Artigo Original
Amanda Dal Piva Gresele1 Alexandre Hundertmarck Lessa2 Leonardo Carvalho Alves3 Enma Mariángel Ortiz Torres1 Ana Valéria de Almeida Vaucher2 Anaelena Bragança de Moraes4 Maristela Julio Costa5
Descritores
Audição Perda auditiva Epidemiologia Sistema único de saúde Auxiliares de audição
Keywords
Hearing Hearing loss Epidemiology Uniied health system Hearing aids
Correspondence address:
Amanda Dal Piva Gresele
Av. Presidente Vargas, 2043/403, Centro, Santa Maria (RS), Brasil, CEP: 97015-513. E-mail: [email protected]
Received: 02/29/2012
Accepted: 09/06/2012
Study carried out in the Speech and Hearing Sciences Course, Universidade Federal de Santa Maria – UFSM – Santa Maria (RS), Brazil, with funds from the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
(1) Post-Graduation Program (Master’s) in Human Communication Disorders, Universidade Federal de Santa Maria – UFSM – Santa Maria (RS), Brazil.
(2) Post-Graduation Program (Doctorate) in Human Communication Disorders, Universidade Federal de Santa Maria – UFSM – Santa Maria (RS), Brazil.
(3) Speech and Hearing Sciences Course, Universidade Federal de Santa Maria – UFSM – Santa Maria (RS), Brazil. (4) Statistics Department and Departamento de Estatística and Post-Graduation Program (Docent) in Human Communication Disorders, Universidade Federal de Santa Maria – UFSM – Santa Maria (RS), Brazil. (5) Speech and Hearing Sciences Course and Post-Graduation Program (Docent) in Human Communication Disorders, Universidade Federal de Santa Maria – UFSM – Santa Maria (RS), Brazil.
Conlict of interest: nothing to declare.
aids grant program
Levantamento e análise de dados de pacientes atendidos
em um programa de concessão de aparelhos de
ampliicação sonora individual
ABSTRACT
Purpose: To establish a proile of the patients treated in a Hearing Aids Grant Program of the Brazilian Ministry of Health, by analyzing the variables: age, sex, type and degree of hearing loss, number of aided patients, adaptation type (unilateral or bilateral), and adapted ear. Methods: This is a descriptive observational study, retrospective in a cross-sectional perspective, which included patients treated between February 2006 and July 2010, totaling 1,572 individuals. Results: Their ages ranged from 3 to 100 years, mostly elderly (52.8%), with no frequency difference between the sexes. The sensorineural (73.12%) and moderate (54.7%) hearing losses were the most frequent ones, except in children, in whom the degree found was more profound (45.3%). More than 99% of the patients were aided, 258 unilaterally and 1,302 bilaterally. Conclusion: Mostly patients presents 60 years old or more, with no frequency difference between the sexes. The sensorioneural and moderate hearing losses were the most frequent ones, except in children. More than 99% of the patients were aided and the conducts were deined based in the audiological diagnosis and patient’s needs.
RESUMO
InTRODUCTIOn
The human body’s ive senses exert great inluence on all learning processes experienced by all individuals as they develop to their greatest potential. When there is an absence or deiciency in any of these senses, without eficient early intervention, a deicit in the reception of some stimuli may bring about signiicant consequences in the lives of individuals.
Within this context, auditory deiciencies appear as one of the most common and handicapping sensory deicits that may be present in a population(1). In Brazil, the Health Minister(2)
estimates that nearly 2,250 million persons have some degree of auditory loss. Nevertheless, few studies actually present prevalence and incidence igures addressing these deiciencies.
Individual hearing aids (IHAs) are a good option for reducing the sensory(3) deprivation and handicap,
improv-ing the auditory function, as well as the social interaction and quality of life of patients(4,5). By amplifying the
dif-ferent modes and intensities of sounds, depending on the individual needs IHAs permit the wearer to eficiently use their residual hearing(5,6).
One of the biggest dificulties encountered, during the selection and itting procedures of IHAs, as it relates to the adjustment period, is the cost, which is quite high(7). Focusing
on the dificulty of community access, the Brazilian Federal Government created, in September 2004, a National Hearing Health Policy, through the decrees 587 and 589, which proposed a hierarchical network, by region and integrated, which includes since prevention and hearing health promotion, to diagnosing and itting hearing prosthesis, including the auditory rehabilita-tion of children, adults, and the elderly(8).
