Medium Term Prognostic Value of Stress Myocardial Perfusion
Scintigraphy in a Chest Pain Unit
Jader Cunha de Azevedo, Renata Christian Martins Félix, Patrícia Lavatori Corrêa, Gustavo Borges Barbirato, Hans
Fernando da Rocha Dohmann, Paulo Roberto Dutra da Silva, Evandro Tinoco Mesquita, Cláudio Tinoco Mesquita
Hospital Pró-Cardíaco – PROCEP, Universidade Federal Fluminense – Rio de Janeiro, RJ - BrazilSummary
Objective: To evaluate the prognostic value of stress myocardial perfusion scintigraphy (MPS) applied to patients with suspected acute coronary syndrome (ACS).
Methods: Retrospective study. Patients with suspected acute coronary syndrome (ACS) admitted into the chest pain unit &38IURP'HFHPEHUWR$SULODIWHUH[FOXVLRQRIDFXWHP\RFDUGLDOLQIDUFWLRQ$0,DQGKLJKULVNXQVWDEOH angina they underwent stress MPS.
Results:6HOHFWHGSDWLHQWV\HDUVDQGPDOHJHQGHU7KHWHVWZDVSHUIRUPHGKRXUV
DIWHUDGPLVVLRQ0\RFDUGLDOLVFKHPLD,64ZDVIRXQGLQSDWLHQWV0DOHJHQGHUQ S KLVWRU\ RIGLDEHWHVPHOOLWXVQ S SDVWRI$0,Q S SDVWRIVXUJLFDOP\RFDUGLDOUHYDVFXODUL]DWLRQ Q S DQGSDVWRISHUFXWDQHRXVUHYDVFXODUL]DWLRQQ S SUHVHQWHGFRUUHODWLRQZLWK,64 7KHIROORZXSZDVGD\V1R036YDULDEOHFRUUHODWHGZLWKWKHRFFXUUHQFHRISULPDU\RXWFRPH$EQRUPDO VFLQWLJUDSK\Q S,64Q SDQGSRVWVWUHVVOHIWYHQWULFXODUHMHFWLRQIUDFWLRQEHORZ Q S FRUUHODWHGZLWKVHFRQGDU\RXWFRPH7KHSUHVHQFHRI,64ZDVWKHPDMRUYDULDEOHLQWKHPXOWLYDULDWH DQDO\VLVIRUWKHSUHGLFWLRQRIVHFRQGDU\RXWFRPH55 &,
Conclusion: Presence of ISQ was the major independent factor in prediction of adverse events for patients admitted into the CPU.
Key words: Chest pain unit, myocardial, myocardial reperfusion scintigraphy.
0DLOLQJDGGUHVV-DGHU&XQKDGH$]HYHGR Serviço de Medicina Nuclear – Hospital Pró-Cardíaco – Rua General Polidoro, 192 – 22280-000 – Rio de Janeiro, RJ, Brazil E-mail: [email protected]
Manuscript received August 23, 2006; revised received November 22, 2006; accepted January 17, 2007.
Introduction
The appropriate approach for patients who seek emergency units complaining of chest pain and other symptoms suggestive of acute coronary failure is a complex one. When the electrocardiogram (ECG) is not diagnostic or presents nonspecific alterations and when clinical data are not typical, diagnosing Acute Coronary Syndrome (ACS) becomes a difficult task. This clinical complexity leads to a large number of unnecessary admissions to hospital and a larger number of undue discharges of patients who should remain under medical care1,2.
Clinical assessment with ECG and measurement of myocardial necrosis markers is very sensitive in the detection of Acute Myocardial Infarction (AMI)3. However, biochemical
markers of myocardial necrosis only rise when there is irreversible cellular damage. Many patients with ACS do not present electrocardiographic alterations and might not present myocardial necrosis on admission. This strategy may therefore
fail to identify patients who, even when considered low-risk patients, present significant coronary injuries3-8.
Up to 5% of the patients admitted into the emergency room with chest pain and who are considered low-risk patients may present ACS9,10. When these patients are
inadvertently discharged, they have a worse prognosis, with a mortality rate two to three times higher than patients who are adequately treated. In the United States of America, approximately 20% of the suits against physicians are due to this bad medical practice11-13.
The Chest Pain Unit (CPU) located in the emergency department is an efficient alternative to assess and screen patients with suspected ACS. It employs a systematic strategy to assess these patients by using protocols for clinical and laboratory assessment (serial measurements of markers of myocardial necrosis and serial electrocardiogram). It allows fast and accurate diagnosis, and allows the stratification of risk and the employment of the appropriate treatment for these patients14. It represents a safe and effective approach able
to reduce costs in the management of patients considered of low to intermediate risk for cardiovascular events15.
transluminal coronary angioplasty (PTCA).
