w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Manometric
analysis
of
the
influence
of
rectal
content
on
anal
pressures
in
chronically
constipated
patients
Rodrigo
Ciotola
Bruno
a,∗,
Fang
Chia
Bin
a,
Maria
Auxiliadora
Prolungatti
César
a,b,
Wilmar
Artur
Klug
a,
Sylvia
Heloisa
Arantes
Cruz
aaFaculdadedeCiênciasMédicasdaSantaCasaSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
bDepartmentofMedicine,UniversidadedeTaubaté(UNITAU),Taubaté,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8October2014 Accepted2February2015 Availableonline2February2015
Keywords: Constipation Manometry Rectaldiseases
a
b
s
t
r
a
c
t
Objective:Theaimofourstudywastoanalyzewhetherthepresenceofcontentinthe rec-tuminfluencestheanorectalmanometryexaminationresultsinchronicallyconstipated patients.
Methods:Weevaluated38chronicallyconstipatedpatients,36womenand2men,withan averageageof53.55yearsofage,allwithascoreabove10ontheAgachanConstipation ScoringSystem.Allthepatientsunderwentrectalpreparationandthenhadtheanorectal manometryexaminationwithoutrectalcontentandafter5minhaditwitharectalballoon inflatedwith200mlofairintherectum.
Statisticalanalysis:Thestatisticalparametricpaired-ttestwasappliedinordertoverifythe differenceinresponsebetweenthegroupsafteranintervention,adoptingasignificantlevel of5%(p<0.05).
Results:Theanalpressurewasanalyzedfromthestandardanalmanometryexamination andwefoundastatisticallysignificantinfluenceonthemanometricresultsforthepatients’ averagerestingpressures,absoluteaveragecontractions,averagecontractions,evacuations, andsustainedcontractionsinthefunctionalanalcanals.
Conclusion:Thepresenceofrectalcontentinfluencesthemanometricvaluesofaverage res-tingpressure,averageabsolutecontraction,averagecontraction,evacuation,andaverage sustainedcontractionsinthefunctionalanalcanalinthegroupofchronicallyconstipated patients.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](R.C.Bruno). http://dx.doi.org/10.1016/j.jcol.2015.01.004
Análise
Manométrica
da
Influência
do
Conteúdo
Retal
nas
Pressões
Anais
em
Pacientes
Cronicamente
Constipados
Palavraschave: Constipac¸ão Manometria Doenc¸asRetais
r
e
s
u
m
o
Objetivo: Oobjetivodesteestudofoianalisarseapresenc¸adeconteúdonoretoinfluencia osresultadosdoexamedemanometriaanorretalempacientescronicamenteconstipados. Métodos: Foram avaliados38 pacientescronicamente constipados, 36 mulherese dois homens,commédiade53,55anosdeidade,todoscompontuac¸ãoacimade10noAgachan ConstipationScoringSystem.Todosospacientesforamsubmetidosapreparoretale,em
seguida,passaramporumexamedemanometriaanorretalsemconteúdoretale,depois
detranscorridoscincominutos,umnovoexamefoirealizado,agoracomumbalãoretal infladocom200mldearnoreto.
Análiseestatística: Naanáliseestatística,foiaplicadootestetparamétrico,comafinalidade deverificaradiferenc¸a,emtermosderesposta,entreosgruposapósumaintervenc¸ão.Para tanto,foiadotadoumníveldesignificânciade5%(P<0,05).
Resultados: Apressãoanalfoianalisadacombasenoexamedemanometriaanalderotina; emnossospacientes,foiobservadainfluênciaestatisticamentesignificativanos
resulta-dos manométricosparaas pressõesmédiasem repouso,contrac¸õesmédiasabsolutas,
contrac¸õesmédias,evacuac¸õesecontrac¸õessustentadasnoscanaisanaisfuncionais. Conclusão: Apresenc¸adeconteúdoretalinfluenciaosvaloresmanométricosdapressão médiaemrepouso,contrac¸ãoabsolutamédia,contrac¸ãomédia,evacuac¸ão,econtrac¸ões sustentadasmédiasnocanalanalfuncionalnogrupodepacientescronicamente constipa-dos.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Changesinbowelmovements,suchasconstipationandfecal
incontinence,are someofthemostcommon
gastrointesti-naldisordersinthegeneralpopulation,ranginginAmerican adultsfrom15%1to20%.2,3Amongthem,constipationismost prevalent,andcanaffectupto27%ofAmericans.3–5Thehigh frequencyofthisdisorder,anditshighcost,justifythe impor-tancegiventotheproblem.
