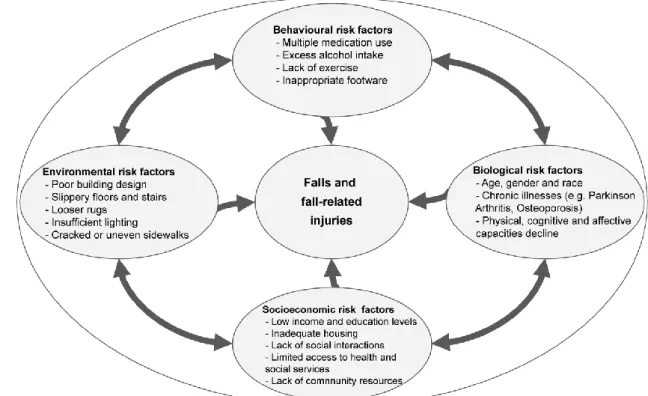
The problem of falls has shown to be the result of the interaction of many risk factors, categorized in four dimensions by the World Health Organization (World Health Organization, 2007): biological, behavioral, environmental and socioeconomic (Figure 1.1). The biological risks factors comprise the individual characteristics related with the human body, including non-modifiable factors, like age, gender and race, and factors that may be modified, such as the decline in physical capacity. The behavioral factors are related with human actions, emotions and daily choices (sedentary behavior and excess alcohol use, for example) and are also potentially modifiable. Environmental
4
risk factors include home hazards and hazardous features in public environment (narrow steps, slippery surfaces of stairs, looser rugs and so on). These factors are not by themselves the direct cause for falling. Instead, falls occur due to the interaction between individuals’ physical conditions and the surrounding environment, to which they are exposed. Finally, socioeconomic risk factors are associated with the social conditions and the economic status of the individual (examples: low income, lack of social interactions and limited access to health and social services).
Figure 1.1: Risk factor model for falls in older age (World Health Organization, 2007)
Although falls are a result of the interaction of multiple factors, specific physical capacity related factors, such as muscle weakness and problems with gait and balance, have been identified as particularly important risk factors for falling (Rubenstein, 2006). Since the mentioned factors are related to physical function decline, which is strongly associated with inactivity rather than age and/or disease alone (Collins, Rooney, Smalley, & Havens, 2004; Spirduso, Francis, & MacRae, 2005; U.S. Department of Health and Human Services, 1996; Visser, Pluijm, Stel, Bosscher, & Deeg, 2002), this will have important consequences for a pro-active approach of fall prevention. In fact, the Fall Prevention Model established by the World Health Organization (World Health Organization, 2007) is built within the Active Ageing Policy Framework (World Health Organization, 2002), which aims to extend the healthy life expectancy (i.e. the years lived without disability) and the quality of life for all people
Cha
pter
1
during the ageing process. The key goal in this framework is to maintain autonomy and independence through life by sustaining an active lifestyle (both in terms of physical activity, as well as through the engagement in social, cultural, civic and other activities) (World Health Organization, 2002).
This interaction between lifestyle behaviors, physical function, falls and disability is shown on the disability conceptual model proposed by Spirduso et al 2005 (Figure 1.2). By combining all factors that have been related to disability in previous predictive models (Lawrence & Jette, 1996; Morey, Pieper, & Cornoni-Huntley, 1998; Nagi, 1991; Verbrugge & Jette, 1994), this model expands the view of disability, as the sole consequence of pathology (Nagi, 1991), to a more complex model.
Figure 1.2: Disability conceptual model (Spirduso et al., 2005)
In this model, physical capacity factors1 are directly related to falls and functional limitations, even on the absence of pathology. Age, race, gender, education, depression and cognitive dysfunction, are included as confounding factors, due to their influence on physical capacity factors. Lifestyle behavioral factors are also considered, showing that the path towards disability should not be assumed as inevitable, but can be reversed by changing health and physical activity habits (Spirduso et al., 2005).
1
Due to the variety terms co-existing in the literature (Rikli & Jones, 1999; Spirduso, Francis, & MacRae, 2005; World Health Organization, 2007), in the scope of this thesis physical capacity factors embrace the terms fitness factors and physical parameters
6
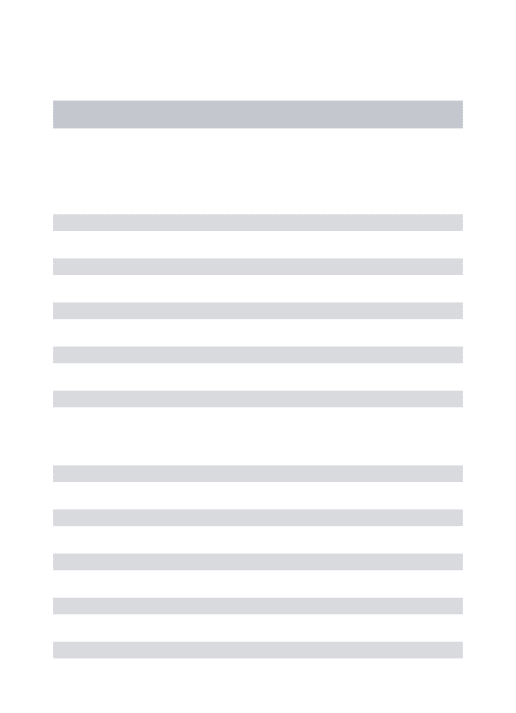
Because of the role of physical function on falls and disability, the measurement of the physiological declines that precede the loss of function became a priority when dealing with community dwelling older adults (Rikli & Jones, 1997, 1999). To this effect, and based on the disability models, Rikli and Jones (1997, 1999) proposed a functional ability framework so that the physical capacity factors necessary to perform certain functions, and essential to accomplish common daily activities, could be identified (Figure 1.3).
