SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Arthroscopic
subcapital
realignment
osteotomy
in
chronic
and
stable
slipped
capital
femoral
epiphysis:
early
results
夽
Bruno
Dutra
Roos
∗,
Marcelo
Camargo
de
Assis,
Milton
Valdomiro
Roos,
Antero
Camisa
Júnior,
Ezequiel
Moreno
Ungaretti
Lima,
Rodolfo
Cavanus
Pagani
UniversidadedePassoFundo,FaculdadedeMedicina,HospitalOrtopédicodePassoFundo,PassoFundo,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1February2016 Accepted29March2016
Availableonline29December2016
Keywords:
Epiphyses,slipped Hip
Femurhead Arthroscopy Child
a
b
s
t
r
a
c
t
Objective:Thisstudyaimedtoevaluatetheclinicalandradiographicoutcomes,aswellas
thecomplicationsofarthroscopicsubcapitalrealignmentosteotomyinchronicandstable slippedcapitalfemoralepiphysis(SCFE).Asindicatedbytheliteraturereview,thisisthe firsttimethistypeofarthroscopicosteotomywasdescribed.
Methods:BetweenJune2012andDecember2014,sevenpatientsweresubmittedto
arthro-scopicsubcapitalrealignmentosteotomyinchronicandstableSCFE.Themeanagewas11 yearsand4months,andthemeanfollow-upperiodwas16.5months(6–36).Clinicalresults wereevaluatedusingtheModifiedHarrisHipScore(MHHS),whichwasmeasuredpre-and postoperatively.RadiographswereevaluatedusingtheSouthwickquantitativeclassification andtheepiphysis–diaphysisangle(pre-andpostoperatively).Complicationswereassessed.
Results:The meanpreoperativeMHHSwas35.8points,and97.5pointspost-operatively
(p<0.05).Radiographically,fivepatientswereclassifiedasSouthwickclassificationgrade IIandtwoasgradeIII.Themeancorrectionoftheepiphysis-diaphysisanglewas40◦.No
immediatepostoperativelycomplicationswereobserved.Onepatientpresentedfemoral headavascularnecrosis,withoutcollapseorchondrolysisatthemostrecentfollow-up(22 months)
Conclusion: Thearthroscopictechniquepresentedforsubcapitalrealignmentosteotomyin
chronicandstableSCFEshowedsatisfactoryclinicalandradiographicoutcomesina16.5 monthsfollow-upperiod.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitalOrtopédicodePassoFundo(HOPF),CirurgiadoQuadril,PassoFundo,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.D.Roos). http://dx.doi.org/10.1016/j.rboe.2016.12.007
Osteotomia
artroscópica
de
realinhamento
subcapital
no
tratamento
da
epifisiólise
proximal
do
fêmur
crônica
e
estável:
resultados
precoces
Palavras-chave:
Epífisedeslocada Quadril
Cabec¸adofêmur Artroscopia Crianc¸a
r
e
s
u
m
o
Objetivo: Avaliaros resultados clínicos e radiográficos,bem como as complicac¸ões da
osteotomiaderealinhamentosubcapitalporviaartroscópicaparatratamentodaepifisiólise proximaldofêmur(EPF)crônicaeestável,relativosaumasérieinicialdepacientes. Con-formeanálisedaliteratura,oestudoapresentaaprimeiradescric¸ãodetécnicaartroscópica dessetipodeosteotomia.
Métodos: Entre junhode2012a dezembrode2014,sete pacientesforamsubmetidos à
osteotomiaderealinhamentosubcapitalporviaartroscópicaparatratamentodaEPFcrônica eestável.Aidademédiadospacientesfoide11anosequatromeses.Oseguimentomínimo foideseisa36meses(médiade16,5meses).Ospacientesforamavaliadosclinicamente deacordocomoHarrisHipScoremodificadoporByrderadiograficamenteconformea classificac¸ãoquantitativadeSouthwickeoânguloepifisio-diafisário.Complicac¸ões pós-operatóriasforamanalisadas.
Resultados: Comrelac¸ãoàavaliac¸ãodoescoreclínicoHarrisHipScoreModificadoporByrd,
observou-semédiapré-operatóriade35,8pontosepós-operatóriade97,5pontos(p<0,05). Radiograficamente,cincopacientesforamclassificadoscomograuIIedoiscomograuIII deSouthwick.Observou-secorrec¸ãomédiadoânguloepifisio-diafisáriode40o.Nãohouve complicac¸õespós-operatóriasimediatas.Umpacienteevoluiucomnecroseavascularda cabec¸afemoral,semcolapsooucondrólisenoúltimoseguimento(22meses).
