BrazJOtorhinolaryngol.2016;82(3):365---367
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Pulsatile
tinnitus
related
to
progestin
from
intrauterine
device
夽
Zumbido
pulsátil
relacionado
a
progestágeno
de
dispositivo
intrauterino
Ektor
Tsuneo
Onishi
∗,
Bruno
Borges
de
Carvalho
Barros,
Fernando
Takashi
Hirose,
Fernando
Kaoru
Yonamine
DivisionofOtologyandOtoneurology,DepartmentofOtolaryngologyandHeadandNeckSurgery,EscolaPaulistadeMedicina, UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
Received11March2015;accepted11April2015 Availableonline7September2015
Introduction
Patientswithpulsatiletinnitus(PT)shouldbeevaluatedwith differentcriteriathanthosesufferingsensorineuraltinnitus, as this feature suggests, in most cases, a specific etiol-ogy (Table 1). The most common cause of vascular PT is atheroscleroticdisease duetoendovascularflow changes, passing from a laminar toturbulent state and generating thesound perceived bythe patient.1,2 The use of contra-ceptivemethods hasbecomepopular,andthesideeffects ofhormoneexposureshouldalwaysbeconsidered.3
The aimof thisstudyis toreportthe caseof afemale patient who had pulsatile tinnitus related to a progestin (levonorgestrel)-containingintrauterinedevice.
Case
report
CLP,a32-year-oldCaucasianwomanborninSãoPaulo,for about1yearhadexperiencedpulsatiletinnitusintheright
夽 Pleasecitethisarticleas:OnishiET,BarrosBBC,HiroseFT,
Yon-amineFK.Pulsatiletinnitusrelatedtoprogestinfromintrauterine
device.BrazJOtorhinolaryngol.2016;82:365---7.
∗Correspondingauthor.
E-mail:[email protected](E.T.Onishi).
earthatwassynchronous withherheartbeat. Thepatient relatedtheonsetofsymptomstomonthsafterthebirthof herson.Shedeniedheadtrauma,dizzinessorhearingloss; sheexperienceddifficultysleeping duetotheintensity of thetinnitus(score=8onavisualanaloguescale,VAS),and reporteddiscreeteveningswellingofherlowerlimbs.Asto herpersonal history,thispatientdeniedsystemicdiseases suchashypertension,diabetes, hyper-or hypothyroidism. Thepatienthadanintrauterinedevice(IUD)placedabout6 monthspreviously.
Onphysicalexamination,thepatientwasnormotensive andwithnormalbilateralotoscopy.Shereporteddecreased tinnitusduring cervical compression maneuver over large vesselsontheright,butwithnochangeonheadrotation. Cervicalauscultation revealed nothrills or murmurs with thestethoscope. Laboratory workup:hemoglobin 14g/dL, hematocrit41%,normallevelsfortotalcholesterolandits fractions,triglyceridesandthyroidhormones.Thispatient exhibited normal pure tone and speech audiometry and impedancetests.
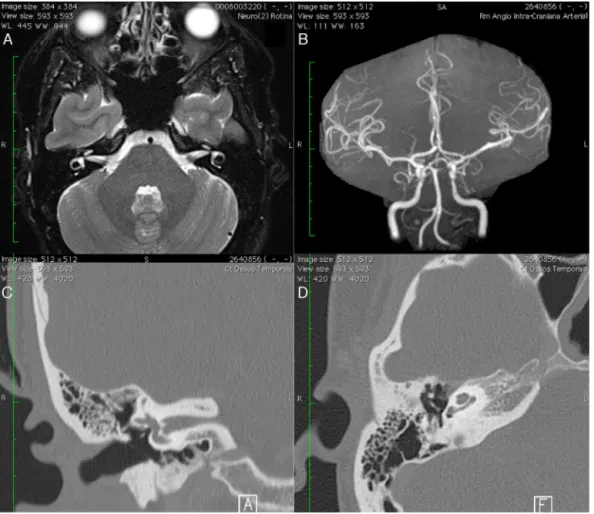
An imaging evaluation (Doppler ultrasound of carotid and vertebrals, tomography of temporal bones, magnetic resonance of inner ears and cranial angioresonance) was performed,withnoidentifiedabnormalities(Fig.1).
After the most frequent causes of vascular PT were ruled out, it was hypothesized a relationship with her progestin-containing intrauterine device. Our patient
http://dx.doi.org/10.1016/j.bjorl.2015.04.005
1808-8694/©2015Associac¸˜aoBrasileirade OtorrinolaringologiaeCirurgiaC´ervico-Facial.Published byElsevierEditoraLtda.Allrights
366 OnishiETetal.
Table1 Causesofpulsatiletinnitus.