From a clinical standpoint, constipationis defined as a
bowelalteration basedonunsatisfactoryevacuation, andit
maybeassociatedwithaninfrequentbowelmovement,
diffi-cultyinpassingstool,orboth.6,7
TheRome III criteria definedfunctional constipation as
occurrenceof2ormoresymptomsforatleast12weeksinthe
absenceofstructuralexplanation.Thesymptomsare
unspe-cific self-reported symptoms, stool frequency of less than
threebowel movementsperweek,guttransittimeofmore
than68h,analblockage,manualmaneuverstodefecate,loose
stoolsareararely presentwithout the use oflaxatives and
thereareinsufficientcriteriaforirritableboweldisease.8–11
In order to classify the prevalence and severity of the
constipation,theAgachanConstipationScoringSystemwas
used.12
Complete evaluationof chronically constipatedpatients
shouldbebasedonamedicalhistoryanddirectedphysical
examination,13andinthemostseverecasessupplemented
withspecificanorectalphysiologyexaminations.11,14
Anorec-tal manometry is considered to be the most important
of these examinations and provides detailed information
on the motor and sensory activities in the region being
studied.4,5,15–18
International gastroenterology and coloproctology
soci-etieshavestandardizedthemethodologyandinterpretation
ofthisanorectalmanometryexamination.15
Thus,consideringtheimportanceofthisexaminationand
reviewingthemedicalliteratureonanorectalmanometryin
chronicallyconstipatedpatients,thereremainsthequestion
ofwhetherthepresenceofcontentintherectuminfluences,
ornot,theexaminationresults.
Cleaning of the rectum before manometry is especially
importantinchronicallyconstipatedpatients,asthepresence
oflargeamounts offecesinthe rectummay influencethe
positioningofthecatheter.18Irrespectiveofthesehypotheses,
anorectalphysiologyservicesignorethisandperformrectal
examinationswithoutrectalpreparation,11,19–22whileothers emptytherectalampullabeforetheexamination.2,5,18
Given this, and not having found in the literature any
clearreferencestotheimportanceorotherwiseofpre-existing
content in the rectum or prior preparation for anorectal
manometry, we came up with this comparative study, in
which weevaluatedthe examinationinquestionwith and
withoutrectalcontentinchronicallyconstipatedpatients.To
simulate thepresenceofcontent intherectum duringthe
examination,weinsertedaninflatedrectalcatheterballoon
and compared it with the data obtained with the balloon
deflated.
Theobjectiveofthispaper,then,istoanalyzewhetherthe
presenceofknowncontentintroducedtotherectalampulla
influencestheanorectalmanometryexaminationresultsin
Material
Weevaluatedthedataobtainedfromtheanorectal
manom-etryexaminationscarriedouton38chronicallyconstipated
patientsatthe ColoproctologyClinicattheUniversity Hos-pitalatTaubatéUniversity(UNITAU)fromJuly2010toApril 2011.
Method
Thisisaprospectivestudywithchronicallyconstipatedadult
patients at the Coloproctology Clinic, at UNITAU
Univer-sityHospital.AllofthepatientsmettheRome III23criteria
and scored above 10 onthe Agachan Constipation Scoring
System.12Thepatientssignedaninformedconsentformand
thestudywasapprovedbytheEthicsCommitteeUniversity
HospitalatTaubatéUniversity(UNITAU).