Conclusão:AtécnicaartroscópicaapresentadapelosautoresparatratamentodaEPFcrônica
eestávelresultouemmelhoriaclínicaeradiográficadospacientesnestasérieinicial. ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Slippedcapitalfemoralepiphysis(SCFE)isthemostcommon diseaseoftheadolescenthip, withanestimatedfrequency of10.8per100,000individuals.1Recentstudiesonthe
biome-chanicsoffemoroacetabularimpingement(FAI)indicatethat small anatomical deformities that may arise from SCFE potentiallycausepermanentacetabularchondraldamage,2,3
leadingtoearlyosteoarthritis.
ThereisnoconsensusregardingthebestSCFEtreatment option,especiallyconsideringhigh-gradeslips(gradesIIand IIIofthe Southwick classification).4 Someauthors indicate
treatmentwithinsitufixationinthesecases,becausethis procedure has a low complication rate. They believe that the residual hip deformity remodelsduring growth allow-ingproperfunction.5,6Others,includingthepresentauthors,
indicatecorrectingthedeformitysite(subcapitalrealignment osteotomy)inorder to achieve ananatomical reductionof theepiphysisanddecreasetheriskofsubsequentchondral degeneration.7
Themaincriticism oftheauthorscontrarytotheuseof thesubcapitalrealignmentosteotomytechniqueistheriskof complicationssuchasavascularnecrosis(AVN)ofthefemoral headandchondrolysis,whichcanoccurinupto28%ofcases.8
However,thegrowingnumberofstudiesinthisareahasled toareductionincomplications.Itisessentialtoobserve tech-nicaldetailstopreservethevascularsupplyoftheepiphysis duringtheprocedure.7
Thisstudyaimedtoassess theclinicalandradiographic results and the complications of arthroscopic subcapital realignmentosteotomyasatreatmentforchronicandstable SCFEinaninitialseriesofpatients.
Accordingtoourliteraturesearch,thisisthefirst descrip-tionofarthroscopicsubcapitalrealignmentosteotomyforthe treatmentofchronicandstableSCFE.
Materials
and
methods
Proximal
B
A
L
H
FN
Lateral
Lateral
Distal Medial
Medial
Anterior
Posterior
H
FN
D
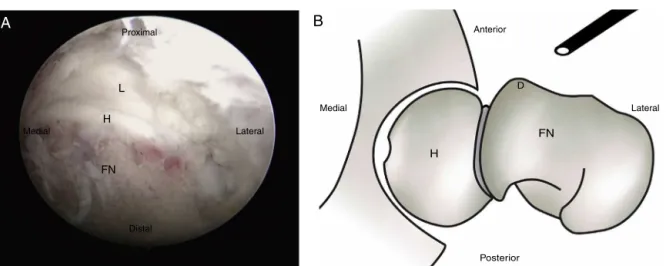
Fig.1–(A)IntraoperativeimageofhiparthroscopyforsubcapitalrealignmentinthetreatmentofchronicandstableSCFE, disclosingtheexposureofthelabrum(L),femoralhead(H),andfemoralneck(FN).(B)Axialcharacterizationofthelefthip showingthefemoralhead(H),femoralneck(FN),andCAM-typedeformityofthefemoralneck(D)resultingfromthe chronicityoftheSCFE.
Regardingclinicalaspects,thepatientswereevaluated pre-andpostoperativelyaccordingtotheHarrisHipScoremodified byByrd(MHHS)apudGuimarãesetal.9
Thecaseswere radiographicallyevaluated in the pelvic anteroposteriorandfroglegviews.Todeterminethedegree ofpreoperativeslippage,the Southwick4 criteriawereused
andthecaseswereclassifiedasgradeI(upto30◦),gradeII (30◦–60◦),orgradeIII(above60◦).Thedegreeofslipcorrection wasalsodetermined,bycomparingthepre-and postopera-tivemeasuresoftheepiphyseal-diaphysealangle4(EDA)inthe
froglegview.Duringfollow-up,thepresenceofAVNand/or chondrolysiswasanalyzed.
The statistical method used for the analysis of paired variables(MHHS,EDA)wastheWilcoxontest,considered sta-tisticallysignificantatp<0.05.
