w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
For
survival,
the
emergence
of
oligoclonal
bands
after
multiple
myeloma
treatment
is
less
important
than
achieving
complete
remission
Luiza
Soares
Vieira
da
Silva
a,∗,
Edvan
de
Queiroz
Crusoe
b,
Lais
Rocha
Guimarães
de
Souza
b,
Carlos
Sérgio
Chiattone
a,
Vânia
Tietsche
de
Moraes
Hungria
aaFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
bHospitalUniversitárioProfessorEdgardSantosdaUniversidadeFederaldaBahia(HUPES/UFBA),Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20August2015
Accepted18May2017
Availableonline1July2017
Keywords:
Abnormalproteinband
Oligoclonalbands
Multiplemyeloma
Prognosis
a
b
s
t
r
a
c
t
Background:Theemergenceofoligoclonalbands,proteinsdifferingfromthoseoriginally
identifiedatdiagnosis,hasbeenreportedinmultiplemyelomapatientsafterhigh-dose
chemotherapyfollowedbyautologousstemcelltransplantationandaftersuccessful
con-ventionalchemotherapy.Theclinicalrelevanceofoligoclonalbandsremainsunclear,but
theiremergencehasbeenassociatedwithbetterprognosis.Theaimofthepresentstudywas
todeterminetheprevalence,clinicalcharacteristicsandprognosticimpactofthepresence
ofoligoclonalbandsinmultiplemyelomapatients.
Methods:Aretrospectivecohortstudywasconducted.Thestudyincludednewlydiagnosed
multiplemyelomapatientswithatleastverygoodpartialresponseafterconventionaldose
orhigh-dosechemotherapyfollowedbyautologousstemcelltransplantation.The
emer-genceofoligoclonalbandswasidentifiedusingserumproteinelectrophoresisaswellas
serumandurineimmunofixationtechniques.
Results:Atotalof101patientswereincludedwithamedianfollow-upof42months.In
total, 55%weremale, andthemedianagewas58years(29–87years).Fifty-one (50.5%)
patientsdevelopedoligoclonalbands.Theycomprised60%(45/75)ofpatientstreatedwith
autologousstemcelltransplantationand23%(6/26)ofthosewhowerenottransplanted.
Patientswitholigoclonalbandsshowedbetterprogression-freesurvivalthanthosewithout
theemergenceofoligoclonalbands(p-value=0.0075).
Conclusion: Theprevalenceofoligoclonalbandsinthisstudypopulationwas50.5%with
itsfrequencybeinggreaterincasestreatedwithautologousstemcelltransplantationand
inthoseattainingcompleteremission.Completeremissionwasmoreimportantthanthe
emergenceofoligoclonalbandsonprogression-freesurvival.
©2017PublishedbyElsevierEditoraLtda.onbehalfofAssociac¸ ˜aoBrasileirade
Hematologia,HemoterapiaeTerapiaCelular.ThisisanopenaccessarticleundertheCC
BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:HematologyandOncologyDepartment–SantaCasaMedicalSchool,R.Dr.CesárioMotaJúnior,112–Vila
Buarque,01221-020SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](L.S.Silva).
http://dx.doi.org/10.1016/j.bjhh.2017.05.010
1516-8484/©2017PublishedbyElsevierEditoraLtda.onbehalfofAssociac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.