In 2005, the Universidade Federal de Santa Maria (UFSM) was integrated into this policy through the credentialing of the Hospital Universitario de Santa Maria, Department of Speech and Hearing Sciences and Service of Speech, Language and Hearing Sciences Care. Consequently, this institution estab-lished the Servico de Atencao a Saude Auditiva de Media Complexidade, to continuously distribute hearing prosthesis through the Nucleo de Selecao e Adaptacao de Proteses Auditivas (NUSEAPA), which serves patients from the central-west sector of the State of Rio Grande do Sul.
From these understandings, important data were collected and some studies were carried out, which in turn have con-tributed with research addressing different aspects related to hearing. Through epidemiological studies, health problems are identiied, described, and analyzed conforming to the different communities in which they occur, how they are distributed and its determinants in order to assess their impacts and plan actions for the change of situation(9).
With this perspective, new research purports to reduce the negative consequences of auditory deiciencies though the global development of the individual. In Brazil, one study(10)
describes epidemiological researches carried out in the area of Audiology and points out the importance of collaborative work between Speech and Hearing Sciences and Epidemiology to increase the eficiency of population work in the three hierar-chical levels of the policy.
It should be noted that there still is a dearth of studies that present proiles of the patients being serviced in hearing health public programs, which would help with the planning of better services to individuals with hearing loss.
With regard to the services in Hearing Health Public Programs, two studies are highlighted: the proile of patients serviced in the Hospital Universitario da Universidade Federal de Santa Catarina through a Hearing Health State Program
(11) and the audiological and epidemiological descriptions
of the populations serviced in the Hospital das Clinicas da Universidade Federal de Minas, through an arrangement with the federal government(12).
Based on the considerations previously presented, the present study had as an objective to elaborate a proile of the patients being serviced by the hearing aids grant program of the Health Ministry, based in UFSM. The variables analyzed were the following: age, gender, type and degree of hearing loss, number of patients itted and not itted, and type of itting (bilateral or unilateral itting).
METhODS
This study was previously approved by the Committee of research ethics of UFSM, no 0138.0.243.246-06, and is part of a registered project in the Gabinete de Projectos no 09731. All patients in this study signed a consent form.
This study obtained and analyzed data, using a descriptive observational and retrospective in a cross-sectional perspective. The data collection was carried out through the databank of NUSEAPA of the Institution, which was created and input using the Microsoft Access 97 software of Microsoft Windows 98.
Data from all the questionnaires belonging to patients from the NUSEAPA, hearing aids grant program, during the period of February 2006 through July 2010 were analyzed.
Those patients whose data were incomplete or whose au-diological diagnosis was inconclusive were excluded from the analysis. The total sample comprised of 1572 questionnaires, from patients ranging in age between 3 and 100 years.
The following variables were considered: age, gender, type and degree of hearing loss, number of patients itted and not it-ted, and the type of aid, if bilateral or unilateral aid. Furthermore, associations between these variables were also analyzed.
With regard to age, the subjects were divided into ive groups using the World Health Organization (2010) classiica-tion: preschool and children up to the age of 12, adolescents between the ages of 13 and 18, young adults aged 19 to 44, middle aged from 45 to 60 years of age, and the elderly which included those older than 60.
The data analysis with regard to audiological diagnosis, with regard to the type and degree of hearing loss, was carried out by considering both ears separately, since there were pos-sibilities of having differences between the diagnoses for each ear in the same individual.
To determine and classify(13) the severity of the hearing
loss from 41 to 70dB NA; severe hearing loss was between 71 and 90dB NA; and profound hearing loss was deemed when the average was above 91dB NA.
Finally, a descriptive and statistical analysis of the data was performed using Statistica 9.0 and BioEstat 5.0 software. The level of conidence used was 95% (p=0.05).
The analysis of signiicance of the isolated variables (gender, age, type, and degree of loss) was carried out using the Lilliefors test. In order to test for relationships between the different variables and gender, a Pearson correlation was performed. Finally, the associations between gender and age, age and type of hearing loss, age and degree of loss, and degree and type of loss were carried using the χ2 test.
RESUlTS
It was analyzed data from 1,572 patients, aged between three and 100 years old. With regard to the distribution of subjects by age, 830 (52.8%) were elderly, 302 (19.21%) were middle-aged adults, 222 (14.12%) were young adults, 150 (9.54%) were children, and 68 (4.33%) were adolescents. A signiicant difference in distribution was observed between the age groups (p<0.05).
Frequency counts by gender were 796 (50.64%) males, and 776 (49.36%) females. A signiicant difference between gen-ders was not found (0<0.61). A signiicant difference between gender by age was found (p=0.00070) (Table 1).
The results of residuals for χ2 analysis revealed that the
difference between genders occurred because of a larger number of young adult females and elderly males in the sample than is estimated by the test, considering the deter-mined of conidence level.