Scintigraphy variables used were: type of stress, either physical or pharmacological (dipyridamole, dobutamine or adenosine), presence of ischemia (area of low uptake of radiotracer in the post-stress images which disappears in rest images) or fibrosis (area of low uptake of radiotracer in the post-stress images which persists in rest images), the number of myocardial segments with ischemia and the post-stress ejection fraction of the left ventricle26.
Follow-up was considered from the date of hospital discharge to the date of the first contact with the patient. We phoned each patient to obtain information from him. When contact with the patient was not possible, the information was obtained from family members, from the assistant doctor or from the hospital records.
We collected information on adverse events which took place after the patient’s discharge from hospital. Interventions (PTCA, SMR) performed during hospitalization were not considered as adverse events, but as a consequence of treatment. We considered only those adverse events which took place after hospital discharge.
For the purpose of statistical analysis and analysis of the prognosis we considered two outcomes – the primary and the secondary outcomes. We defined adverse events such as death due to any cause or acute myocardial infarction as primary outcomes. Acute myocardial infarction was defined as a new episode of chest pain with duration greater than 20 minutes which required hospitalization and was confirmed by the elevation of myocardial necrosis markers (creatine phosphokinase fraction MB [CK-MB] or Troponin I) or the appearance of Q waves on the ECG and the need for reperfusion therapy with thrombolysis or emergency PTCA27.
The combination of any of the following adverse events occurring after hospital discharge was considered a secondary outcome: death due to any cause, AMI, angina or rehospitalization due to angina (defined as type A or type B precordial pain, with no other determining cause3), SMR
or PTCA and hospitalization due to heart-related causes (arrhythmias, heart failure, etc) 27.
The presence of coronary obstructive injury with luminal reduction equal to or above 50% was considered a significant coronary injury28.
Statistical analysis - We used the chi-square test (C2) or Fisher’s exact test, whenever the C2 test could not be applied due to the small number of cases. For the analysis of continuous variables between the two groups we used Student’s t test for independent samples. Multivariate analysis, used to identify independent factors that simultaneously influence or explain the occurrence of events and to assess the simultaneous influence of clinical variables on events, was carried out using Logistic Regression, and we used a stepwise process with a level of 5% to select the factors. The uneventful survival rate (free of primary and secondary outcomes) was adjusted by the Kaplan-Meier method. Log-rank statistics was applied to verify if there is significant difference in the event-free survival curve for primary and combined events stratified according to scintigraphy results. The criterion to determine significance was a level of 5%.
the best known ones are the treadmill exercise test, stress echocardiogram, myocardial perfusion scintigraphy (MPS) and magnetic resonance imaging. The number of papers on computerized tomography has been growing but this method is not widely available in Brazil yet16,17.
MPS has been increasingly used to diagnose ACS in the CPU, and many protocols for chest pain assessment use this method to assess the prognosis of these patients18-20. MPS has
proved effective in reducing the number of undue discharges and unnecessary admissions18,21,22. Whether the employment
of this technique in CPUs in Brazil can assess the medium term prognosis of patients admitted with chest pain remains to be proven.
The objective of our study was to determine the medium term prognostic value of stress MPS when performed on patients admitted into the CPU with suspected ACS, after the diagnosis of AMI and High Risk Unstable Angina are ruled out.
Methods
We carried out a retrospective cohort study where we selected consecutive patients admitted into the CPU of
Hospital Pró-Cardíaco with suspected ACS from December 2002 to April 2004, and submitted to stress MPS.
These patients were assessed based on the Hospital’s CPU care methodology which follows the model of stratification in investigative routes described by Bassan et al3,23. This protocol
includes not only the clinical history but also the performance of ECG and the serial measurement of heart enzymes in an interval not lower than six hours. Once the diagnosis of AMI or high risk unstable angina has been excluded24,25, the patients were
stratified through the performance of MPS at rest and under physical or pharmacological stress upon request of the physician of the emergency department or of the assistant doctor.
The study was approved by the Research Ethics Committee ofHospital Pró-Cardíaco under docket nº 137/2005. The free informed consent term was not required for this study.
All the tests were carried out in a dual head gamma chamber (Ecam-Duet – Siemens), with a low-energy and high resolution collimator with tomographic image acquisition (SPECT - Single Photon Emission Computed Tomography) coupled with the ECG (ECG-Gated), with 64 projections and a 64 x 64 matrix. After their acquisition, the images were reconstructed through backprojection with a Butterworth filter and processed using e-Soft (Cedars Sinai, Guido Germano and Emory Cardiac Toolbox), an image processing software package. The analysis of global and segmental contractility and of ejection fraction was accomplished using the Gated SPECT. The unit used the 17-segment myocardial segmentation model26.
Results
We selected 301 patients with suspected ACS who were submitted to MPS to stratify risk. Our sample was composed by 164 male (54.5%) and 137 (45.5%) female patients, with a mean age equal to 65.3 ± 12.5 years for this population.