Introduction
Multiplemyeloma(MM)isahematologicdisorderthatis
char-acterizedbytheclonalexpansionofplasmacellsinthebone
marrow.Theseplasmacellsareresponsibleforthe
produc-tionofauniquemonoclonalimmunoglobulinwithaconstant
isotypeandlightchainrestrictionthatcanbefoundinserum
and/orurineandistermedparaproteinortheMcomponent.1
Themeasurementofthismonoclonalproteinbyserum
pro-teinelectrophoresis(SPE)andimmunofixationisinvaluable
formonitoringpatientswithMM.1
Sincetheintroductionofhigh-dosemelphalanfollowedby
rescueusingautologoushematopoieticstemcell
transplan-tation(ASCT),theemergenceofoligoclonalityoroligoclonal
bands(OB)hasbeendescribedinnumerousstudies.2–9 This
isdefinedasfollows:(1)anewmonoclonalcomponent
iden-tifiedbySPE,(2)avariationoftheimmunoglobulinsubtype,
and/or(3)theemergenceofmorethanoneimmunoglobulin
subtypedetectedbyserumorurineimmunofixationthat
dif-fersfromtheinitialpatternobservedatdiagnosis.2–5 These
invariablysmallcomponentscanremainundetectedbySPE
butareidentifiedbyimmunofixationinupto66%ofcases.3
TheprevalenceofOBvaries,rangingfrom6.6%to73%.3,6
Theyarecommonlyfoundinpatientswhohaveundergone
ASCT.2,3,7,8 However,OBcanalsoemerge afterconventional
chemotherapy, particularly following the use of the novel
agents,suchasimmunomodulators(IMIDs)andproteasome
inhibitors (PI).4,5 The presence of OB has been associated
withsuperiorresponserates.2,5Whileinitiallydescribedasa
meretransientphenomenonofimmunologicrecovery,some
authorshavesuggestedthattheappearanceofthesebandsis
associatedwithimprovedprognosisandlongersurvival.2–4,9,10
TheemergenceofOBcanbemistakenasdisease
progres-sion,leadingtounwarrantedchangesintreatment.Thus,to
betterunderstandthefrequency,theclinicalcharacteristics
andtheprognosticimpactofOB,theclinicalrecordsandthe
resultsofSPEandimmunofixationtestsofMMpatientswho
hadatleastverygoodpartialresponse(VGPR)aftertreatment
wereanalyzed.Thisisthefirststudyanalyzingtheimpactof
OBinMMpatientstreatedinBrazil.
Methods
The medical records of 328 patients who were treated at
tworeferralcentersforMMintheBraziliannationalhealth
system(SantacasadeSãoPauloHospitalandUniversity
Hos-pitalof the Universidade Federal da Bahia) from July 2003
to June 2013 were reviewed. Participants had achieved at
leastVGPR,definedasserumandurineM-proteindetectable
byimmunofixation,butnotbySPE, orwho achieved≥90%
reduction in serum M-protein plus urine M-protein level
<100mg/24h after first-line therapy,11 specifically,
conven-tionaldosesofchemotherapyorhigh-dosechemotherapyand
ASCT.Atotalof101patientswereincludedforthe
identifica-tionoftheemergenceofOBusingtheSPEandimmunofixation
techniques.ThestudywasapprovedbytheResearchEthics
Committeesofbothinstitutions.
Table1–Clinicalandlaboratorycharacteristicsofthe studypopulation.
Characteristic
Ageatdiagnosis–years(n=101)
Range 29–87
Median 58
Sex–n(%)(n=101)
Male 55(54.5)
Female 46(45.5)
ECOG–n(%)(n=101)
0 34(33.7)
1 18(17.8)
2 16(15.8)
3 17(16.8)
4 2(2.0)
Notassessed 14(13.9)
DS–n(%)(n=100)
I 2(2.0)
II 6(6.0)
III 92(92.0)
ISS–n(%)(n=94)
I 33(35.1)
II 30(31.9)
III 31(33.0)
M-component–n(%)(n=101)
IgA 24(23.8)
IgG 61(60.4)
IgM 1(1.0)
Kappa(free) 7(6.9)
Lambda(free) 8(7.9)
ECOG: Eastern cooperative oncology group; DS: Durie-Salmon; ISS: International staging system; M-component: monoclonal component.
The analyzed variables were sex and age at
diagno-sis, type of immunoglobulin secreted, Eastern cooperative
oncologygroup(ECOG)performancestatus,stagingsystems
(Durie-SalmonandInternationalstagingsystem–ISS),
treat-ment (high-dose chemotherapy and ASCT or conventional
chemotherapy),responseassessmentandemergenceofOB.