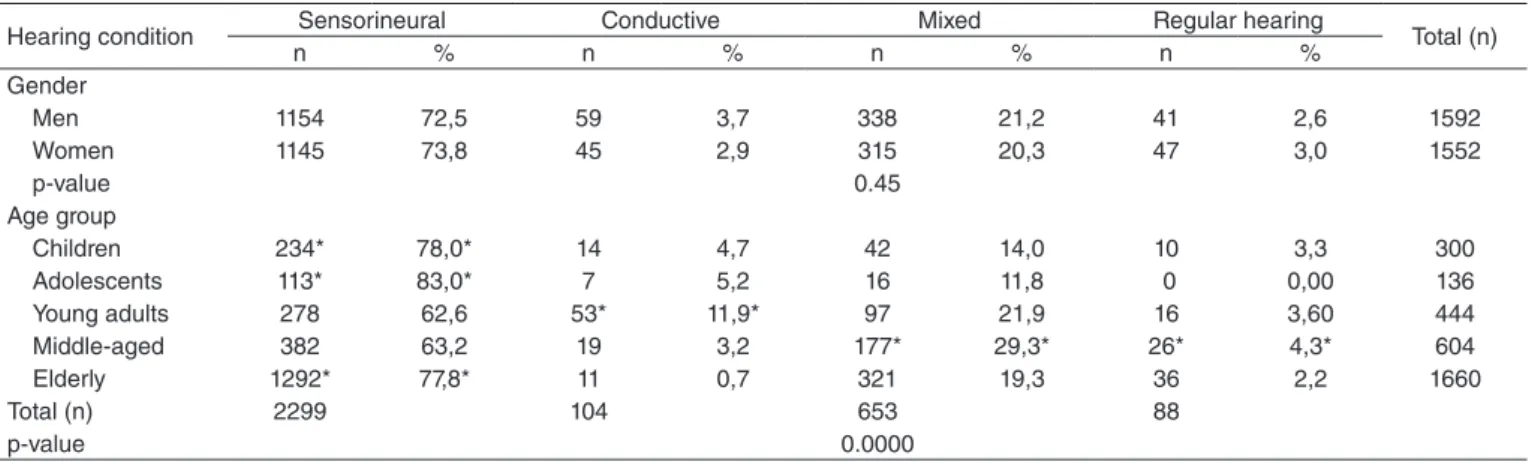
With regard to hearing condition, of the 3,144 ears consid-ered, 2,299 (73.12%) presented sensorineural hearing loss. The second condition most found was mixed hearing loss in 653 (20.77%) ears, followed by 104 (3.31%) ears with conductive hearing loss and 88 (2.8%) with normal hearing. The results of the statistical analysis conirmed a difference in the distribution of the hearing loss types in the groups studied (p<0.05).
The distribution analysis of the subjects with regard to gender and age, and type of hearing loss, found no difference in the distribution of the type of hearing loss between gender (p=0.45) (Table 2).
Large percentages of sensorineural hearing loss were observed in all age ranges. residuals for χ2 analysis proved
the following: a larger number than expected of sensorineural loss in children, adolescents, and elderly; larger number than expected of conducted hearing loss in young adults as well as mixed hearing loss and normal hearing among middle-aged persons.
In the distribution of subjects by type of hearing loss such as sensorineural loss, of the 2,299 ears with this condition, 1,292 (56.2%) were from the elderly. Similarly, of the 653 ears with mixed hearing loss and 88 with normal hearing, 321 (49.16%) and 36 (40.91%) respectively were also observed within this age group. Conductive hearing loss percentages were mostly concentrated in the ears of young adults, with 53 (50.96%) of the 104 ears manifesting this type of hearing loss.