The test was performed early, that is 12 hours after admission, in 146 patients (48.6%); between 12 and 24 hours after admission in 132 patients (44%) and after 24 hours following the admission into the CPU in 23 patients (7.4%). The mean time between admission and the performance of scintigraphy was 13 ± 12 hours. We did not record any serious events such as AMI or death during the performance of the cardiovascular stress test.
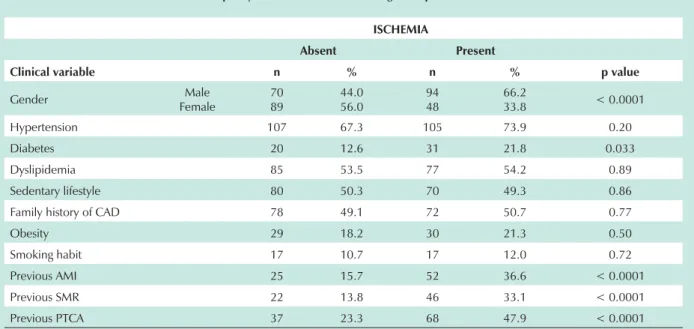
The presence of altered scintigraphy was verified in 162 patients (53.8%). We also observed an elevated percentage of patients who presented ischemia which corresponded to 47.2% (n=142) of our sample and a significant percentage of these patients presented ischemia in three or more segments 33.9% (n = 102). Patients with and without ischemia did not present significant difference regarding age (65.5 ± 13.1 years as compared with 65.2 ± 11.9 years respectively; p = 0.82). Male gender (n = 94, p = <0.0001), diabetes mellitus (n = 31, p = 0.033), past AMI (n = 52, p = <0.0001), past SMR (n = 46, p = <0.0001) and past PTCA (n = 68, p = <0.0001) presented statistically significant correlation with the presence of ischemia. Other clinical characteristics are shown on Table 1.
The type of stress that was used most frequently was pharmacological stress. Dipyridamole stress was used in 161 patients (53.5%), dobutamine stress in 17 patients (6%) and adenosine stress in 2 patients (0.5%). Physical stress on the treadmill was used with 121 patients (40%). The rate of altered tests in patients who were submitted to pharmacological stress
(n = 109) was significantly higher than the rate for those submitted to physical stress (n = 53) (60.6% as compared with 43.8% respectively, p = 0.004).
After the performance of MPS, 66.1% of the patients were discharged from hospital and 33.9% were referred to coronary angiography while still in hospital. Of these, 87 patients (85%) presented significant coronary obstructions (reduction of 50% or more of the arterial lumen28) and 68 (22.6%) patients were
submitted to surgical or percutaneous revascularization while still in hospital.
The mean follow-up period was 697.7dias ± 326.6 days, in that it was impossible to complete the follow up of 28 patients due to failure to contact the patient, the assistant doctor or family members by phone. These patients were excluded from the analysis of prognosis.
We did not find any significant statistical correlation in our sample between clinical and scintigraphic variables and the occurrence of a primary outcome. There was only a trend towards statistical significance between the presence of altered scintigraphy (1.71 as compared with 6.04%; p = 0.086) and the occurrence of a primary outcome within one year.
With regard to the type of stress employed, the group of patients submitted to pharmacological stress presented a higher rate of secondary outcomes when compared with the group of patients submitted to physical stress (n = 44, 40% as compared with n = 103, 56%; p = 0.02) – Figure 1. Other clinical characteristics of these two groups are on Table 2.
The patients with altered scintigraphy (n=76) as compared with those with normal scintigraphy (n=22) presented a secondary outcome rate significantly higher in the follow-up period (77.5% as compared with 22.5%; p < 0.0001), just as those patients who presented isolated ischemia (n=73) as compared with patients who presented
Table 1 – Frequency of clinical variables according to the presence of ischemia
,6&+(0,$
Absent Present
Clinical variable n n p value
Gender Male
Female
70 89
44.0 56.0
94 48
66.2
33.8 < 0.0001
Hypertension 107 67.3 105 73.9 0.20
Diabetes 20 12.6 31 21.8 0.033
Dyslipidemia 85 53.5 77 54.2 0.89
Sedentary lifestyle 80 50.3 70 49.3 0.86
Family history of CAD 78 49.1 72 50.7 0.77
Obesity 29 18.2 30 21.3 0.50
Smoking habit 17 10.7 17 12.0 0.72
Previous AMI 25 15.7 52 36.6 < 0.0001
Previous SMR 22 13.8 46 33.1 < 0.0001
Previous PTCA 37 23.3 68 47.9 < 0.0001
normal tests (n=25) (74.5% as compared with 25.5%; p < 0.0001). The presence of fibrosis alone did not correlate with a higher occurrence of secondary outcome (p=0.10). When we stratified the patients according to the number of segments with ischemia we verified that patients with 1 to 2 (n=19) myocardial segments with ischemia and those with 3 or more (n=54) segments with ischemia presented a higher number of secondary outcomes when compared with patients without ischemia (n=25) (p=0.0001). However, the two first groups did not present statistically significant differences between them (Figure 2).