TheemergenceofOBwasdefinedas(1)newmonoclonal
spikeonSPE,whichdifferedfromtheinitialpatternevidenced
bydirectcomparisonofassays,(2)immunoglobulinsubtype
switching,and/or(3)morethanoneimmunoglobulinsubtype
atserumandurineimmunofixation.
Theresponsecriteriawerebasedonthe2006International
myeloma working group.11 Overall survival was calculated
fromthestartoftreatmenttodeathorlosstofollow-upand
progression-freesurvival(PFS)wascalculatedfromthestart
oftreatmenttoprogression,deathorlosstofollow-up.
CategoricalvariableswerecomparedusingtheChi-square
orFisherexacttests,thet-testwasusedtocompareageamong
groupsandtheKaplan–Meiercurvewasemployedforsurvival
analysis,withcomparisonacrossgroupsusingthelogrank
test.Kaplan–Meieranalyseswerealsousedtoidentify
intheCoxregressionmodelthatalsohadthetreatmentgroup
asacovariate.Statisticalanalyseswereperformedusing
Med-Calcsoftware(Mariakerke,Belgium,v11.3.3.0).
Results
Atotalof101multiplemyelomapatientswithVGPRorbetter
responsesafterconventionalorhigh-dosechemotherapyas
thefirstlineoftreatmentwereincluded.Themedian
follow-upwas42months(range:7.63–131.4months).Fifty-five(54.5%)
patientsweremaleand46(45.5%)werefemale.Themedian
ageatdiagnosiswas58(range:29–87)years.Theclinical
char-acteristicsofthestudypopulationaregiveninTable1.
Seventy-fivepatientswereconsideredeligibleforASCT.For
inductiontherapy, the cyclophosphamide,thalidomideand
dexamethasoneregimen(CTD),usedin52%ofpatients,was
themostcommontreatment.Thiswasfollowedby
thalido-mideand dexamethasone(TD)in21.3%ofpatientsand by
vincristine,doxorubicinanddexamethasone(VAD)in17.3%
ofpatients.Thepatientswhowereconsideredineligiblefor
ASCT(n=26)weremainlytreatedwithCTD(38.5%),
melpha-lanand prednisone (23%), and melphalan,prednisone and
thalidomide(MPT)(15.4%).
OBemerged in51(50.5%)patients, ofwhich 54.9%were
femaleand45.1%weremale.Despiteaslightpredominance
offemales,there was no statisticallysignificant difference
betweenthegroups.Themedianageofthesepatientswas58
(range:52–63)years.Fromthe51casesinwhichOBemerged,
45cases(88.2%)wereASCTpatients,andsix(11.8%)were
inel-igiblecases.AnanalysisoftheprevalenceofOBbytreatment
typerevealedthat60%ofASCTpatientspresentedOBversus
only23%oftransplant-ineligiblepatients.Achievingcomplete
response(CR)wasassociatedwithagreaterlikelihoodofthe
emergenceofOB,andspecifically,62.7%ofCRpatients
devel-oped OB (p-value=0.03). Table 2 shows the comparison of
patientswithandwithouttheemergenceofOB.
OBweredetectablebyserumorurineimmunofixation,but
notbySPE,in64%ofcases.Themostfrequentfindingwasthe
combinationofmorethanoneimmunoglobulinsubtype(IgG,
kappaandLambda),whichwasidentifiedin21cases.
Themedian PFSfor the entiregroup was 38.4 months.
ThemedianPFSwere45.4and34.7monthsforpatientswith
andwithouttheemergenceofOB,respectively[Hazardratio
(HR)=0.5249; 95% confidenceinterval (CI): 0.3194–0.8625; p
-value=0.0075;Figure1].
Themedianoverallsurvivalfortheentiregroupwas89.9
months.PatientswithouttheemergenceofOBhadamedian
overallsurvivalof80.7monthsversus89.9monthsforpatients
withtheemergenceofOB(HR:0.5291;95%CI:0.2293–1.2212;
p-value=0.1431).