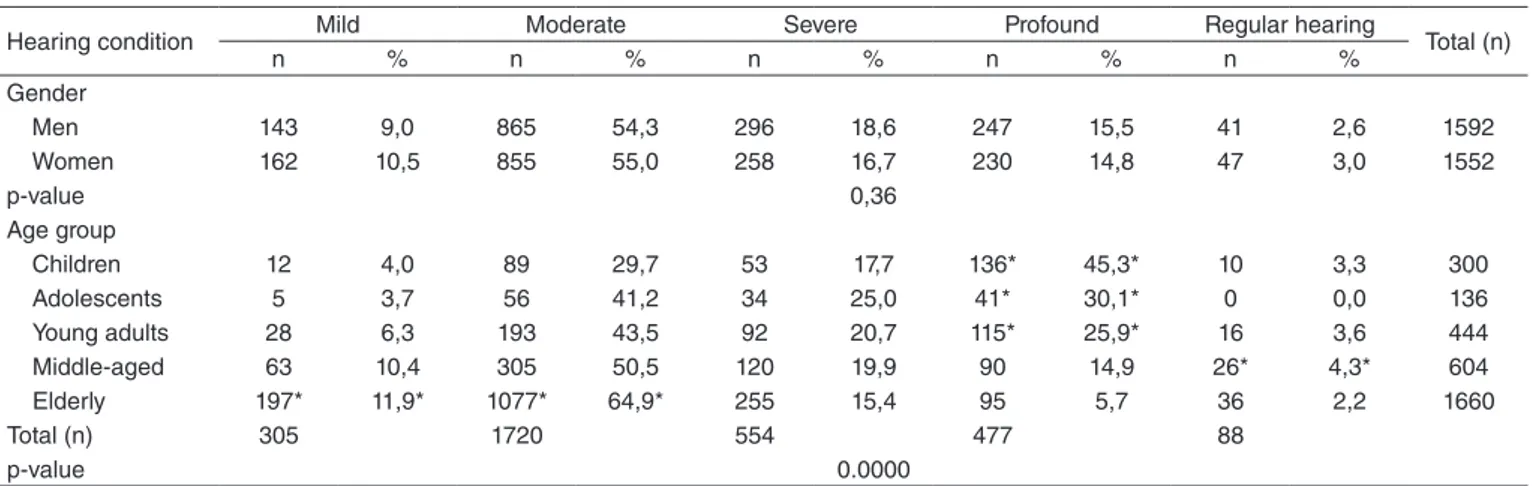
With regard to hearing conditions as they relate to degree of hearing loss, of the 3,144 ears of the subjects in this study, 1,720 (54.7%) presented moderate hearing loss, followed by 554 (17.62%) with severe hearing loss, 477 (15.17%) profound hearing loss, 305 (9.7%) mild hearing loss, and 88 (2.8%) with normal hearing. A statistical analysis conirmed signiicant dif-ferences between the degree of hearing loss exhibited (p<0.05).
A distribution of the subjects by gender and age with regard to degree of hearing loss revealed that there were no
Table 1. Distribution of subjects according to the variables gender and age group
Age group
Gender
Total (n)
Male Female
n % n %
Children 84 56,0 66 44,0 150
Adolescents 27 39,7 41 60,3 68
Young adults 88 39,6 134* 60,4* 222
Middle-aged 150 49,7 152 50,3 302
Elderly 447* 53,9* 383 46,1 830
Total (n) 796 776
p-value 0.00070
*Significant values (p<0.05) – Pearson’s Correlation Test, χ2 test of association and χ2 residual analysis
Table 2. Distribution of subjects, considering gender and age group according to the variable hearing condition (hearing loss) per ear
Hearing condition Sensorineural Conductive Mixed Regular hearing Total (n)
n % n % n % n %
Gender
Men 1154 72,5 59 3,7 338 21,2 41 2,6 1592
Women 1145 73,8 45 2,9 315 20,3 47 3,0 1552
p-value 0.45
Age group
Children 234* 78,0* 14 4,7 42 14,0 10 3,3 300
Adolescents 113* 83,0* 7 5,2 16 11,8 0 0,00 136
Young adults 278 62,6 53* 11,9* 97 21,9 16 3,60 444
Middle-aged 382 63,2 19 3,2 177* 29,3* 26* 4,3* 604
Elderly 1292* 77,8* 11 0,7 321 19,3 36 2,2 1660
Total (n) 2299 104 653 88
p-value 0.0000
signiicance differences between gender and degree of hearing loss (p=0.36) (Table 3).
When analyzing the percentages taking into account the degree of hearing loss, it was noted that of the 477 ears of subjects with profound hearing loss, 136 (28.51%) were from children. Of the 305 ears with mild hearing loss and of the 1,720 with moderate hearing loss, 197 (62.62%) and 1,077 (64.88%) were found in the elderly respectively. Of 88 ears with normal hearing, 26 (29.55%) were from middle-aged persons. A residuals for χ2 analysis revealed that these
val-ues were within the upper limits of the conidence interval band (a=95%), that is, they were larger than estimated. The same test also revealed that there were more ears of adoles-cents and young adults with profound hearing losses than predicted, since these groups presented less moderate and mild hearing losses than the other groups. In the ears of the adolescents, values lower than expected were found with relation to normal hearing.
Associations made between the type of hearing loss and the degree of hearing loss revealed that for all types of hearing loss, the most prevalent degree was the moderate type. Using the residuals for χ2 analysis, it was seen that the ears of subjects
with sensorineural losses presented mostly with mild, moderate and profound hearing losses, and that those with conductive hearing loss were mostly concentrated within the moderate hearing loss range (Table 4).