Surgical
technique
Generalanesthesiawithfemoralnerveblockwasusedtoall cases.Physicalexaminationofthehipwiththepatientunder anesthesia was used to passively assess bilateral range of motion.
Thepatientwasplacedinthesupinepositionona radiolu-centtable.Theorthopedictractiontablewasnotused,due tothe needforgreater hipmobility forthemultiple intra-operative maneuvers. The pelviswas slightly tilted to the contralateralside,andaradiolucentcushionwasplacedunder theaffectedhemipelvis.
Theanatomicalreferencesweremarkedwithan appropri-atepen.Averticallinewasdrawn fromtheanterosuperior iliacspinetowardthecenterofthepatella.Theanterior, pos-terior,andproximalbordersofthegreatertrochanterofthe femurwere marked. Theportals were positioned withthe assistanceoffluoroscopy.Thefirstportalwasthemid-anterior (MAP),whichisusedforthecamera.Subsequently,the proxi-malmid-anteriorportal(PMAP),whichistheworkingportal,is
positionedtoprovideaparallelaccesstotheproximalfemoral physis.
Thearthroscopicapproachusedforsubcapitalrealignment was extracapsular,10 followingthe accesstothe peripheral
jointcompartmentdescribedbySampson.11
Withtheaffectedlimbinaneutralpositionandafter estab-lishingthearthroscopicportals,theanteriorjointcapsuleand the iliocapsularmuscleweredissectedwithradiofrequency andshavertoobtainproperexposure.Then,aT-capsulotomy of the femoral neck was made, which could be extended as required. Subsequently, capsulectomy was made until a proper exposure of the anterior metaphysis and epiph-ysisoftheproximalfemurinits mid-lateralextensionwas obtained.Withradiofrequency,thelongitudinalopeningofthe periosteumanditsdetachmentfromthefemoralneckwere made,formingaretinacularflaptogetherwiththeepiphysis (Fig.1).
After proper exposure, an osteochondroplasty of the femoral neck-head transition is made, which allows the resection of a CAM-type deformity originated by the SCFE chronicity; it also allows a better identification of physis (Fig.2).Inmoreseveredegreesofslippage,externalrotation andlimbextensionmayberequiredtoexposetheepiphyseal plate.Theosteotomyisperformed2mmdistaltothegrowth plate(tofacilitateasubsequentneckshortening)witha spe-cificcurvedosteotomeatdifferentlocationsoftheepiphyseal plate, until the epiphysis and metaphysis are completely separated.Allpatientshadopenepiphysealplate,andno dif-ficultieswereobservedatthissurgicalstep(Fig.3).
Whenthefemoralmetaphysiswasseparatedfromthe epi-physis,thehipwasexternallyrotatedandgentlytractionedto enabletheshorteningoftheneckandgrowthplateresection usingarthroscopiccurette(Fig.4).Subsequently,thehipwas adductedtoremovethe neoformedbonetissueinthe pos-teromedialfemoralneckregion,whichcanbeanobstacleto subsequentreduction.
Proximal
B
A
H
FN Lateral
Lateral
Distal Medial
Medial
Anterior
Posterior
H
FN
Fig.2–(A)IntraoperativeimageofthelefthipafterfemoralneckosteochondroplastyforthecorrectionofCAM-type deformityshowingthefemoralhead(H)andfemoralneck(FN).(B)Axialcharacterizationofthelefthip,showingthe femoralhead(H)andfemoralneck(FN)afterfemoralneckosteochondroplastyforthecorrectionofCAM-typedeformity.
Proximal
B
A
CO
CO
FN
Lateral
Lateral
Distal Medial
Medial
Anterior
Posterior H
FN
GP
Fig.3–Intraoperativeimageofthelefthipshowingthefemoralneck(FN)andthecurvedosteotome(CO)duringneck osteotomyatthelevelofthegrowthplate.(B)Axialcharacterizationofthelefthipshowingthefemoralhead(H),femoral neck(FN),thegrowthplate(GP),andthecurvedosteotome(CO)positionedforneckosteotomy.
Proximal
B
A
AC
FN
Lateral
Lateral
Distal Medial
Medial
Anterior
Posterior
H FN
AC
Lateral Medial
Anterior
Posterior H
FN
Fig.5–Axialcharacterizationofthelefthipshowingthe femoralhead(H)andfemoralneck(FN)afterosteotomy reduction.
partially threaded cancellous screw was used for percuta-neousfixation(Figs.6–8).