Patients with ejection fraction below 45% (n=21) presented a rate of secondary outcomes which was significantly higher than patients with LVEF above 45% (n=72) (relative risk = 1.72, confidence interval 95% = 1.38 to 2.06; p=0.006).
Multivariate analysis - No clinical or scintigraphic variable was selected by the multivariate analysis to explain the occurrence of the primary outcome. The loss of significant variables to the level of 5% is probably due to the small number of patients who presented primary outcome (n=13).
The presence of myocardial ischemia was the major independent variable to explain the occurrence of secondary outcome (Relative Risk = 6.5; Confidence Interval 95% = 1.61 to 26.83, standard error = 0.717; p=0.009) followed by history of previous PTCA (Relative Risk = 3.8; Confidence Interval 95% = 1.95 to 7.70, standard error = 0.35; p<0.0001) and previous SMR (Relative Risk =
Fig. 1 -Graphic demonstrating the secondary outcome rate according to the W\SHRIVWUHVVHPSOR\HGDQGWKHVFLQWLJUDSKLFILQGLQJVS S
20% 15%
54%
40%
0% 10% 20% 30% 40% 50% 60%
Physical Pharmacological
Normal Abnormal
**
*
p=0.02
Table 2 – Analysis of clinical variables relative to the occurrence of combined events
Combined Events
Absent Present
Clinical variable Category n n p value
Gender Male
Female
87 88
49.7 50.3
65 33
66.3
33.7 0.008
Hypertension yes 123 70.3 66 67.4 0.61
Diabetes yes 29 16.6 19 19.4 0.55
Dyslipidemia yes 96 54.9 54 55.1 0.96
Sedentary lifestyle yes 90 51.4 41 41.8 0.12
Family history of CAD yes 81 46.3 50 51.0 0.45
Obesity yes 37 21.1 12 12.4 0.071
Smoking habit yes 17 9.7 13 13.3 0.36
Previous AMI yes 35 20.0 36 36.7 0.002
Previous SMR yes 27 15.5 36 37.5 < 0.0001
Previous PTCA yes 42 24.0 57 58.2 < 0.0001
CAD - coronary artery disease; AMI - acute myocardial infarction; SMR - surgical myocardiatl revascularization; PTCA - percutaneous transluminal coronary angioplasty.
Fig. 2 -Graphic demonstrating the frequency of combined events according WRWKHQXPEHURIVHJPHQWVZLWKLVFKHPLDQVQRWVLJQLILFDQWVHJ QR P\RFDUGLDOVHJPHQWZLWKLVFKHPLDRQVFLQWLJUDSK\WRVHJ RQHRUWZR P\RFDUGLDOVHJPHQWVRQVFLQWLJUDSK\VHJ WKUHHRUPRUHP\RFDUGLDO segments on scintigraphy.
2.41;Confidence Interval 95% = 1.17 to 4.97, standard error = 0.36, p=0.01).
Analysis of event-free survival - Survival free of primary outcome presented a trend to be higher for the group of patients with normal scintigraphy (p=0.086) (Figure 3).
We observed that there is significant difference (p=0.0001) in the curve for survival free of secondary outcome between the groups of patients without ischemia and the groups with one or two and three or more segments with ischemia, but we did not observe a significant difference between the two latter ones (Figure 4).
The patients who presented left ventricle ejection fraction below 45% also presented shorter survival free of secondary outcome (p=0.001) (Figure 5).
Discussion
Our study demonstrated that patients admitted into the
Fig. 4 -Curve of survival free of secondary outcome according to the number of segments with ischemia.
Time (days)
Su
rv
iv
a
l
fr
e
e
o
f
s
e
c
o
n
d
a
ry
o
u
tc
o
m
e
(%
)
0 120 240 360 480 600 720 840 960 0
30 p(Log-rank)
= 0.0001
30 40 50 60 70 80 90 100
without ischemia 1 or 2 segments 3+ segments
chest pain unit with suspected ACS can benefit from the use of stress myocardial perfusion scintigraphy, because this test was able to determine the prognosis in the medium term. The presence of myocardial ischemia on scintigraphy in this group of patients was associated with a 6.5 times higher risk for combined adverse events as compared with the patients with normal scintigraphy.
Some clinical characteristics should be taken into account in the global assessment of the impact of a complementary test. Although the mean age of the population studied was higher than in other studies carried out in a chest pain unit20,22,
stress myocardial scintigraphy proved viable, safe and effective in the determination of the prognosis.