Addressing the number of patients itted, the type of it, if uni-lateral or biuni-lateral, and if a uniuni-lateral it, which ear was itted, it was revealed that only 12 (0.8%) were not itted with IHA (Table 5).
DISCUSSIOn
In Brazil, there is a dearth of studies presenting the proiles of patients seen in hearing health public programs, making it dificult to adequately plan collective health prevention and intervention measures that would address the real needs of the population. Within this context, epidemiological studies that delineate the proiles of these patients are basic for help-ing with the process and best service delivery to persons with hearing loss.
The analysis of the data being seen by the Programa de Concessao de Proteses Auditivas, with regard to the age at
Table 4. Distribution of subjects, considethe variables type and degree of hearing loss, per ear
Degree of Hearing Loss
Mild Moderate Severe Profound Regular hearing
Total (n)
n % n % n % n % n %
Type of loss Hearing
Sensorineural 261* 11,3* 1326* 57,7* 329 14,3 383* 16,7* 0 0,0 2299
Conductive 25 24,0 72* 69,3* 7 6,7 0 0,0 0 0,0 104
Mixed 19 2,9 322 49,3 218 33,4 94 14,4 0 0,0 653
Regular hearing 0 0,0 0 0,0 0 0,0 0 0,0 88 100,0 88
Total (n) 305 1720 554 477 88
p-value 0.0000
*Significant values (p<0.05) – Pearson’s Correlation Test, χ2 test of association and χ2 residual analysis
Table 5. Distribution of subjects according to the variables adaptation of IHAs, unilateral, bilateral and adapted ear
Unilateral Bilateral
Total (n) Right
ear
Left
ear RE + LE
n % n % n %
Adapted 143 9.1 115 7.3 1302* 82.8* 1560
p-value 0.0000
*Significant values (p<0.05) Caption: RE = right ear; LE = left ear
Table 3. Distribution of subjects, considering gender and age group according to the variable hearing condition (degree of hearing loss)
Hearing condition Mild Moderate Severe Profound Regular hearing Total (n)
n % n % n % n % n %
Gender
Men 143 9,0 865 54,3 296 18,6 247 15,5 41 2,6 1592
Women 162 10,5 855 55,0 258 16,7 230 14,8 47 3,0 1552
p-value 0,36
Age group
Children 12 4,0 89 29,7 53 17,7 136* 45,3* 10 3,3 300
Adolescents 5 3,7 56 41,2 34 25,0 41* 30,1* 0 0,0 136
Young adults 28 6,3 193 43,5 92 20,7 115* 25,9* 16 3,6 444
Middle-aged 63 10,4 305 50,5 120 19,9 90 14,9 26* 4,3* 604
Elderly 197* 11,9* 1077* 64,9* 255 15,4 95 5,7 36 2,2 1660
Total (n) 305 1720 554 477 88
p-value 0.0000
which time they seeked services, revealed a prevalence of elderly with more than 60 years of age, supporting the results found in other studies(12-14). This relects the changes in aging
that start to occur from the age of 30, which leads to progres-sive hearing loss(15). Therefore, it should be considered that the
gradual increase of hearing loss, the time of auditory depriva-tion(16), and the dificulties related to the loss encountered
mo-tivate the individuals to seek audiological services just several years after the initial identiication.
Demographic Census data reveal that the elderly already comprise 11.6% of the general population, reafirming the increase in longevity and the reduction of mortality rates occur-ring within the last decades. Thus, the aging of the population and the quality of life in this age group has been a focus of Brazilian public health activity. As alluded to in international studies(17), epidemiological studies have the potential of
con-tributing to the knowledge about presbycusis, its genetics, environmental, and gender aspects; identifying potential in-tervention strategies; and improving existing treatments, such as the itting of prosthesis.
In keeping, it is possible that new and rising invest-ments of the Federal Government Programs can help with the promotion of hearing health, through actions directed at communities and professionals (from community health workers to doctors — who are responsible for referrals), so that a diagnosis does not occur years after the identiication of the deiciency.
Regarding the low percentage of children seeking these services, it may be that this center is for average care, therefore serving persons older that three. In the meantime, it is noted that other research have also found less representation of chil-dren receiving audiological diagnostic services(12,18), revealing
the importance of implementing a universal neonatal hearing screening program and the implementation of programs and campaigns speciically educating parents with regard to the identiication of hearing loss in their children(18).
Taking into account the gender variable, in this study no differences were found between the number of men and women serviced, agreeing with the data of population serviced in another hearing health program in the country(12). With regard
to the prevalence of hearing loss, a study carried out in Asia did not ind any differences between genders(19). Already,
some Brazilian studies have found larger numbers of men with hearing loss(13,14), and others in women(20,21), without any
conirmation as to which gender has a larger incidence in the global population.