Toreducethe riskofavascularnecrosisoftheproximal femoralepiphysis, atthe time ofthe neck osteotomyit is essentialtoavoiddirectingtheosteotometowardthe postero-superiorretinaculum(whichcontainstheterminalbranches ofthe medialcircumflexartery)andtowardthe lower reti-nacularartery(whichisdirectedtowardtheepiphysisoutside theretinaculartissueofthefemoralneckinthemedial Weit-brechtligament),whicharenotvisualizedduringarthroscopy. Likewise, shortening of the femoral neck and appropriate
resectionoftheposteromedialboneformationareessentialto avoidexcessivetensioningofthevesselsduringtheosteotomy reductionmaneuver.
Postoperatively, patients were hospitalized for 24h for observation ofclinical outcome.Naproxenwasused for30 days toprevent heterotopic ossification; patients were ori-entedtousecrutcheswithoutweightbearingontheoperated limbforthesameperiod,withoutrestrictionstothehiprange ofmotion.At30postoperativedays,controlradiographswere madeandfullweightbearingwasauthorized.
Results
RegardingtheassessmentoftheMHHSscore,themean pre-operativescorewas35.8points(SD=4.1,range=30.8–41.8)and themeanpostoperativescore,97.5(SD=2.9,range=93.5–100), withameanpostoperativeincreaseof61.7.Therewasa sta-tisticallysignificantdifference(p<0.05)whencomparingthe pre-andpostoperativeMHHS.9
Regardingtheradiographicevaluation,fivepatientswere preoperatively classifiedasSouthwick4 gradeIIand twoas gradeIII.Themeanpre-operativeEDA4was51.2◦ (SD=12.4, range=32◦–68◦) and postoperative, 11.2◦ (SD=5.1, range= 6◦–18◦),withameanpostoperativecorrectionof40◦.A sta-tisticallysignificant differencewasobserved(p<0.05)when comparingthepre-andpostoperativeEDA4(Table1).
There were no immediate postoperative complications. Onepatient(case2)evolvedwithAVN60daysaftersurgery, withoutcollapseorchondrolysisuntilthelastfollow-up(22 months).Thiscasehadalargeposteromedialboneformation
Fig.7–Femalepatientaged12yearsandtwomonths.Paininthelefthipforonemonth,wasabletowalkwithoutcrutches. HiplockedinIR,90◦offlexion.(A)and(B)PreoperativeradiographsshowingSouthwickgradeIISCFEtotheleft,EDA45◦.(C) and(D)Postoperativeradiographsatsixmonthsoffollow-updisclosingdeformitycorrection,EDA6◦.
inthefemoralneck,whichtheauthorsbelievetohavebeen insufficientlyresected.
Discussion
SCFEisthemostcommondiseaseoftheadolescenthip, esti-matedat10.8per100,000individuals.1Recentstudiesonthe
biomechanicsofFAIindicatethatsmallanatomical deformi-tiesofthehipthatmayarisefromSCFEareapotentialcause ofpermanentacetabularchondraldamage2andleadtoearly
osteoarthritis.
The anterior displacement of the femoral meta-physis caused by mild or moderate slips (Southwick classification)4 leads to CAM-type FAI and generates a
progressive injury on the chondrolabral junction due to excessive shear stress on the structure. In severe SCFE, the degenerative biomechanical mechanism is PINCER-type FAI, since the large deformity generates compression and primary failure of the acetabular labrum, as well as contrecoup injury in the posteroinferior cartilage of the acetabulum.8
Leunig et al.2 evidenced labral and chondral acetabular
injuries in14 patientswith unstable SCFE3 duringsurgery
using the surgical dislocation of the hip technique; they observed that these injuries occurred when the femoral metaphysiswasatorextendedbeyondtheepiphysealline. Likewise, Sink et al.,12 using the same technique,
demon-stratedthepresenceofintra-articularinjuriesin39patients withSCFE,34labraland33chondral.
Table1–Operatedcases,description,andmeanmeasurements.
Patient Gender Age(months) Side Follow-up (months)
MHHS pre-op
MHHS post-op
EDA pre-op
EDA post-op
Complications
1 M 147 L 36 30.8 93.5 62 18
2 M 130 R 22 30.8 93.5 42 6 AVN
3 M 132 R 20 34.1 100 54 8
4 M 133 L 12 37.4 97.9 56 12
5 F 134 L 10 38.5 97.9 68 18
6 M 135 L 10 41.8 100 32 11
7 F 146 L 6 37.4 100 45 6
Mean 136.7 16.5 35.8 97.5 51.2 11.2
Anterior X X Proximal Posterior Distal
∗
Fig.8–Aspectoftheincisionsshowingthearthroscopic portals(X)andtheincisionforpercutaneousfixationofthe femoralneck(*).