The male gender has been associated with a higher rate of altered scintigraphies. Miller et al29 demonstrated
a higher frequency of tests with ischemia in male patients (58% as compared with 31%; p<0.001) and verified that these patients were more frequently referred to coronary
Fig. 3 -Curve of survival free of primary outcome according to the presence of altered scintigraphy.
Time (days)
\Su
rv
iv
a
l
fr
e
e
o
f
p
ri
m
a
ry
o
u
tc
o
m
e
(%
)
0 60 120 180 240 300 360 420 480 540 600
0
80 p(log-rank)= 0.086 Cintilografia positiva Cintilografia negativa
80 82 84 86 88 90 92 94 96 98 100
Normal scintigraphy
angiography (17% as compared with 8%; p < 0.001)29. In
our sample, the male gender correlated with the presence of ischemia on myocardial scintigraphy. However, in the multivariate analysis, it did not present an independent correlation with adverse events.
A history of previous AMI, SMR or PTCA correlated with the occurrence of a secondary outcome. We did not find any similar paper in the literature that assessed the prognostic value of MPS in a population with these characteristics – with a high prevalence of coronary artery disease30. In all, 140 patients
(46%) presented a previous history of coronary artery disease and these variables correlated with the presence of ischemia and adverse events. Elhendy et al. assessed 218 patients and demonstrated that a previous history of coronary disease was the major factor to predict adverse events31.
Acampa et al demonstrated that patients with a negative scintigraphy for ischemia had a lower risk of heart events in the long term than patients who presented ischemia, demonstrating that even patients who knowingly have coronary artery disease benefit from the performance of MPS, and comparing with the patients who presented negative stress echocardiogram for ischemia, the latter had more adverse events when compared with patients who presented negative MPS for ischemia (14% as compared with 9%; p<0.001)3.
Pharmacological stress correlated with the presence of altered tests (p=0.04) and with the occurrence of secondary outcome (p=0.02), but was not significant regarding the occurrence of primary outcome (p=0.08). In agreement with the literature, we found a higher rate of adverse heart events in the group of patients who were submitted to pharmacological stress both for patients with normal tests and for those with altered tests33,34. We believe that this was due to the fact
that the population submitted to pharmacological stress was comprised of patients with more severe cardiac disease than the population submitted to physical stress.
According to the multivariate analysis, the major independent variable to predict secondary outcomes was
the presence of myocardial ischemia. This result is similar to the results obtained in several papers published where the presence of ischemia correlated with a higher rate of adverse events in patients admitted with suspected ACS20,22,27,35,36.
Based on the results obtained in this study, we believe that patients admitted into the CPU with suspected ACS and with a normal MPS present low risk of adverse events within one year. We found a rate of primary outcome of 1.71% within one year for the patients with altered scintigraphy, as compared with 6.04% for patients with normal tests. Our results, although they present only a trend towards statistical significance (p=0.086) for the occurrence of primary outcome are in accordance with the literature19,31,37-39 (Chart 1).
Studies which assessed the prognostic value of myocardial scintigraphy demonstrated that when this test presents altered results it has an independent predictive value for major heart events (death or myocardial infarction)27,40,41. The population
that presents altered tests presents a risk for severe adverse events which is 3 to 5 times higher than the population with normal tests, and the mean rate of events in the population with altered tests is 5.9% per year34. Shaw et al assessed
4,728 patients and verified that the rate of severe adverse events, death or AMI, in patients with normal MPS was 0.6% per year, in a three-year follow up42. However, higher
rates of severe events are expected for the population with a previous diagnosis of DAC or high risk of developing it. In this population, the yearly rate of events is approximately 2% per year34,42,43. Unlike other studies, we did not find a
significant statistical difference between patients with different ischemic loads and the presence of fibrosis alone did not present correlation with a higher rate of adverse events either19. Fesmire et al. did not find significant difference in the
occurrence of events in patients admitted into the CPU with suspected ACS and that presented different quantifications of ischemic areas44.
Ejection fraction is important information for prognosis and can be assessed on MPS when we use ECG-gated
Fig. 5 -Curve of survival free of combined outcome according to post stress LVEF. LVEF - left ventricle ejection fraction. Time (days)
Su
rv
iv
a
l
fr
e
e
o
f
s
e
c
o
n
d
a
ry
o
u
tc
o
m
e
(%
)
0 120 240 360 480 600 720 840 960
0
30 p(Log-rank)= 0.001
30 40 50 60 70 80 90 100
References
1. Yusuf S, Collins R, Peto R, Furberg C, Stampfer MJ, Goldhaber SZ, et al. Intravenous and intracoronary fibrinolytic therapy in acute myocardial infarction: overview of results on mortality, reinfarction and side-effects from 33 randomized controlled trials. Eur Heart J. 1985; 6: 556-85.