We excluded patients with anorectal diseases known
to lead to impairment in anorectal manometry values,
suchasgradeIVhemorrhoids,analfissures,and fistulas.24
Associated with these, we also excluded patients who
had had anorectal surgery, abdominal pain concomitant
withamanometryexamination,organic diseasediscovered
throughcolonoscopy,patientswithirritablebowelsyndrome,
megacolon,24 those who used oral antihypertensive drugs
basedoncalciumchannelblockers,11andpatientswhohad
notbeensuccessfullyrectallyprepared.
All 38 patients underwent the anorectal manometry
examinationhavingpreviouslybeen rectallyprepared. The
preparationwascarriedoutwithasorbitol-basedstimulant
andsodiumlaurylsulphate,applyinga5mlvialrectallythe daybeforeandtwovials2hbeforetheexamination.
Eachexaminationwasconductedintwophases:thefirst
phasewiththerectalballoondeflated,andsoonafter, with-outremovingthecatheterfromtheanorectalregion.Thefirst
phasewascalledgroup1.Theexaminationwasrepeated,but
thistimewiththerectalballooninflatedintherectalampulla, simulatingfecalcontentintherectum.Thesecondphasewas calledgroup2.
Nodigitalrectalexaminationwascarriedoutinadvance,
soasnottocompromisethetoneoftheanalsphincters.
Thestudywasbasedonthestandardanorectal
manom-etry examination, measuring pressure at rest, contraction,
absolute contraction, evacuation, maintained contraction,
sustentioncapacity, andfatiguerate forthe anal sphincter
muscles,centimeterbycentimeter,from5cmfromtherectum (Fig.1).Followingthisstep,rectalsensitivitywasanalyzedby measuringtheanalinhibitoryreflex,thelowestsensitive vol-umeintherectum,andthevolumeforthedesireforconstant
evacuation.Themaximumrectalcapacitywasnotanalyzed,
inordernottocompromisethenextphaseoftheexamination.
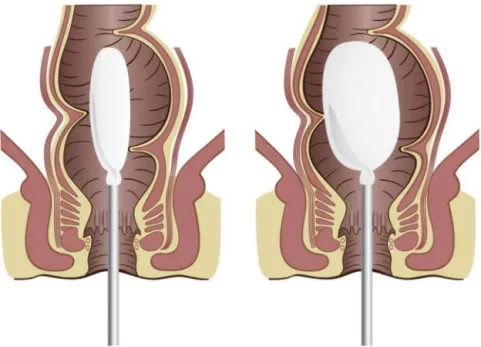
Attheendofthisphase,thecatheterballoonwasslowly
inflatedintherectalampulla,approximately 5cmfromthe
analverge,with200mlofair,tofilltheentirerectalampulla andthussimulatearectumwithcontent(Fig.1).5,25Wewaited forapproximately5min5fortherectalandsphinctermuscles tosettle.Thecatheterwasthenwithdrawn,andallthe
mea-surementswerecomparedwiththosetakenwithadeflated
balloon.
Statistical
analysis
The statistical analysis evaluated possible differences
between the data obtained in anorectal manometry
per-formedinchronicallyconstipatedpatientswithandwithout
rectalcontent.
Forthispurpose,thestatisticalparametricpaired-ttestwas appliedinordertoverifythedifferenceinresponsebetween thegroupsafteraninterventionadoptingasignificantlevel of5%(p<0.05).Theanalysiswasperformedwiththesoftware SPSSStatisticsversion22.
Results
Inthisstudy,outof38patients,36(94.7%)werefemaleand
onlytwo(5.3%)weremale. Theaverageageofthepatients
was53.55yearsold,themainagegroupbeingthatbetween
thefifthandsixthdecadesoflife,accountingfor65.78%ofthe sample.
Thesamplescoredanaverageof17.66outofamaximumof
30ontheAgachanConstipationScoringSystem,illustratinga highlevelofconstipationforthegroupaverage.Inthissame
sample,21patients(55.26%)hadsevereconstipation,witha
scoreofmorethan18points.
Withregardtothetimeofonsetofthesymptomstodate,11 patients(28.9%)hadanaveragetimeof5–10years;13patients (34.2%)from10to20years;9patients(23.7%)hadmorethan
20 years,and onlyfive ofthe 38 patients(13.2%)had been
constipatedforaperiodof1–5years.