Figure 1.3: A functional ability framework (Rikli & Jones, 1997, 1999)
Within this framework, the authors also defined functional fitness as “having the physiologic capacity to perform normal daily activities safely and independent without the undue fatigue” (Rikli & Jones, 1999; pp133). The expression “without undue fatigue” is used to integrate the concept of physiological reserve and thus emphasize the need of having an adequate reserve of the physical capacity factors (e.g. muscle strength, aerobic endurance, balance) in order to perform the correspondent daily activities. The majority of these activities require the ability to move from a place to another, independently and safely, which is defined as mobility (Rantakokko, Mänty, & Rantanen, 2013). Elderly physical capacity decline, namely muscle strength decline, is shown to be particularly high in lower limb muscles, leading to problems in mobility and difficulties in performing daily activities (Vandervoort, 2002). Therefore, it is not surprising that older adults report difficulties in gait activities performance, especially
Cha
pter
1
when dealing with stairs, and that most falls occur during these activities (Berg, Alessio, Mills, & Tong, 1997; Startzell, Owens, Mulfinger, & Cavanagh, 2000).
In exercise and rehabilitation contexts, mobility limitations can be measured through self report, which is based on the subjects’ self perception of mobility, or through performance tests, in which the examiner rates the subject’s performance during a specific task, therefore providing a more objective measure of mobility (Rantakokko et al., 2013). Nevertheless, to have a better understanding of the mechanisms underlying the functional changes in gait activities, a more complex approach is needed. Through instrumented gait analysis it is possible to quantify the mobility changes associated to a determined disorder/condition, as well as to determine the neuromuscular-skeletal parameters causing those changes (Simon, 2004). This assessment technique is shown to offer a reliable assessment of gait performance (Wilken, Rodriguez, Brawner, & Darter, 2012). In older adults, instrumented gait analysis may yield important information regarding the biomechanical mechanisms of balance control underlying the performance of gait activities, and thus help to pin-point useful changes related to functional impairments and falls (Winter, 1991).
It is fairly difficult to compare the results of the studies concerning the biomechanical changes in elderly gait patterns, since they differ highly regarding the data collection equipment used, the biomechanical model chosen and the normalization process of the data. Even though, there are some consistent findings in the literature, especially in what concerns temporal-distance and/or kinematic parameters while walking. When compared with younger adults, older individuals were shown to walk with a slower velocity, a shorter stride length and an increased stance time (namely, double support time) (DeVita & Hortobagyi, 2000; Prince, Corriveau, Hébert, & Winter, 1997; Winter, Patla, Frank, & Walt, 1990). A decrease in ankle and knee flexion/extension range of motion and an increase of hip flexion/extension range of motion and hip flexion are also consistent kinematic changes related with ageing (DeVita & Hortobagyi, 2000; Kerrigan, Todd, Della Croce, Lipsitz, & Collins, 1998; Prince et al., 1997). Furthermore, although kinetic changes in elderly walking patterns are less studied, a less vigorous push off, reflected through a reduction in the peak of the anterior ground reaction force and of the plantaflexor joint moment, seems to be a consistent characteristic of older adults gait patterns (DeVita & Hortobagyi, 2000; Prince et al., 1997; Winter et al., 1990). Studies regarding elderly changes in stair walking patterns are scarce and some
8
of them are focused only on the negotiation of a single step (Begg & Sparrow, 2000; T Hortobágyi & DeVita, 1999; Lark, Buckley, Bennett, Jones, & Sargeant, 2003; Lark, Buckley, Jones, & Sargeant, 2004), while others are centered on the behavior of one or two lower limb joints (Tibor Hortobágyi, Mizelle, Beam, & DeVita, 2003; Reeves, Spanjaard, Mohagheghi, Baltzopoulos, & Maganaris, 2008, 2009). Nevertheless, it is interesting to note that both during level and stair walking older adults, when compared with their younger counterparts, seem to redistribute lower limb joint moments by consistently applying a lower plantarflexor joint moment (DeVita & Hortobagyi, 2000; Novak & Brouwer, 2011; Reeves et al., 2008, 2009). Further studies are needed to have more consistent findings regarding the behavior of other lower limb joints.
Another issue is that the majority of the mentioned studies commonly compare healthy independent older adults with younger counterparts, which are expectable different groups. Additionally, older adults are an heterogeneous group in terms of physical function, and even within community dwelling older adults, a widely range of capacities can be found (Spirduso et al., 2005). This issue was already stressed out by Kressig et al. (2004), who affirmed that one of the problems, when comparing the results of studies involving older adults, is the difficulty in accurately define their functional capabilities. Lord, Sherrington, Menz, & Close (2007b) also point out the need of further research, especially in gait activities involving obstacles (e.g. dealing with stairs), in order not only to determine gait pattern compensations in the elderly, but also to identify the physiological factors responsible for those compensations.
The main aim of this thesis is to provide a better understanding on the determinant factors for falling in Portuguese older adults, with a special emphasis on the biomechanical changes in gait patterns associated with functional fitness decline in this population. Our methodological approach to this problem encompasses two different levels of analysis: in the first part two epidemiological studies were conducted in order to establish the determinant factors for falling within the Portuguese older adults (1); in the second part three laboratory-based studies were performed in order to determine the influence of functional fitness levels on elderly gait patterns (2).