2. Lee TH, Rouan GW, Weisberg MC, Brand DA, Acampora D, Stasiulewicz C, et al. Clinical characteristics and natural history of patients with acute myocardial infarction sent home from the emergence room. Am J Cardiol. 1987; 60: 219-24.
3. Bassan R; Gibler W B. Unidades de dolor torácico: estado actual del manejo de pacientes com dolor torácico em los servicios de urgências. Rev Esp Cardiol. 2001; 54: 1103-9.
4. Kontos MC, Jesse RL, Anderson P, Schimidt KL, Ornato JP, Tatum JL. Comparison of myocardial perfusion imaging and cardiac troponin in patients admitted to the emergency department with chest pain. Circulation. 1999; 99: 2073-78.
5. Gibler WB, BlonkaIns AL. Diagnosis of acute coronary syndromes in the emergency department. In: Topol EJ, ed. Acute coronary syndromes. 2nd ed. New York: Marcel Dekker; 2001. p. 293-327.
6. Mair J. Progress in myocardial damage detection: new biochemical markers for clinicians. Crit Rev Clin Lab Sci. 1997; 34: 1-66.
7. Newby LK, Christenson RH, Ohman EM, Armstrong PW, Thompson TD, Lee Chart 1 - Prognostic value of MPS in the prediction of major adverse heart events (death or AMI)
Author/year n Method/scenario 1HJDWLYHWHVW
x events/year Positive test x events/year
Elhendy, 200519 458 Stress MPS/outp 1.5% 4.5%
Elhendy, 200331 218 Stress MPS/outp 0.7%
-Stratmann, 199437 534 Stress MPS/outp 1.6% 8.7%
Geleijnse, 199738 392 Stress MPS/outp 0.8% 14.3%
Heller, 199539 512 Stress MPS/outp 1.3% 6.9%
Azevedo, 2007 301 Stress MPS/CPU 1.71% 6.04%
MPS - myocardial perfusion scintigraphy; Outp - outpatient facility; CPU - chest pain unit.
image acquisition45. In our study we verified that patients
with ejection fraction below 45% presented a higher rate of secondary outcomes but we found no statistical significance for the occurrence of primary outcomes. We believe that this was partly due to the small number of events for primary outcome. Travin et al. in a study with 3,207 patients demonstrated that the patients who presented ejection fraction below 50% presented a higher cumulative rate of heart events, AMI and heart death, 13.1% as compared with 3.7% of events (p < 0.001) in the group of patients with ejection fraction above 50%46.
In our study the low incidence of adverse events in the medium term for patients with negative scintigraphy suggests that the existence of coronary injury, at the time of test, was not the cause of the chest pain symptom that led to hospitalization or that, even when such injury was present, the degree of obstruction was not significant so as to require intervention treatment at that time.
Our study has some limitations: the data were analyzed retrospectively, 28 patients were not followed up, and the study was carried out in a tertiary hospital that is a reference for the treatment of cardiovascular diseases to where patients with severe conditions and with a high degree of prevalence of preexisting cardiopathy are referred. The combined adverse events included a rate of myocardial revascularization in the follow up. This variable may suffer direct influence from the decision of the assistant doctor and the result of the scintigraphy, although we have not
considered the revascularization procedures carried out in the index-hospitalization. The decision to include this variable was based on the other studies which include it as well32. Another limitation was the performance of coronary
angiography in a limited group of patients. This fact interferes on the analysis of the diagnostic capacity of scintigraphy, although it does not seem to interfere with the analysis of the prognosis. The patients referred to stress scintigraphy at the CPU of our institution are pre-selected according to a local risk stratification protocol and therefore our results might not be applicable to the population of patients admitted with chest pain into the emergency room.
Conclusion
We conclude that stress myocardial perfusion scintigraphy is able to determine in the medium term the prognosis of patients admitted into the CPU with suspected ACS, after the diagnostic of AMI and high risk unstable angina have been ruled out. The presence of myocardial ischemia on scintigraphy presented an independent contribution in the multivariate analysis to predict adverse events.
Acknowlegments
KL, et al. Value of serial troponin T measures for early and late risk stratification in patients with acute coronary syndromes. The GUSTO-IIa Investigators. Circulation. 1998; 98: 1853-9.
8. Swinburn JMA, Stubbs P, Soman P, Collinson P, Raval U, Senior R. Rapid assessment of patients with non-ST-segment elevation acute chest pain: Troponins, inflamatory markers, or perfusion imaging. J Nucl Cardiol. 2002; 9: 491-9.
9. Ewy GA, Ornato JP. 31st Bethesda Conference. Emergency Cardiac Care. Task force 1: cardiac arrest. J Am Coll Cardiol. 2000; 35 (4): 832-46.
10. Goldman L, Cook EF, Johnson PA, Brand DA, Rouan GW, Lee TH. Prediction of the need for intensive care in patients who come to the emergency departments with acute chest pain. N Engl J Med. 1996; 334: 1498-504.