PatientswithISS1andtheemergenceofOBhadamedian
PFSof45.1months,whilethose without theemergence of
OBhad a median PFSof28.3 months(HR: 0.3720; 95% CI:
0.1505–0.9192;p-value=0.0120;Figure2).
Themediansurvivalrateofpatientswho receivedASCT
andhadtheemergenceofOBwas49.6months,andforthose
withouttheemergenceofOBthemediansurvivalratewas32.8
months(HR: 0.4552;95% CI:0.2345–0.8835; p-value=0.0063;
Figure3).
ThePFSwasevaluatedinmultivariateanalysis(Coxmodel)
usingISS(1vs.2/3),responserate(CRvs.VGPR),typeof
treat-ment(transplantvs.notransplant)andemergenceofOB(yes
vs.no)asindependentvariables.Intheanalysisofthemodel
thatincluded (OB,ResponseRateandISS)onlyOB,andCR
wereindependentpredictorsforbetterPFS.Asecondmodel
wasrunusinghigh-dosechemotherapyasafourthvariable,
inadditiontothosedescribedbefore.Inthissecondmodel,
theemergenceofOBlostitsprognosticsignificance,andthe
onlyvariablesignificantlyassociatedwithincreasedPFSwas
CR.
Discussion
Here,wereportthefirstBrazilianstudyinvolvingthe
emer-genceofOBinMMpatientsafterconventionalchemotherapy
orhigh-dosechemotherapyfollowedbyASCT.Aprevalence
of50.5% ofOBemergedinMM patientswithVGPR or
bet-ter,andtheemergenceofOBwasmorecommoninpatients
who underwenttransplantationandinthosewhoachieved
CR.Previousstudiesreportedaprevalenceoftheemergence
ofOBintransplantedpatients, rangingfrom 5.9%to24.5%
andlikewise,thisstudyfoundthattheratesoftheemergence
ofOBwerehigherintransplantedpatients.3,7,8,12Theuseof
novelagentsinbothtransplantandnon-transplantsettings
wasalsoassociatedwithahighprevalenceofOB.4,5,13
Theimpactonoverallsurvivalcouldnotbeproven,
pos-sibly due to the relatively small sample size. Studies with
largersamplesizeshaveshownlongeroverallsurvivalamong
individuals presenting the emergence of OB.2,3,8,13 In one
study involving1942patients,Wadheraet al.3 found
signif-icantlygreateroverallsurvivalamongthosewhodeveloped
secondarymonoclonalgammopathyofundetermined
signif-icance (sMGUS) compared tothose who didnot (73 vs. 38
months,respectively).
In this study, PFS was superior in patients who
devel-opedOB,afindingthathasbeenreportedinpreviousstudies
assessing transplanted patients only2,9,10,13 and in studies
involvingpatientswhohadundergoneASCTornot.7,12
Itiswellestablishedintheliteraturethatbetterresponse
predictssuperiorsurvival.14–16Thisstudyselectedthe
emer-genceofOBamongpatientswithbetterresponses(atleast
VGPR)andeveninthisspecificgroupofpatients,the
emer-genceofOBhadafavorableimpactonPFS.AnalyzingPFSin
aCoxregressionmodelincludingISS(1vs.2/3)andresponse
rate(CRvs.VGPR)aswellastheemergenceofOB,thelatter
remainedanindependentvariabletopredictPFS.However,on
addingthetypeoftreatmentperformed(ASCTvs.noASCT)
to themodel, onlyCR was significant eventhoughthe OB
wasclosetothesignificancelimit(p-value=0.07).Thesizeof
cohortcouldhaveinfluencedthisresult.