Dunn’s original procedure for the treatment of SCFE, describedin1964,consistedofatrapezoidalproximalfemoral neck osteotomy for further reduction and fixation of the slippage.13Theirresultswerefirstpublishedin1978,
compris-ing78hips(25acuteand48chronic);ninecasesprogressedto AVN(twocaseswithcompleteepiphysealnecrosis).14
Ganzetal.15described theuse ofthesurgicalhip
dislo-cationtechniqueinamodifiedDunnosteotomy(subcapital realignmentosteotomy)inthetreatmentofhigh-gradeSCFE.4
Accordingtotheauthors,thisapproachprovidesaccesstothe hip,preservestheepiphysealvascularsupply,andallows ade-quateresectionoftheposteromedialboneformationinthe femoralneckandsatisfactoryreductionoftheepiphysis.This makesitpossibletorestoretheanatomyoftheproximalfemur withatechniquethatreducestheriskofAVN.15
Leunigetal.16publishedthefirstresultsofthistechniquein
2007,with30hipstreatedandameanfollow-upof55months. Ofthese,24caseswereconsideredchronicslips,andnocase progressedtoAVN.Twocases(6.66%)underwentreoperation due tofailure ofthe fixation withscrews. Ziebarthet al.7
alsoretrospectivelyevaluatedthistechniquein40patients, dividedinto twocohortsfrom differentcenters,withmean follow-upsof5.4and2.2years.Thealphaangleandtheslip anglewerenormalizedinallcases,withnocasesofAVNor chondrolysis.7
Otherauthorswhohavepublishedtheirresultsontheuse ofthetechniquedescribedbyGanzshowedagreaternumber ofcomplications.Sankaretal.,17inamulticenterstudythat
evaluated27patientswithunstableSCFE3inmeanfollow-up
of22.3months,observedfourpatients(15%)requiring reope-rationforfailure offixationand sevencases(26%) ofAVN. Themeanpostoperativecourseuntilosteonecrosiswas21.4 weeks;patientswhodidnotdevelopthiscomplication pre-sented asignificantly lower clinical painscore and greater postoperativesatisfaction.17 Upasani et al.18 presentedthe
resultsof43patientstreatedwiththistechnique;60%ofcases patientshadunstableSCFE,340%wereconsideredacute,and
86%wereclassifiedassevereslip.4Thoseauthorsobserved22
complicationsin16patients;therewere15reoperationsdue
toAVN,fixationfailure,andpostoperativehipdislocation.Two patientsreceivedindicationfortotalhiparthroplasty.
TwoBrazilianstudiesreportedthearthroscopictreatment ofchronic-acutizedSCFE(unstable).3Akkarietal.19presented
theresultsoffivecasestreatedwitharthroscopictrapezoidal osteotomywithameanpreoperativeEDA4of82◦andamean postoperativeEDAof14◦;onecasedevelopedAVN.19Dobashi etal.20presentedacasereportofa12-year-oldpatientwho
underwentaDunn-typearthroscopicfemoralneckosteotomy; theslippagewascorrectedfrom70◦to30◦.
The present study presented an alternative to classical techniques of subcapital realignment for the treatment of chronicandstableSCFE3thatallowsadequateaccesstothe
hip joint andappropriatereductionofthe slippage,witha theoretical advantageofrapidrehabilitation.Theperiodof slippageevolutionisnotalimitingfactorfortheapplication ofthistechnique;nonetheless,itwasonlyindicatedincases withopenepiphysealplate.
Accordingtoaliteraturesearch,thisisthefirstdescription ofanarthroscopicsubcapitalrealignmentosteotomyforthe treatmentofchronicandstableSCFE.Theauthorsreiterate that,priortotheperformanceofthearthroscopictechnique described,itisessentialthatthesurgeonreceivesadequate traininginhiparthroscopy,aswellasexperienceinopen sub-capitalosteotomy,duetothemultipletechnicaldifficultiesof treatment.