Theaveragelengthofthepatients’functionalanalcanal
was2.42cm,whichisinlinewiththeanatomicalstandard,
with94.7%ofthesepatientsbeingfemale.
Intherectalsensitivitytest,thesmallestsensitivevolume intherectumwasanaverageof33.29ml,andinitialvolumefor thedesireforconstantevacuationwasanaverageof53.29ml ofHg.
Theanorectalpressuresanalyzedinthemanometry
exam-inationsinbothgrouponeandgrouptwoarecomparedbelow,
showinganimportantandstatisticallysignificantdifference betweenthepressuresatrest,contraction,absolute contrac-tion,evacuation,andsustainedcontraction.Neithertherate
offatiguenorthecontractionsustentioncapacityshoweda
statisticallysignificantdifference.
The following Table 1 compares the average resting
pressures, the absolute contraction pressure, contraction
pressuresaverageandaverageevacuationpressurefor3cm
fromtheanalcanal.
Table2comparestheaveragesustainedcontraction pres-sureinthefunctionalanalcanalsofchronicallyconstipated patientsingroups1(rectalballoondeflated)and2(rectal bal-looninflated),obtainingstatisticallysignificantresults.
Discussion
Anorectal manometry is part of the study protocol for
Fig.1–Simulationofanorectalmanometryexaminationwithandwithouttherectalballoondeflated.
Table1–Comparisonwiththepressuresfoundduringanorectalmanometryfrom3cmoftheanalcanalinchronically constipatedpatientsingroups1and2fromJuly2010toApril2011.
Groups Average
resting
Standard deviation
Absolute contraction
Standard deviation
Average contraction
Standard deviation
Evacuation Standard deviation
1 52.98 26.7 12.528 60.01 73.82 49.33 64.52 30.60
2 40.17 25.21 96.71 54.61 57.98 39.55 44.33 26.04
p=0.001 p<0.001 p<0.001 p<0.001
Source:ColoproctologyClinic–UNITAUUniversityHospital.
additiontotherebeingagreatdealofnon-comparable equip-mentandcriteriaintermsofmethodology.
There is also disagreement over whether or not there
shouldbepriorpreparationandwhetherornottherectal con-tentcaninfluenceresults.SeveralBrazilianandinternational
serviceshaveperformedanorectalmanometryexaminations
andpostedtheirresultsinextensivestudies,butwithoutthere beingany standardizationregardingrectal preparationand theimportanceoftheexistenceorotherwiseofsolidorother fecalwasteintherectum.
Klugetal.,27,28inhisstudiesattheFacultyofMedical Sci-encesatSantaCasainSãoPaulo,andCaesaretal.,11,20,21at
theDepartment ofMedicine,University ofTaubaté, donot
routinelycarryoutrectalpreparationbeforetheexamination. However,theworkpublishedbyauthorssuchasRaoetal.,5,25
Raza and Bielefeldt,2 Pfeifer et al.24 and Oliveira24
recom-mendsrectalpreparationinpatientspriortocompletionof
amanometrytestasroutine.
Rao et al. intheir work perform a500ml rectal enema
30minbeforetheexamination.5,25 RazaandBielefeldt,
how-ever,recommendedcleaningwithanenemaonthemorning
oftheexamination,alsoinordertoemptytherectalampulla.2
These authors believe that in chronically constipated
patients,notcleaningtherectalampullamayinfluencethe
positioningofthecatheter,influencingtheacquisitionofdata,
aswellasobstructingthechannels,compromisingthe
exam-inationresults,24 thisbeingoneofthereasonstoclean the rectum.
However,basedonthesedifferentstudies,theneedarose
todefinetheimportanceofcontentintherectum,whichcould
Table2–Comparisonbetweentheaveragessustainedcontractionpressureinthefunctionalanalcanalsofchronically constipatedpatientsingroups1and2fromJuly2010toApril2011.