Cha
pter
1
1.2 Thesis goals and overview
Although the identification of risk factors and determinants of falls is one of the pillars of the World Health Organization Falls Prevention Model (World Health Organization, 2007), information about the fall determinants within the Portuguese older population is scarce. Therefore, the aim of the first part of this thesis (chapters 2 and 3) was to determine the risk factors for falling in Portuguese older adults.Specifically, the cross-sectional study “Falls in Portuguese older people: procedures and preliminary results of the study Biomechanics of locomotion in the elderly”, presented on chapter 2 of this thesis, aimed: (1) to present preliminary results regarding the field procedures (physical activity and functional fitness assessments) followed in the epidemiological studies; (2) to present a preliminary characterization of Portuguese older people regarding sociodemographic, health, physical activity and functional fitness parameters; and (3) to identify, the independent contribution of those parameters as determinants for falling in Portuguese older adults.
In order to gain a better insight about fall determinants, the study “Using a multifactorial approach to determine fall risk profiles in Portuguese older adults” (chapter 3) was performed. This approach allowed us to go further on the establishment of fallers (episodic and recurrent) risk profiles in the Portuguese population by adjusting the models for possible confounders.
Considering that the decline in physical capacity is particularly determinant for falling (Rubenstein, 2006), and that further research is needed concerning gait pattern compensations in the elderly, especially in activities involving obstacles (e.g. dealing with stairs) (Lord et al., 2007b), the second part of this thesis (chapters 4 to 6) aimed to determine the influence of functional fitness levels on elderly gait patterns.
When performing a biomechanical gait analysis, one essential step for the computation of joint kinematics and kinetics is the choice of the model used to determine the position and orientation of the body segments (segments’ pose). From the different sources of error affecting segments’ pose estimation, soft tissue artifact (STA) is
10
considered the most critical (Andriacchi & Alexander, 2000). When testing older adults, the effects of STA are especially critical, due to the decrease in muscle and skin stiffness and the increase in fat mass that occurs with ageing. The technical note showed on chapter 4 (“Sensitivity of joint kinematics and kinetics to different pose estimation algorithms and joint constraints in the elderly”) aimed to study the influence of different optimization methods used to compensate for STA on joint kinematics and kinetics. This study was essential for choosing the most appropriate kinematic model to carry out the following study.
Joint moments of force, computed with traditional inverse dynamics methods, are central parameters when performing a biomechanical analysis because they are the causes of the movement pattern. The aging process has been associated with a lower limb joint moment redistribution both during level (DeVita & Hortobagyi, 2000) and stair walking (Novak & Brouwer, 2011). However, there is still some controversy about the kinetic strategies adopted by the elderly during these tasks. The study “Gait patterns in the elderly: the influence of functional fitness level”, presented on chapter 5, aimed to contribute for the characterization of sagittal and frontal lower limb joint moment patterns in three different functional tasks (level walking, stair ascent and stair descent) within a group of older adults; and to verify the influence of subjects’ functional fitness level in those task patterns.
Although the inverse dynamics approach for the quantification and description of joint moment patterns is a valuable tool to perform a biomechanical analysis, the cause-effect relation between kinetics and kinematics, when using this method, is inferred by comparison with normative data. The mentioned approach also assumes that the generated net moments crossing a joint are the primary controllers of the movement at that joint, but it was already shown that the joint moments produced by muscles that span a certain joint will generate acceleration in all body joints (Zajac & Gordon, 1989). Induced acceleration analysis is an interpretative method based on the principles outlined by Zajac and Gordon (1989), which allows the direct quantification of joint moments (and/or individual muscles) contribution to the acceleration of each body joint (and/or center of mass). This technique has proven to be a powerful clinical assessment tool (Goldberg & Kepple, 2009; Siegel, Kepple, & Stanhope, 2006) and thus, has been gaining popularity within the biomechanics research community. Chapter 6 is a preliminary study whose purpose was to quantify the potential changes
Cha
pter
1
in the contributions of lower limb joint moments and gravity to center of mass forward progression and support in elderly gait patterns, using induced acceleration analysis.
In the final chapter of this thesis (chapter 7) the main findings of each study are summarized and discussed, as well as the general methodological issues concerning those studies. Recommendations for future research are also provided.
References
Andriacchi, T. P., & Alexander, E. J. (2000). Studies of human locomotion: past, present and future.
Journal of biomechanics, 33(10), 1217–1224.
Begg, R. K., & Sparrow, W. A. (2000). Gait characteristics of young and older individuals negotiating a raised surface: implications for the prevention of falls. The Journals of Gerontology. Series A,
Biological Sciences and Medical Sciences, 55(3), M147–154.
Berg, W. P., Alessio, H. M., Mills, E. M., & Tong, C. (1997). Circumstances and consequences of falls in
independent community-dwelling older adults. Age and Ageing, 26(4), 261–268.
doi:10.1093/ageing/26.4.261
Collins, K., Rooney, B. L., Smalley, K. J., & Havens, S. (2004). Functional fitness, disease and independence in community-dwelling older adults in western Wisconsin. WMJ: official publication
of the State Medical Society of Wisconsin, 103(1), 42–48.
DeVita, P., & Hortobagyi, T. (2000). Age causes a redistribution of joint torques and powers during gait.
Journal of Applied Physiology, 88, 1804–1811.