In the present research, a relationship was found between gender and age of the sample. The prevalence of hearing loss among women, as age is considered in adults, has also been presented in other studies(11,20,21). When considering the elderly,
just as has been found in this analysis, researchers indicate a larger prevalence of hearing loss among males, also indicating that with aging men are four times more likely to present with some hearing issue when compared to females(17,22). Thus, it
was observed that there is no consensus in the national and international literature with regard to the prevalence of hearing loss when gender and age are considered.
With regard to the type of hearing loss, sensorineural hearing loss was observed as having a larger prevalence rate in the services addressed, as was unanimously found in the references obtained for this research(12,15,20-23). In studies carried
out in infant populations, sensorineural hearing loss is most prevalent; however the percentage of conductive hearing loss has increased(11,24).
The large number of sensorineural hearing loss found in this study is justiied by the elevated number of elderly patients and the presence of presbycusis that causes the increased percent-age. Furthermore, since it is a program which grants hearing prosthesis, it is understood that few patients come with any modiications to the external or middle ear, since they experi-ence an evaluation by a doctor and only in extreme cases are they referred for a itting.
When verifying any associations between gender and type of hearing loss, there were no signiicant relationships between the variables. Prevalence data were obtained for sensorineural hearing loss in both men and women, agreeing with results found in other studies(14,25).
Sensorineural hearing loss was the most found in all age ranges. The fact that larger than estimated numbers of ears of children, adolescents, and the elderly presented with this type of hearing loss, as veriied through residuals for χ2 analysis,
can be justiied by several factors. In the elderly, presbycusis may be the most common cause for this hearing deiciency. The degeneration of the cochlea caused by the presbycusis , in addition to harming the auditory function as a whole, is char-acterized by the hearing loss mentioned, agreeing with other studies. Studies with children already indicate that pre-, peri- and postnatal factors can contribute to hearing loss, primarily sensorineural. In adolescents, the increase in the incidence of hearing loss, primarily of the sensorineural type, also has been observed in international studies(26), correlating with the
increase in hearing thresholds with the elevated levels of sound pressure to which adolescents are exposed to on a daily basis. The same study also noted that adolescents underestimate hear-ing problems or tinnitus, or to temporary changes in thresholds after being exposed, which leads to a delay in searching for diagnostic centers to carry out treatment measures.
The fact that the residuals for χ2 analysis test points to
numbers above those estimated by the tests of ears with con-ductive and hearing losses in young adults, and mixed hear-ing loss in middle-aged adults, can be justiied by one of the most commonly itted pathologies with conductive hearing loss — otosclerosis. This ailment is one of the most common causes of hearing loss in adults, with an incidence more com-mon acom-mong women aged 20–40 years(27). In more advanced
ages, otosclerosis may be associated with sensorineural loss, resulting in a mixed loss(11). In cases in which surgical
treat-ment is not appropriate, referral for hearing prosthesis would be indicated.
In the analysis of the degree of hearing loss, a larger con-centration of the moderate hearing loss was observed, agreeing with results found in demographic research(13), and with two
Brazilian hearing health programs(11,12). Similarly, the
keeping in mind the gender of the subjects, though moderate and severe hearing are represented in larger percentages, fol-lowing what resulted from the analysis of these variables(14).
The statistical analysis of the degree of hearing loss revealed an elevated number of children with profound hearing loss, as has been found in other studies carried out with this popula-tion(11,12,24,28). It is known that one of the most frequent causes of
congenital hearing loss is maternal infections, and within these, the most prominent is the Rubeola Congenita syndrome(29). In
spite that the vaccination programs have been successful with reducing the number of cases with this ailment in Brazil, still hearing losses with this etiology continue to be found.
Already among the causes for acquired hearing loss, bacterial meningitis(29) has been identiied; therefore periodic hearing
evalu-ations must be made in all children presenting with this ailment, since the hearing loss may appear after all symptoms have ceased.
Both hearing losses caused by congenital rubella and bacterial meningitis present with sensorineural loss patterns with degrees varying between severe and profound, therefore justifying the high degree between the ears of children analyzed in this study.
With regard to the prevalence of mild and moderate hearing loss in the elderly, this is justiied since the degree of presby-cusis for 500, 1,000, and 2,000 Hz is generally between 15 and 60 dB NA(15). This data was also found in international and
national studies(17,22). In spite that hearing changes in aging are
expected in middle-aged persons, the number of subjects in this age range of this study with normal hearing still remained above the estimated number. It should be noted that in this study the Davis and Silvemann(13) classiication was used. It considers the
tritonal average in the 500, 1,000, and 2,000 Hz frequencies. Therefore, the causes with reduced tonal thresholds in only high frequencies, common in the initial stages of presbycusis, were not classiied as presenting with hearing loss.