11. Collinson P O, Premachandram S, Hashemi K, Lee KR. Prospective audit of incidence of prognostically important myocardial damage in patients discharged from emergency department: time for improved diagnosis and management of patients presenting with acute chest pain. BMJ. 2000; 320: 1702-5.
12. McCarthy BD, Beshansky JR, D’Agostino RB, Selker HP. Missed diagnosis of acute myocardial infarction in the emergency department: results from a multicenter study. Ann Emerg Med. 1993; 22: 579-82.
13. Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000; 342: 1163-70.
14. Bahr RD. Chest pain centers: moving toward proactive acute coronary care. Int J Cardiol. 2000; 72 (2): 101-10.
15. Farkouh ME, Smars PA, Reeder GS, Zinsmeister AR, Evans RW, Meloy TD, et al. A clinical trial of a chest-pain observation unit for patients with unstable angina. N Engl J Med. 1998; 339: 1882-8.
16. Achenbach S, Giesler T, Ropers D, Ulzheimer S, Derlien H, Schult C, et al. Detection of coronary artery stenoses by contrast-enhanced, retrospectively electrocardiographically-gated, multislice spiral computed tomography. Circulation. 2001; 103: 2535-8.
17. Rodrigues ARV, Barbosa MR, Brito MSV, Silva LC, Machado FS. Angiografia coronariana minimamente invasiva através de tomografia com múltiplos detectores. Arq Bras Cardiol. 2006; 86: 323-30.
18. Conti A, Gallini C, Costanzo E, Ferri P, Matteini M, Paladini B, et al. Early detection of myocardial ischemia in the emergency department by rest or exercise 99mTC tracer myocardial SPET in patients with chest pain and non-diagnostic ECG. Eur J Nucl Med. 2001; 28: 1806-10.
19. Elhendy A, Schinkel AFL, van Domburg RT, Bax JJ, Valkema R, Huurman A, et al. Risk stratification of patients with angina pectoris by stress 99mTc-Tetrofosmin myocardial perfusion imaging. J Nucl Med. 2005; 46: 2003-8.
20. Fesmire FM, Hughes AD, Fody EP, Jackson AP, Fesmire CE, Gilbert MA, et al. The enlarger chest pain evaluation protocol: a one year serial 12-lead ECG monitoring, Two-Hour delta serum marker measurements, and selective nuclear stress testing to identify and exclude acute coronary syndromes. Ann Emerg Med. 2002; 40: 584-94.
21. Abbot BG; Jain D. Symposium on myocardial perfusion imaging in acute coronary syndromes. Nucl Med Commun. 2003; 24: 1061-9.
22. Conti A, Zanobetti S, Grifoni S, Berni G, Costanzo E, et al. Symposium on myocardial perfusion imaging in acute coronary syndromes. Implementation of myocardial perfusion imaging in the early triage of patients with suspected acute coronary syndromes. Nucl Med Commun. 2003; 24: 1055-60.
23. Bassan R, Scofano M, Gamarskii R, Dohmann HF, Pimenta L, Volschan A, et al. A dor torácica na sala de emergência: a importância de uma abordagem sistematizada. Arq Bras Cardiol. 2000; 74: 13-21.
24. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, et al. ACC/AHA 2002 Guideline Update for the Management of Patients With Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction - Summary Article A Report of the American College of Cardiology / American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol. 2002; 40: 1366-74.
25. Gibler WB, Cannon CP, Blomkalns AL, Char DM, Drew BJ, Hollander JE, et al. Practical implementation of the Guidelines for Unstable
Angina/Non–ST-Segment Elevation Myocardial Infarction in the Emergency Department. A Scientific Statement From the American Heart Association Council on Clinical Cardiology (Subcommittee on Acute Cardiac Care), Council on Cardiovascular Nursing, and Quality of Care and Outcomes Research Interdisciplinary Working Group, in Collaboration With the Society of Chest Pain Centers. Circulation. 2005; 111: 2699-710.
26. Cerqueira MD, Weissman NJ, Dilsizian V, Jakobs AK, Kaul S, Laskey WK. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the cardiac imaging committee of the council on clinical cardiology of the American Heart Association. Circulation. 2002; 105: 539-42.
27. Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS. Stress myocardial perfusion single-photon emission computed tomography is clinically effective and cost effective in risk stratification of patients with a high likelihood of coronary artery disease (CAD) but no known CAD. J Am Coll Cardiol. 2004; 43: 200-8.
28. Smith SC, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ, et al. ACC/AHA guidelines for percutaneous coronary intervention: executive summary and recommendations: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1993 Guidelines for Percutaneous Transluminal Coronary Angioplasty). J Am Coll Cardiol. 2001; 37: 2215-38.