Groups Numberof
patients
Minimum Maximum Average Standard
deviation
1 38 24.7 163 93.02 33.14
2 38 4.3 138.4 72.51 35.32
p<0.001
possiblyaltertheresultsofmanometrytestsandother exam-inations.Ifthecontentpresentintherectumofchronically constipatedpatientsdoesinterferewithanorectalmanometry results,besidestheneedtoestablishapreparationstandard,
then there is a need to more carefully interpret some of
theresultsobtainedand,furthermore,understandhowthese
functionaldisorderswork.
AuthorssuchasRazaand Bielefeldt andRaoand Singh
performdigitalrectalexaminationspriortointroducingthe manometrycatheter.2Klugetal.27,28 andCesaretal.,11,19–22
onthe other hand, donotbelieve thatthis dilation ofthe
sphinctermusclescouldcompromisetheexamination.
Thesampleof38patientsstudiedhereinhadamoderate
toseveredegreeofconstipation,accordingtothescoring
sys-temrecommendedbyAgachan.12Theminimumscorewas12
points,andthemaximumwas24points,withanaverageof
17.66,inarangefrom0to30.
In our study, the symptoms of constipation had been
present in75% ofthe patients formorethan 5years,and
in34.2%(13patients)theyhadbeenpresentfor10–20years,
with23.7%havingthemforover20years.Thesefigures
cor-roboratetheepidemiologicalconcernsheldbysomeBrazilian
andinternationalauthors,29,30whostressonlargesizeofthe groupaffectedbythisdisorderandthepsychological,social, andeconomicproblemsitcausesinoursocietyasawhole.
Thedataonrectalsensitivityanalyzedwerethefirst
sen-sation and the desireforconstant evacuation. The results
obtainedforthe lower sensitivevolume inthe rectum, on
inflatingtheballoon,producedvaluescompatiblewiththose describedintheliteratureforchronicallyconstipatedpatients, i.e.greaterthan30mmHg.5,24,31,32
Ineverydayclinicalpractice,themostreliablewayto mea-surerectalsensationisbymanualdistensionwithanair-filled balloon.31Thus,basedontheresultsformaximumtolerable
pressureintherectalampullainanorectalmanometry
sen-sitivitytestsfoundintheliterature,theballoonwasinflated with200mlofairtoperformthemanometrytestwithrectal content.2,5,24,28 Thisissufficientvolumetoshapetherectal
ampulla,stimulatingsensitivityandsimulatingthepresence
ofcontentintherectum,asoccursinchronicconstipation,
whencarryingouttheexaminationunprepared.31
Scottetal.31 in2011,whenanalyzingmotordysfunction
andrectalsensitivityinchronicallyconstipatedpatients,also
demonstrated the highest capacity ofthe rectum in these
patients,callingthemmegarectums(orcompliantrectums).
Thesetwofactors–greatercapacityoftherectalampulla
inthechronicallyconstipated31andthemaximumvolumeof
200mltofeelthedesiretoevacuate–ledustothisvalueforthe performanceoftheanorectalmanometrytestwithaninflated balloon.5
Inourresults, wefoundastatisticallysignificant
differ-ence inthepatients’ functional analcanalsinmostofthe
pressuresanalyzedwhenweconductedtheexaminationwith
andwithoutcontentintherectum.
Toachieveabetteranalysisofthepressures,wethen
com-pared,centimeterbycentimeterintheanorectalcanal,the
averageforthe3cmfromtheanalcanal,andtheaveragesfor thefunctionalanalcanalforeachpatient.
Analyzingtheaveragepressuresforthe3cmfromtheanal canalandtheaveragesofthepressuresforthefunctionalanal
canalatrest,absolutecontraction,contraction,andsustained
contraction fromgroup 1(withtherectal balloondeflated),
weconcludedthattheyare greaterthan thepressures and
average pressures in group2 (rectalballoon inflated), thus
showing,whencomparedwitheachother,statistically signif-icantdifferences.
Comparingcentimeterbycentimeter,therearesomeslight
differencesinthesemeasurementsbuttheydonotinterfere
withthefinalresult.Theratesoffatigueinanalcontraction
andsustentioncapacity,however,showednosignificant
dif-ferenceinanymeasurements.