The number of adolescents and young adults with profound hearing loss may have the same justiication as the high inci-dence of this hearing loss type in children. Many adolescents and young adults are itted with IHAs as children in other set-tings and come to NUSEAPA when older to request new aids and follow-up services through the Hearing Health Program of the Federal Government.
The association between the type and degree of hearing loss conirmed previously conirmed data pointing to increased occurrence of moderate loss in any type of hearing loss. Furthermore, the high degree of concentration of sensorineural hearing loss of the mild, moderate, and profound types is justi-ied since they are the most found in the elderly and children, respectively(11,12,17,22,24,28). These two age ranges, together,
ac-count for more than 60% of the total sample.
In cases of conductive hearing loss, the causing patholo-gies for those with itting possibilities, like otosclerosis, do not exceed the moderate loss degree. Therefore, it is justiied that there is a larger concentration of conductive hearing loss in subjects of this study.
With regard to prosthesis, in this study, it was observed that more than 99% of the patients were itted, with differences between bilateral and unilateral ittings. A bilateral itting of-fers advantages such as better localization of the sound source,
binaural summation, elimination of head shadow effect, better speech discrimination in the presence of noise, and dimin-ished efforts to hear(6). Because of the advantages described,
a bilateral ampliication recommendation is preferred for all candidates, except when there is a contraindication, such as big differences in auditory thresholds between each ear, severe problems with motor skills, changes in auditory processing, and rejections due to esthetics or inances(6). As a consequence,
these are considered at the moment of selecting and itting the auditory prosthesis in the service being addressed, and when possible, a bilateral prosthesis is implemented, since it is be-lieved that they provide better auditory results, and further, a better quality of life to the users of hearing prosthesis.
COnClUSIOn
The majority of patients in this study were 60 years of age and older, without a frequency count difference between genders. Sensorineural hearing loss type and moderate hearing loss were the most frequently diagnosed in all genders and age ranges studied, except in children where profound hearing loss was mostly identiied.
With regard to itting, it was observed that of the 1,572 patients seen, more that 99% were itted, 258 unilaterally and 1,302 bilaterally, which is the preferred identiied procedure in accordance to their audiological diagnosis and needs.
* ADP Gresele contributed in the data analysis and interpretation and write-up of the inal article draft; AH Lessa contributed in the data analysis and interpretation and critical revision of the content; LC Alves contributed in the data analysis and interpretation and write-up of the inal article draft; EMO Torres participated in the critical revision of the content and revision of the inal article draft; AVA Vaucher contributed with the conceptualization of the project and data; AB de Moraes participated in the data analysis and interpretation; MJ Costa participated in the coordination of the concept, data analysis and interpretation, write-up and revision of the inal article draft.
REFEREnCES
1. Brasil. IBGE. Censo Demográico 2010 - resultados preliminares da amostra. [citado 2011 Out 18] Disponível em: http://www.censo2010. ibge.gov.br/sinopse/webservice.
2. Brasil. Ministério da Saúde. Portaria GM/MS nº. 2.073, de 28 de setembro de 2004. Institui Política Nacional de Atenção à Saúde Auditiva. Diário Oicial da União. 29 set 2004; Seção 1:34). [citado 2011 Ago 30]. Disponível em: http://portal.saude.gov.br/portal/sas/mac/area. cfm?id_area=848.
3. Silman S, Iório MCM, Mizhahi MM, Parra VM. Próteses auditivas: um estudo sobre seu benefício na qualidade de vida de indivíduos portadores de perda auditiva neurossensorial. Distúrb.comun. 2004;16(2):153-65. 4. Magni C, Freiberger F, Tonn K. Avaliação do grau de satisfação entre
os usuários de ampliicação de tecnologia analógica e digital. Rev Bras Otorrinolaringol. 2005;71(5):650-57.
5. Russo ICP. Editorial II: a relevância da pesquisa cientíica na audiologia brasileira. Rev CEFAC. 2009;11(Suppl1):0-0.
6. Almeida K. O processo de seleção e adaptação de aparelhos de amplificação sonora. In: Lopes Filho OC. organizador. Tratado de fonoaudiologia. São Paulo: Tecmedd; 2005. p471-92.
dos questionários de auto-avaliação. Rev Bras Otorrinolaringol. 2007;73(5):660-70.