29. Miller TD, Roger VL, Hodge DO, Hopfenspirger MR, Bailey KR, Gibbons RJ. Gender differences and temporal trends in clinical characteristics, stress test and use of invasive procedures in patients undergoing evaluation for coronary artery disease. J Am Coll Cardiol. 2001; 38: 690-7.
30. Shaw LJ, Peterson ED, Kesler K, Hasselblad V, Califf RM. A metanalysis of predischarge risk stratification after acute myocardial infarction with stress electrocardiographic, myocardial perfusion, and ventricular function imaging. Am J Cardiol. 1996; 78: 1327-37.
31. Elhendy A, Schinkel A, Bax JJ, van Domburg RT, Poldermans D. Long-term prognosis after a normal exercise stress Tc-99m sestamibi SPECT study. J Nucl Cardiol. 2003; 10: 161-6.
32. Acampa W, Spinelli L, Petretta M, Salvatore M, Cuocolo A. Comparison of prognostic value of negative dobutamine stress echocardiography versus Single-Photon Emission Computed Tomography after acute myocardial infarction. Am J Cardiol. 2005; 96: 13-6.
33. Navare SM, Mather JF, Shaw LJ, Fowler MS, Heller GV. Comparison of risk stratification with pharmacologic and exercise stress myocardial perfusion imaging: a meta-analysis. J Nucl Cardiol. 2004; 11: 551-61.
34. Shaw LJ, Iskandrian AE. Major achievements in nuclear cardiology: III – Prognostic value of gated myocardial perfusion SPECT. J Nucl Cardiol. 2004; 11: 171-85.
35. Conti A, Sammicheli L, Gallini C, Costanzo EN, Antoniucci D, Barletta G. Assessment of patients with low-risk chest pain in the emergency department: head-to-head comparison of exercise stress echocardiography and exercise myocardial SPECT. Am Heart J. 2005; 149: 894-901.
36. Underwod SR, Anagnostopoulos C, Cerqueira M, Ell PJ, Flint EJ, Harbinson M, et al. Myocardial perfusion scintigraphy: the evidence. A consensus conference organised by the British Cardiac Society, the British Nuclear Cardiology Society and the British Nuclear Medicine Society, endorsed by the Royal College of Physicians of London and the Royal College of Radiologists. Eur J Nucl Med Mol Imaging. 2004; 31: 261-91.
37. Stratmann HG, Tamesis BR, Younis LT, Witry MD, Miller DD. Prognostic value of dipyridamole technetium-99m sestamibi myocardial tomography in patients with stable chest pain who are unable to exercise. Am J Cardiol. 1994; 73: 647-52.
38. Geleijnse ML, Elhendy A, van Domburg RT, Cornel JH, Rambaldi R, Salustri A, et al. Cardiac imaging for risk stratification with dobutamine-atropine stress testing in patients with chest pain. Echocardiography, perfusion scintigraphy, or both? Circulation. 1997; 96: 137-47.
39. Heller GV, Herman SD, Travin MI, Baron JI, Santos-Ocampo C, McClellan JR. Independent prognostic value of intravenous dipyridamole with technetium-99m sestamibi tomographic imaging in predicting cardiac events and cardiac related hospital admissions. J Am Coll Cardiol. 1996; 26: 1202-8.
artery disease: incremental prognostic value and use in risk stratification. Circulation. 1996; 93: 905-14.
41. Lee DS, Jang MJ, Cheon GJ, Chung JK, Lee MC. Comparison of the cost-effectiveness of stress myocardial SPECT and stress echocardiography in suspected coronary artery disease considering the prognostic value of false-negative results. J Nucl Cardiol. 2002; 9: 515-22.
42. Shaw LJ, Hendel R, Borges-Neto S, Lauer MS, Alazraki N, Burnette J, et al. Prognostic value of normal exercise and adenosine 99mTc-tetrofosmin SPECT imaging: for the myoview multicenter registry: results from the multicenter registry of 4,728 patients. J Nucl Med. 2003; 44: 134-9.
43. Hachamovitch R, Hayes S, Friedman J D, Cohen I, Shaw LJ, Germano G, et al. Determinants of risk and its temporal variation in patients with normal stress myocardial perfusion scans: what is the warranty period of a normal scan? J
Am Coll Cardiol. 2003; 41: 1329-40.
44. Fesmire FM, Hugues AD, Stout PK, Wojcik JF, Wharton DR. Selective dual nuclear scaning in low-risk patients with chest pain to reliably identify and exclude acute coronary syndromes. Ann Emerg Med. 2001; 38: 207-15.
45. Sharir T, Germano G, Kang X, Lewin HC, Miranda R, Cohen I, et al. Prediction of myocardial infarction versus cardiac death by gated myocardial perfusion SPECT: Risk stratification by the amount of stress-induced ischemia and the post-stress ejection fraction.J Nucl Med. 2001; 42: 831-7.