Grouponeofoursample,with38examinationswiththe
rectalballoondeflated,wasatanaverageof3cmfromtheanal canalandtheaveragerestingpressuresforthefunctionalanal
canal were 52.98mmHgand 59.9mmHg, respectively,
com-paredwith40.17mmHgand48.9mmHgingroup2,withthe
rectalballooninflated.Thesamehappenedwiththeabsolute
pressureofcontractionfortheaverageof3cmfromtheanal
canaland the averageforthefunctional anal canal,which
hadvaluesof125.28mmHgand136.92mmHg,respectivelyin
the groupwiththeballoondeflated,and 114.47mmHgand
96.71mmHgingroup2.
Thefallinpressureincontraction,evacuation,and
sus-tained contraction both in the average forthe 3cm range
and the average for the functional anal canal was clear,
showing the influence that the rectal content has on rest
pressures.
Thefatigueratesand sustentioncapacityvaluesforthe
group withthe rectal balloon deflated compared with the
inflatedballoongroupshowednostatisticallysignificant inter-ferenceforthiscontentonpressures.
Wehave,therefore,demonstratedthatsomeofthe
sphinc-terpressuresmeasuredinanorectalmanometrytestsinthe
chronically constipatedvary depending onthe presenceor
otherwiseofrectalcontent.Thisiscertainlyimportant,given
thewidespreadandlargenumberofpatientswiththis
com-plaintinsocietyanditssocial,economic,andpsychological impacts.
The results found lead us to conclude that there is
a decrease in the average resting pressures in the
func-tional anal canal, in the average pressures for absolute
contraction in the functional anal canal, in the average
pressures forcontraction ofthe functional anal canal, and
in the average pressures for sustained contraction in the
group with examinations carried out with a full rectal
ampulla.
Fortheothervaluesmeasured,suchastherateoffatigue inanalcontractionandthesustentioncapacity,despitethere beingatendencyforthepressurestofall,theresultswerenot statisticallysignificant.
Inconclusion,itispossibletoidentifyanalterationinsome
measurementsofanalpressureinconstipatedpatientswith
intrarectalcontent.Andthepreparationisjustifiedpriorto theexaminationtoavoidsuchinterference.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. BenningaMA,ScottSM.Chronicconstipation.Preface.Best PractResClinGastroenterol.2011;25:1–2.
2. RazaN,BielefeldtK.Discriminativevalueofanorectal manometryinclinicalpractice.DigDisSci.2009;54:2503–11. 3. Lacerda-FilhoA,LimaMJ,MagalhaesMF,PaivaRdeA,
Cunha-MeloJR.Chronicconstipation–theroleofclinical assessmentandcolorectalphysiologicteststoobtainan etiologicdiagnosis.ArqGastroenterol.2008;45:50–7. 4. Remes-TrocheJM.Constipation:initialevaluationand
diagnosticapproach.RevGastroenterolMex.2005;70:312–22. 5. RaoSS,SinghS.Clinicalutilityofcolonicandanorectal
manometryinchronicconstipation.JClinGastroenterol. 2010;44:597–609.
6. RantisPCJr,VernavaAM3rd,DanielGL,LongoWE.Chronic constipation–isthework-upworththecost?DisColon Rectum.1997;40:280–6.
7. BrandtLJ,PratherCM,QuigleyEM,SchillerLR,SchoenfeldP, TalleyNJ.Systematicreviewonthemanagementofchronic constipationinNorthAmerica.AmJGastroenterol.2005;100 Suppl.1:S5–21.
8. CamilleriM,ThompsonWG,FleshmanJW,PembertonJH. Clinicalmanagementofintractableconstipation.AnnIntern Med.1994;121:520–8.
9. LemboA,CamilleriM.Chronicconstipation.NEnglJMed. 2003;349:1360–8.
10.MellgrenA.Diagnosisandtreatmentofconstipation.EurJ Surg.1995;161:623–34.
11.CesarMAP,KlugWA,AguidaHAC,OrtizJA,FangCB, CapelhuchinikP.Alterac¸õesdaspressõesanaisemapcientes constipadospordefecac¸ãoobstruida.RevBrasColoproct. 2008;28:402–8.