Goldberg, S. R., & Kepple, T. M. (2009). Muscle-induced accelerations at maximum activation to assess individual muscle capacity during movement. Journal of Biomechanics, 42(7), 952–955. doi:10.1016/j.jbiomech.2009.01.007
Graafmans, W. C., Ooms, M. E., Hofstee, H. M., Bezemer, P. D., Bouter, L. M., & Lips, P. (1996). Falls in the elderly: a prospective study of risk factors and risk profiles. American journal of epidemiology,
143(11), 1129–1136.
Hortobágyi, T., & DeVita, P. (1999). Altered movement strategy increases lower extremity stiffness during stepping down in the aged. The Journals of Gerontology. Series A, Biological Sciences and
Medical Sciences, 54(2), B63–70.
Hortobágyi, T., Mizelle, C., Beam, S., & DeVita, P. (2003). Old adults perform activities of daily living near their maximal capabilities. The Journals of Gerontology. Series A, Biological Sciences and
Medical Sciences, 58(5), M453–460.
Kerrigan, D. C., Todd, M. K., Della Croce, U., Lipsitz, L. A., & Collins, J. J. (1998). Biomechanical gait alterations independent of speed in the healthy elderly: evidence for specific limiting impairments.
Archives of Physical Medicine and Rehabilitation, 79(3), 317–322.
Kressig, R. W., Gregor, R. J., Oliver, A., Waddell, D., Smith, W., O’Grady, M., … Wolf, S. L. (2004). Temporal and spatial features of gait in older adults transitioning to frailty. Gait & Posture, 20(1), 30–35. doi:10.1016/S0966-6362(03)00089-4
Lark, S. D., Buckley, J. G., Bennett, S., Jones, D., & Sargeant, A. J. (2003). Joint torques and dynamic joint stiffness in elderly and young men during stepping down. Clinical Biomechanics (Bristol,
12
Lark, S. D., Buckley, J. G., Jones, D. A., & Sargeant, A. J. (2004). Knee and ankle range of motion during stepping down in elderly compared to young men. European Journal of Applied Physiology, 91(2-3), 287–295. doi:10.1007/s00421-003-0981-5
Lawrence, R. H., & Jette, A. M. (1996). Disentangling the disablement process. The Journals of
Gerontology. Series B, Psychological Sciences and Social Sciences, 51(4), S173–182.
Lord, S. R., Sherrington, C., Menz, H. B., & Close, J. C. T. (2007a). Epidemiology of falls and fall-related injuries. Em Falls in older people: risk factors and strategies for prevention (2nd ed., pp. 3–25). Cambridge ; New York: Cambridge University Press.
Lord, S. R., Sherrington, C., Menz, H. B., & Close, J. C. T. (2007b). Gait characteristics and falls. Em Falls
in older people: risk factors and strategies for prevention (2nd ed., pp. 50–69). Cambridge ; New
York: Cambridge University Press.
Morey, M. C., Pieper, C. F., & Cornoni-Huntley, J. (1998). Physical fitness and functional limitations in community-dwelling older adults. Medicine and Science in Sports and Exercise, 30(5), 715–723. Nagi, S. (1991). Disability concepts revisited: Implication for prevention. Em A. M. Pope & A. R. Tarlov
(Eds.), Disability in America: toward a national agenda for prevention (pp. 1309–1327). Washington, D.C: National Academy Press.
Novak, A. C., & Brouwer, B. (2011). Sagittal and frontal lower limb joint moments during stair ascent and
descent in young and older adults. Gait & Posture, 33(1), 54–60.
doi:10.1016/j.gaitpost.2010.09.024
Pluijm, S. M. F., Smit, J. H., Tromp, E. A. M., Stel, V. S., Deeg, D. J. H., Bouter, L. M., & Lips, P. (2006). A risk profile for identifying community-dwelling elderly with a high risk of recurrent falling: results of a 3-year prospective study. Osteoporosis international: a journal established as result of
cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA, 17(3), 417–425. doi:10.1007/s00198-005-0002-0
Prince, F., Corriveau, H., Hébert, R., & Winter, D. A. (1997). Gait in the elderly. Gait & Posture, 5, 128– 135.
Rantakokko, M., Mänty, M., & Rantanen, T. (2013). Mobility decline in old age. Exercise and Sport
Sciences Reviews, 41(1), 19–25. doi:10.1097/JES.0b013e3182556f1e
Reeves, N. D., Spanjaard, M., Mohagheghi, A. A., Baltzopoulos, V., & Maganaris, C. N. (2008). The demands of stair descent relative to maximum capacities in elderly and young adults. Journal of
Electromyography and Kinesiology, 18(2), 218–227. doi:10.1016/j.jelekin.2007.06.003
Reeves, N. D., Spanjaard, M., Mohagheghi, A. A., Baltzopoulos, V., & Maganaris, C. N. (2009). Older adults employ alternative strategies to operate within their maximum capabilities when ascending
stairs. Journal of Electromyography and Kinesiology, 19(2), e57–e68.
doi:10.1016/j.jelekin.2007.09.009
Rikli, R. E., & Jones, C. J. (1997). Assessing physical performance in independent older adults: issues and guidelines. Journal of Aging and Physical Activity, 5, 244–261.
Rikli, R. E., & Jones, C. J. (1999). Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. Journal of Aging and Physical Activity, 7, 129–161.
Rubenstein, L. Z. (2006). Falls in older people: epidemiology, risk factors and strategies for prevention.