Conclusion
Thearthroscopictechniquepresentedbytheauthorsforthe treatmentofchronicand stableproximalfemoral epiphysi-olysis resultedinclinicaland radiographicimprovementof patientsinthisinitialseries,withameanfollow-upof16.5 months.OnecaseofAVN,withoutcollapseorchondrolysis, wasobservedat22monthsoffollow-up.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LehmannCL,AronsRR,LoderRT,VitaleMG.The
epidemiologyofslippedcapitalfemoralepiphysis:anupdate. JPediatrOrthop.2006;26(3):286–90.
2.LeunigM,CasillasMM,HamletM,HerscheO,NotzliH,Slongo T,etal.Slippedcapitalfemoralepiphysis:earlymechanical damagetotheacetabularcartilagebyaprominentfemoral metaphysis.ActaOrthopScand.2000;71(4):370–5.
3.LoderRT,RichardsBS,ShapiroPS,ReznickLR,AronsonDD. Acuteslippedcapitalfemoralepiphysis:theimportanceof physealstability.JBoneJointSurgAm.1993;75(8):1134–40. 4.SouthwickWO.Osteotomythroughthelessertrochanterfor
slippedcapitalfemoralepiphysis.JBoneJointSurgAm. 1967;49(5):807–35.
6. JonesJR,PatersonDC,HillierTM,FosterBK.Remodellingafter pinningforslippedcapitalfemoralepiphysis.JBoneJoint SurgBr.1990;72(4):56873.
7. ZiebarthK,ZilkensC,SpencerS,LeunigM,GanzR,KimY. CapitalrealignmentformoderateandsevereSCFEusinga modifiedDunnprocedure.ClinOrthopRelatRes.
2009;467:704–16.
8. SucatoDJ,DeLaRochaA.HighgradeSCFE:theroleofsurgical hipdislocationandreduction.JPediatrOrthop.
2014;34(1):18–24.
9. GuimarãesRP,AlvesDPL,AzuagaTL,OnoNK,HondaE, PoleselloGC,etal.Traduc¸ãoeadaptac¸ãotransculturaldo HarrisHipScoremodificadoporByrd.ActaOrtopBras. 2010;18(6):339–43.
10.RoosBD,RoosMV,CamisaJúniorA,LimaEMU,GyboskiDP, MartinsLS.Abordagemextracapsularparatratamentodo impactofemoroacetabular:resultadosclínicos,radiográficos ecomplicac¸ões.RevBrasOrtop.2015;50(4):430–7.
11.SampsonTG.Arthroscopictreatmentoffemoroacetabular impingement.TechOrthop.2005;20(1):56–62.
12.SinkEL,ZaltzI,HeareT,DaytonM.Acetabularcartilageand labraldamageobservedduringsurgicalhipdislocationfor stableslippedcapitalfemoralepiphysis.JPediatrOrthop. 2010;30(1):26–30.
13.DunnDM.Thetreatmentofadolescentslippingoftheupper femoralepiphysis.JBoneJointSurgBr.1964;46:621–9.
14.DunnDM,AngelJC.Replacementofthefemoralheadbyopen operationinsevereadolescentslippingoftheproximal femoralepiphysis.JBoneJointSurg.1978;60(3):394–403. 15.GanzR,GillTJ,GautierE,GanzK,KrugelN,BerlemannU.
Surgicaldislocationoftheadulthip.Atechniquewithfull accesstothefemoralheadandacetabulumwithouttherisk ofavascularnecrosis.JBoneJointSurgBr.2001;83(8):1119–24. 16.LeunigM,SlongoT,KleinschmidtM,GanzR.Subcapital
correctionosteotomyinslippedcapitalfemoralepiphysisby meansofsurgicalhipdislocation.OperOrthopTraumatol. 2007;19(4):389–410.
17.SankarWN,VanderhaveKL,MatheneyT,Herrera-SotoJA, KarlenJW.ThemodifiedDunnprocedureforunstableslipped capitalfemoralepiphysis:amulticentricperspective.JBone JointSurgAm.2013;95(7):585–91.
18.UpasaniVV,MatheneyTH,SpencerSA,KimYJ,MillisMD, KasserJR.ComplicationsaftermodifiedDunnosteotomyfor thetreatmentofadolescentslippedcapitalfemoral epiphysis.JPedriatrOrthop.2014;34(7):661–7.
19.AkkariM,SantiliC,BragaSR,PolesselloGC.Trapezoidalbony correctionofthefemoralneckinthetreatmentofsevere acute-on-chronicslippedcapitalfemoralepiphysis. Arthroscopy.2010;26(11):1485–95.