Fujisawaetal.failedtoconfirmimprovementinsurvival
assessingtheimpactofOBonsubgroupswithatleastVGPR
orCRinpatientssubmittedtoASCTorotherwise,and
simi-larly,noimpactwasfoundforthesubgroupofpatientseligible
for ASCT. Theauthors questionedthe potential prognostic
factor of oligoclonality, specifically, that it might be more
closelylinkedtobetterresponsesthantotheemergenceof
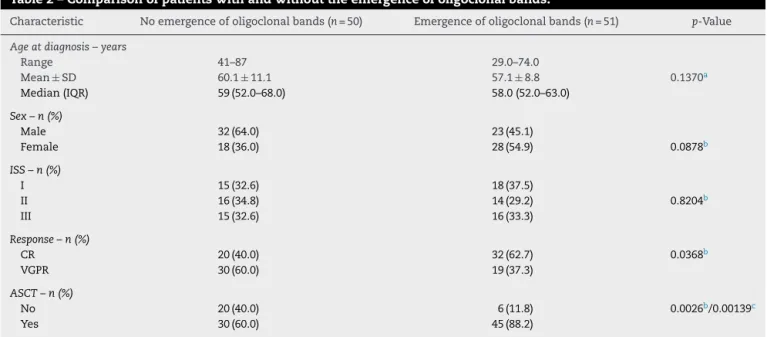
Table2–Comparisonofpatientswithandwithouttheemergenceofoligoclonalbands.
Characteristic Noemergenceofoligoclonalbands(n=50) Emergenceofoligoclonalbands(n=51) p-Value
Ageatdiagnosis–years
Range 41–87 29.0–74.0
Mean±SD 60.1±11.1 57.1±8.8 0.1370a
Median(IQR) 59(52.0–68.0) 58.0(52.0–63.0)
Sex–n(%)
Male 32(64.0) 23(45.1)
Female 18(36.0) 28(54.9) 0.0878b
ISS–n(%)
I 15(32.6) 18(37.5)
II 16(34.8) 14(29.2) 0.8204b
III 15(32.6) 16(33.3)
Response–n(%)
CR 20(40.0) 32(62.7) 0.0368b
VGPR 30(60.0) 19(37.3)
ASCT–n(%)
No 20(40.0) 6(11.8) 0.0026b/0.00139c
Yes 30(60.0) 45(88.2)
SD:standarddeviation;IQR:interquartilerange;ISS:Internationalstagingsystem;CR:completeresponse;VGPR:verygoodpartialresponse; ASCT:autologoushematopoieticstemcelltransplantation.
a t-Testforindependentsamples.
b Chi-squaretest.
c Fisher’sexacttest.
Progression free survival
0 20 40 60 80 100 120
0 20 40 60 80 100
Time (months)
Survival probability (%)
Number at risk Group: No
50 37 11 4 1 1 0
Group: Yes
51 42 20 9 3 0 0
OB No Yes
Figure1–Progression-freesurvivalaccordingtotheemergenceofoligoclonalbands(OB)orotherwise.(p=0.0075).
Theseconflictingresults,bothintermsofprevalenceand
impact on survival, are probably attributed to the
hetero-geneityofthestudiespublishedtodate.Moststudieshada
retrospectivedesign,differentpopulationsizes,different
def-initionsofOB,frequencyofSPEandimmunofixationtests,and
useddifferenttreatments.
Thedetection ofthesenewmonoclonalpeaksinSPEor
byimmunofixationduringthefollow-upofMMpatientscan
bemistakenforrelapse and/ordisease progression,leading
tounwarrantedtreatmentorchangesintreatment.Assuch,
thefindingofoligoclonality,asmallmonoclonalcomponent
differentfromthatidentifiedatdiagnosis,mustbecarefully
interpreted and regular follow-ups should be carried out
beforetreatmentdecisionsaremade.