Age and Ageing, 35(Supplement 2), ii37–ii41. doi:10.1093/ageing/afl084
Siegel, K. L., Kepple, T. M., & Stanhope, S. J. (2006). Using induced accelerations to understand knee stability during gait of individuals with muscle weakness. Gait & Posture, 23(4), 435–440. doi:10.1016/j.gaitpost.2005.05.007
Simon, S. R. (2004). Quantification of human motion: gait analysis—benefits and limitations to its
application to clinical problems. Journal of Biomechanics, 37(12), 1869–1880.
Cha
pter
1
Spirduso, W. W., Francis, K. L., & MacRae, P. G. (2005). Physical function of older adults. Em Physical
dimensions of aging (2nd ed., pp. 261 – 286). Champaign, IL: Human Kinetics.
Stalenhoef, P. A., Diederiks, J. P. M., Knottnerus, J. A., Kester, A. D. M., & Crebolder, H. F. J. M. (2002). A risk model for the prediction of recurrent falls in community-dwelling elderly: a prospective cohort study. Journal of Clinical Epidemiology, 55(11), 1088–1094.
Startzell, J. K., Owens, D. A., Mulfinger, L. M., & Cavanagh, P. R. (2000). Stair negotiation in older people: a review. Journal of the American Geriatrics Society, 48(5), 567–580.
Stel, V. S., Smit, J. H., Pluijm, S. M. F., & Lips, P. (2003). Consequences of falling in older men and women and risk factors for health service use and functional decline. Age and Ageing, 33(1), 58– 65. doi:10.1093/ageing/afh028
Tinetti, M. E., & Williams, C. S. (1997). Falls, injuries due to falls, and the risk of admission to a nursing
home. The New England journal of medicine, 337(18), 1279–1284.
doi:10.1056/NEJM199710303371806
Tinetti, M. E., & Williams, C. S. (1998). The effect of falls and fall injuries on functioning in community-dwelling older persons. The journals of gerontology. Series A, Biological sciences and medical
sciences, 53(2), M112–119.
Todd, C., & Skelton, D. (2004). What are the main risk factors for falls among older people and what are
the most effective interventions to prevent these falls? (Health Evidence Network Report).
Copenhagen: WHO Regional Office for Europe. Obtido de
http://www.euro.who.int/document/E82552.pdf
Tromp, A. M., Pluijm, S. M., Smit, J. H., Deeg, D. J., Bouter, L. M., & Lips, P. (2001). Fall-risk screening test: a prospective study on predictors for falls in community-dwelling elderly. Journal of clinical
epidemiology, 54(8), 837–844.
U.S. Department of Health and Human Services. (1996). Physical Activity and Health: A Report of the
Surgeon General. Atlanta. GA: U.S. Department of Health and Human Services, Centers for
Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion.
Vandervoort, A. A. (2002). Aging of the human neuromuscular system. Muscle & Nerve, 25(1), 17–25. Verbrugge, L. M., & Jette, A. M. (1994). The disablement process. Social Science & Medicine (1982),
38(1), 1–14.
Visser, M., Pluijm, S. M. F., Stel, V. S., Bosscher, R. J., & Deeg, D. J. H. (2002). Physical activity as a determinant of change in mobility performance: the Longitudinal Aging Study Amsterdam. Journal
of the American Geriatrics Society, 50(11), 1774–1781.
Voermans, N. C., Snijders, A. H., Schoon, Y., & Bloem, B. R. (2007). Why old people fall (and how to stop them). Practical Neurology, 7(3), 158–171. doi:10.1136/jnnp.2007.120980
Wilken, J. M., Rodriguez, K. M., Brawner, M., & Darter, B. J. (2012). Reliability and minimal detectible change values for gait kinematics and kinetics in healthy adults. Gait & Posture, 35(2), 301–307. doi:10.1016/j.gaitpost.2011.09.105
Winter, D. A. (1991). The Biomechanics and Motor Control of Human Gait: Normal, Elderly and
Pathological. Waterloo: University of Waterloo Press.
Winter, D. A., Patla, A. E., Frank, J. S., & Walt, S. E. (1990). Biomechanical Walking Pattern Changes in the Fit and Healthy Elderly. Physical Therapy, 70(6), 340–347.
World Health Organization. (2002). Active ageing: a policy framework (World Health Organization.). Geneva.
World Health Organization. (2007). WHO global report on falls prevention in older age. Geneva, Switzerland: World Health Organization.
14
Yamashita, T., Noe, D. A., & Bailer, A. J. (2012). Risk Factors of Falls in Community-Dwelling Older
Adults: Logistic Regression Tree Analysis. The Gerontologist, 52(6), 822–832.
doi:10.1093/geront/gns043
Zajac, F. E., & Gordon, M. E. (1989). Determining muscle’s force and action in multi-articular movement.
2
Falls in Portuguese older people:
Procedures and preliminary results
of the study Biomechanics of
Locomotion in the Elderly
Vera Moniz-Pereira, Filomena Carnide, Maria
Machado, Helô André and António Veloso
Based on:
ACTA REUMATOL PORT. 2012;37:324-332
16
Abstract
Aim: The aims of this study were to: (1) present preliminary results about the evaluation of the procedures (physical activity and functional fitness tests) followed in the baseline period of our research program; (2) present a preliminary characterization of Portuguese older people regarding sociodemographic, health, physical activity and functional fitness variables; (3) identify, within those parameters, the ones which are determinant to predict falls in Portuguese older adults.
Material and Methods: 647 subjects aged over 65 years were randomly recruited in
Lisbon and Tagus Valley area. Trained interviewers administered: (1) a standardized questionnaire that included sociodemographic, health and falls parameters; (2) YPAS questionnaire for PA and (3) six FF tests (30sec Chair-Stand and 8 foot Up&Go from SFT battery and items 4-7 from FAB Scale).