8. Brasil. Ministério da Saúde. Saúde auditiva. Portarias de saúde auditiva. Brasília, DF: Ministério da Saúde; 2004. [citado 2011 Out 18]. Disponível em: http://portal.saude.gov.br/portal/sas/mac/area.cfm?id_ area=848.
9. Goldbaum M. Epidemiologia e serviços de saúde.Cad Saúde Pública. 1996;12(Suppl 2):95-8.
10. Arakawa AM, Sitta EI, Caldana ML, Sales-Peres SHC. Análise de diferentes estudos epidemiológicos em Audiologia realizados no Brasil. Rev CEFAC. 2010;13(1):152-8.
11. Dimatos OC, Ikino CMY, Philippi PA, Dimatos SC, Birck MS, Freitas PF. Peril dos pacientes do Programa de Saúde Auditiva do Estado de Santa Catarina atendidos no HU-UFSC. Arquivos Int Otorrinolaringol. 2011;15(1):59-66.
12. Domingos BP. Caracterização do peril audiológico e epidemiológico da população atendida em um programa de saúde auditiva. [monograia] Minas Gerais: Curso de Fonoaudiologia, Universidade Federal de Minas Gerais; 2010.
13. Davis H, Silvemann RS. Hearing and Deafness. New York: Holt, Rinehart e Winston; 1970.
14. Béria JU, Raymann BCW, Gigante LP, Figueiredo ACL, Jotz G, Roithman R et al. Hearing impairment and socioeconomic factors: a population-based survey of an urban locality in southern Brazil. Rev Panam Salud Publ./Pan Am J. Public. 2007;21(6):381-7.
15. Mondelli MFCG, Silva LSL. Perfil dos pacientes atendidos em um sistema de alta complexidade. Arquivos Int Otorrinolaringol. 2011;15(1):29-34.
16. Jerger S, Jerger J. Presbiacusia. In: Jerger S, Jerger J. Alterações auditivas: um manual para avaliação clínica. São Paulo, Livraria Atheneu; 1989. 17. Paiva KM, Cesar CLG, Alves MCGP, Barros MBA, Carandina L,
Goldbaum M. Envelhecimento e deficiência auditiva referida:
um estudo de base populacional. Cad Saúde Pública. 2011;27(7): 1292-300.
18. Cruickshanks KJ, Wiley TL, Tweed TS, Klein BEK, Klein R, Mares-Perlman JA et al.Prevalence of hearing loss in older adults in Beaver Dam, Wisconsin. Am J Epidemiol. 1998;148(9):879-86.
19. Marini ALS, Halpern R, Aerts D. Sensibilidade, especiicidade e valor preditivo da queixa auditiva. Rev Saúde Pública. 2005 Dec;39(6):982-4. 20. Al Khabori M, Khandekar R. The prevalence and causes of hearing
impairment in Oman: a community-based cross-sectional study. Int J Audiol. 2004;43(8):486-92.
21. Santos MAO, Vianna MF, Marotta L, Almeida CM, Sousa Neto OM. A deiciência auditiva em hospital terciário: estudo epidemiológico. Rev Bras Otorrinolaringol. 2008;74(1):222-6.
22. Jardim IS, Iwahashi JH, Paula VC. Estudo do peril audiológico de indivíduos atendidos em um serviço de diagnóstico brasileiro. Arquivos Int Otorrinolaringol. 2010;14(1):32-7.
23. Mattos LC, Veras RP. A prevalência da perda auditiva em uma população de idosos da cidade do Rio de Janeiro: um estudo seccional. Rev Bras Otorrinolaringol. 2007;73(5):654-9.
24. Figueiredo W. Assistência à saúde dos homens: um desaio para os serviços de atenção primária. Ciên Saúde Colet. 2005;10(1):105-9. 25. Santos FR, Manfredi AKS, Isaac ML. Caracterização da perda auditiva
de crianças atendidas em um programa de saúde auditiva. Medicina (Ribeirão Preto). 2009;42(3):366-71.
26. Silva BSR, Sousa GB, Russo ICP, Silva JAPR. Caracterização das queixas, tipo de perda auditiva e tratamento de indivíduos idosos atendidos em uma clínica particular de Belém – PA. Arquivos Int Otorrinolaringol. 2007;11(4):387-95.
27. Schargorodsky J, Curhan SG, Curhan GC, Eavey R. Change in prevalence of hearing loss in US adolescents. JAMA. 2010;304(7):772-8. 28. Jafek BW, Murrow BW. Segredos em Otorrinolaringologia: respostas
necessárias ao dia-a-dia em rounds, na clínica, em exames orais e escritos. 2a ed. Porto Alegre: Artmed; 2006.