12.AgachanF,ChenT,PfeiferJ,ReissmanP,WexnerSD.A constipationscoringsystemtosimplifyevaluationand managementofconstipation.DisColonRectum.1996:681–5. 13.CormanML.Disordersofdefecation.ColonRectSurg.
1998;5:368–400.
14.GliaA,LindbergG,NilssonLH,MihocsaL,AkerlundJE. Clinicalvalueofsymptomassessmentinpatientswith constipation.DisColonRectum.1999;42:1401–8,discussion 1408–10.
15.KellerJ,LayerP.Intestinalandanorectalmotilityand functionaldisorders.BestPractResClinGastroenterol. 2009;23:407–23.
16.TernentCA,BastawrousAL,MorinNA,EllisCN,HymanNH, BuieWD.Practiceparametersfortheevaluationand managementofconstipation.DisColonRectum. 2007;50:2013–22.
17.PfeiferJ,TeohTA,SalangaVD,AgachanF,WexnerSD. Comparativestudybetweenintra-analspongeandneedle electrodeforelectromyographicevaluationofconstipated patients.DisColonRectum.1998;41:1153–7.
18.OliveiraLCC.Anorectalmanometryandtherectoanal inhibitoryreflex.Springer;2006.
19.CesarMAP,KlugWA,AguidaHAC,OrtizJA,FangCB, CapelhuchinikP.Apresenc¸adaretoceleinterferenos resultadosdeexamedefisiologiaanal?RevBrasColoproct. 2008:58–62.
20.CesarMAP,KlugWA,AguidaHAC,OrtizJA,FangCB,
CapelhuchinikP.Diagnósticodeanismusatravésdosexames defisiologiaanal.RevBrasColoproct.2009;29:192–6.
21.CesarMAP,OrtizJA,FariaFG,SalgadoFC,SalanFO,Branco GAR,etal.Reprodutibilidadedamanometriaanalem mulheressemdistúrbioevacuatórios.RevBrasColoproct. 2004;24:33–7.
22.CesarMAP,OliveiraCC.Existeimportâncianautilizac¸ãoda manometriaanorretalnodiagnósticodasíndromedo intestinoirritável?RevBrasColoproct.2009;3:8–32.
23.DrossmanDA,CheyWD,JohansonJF,FassR,ScottC,PanasR, etal.Clinicaltrial:lubiprostoneinpatientswith
constipation-associatedirritablebowelsyndrome–resultsof tworandomized,placebo-controlledstudies.Aliment PharmacolTher.2009;29:329–41.
24.PfeiferJ,OliveiraLLC.Anorectalmanometryandthe rectoanalinhibitoryreflex.Springer;2006.
25.RaoSS,PatelRS.Howusefularemanometrictestsof anorectalfunctioninthemanagementofdefecation disorders.AmJGastroenterol.1997;92:469–75.
26.VreesMD,WeissEG.Theevaluationofconstipation.Clin ColonRectalSurg.2005;18:65–75.
27.KlugWAAH,OrtizJA,FangCB,CapelhuchinikP.Rectaland analstrainingpressuresinprimigravidae.RevBrasColoproct. 2008:150–3.
28.KlugWAAH,OrtizJA,FangCB,CapelhuchinicP.Alterac¸õesdas pressõesanaisnagravidez.RevBrasColoproct.2007;27:33–7. 29.MugieSM,BenningaMA,DiLorenzoC.Epidemiologyof
constipationinchildrenandadults:asystematicreview.Best PractResClinGastroenterol.2011;25:3–18.
30.ColleteVL,AraujoC.Prevalênciaefatoresassociadosá constipac¸ãointestinal:umestudodebasepopulacionalem Pelotas,RioGrandedoSul,Brasil.CadSaúdePúbl.
2007;26:1391–402.
31.ScottSM,VandenBergMM,BenningaMA.Rectal
sensorimotordysfunctioninconstipation.BestPractResClin Gastroenterol.2011;25:103–18.