Reproducibility and convergent validity of the FF and PA tests were determined by ICC and Pearson correlations. Logistic regression analysis was used to model fall occurrence considering three different fall groups (non-fallers (NF: 0 falls), episodic fallers (EF: 1 fall) and recurrent fallers (RF: >1 fall).
Results: FF and PA tests showed to have a good convergent validity and
reproducibility, giving us confidence about the results obtained.
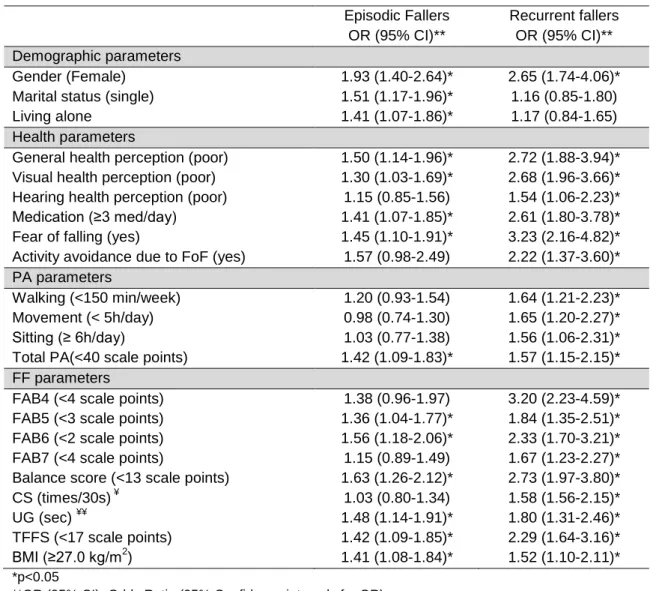
Approximately 37% of the elderly tested fell during the previous year. From these, 41% were RF. Our results showed that age is not a risk factor for falling and that health and FF variables are the most determinant factors to assess fall risk.
Conclusion: According to the results, falls might not be an inevitable consequence of
age, but instead, mainly associated with poor health and functional fitness. Moreover, PA seems to play a key role in this process, not only because a higher level of PA will lead to a better functional fitness level, but also because PA was found to be a protective factor for both episodic and recurrent falls.
Cha
pter
2
2.1 Introduction
The increase of life expectancy in the industrialized countries has raised new public health issues derived from the increment of the number of years lived by the elderly. Thus, improving elderly functional status and minimizing their disability burden, became a primary concern (Anderson & Hussey, 2000; World Health Organization, 2007). Among other things, elderly quality of life depends on their ability to perform activities of daily living (ADLs). In this sense, it is important to determine the mechanisms that can improve functionality and, consequently, quality of life in the elderly (Oztürk, Simşek, Yümin, Sertel, & Yümin, 2011).Inactivity is one of the factors that can lead to the decline in physical and psychological functions, therefore affecting the ability of people to perform ADLs. This potential impairment is especially critical for older adults(Collins, Rooney, Smalley, & Havens, 2004), whose activity levels are extremely low. Many older adults who have become increasingly sedentary may be performing ADLs at their maximum capacity being, therefore, at risk of losing independence, becoming disabled and also, at risk of falling (Gu & Conn, 2008; Shumway-Cook et al., 2009).
Fall-related morbidity and mortality rates are referred to as one of the most common and serious problems faced by the elderly (Hausdorff, Rios, & Edelberg, 2001; Hornbrook et al., 1994). About 40% of the community-living population aged over 65 years will fall at least once each year, and about 1 in 40 of them will be hospitalized (Rubenstein, 2006). Nevertheless, the problem of falls in the elderly is clearly more complex than a high incidence issue. Young children and athletes have higher fall rates than older adults (Mertz, Lee, Sui, Powell, & Blair, 2010) but, as older people have higher incidence of chronic diseases (CD), like osteoporosis, reduced bone density and age-related physiological changes, the likelihood of an injury increases, making even a relatively mild fall particularly dangerous (Rubenstein, 2006).
Although most falls do not cause serious injury, 5% of older people suffer major injuries such as fractures, head trauma and other musculoskeletal and soft tissue injuries (van Dieën, Pijnappels, & Bobbert, 2005). Moreover, fall rates and their associated
18
complications are reported to rise steadily with age, being about two times higher for persons aged over 75 years (Rubenstein, 2006; van Dieën et al., 2005).
Thus, identifying old people who are at risk of falling seems to be a key step to establish interventions aiming at the prevention or the delay of physical frailty of that population.
Many studies have been done (e.g. Chan et al., 2007; Graafmans et al., 1996; Neyens et al., 2006; Pluijm et al., 2006; Todd & Skelton, 2004; Voermans, Snijders, Schoon, & Bloem, 2007) to identify the risk factors for falling. Among others, the most referenced risk factors for falling are: age, gender, specific chronic diseases, impaired mobility, balance and gait, muscle weakness, sedentary behaviour, cognitive impairment, fear of falling, visual impairment, medication intake, health perception and history of falling.
Although there is a general agreement regarding to what are the main risk factors for falling, the mentioned studies were done using different tools, procedures and variables definitions (e.g fall, level of physical activity or functional level definitions) that are not always well clarified, making therefore difficult the comparison between studies. Moreover, no study was done to verify these relations in Portuguese older adults.