Vascularcauses
Arterial Atheroscleroticdisease;aberrant carotidinmiddleear;dehiscence ofinternalcarotidinthemiddle ear;persistentstapedialartery; intrameatalvascularloop Venous Venoushum;dehiscentorhigh
jugularbulbinmiddleear Tumors Paraganglioma;arteriovenous
malformations
Muscularcauses
Myoclonus Softpalate;pharyngealmuscles; middleearmuscles
Eustachian tube
PatentEustachiantube
Thirdwindow syndrome
Superiorsemicircularcanal dehiscence;vestibularaqueduct syndrome;perilymphaticfistula
receivedinstructions regarding the cause of tinnitus,and was treated with a beta-blocker (metoprolol 50mg/day) with significant improvement of symptoms. The patient started to sleepbetter (score=3 for tinnitus in VAS) and
discontinuedthemedicationaftertwomonths,resultingin increasedintensity oftinnitus.Becauseofthepersistence ofconsiderablediscomfort,removaloftheIUDwascarried out,withcompleteremissionoftinnitus.
Discussion
Levonorgestrel is a progestin (synthetic progesterone) widely usedashormonalcontraceptive, withefficacy and safetyalreadydefined.Theagentcanbeadministeredorally orasanintrauterineimplant.4
Progesteroneinlargerquantitiesincreasesthe reabsorp-tionof sodium, chloride andwater indistal renal tubules withconsequentchangeinthebloodcrasisandinits dynam-icsandendovascularflow.A searchwithimagingmethods (p.ex.,Dopplerultrasound,MRIandangio-MR)isthemost appropriatechoice.2,5 Inthepresent case, theabsenceof lesionsthatcouldjustifythepresenceofPTreinforcedthe hypothesisofhemodynamicchange,secondarytotheuseof levonorgestrel.
The inner earis verysusceptible tohormonal changes andfluctuations;nevertheless,wedonotbelievethatthisis themechanismoftinnitusgeneration,sincespecific proges-teronereceptorshavenotbeenidentifiedinthecochlea.3 The use of oral contraceptiveswasassociated with vesti-bulardisorders,withalterationsin vestibularexamination
Pulsatiletinnitusrelatedtoprogestinfromintrauterinedevice 367
and tinnitus,5 but our search did not find studies with intrauterinedevicesintheliteraturereview.
The greatdiversity ofdiagnosesrelated toPTrequires a thorough investigation; and this is time-consuming and demands financialresources.1,6 The AmericanAcademyof Otolaryngology(AAO-HNS)reviewrecommendsinvestigation incasesofunilateraltinnitus,pulsatiletinnitus,focal neu-rological abnormalities (focal neurological symptoms), or asymmetrichearingloss.7
In this case, of those factors that would be associ-atedwiththegenerationofvascularpulsatiletinnitus,we emphasizehypertension,atherosclerosis,thyroidhormones or bloodcrasischanges,andchangesinendovascularflow dynamics caused by fluid retention related to progestin. Consideringthatclinicalandancillary(laboratoryand imag-ing) tests ruled out primary causes, and in view of an improvementofsymptomswithalow-dosebeta-blocker,we suggesteddiscontinuationofthecontraceptiveagent.With tinnitus improvement after the removal of the intrauter-inedevice, werealizedthat theprogestin wasassociated withthe generation of theproblem, evenwithout having reintroducedthedrugtoevaluateitseffect.
Final
considerations
The investigation of PT with imaging methods should be clear-sighted,insearch ofthat injuryjustifying its gener-ation, andwith the choice of a specific treatment. Good clinicaldataanda judicioushistoryareequallyimportant toestablishthediagnosis.Thesideeffectsofcontraceptive
medications should be considered as possible causes of pulsatiletinnitus.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Sismanis A. Pulsatile tinnitus: contemporary assessment and management. Curr Opin Otolaryngol Head Neck Surg. 2011;19:348---57.
2.MadaniG,ConnorSEJ.Imaginginpulsatiletinnitus.ClinRadiol. 2009;64:319---28.
3.Al-ManaD,CeranicB,DjahanbakhchO,LuxonLM.Hormonesand theauditorysystem:areviewofphysiologyandpathophysiology. Neuroscience.2008;153:881---900.
4.Jensen JT. Contraceptive and therapeutic effects of the lev-onorgestrel intrauterine system: an overview. ObstetGynecol Surv.2005;60:604---12.
5.Mitre EI, Figueira AS, Rocha AB, Alves SMC. Avaliac¸ões audiométrica e vestibular em mulheres que utilizam o métodocontraceptivohormonaloral.RevBrasOtorrinolaringol. 2006;72:350---4.
6.ShweelM, HamdyB. Diagnosticutility ofmagnetic resonance imaging and magnetic resonance angiography in the radio-logical evaluation of pulsatile tinnitus. Am J Otolaryngol. 2013;34:710---7.