Therefore, this paper aims to: (1) present preliminary results about the evaluation of the procedures (physical activity (PA) and functional fitness (FF) tests) followed during baseline period of the project "Biomechanics of Locomotion in the Elderly: Determinants in Fracture Risk Reduction"; (2) present a preliminary characterization of Portuguese older people regarding sociodemographic, health, PA and FF parameters and (3) identify, within the previous mentioned variables, the ones which are determinant to predict falls in Portuguese older adults.
Cha
pter
2
2.2 Materials and Methods
Sample Recruitment
The first stage of this project has enrolled 647 from 870 subjects, aged 65 years or older, recruited in Lisbon and Tagus Valley area. The subjects were randomly selected from day care centres, senior schools, gyms and health promotion community events. To obtain a representative sample, a multistage stratified sampling design was used.
The institutions were selected within a 50 km distance from the Faculty of Human Kinetics, Technical University of Lisbon. The choice of this area for sample recruitment was done, not only due to geographic proximity, but also because the selected area allowed us to establish a cohort of representative elderly subjects from the Lisbon region by encompassing people from both urban and country side areas.
The mentioned institutions were selected randomly from a list available on the website of the Directorate-General of Health (Ministry of Health).
The general inclusion criteria were: to be 65 years of age or older, to correctly understand the Portuguese language, to be autonomous, to not have dementia, cognitive and cerebrovascular impairments and to not be recovering from an acute illness. For Functional Fitness (FF) tests, the following inclusion criteria were added: to be able to walk independently and/or without assistance of a walking aid and not to have a hip or knee prosthesis.
Immediately prior to data collection, all participants were informed about the study, accepted to participate and signed the informed consent. The Ethics Committee of Faculty of Human Kinetics, Technical University of Lisbon, approved all the study protocols.
Health and Falls interview
Trained examiners administered a structured and standardized questionnaire, by interview, that included sociodemographic characteristics, health, vision and hearing
20
perception status, medical history (medical visits, hospitalizations, surgeries), medication intake (total and number for each disease, with specification of the drug name) fear of falling (FOF), activity avoidance due to FOF, fall prevalence (in the previous year) and falls characteristics (location, circumstances and consequences of, at most, 3 of the reported falls). A fall was defined as “an unexpected event in which the participant comes to rest on the ground, floor or lower level” (Lamb, Jørstad-Stein, Hauer, & Becker, 2005). The mean duration of the interview was 12 minutes.
Physical activity interview
Physical activity was assessed by interview, following the health questionnaire, with the Yale Physical Activity Questionnaire – YPAS (Dipietro, Caspersen, Ostfeld, & Nadel, 1993). This tool reports to a typical week during the month prior to evaluation and is divided in two parts:
(1) YPAS activity checklist allows to obtain detailed information about the type, duration (Hrs/week) and intensity (Kcal/min) of the typical activities carried out by the elderly (housework, exercise, caretaking, yard work and recreational activities).
(2) YPAS activity scores allow to assess an index of intensity of five distinct PA dimensions: (a) the vigorous index (VI) combines the frequency and the duration engaged in activities that cause large increases in breathing rate and heart rate, sweating or leg fatigue; (b) the walking index (WI) reports the frequency and the duration of walking activities that last at least 10 minutes without stopping or making an vigorous effort; (b) the moving index (MI) comprehends the time spent daily in activities with movement while standing, including walking, (c) the standing
index (SI) evaluates the daily time spent in activities while standing but without
movement; and, (d) the sitting index (STI) assesses daily time spent in the seated position. Partial scores are multiplied by the specific weighting factor to calculate the individual indexes and then summed to determine the summary index of activity (SumI).
The mean duration of interview was 13 minutes. The subjects who answerd the interview and fulfilled the inclusion criteria were then invited to participate in the FF assessment.
Cha
pter
2
Functional Fitness Assessment
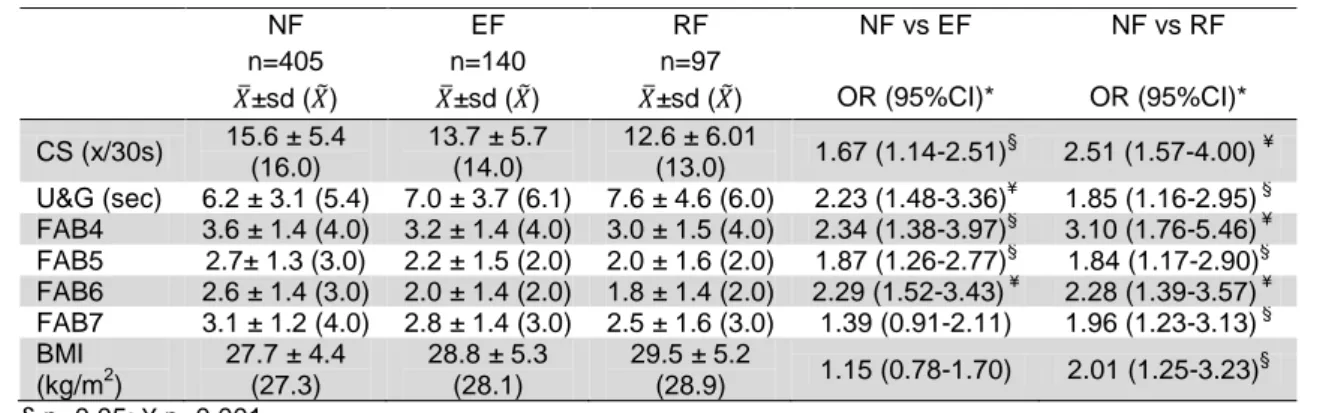
Several FF tests for older adults have been developed and reported (Berg, Wood-Dauphinee, & Williams, 1995; Duncan, Weiner, Chandler, & Studenski, 1990; Rikli & Jones, 1999; Rose, Lucchese, & Wiersma, 2006). Among these, we have selected 6 for this study (30sec Chair-Stand (CS) and 8 foot Up and Go (UG) from Senior Fitness test (Rikli & Jones, 1999) and items 4 to 7 from Fullerton Advance Balance Scale(Rose et al., 2006)), based on their reported ability to discriminate fallers and detect age functional decline in community-dwelling older adults (Hernandez & Rose, 2008; Rose, Jones, & Lucchese, 2002), as well as their feasibility in clinical and exercise field. The first two tests (CS and UG) assess lower limb strength, power and mobility, while the last four measure static (FAB6 – stand on one leg – and FAB7 – stand on a foam with eyes closed) and dynamic (FAB4 – step up and over a bench – and FAB5 – tandem walk along a line) balance. Besides the referred tests, during FF assessment, height and weight were also collected for Body Mass Index (BMI) calculation.
Before testing, a demonstration was performed by the examiner and the subjects completed one or two practice trials.
At the end of the each session, participants received feedback, through a written report, concerning their test results.
The duration of FF assessment was on average approximately 12 minutes.
Examiners Training
For all the tests, forty examiners were trained by the research team over a total period of 51 hours (33 hours of theoretical and practical training and 18 hours of field assessments).
The examiners received an instruction manual for field data collection containing: (1) a script with the questions included in both questionnaires and the most common difficulties of the subject when responding to the questionnaires; (2) basic instructions on conducting the interview; (3) basic FF test instructions, according to the respective authors method (Rikli & Jones, 1999; Rose et al., 2006).
22
All examiners were supervised while interviewing and applying FF test to older subjects, who kindly offered to be tested, by at least two members of the research team. At the end of the work sessions, a verbal feedback was given to each examiner.
Examiners were also asked to classify the performance of the same older subject in all FF tests, presented through video recording during one of the classes. These results were compared between examiners, in order to perform an inter-observer analysis, and with the assessment made by two research team members, experts in Health & Exercise, to assess the convergent validity of these tests. For the UG and the CS tests the convergent validity was also assessed by comparing examiners assessment with accelerometer data (xyzPlux triaxial accelerometer sensor, with a dynamic range of ±3g) that was collected from 33 elderly subjects during the field assessments.
Besides answering the PA questionnaire, 98 of the subjects worn uniaxial accelerometers (Actigraph Model 7194) and the results were compared to assess the convergent validity of the questionnaire. Furthermore, the reproducibility of this test was assessed using the test-retest results of 31 subjects.
Statistical analysis
Reproducibility and convergent validity for PA and FF field tests were determined respectively by Intra-class correlation (ICC-parallel; one-way random effect model; 95%CI) and Pearson’s correlation coefficient.
A cross-sectional study was designed and the subjects were divided in three different groups according to fall prevalence: non-fallers (NF), subjects who did not report any falls during the previous year, episodic fallers (EF), those who reported to have fallen only once during the previous year, and recurrent fallers (RF), the ones that fell twice or more times during the previous year. Statistical analysis was done according to these groups.
The characterization of Portuguese older adults in matters of sociodemographic, health, PA and FF variables was performed through basic descriptive statistics.The identification of main factors for falling in Portuguese older adults was evaluated via Mantel–Haenszel chi-square, t-Student or Mann-Whitney tests, with the significance of the results set at p<0.05. The Spearman correlation coefficient was also used to
Cha
pter
2
investigate associations among quantitative independent variables. Finally, binary logistic regression analysis was used to model fall occurrence (NFvsF, FvsRF and FvsRF). Because risk factors must be easily and quickly measurable, for use in clinical/exercise settings, independent variables were dichotomized throughout their median value, as normality could not be assumed by Kolmogorov-Smirnov test for continuous variables. BMI was the only exception, being classified as good between 22.0 and 26.9 Kg/m2 and poor for results ≥27.0 Kg/m2 (Cervi, Franceschini, & Priore, 2005). Values below its median were classified as “poor level”, and values equal or greater than the median were classified as “good level”, with the exceptions of the number of medications, the sitting index and the 8 foot Up and Go test.
All the analyses were performed using PASW 18.0.
2.3 Results
Reproducibility and convergent validity of Functional Fitness and Physical activity tests
The reproducibility results indicate significantly high inter-examiners correlations for all FF tests. The inter-observer ICC for each item ranged from 0.588 to 0.965 while the ICC for average measures ranged from 0.938 to 0.998. According to the literature (Szklo, 2000; Pynsent, 2001), our results show a very good reproducibility for most of FF testes. The exceptions were observed for CS and FAB5 tests, which had a satisfactory level of reproducibility.
The Pearson correlation coefficients associating both CS and U&G tests and accelerometry were strong and highly significant (CS: 0.83, U&G: 0.92, p<0.001), confirming the good results for convergent validity of these tests.
The test-retest results for YPAS questionnaire were very good for SI (ICC=0.76) and MI (ICC=0.79). For other indexes the results were satisfactory with ICC ranging from 0.620 to 0.73 (Pynsent, 2001; Szklo, 2000). The results of the convergent validity using accelerometry (Copeland & Esliger, 2009) showed a positive correlation among active indexes (0.307<rho<0.373; 0.004<p<0.001) and a negative correlation with the SIT (rho=-0.469; p<0.001).