The advances in the MM treatment have led to
bet-ter responses. The incidence of the emergence of OB has
increasedanditsimpactonsurvivalshouldbeconfirmedin
Progression free survival (ISS=1)
0 10 20 30 40 50 60 70 80 90
0 20 40 60 80 100
Time (months)
Survival probability (%)
Number at risk Group: No
15 9 5 2 0 0 0
Group: Yes 18 15
18 14 11 4
2
5 3
9 3 1 0
OB No Yes
Figure2–Progression-freesurvivalaccordingtotheemergenceofoligoclonalbands(OB)inISS1patients(p=0.0120).
Time (months)
Survival probability (%)
100
90
80
70
60
50
40
30
20
10
0
0 20 40 60 80 100
Number at risk Group: No
Group: Yes30 45
22
38
5
19
2
9
0
3
0
0
Progression free survival (ASCT)
OB No Yes
Figure3–Progression-freesurvivalaccordingtotheemergenceofoligoclonalbands(OB)inASCTpatients(p=0.0063).
Conclusion
AhighprevalenceoftheemergenceofOBwasseeninpatients
whohadatleastVGPRafterconventionalorhigh-dose
ther-apy.Thisfrequencywasgreaterinpatientswhounderwent
ASCTandinthosewithCR.CRwasmoreimportantthanthe
emergenceofOBonthePFS.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KyleRA,RajkumarSV.Criteriafordiagnosis,staging,risk stratificationandresponseassessmentofmultiplemyeloma. Leukemia.2009;23(1):3–9.
2.ZentCS,WilsonCS,TricotG,JagannathS,SiegelD,Desikan KR,etal.OligoclonalproteinbandsandIgisotypeswitching inmultiplemyelomatreatedwithhigh-dosetherapyand hematopoieticcelltransplantation.Blood.1998;91(9):3518–23. 3.WadheraRK,KyleRA,LarsonDR,DispenzieriA,KumarS,
significanceinpatientswithmultiplemyeloma.Blood. 2011;118(11):2985–7.
4. FernándezdeLarreaC,TovarN,CibeiraMT,ArósteguiJI, Rosi ˜nolL,ElenaM,etal.Emergenceofoligoclonalbandsin patientswithmultiplemyelomaincompleteremissionafter inductionchemotherapy:associationwiththeuseofnovel agents.Haematologica.2011;96(1):171–3.
5. MarkT,JayabalanD,ColemanM,PearseRN,WangYL,LentR, etal.Atypicalserumimmunofixationpatternsfrequently emergeinimmunomodulatorytherapyandareassociated withahighdegreeofresponseinmultiplemyeloma.BrJ Hematol.2008;143(5):654–60.
6. HovengaS,deWolfJT,GuikemaJE,KlipH,SmitJW,Smit SibingaCT,etal.Autologousstemcelltransplantationin multiplemyelomaafterVADandEDAPcourses:ahigh incidenceofoligoclonalserumIgsposttransplantation.Bone MarrowTransplant.2000;25(7):723–8.
7. FujisawaM,SeikeK,FukumotoK,SueharaY,FukayaM, SugiharaH,etal.oligoclonalbandsinpatientswithmultiple myeloma:itsemergencepersecouldnotbetranslatedto improvedsurvival.CancerSci.2014;105(11):1442–6. 8. JoJC,YoonDH,KimS,LeeK,KangEH,JangS,etal.Clinical
significanceoftheappearanceofabnormalproteinbandin patientswithmultiplemyeloma.AnnHematol.
2014;93(3):463–9.
9. LiuAJ,ZongH,YangGZ,ZhaiYH,LiLH.Significanceof oligoclonalbandsafterstemcelltransplantationinmultiple myelomacases.AsianPacJCancerPrev.2012;13(4):1483–6. 10.Jimenez-ZepedaVH,ReeceDE,TrudelS,FrankeN,WinterA,
ChenC,etal.Oligoclonalandmonoclonalbandsaftersingle
autologousstemcelltransplantinpatientswithmultiple myeloma:impactonoverallsurvivalandprogression-free survival.LeukLymphoma.2014;55(10):2284–9.
11.DurieBG,HarousseauJL,MiguelJS,BladéJ,BarlogieB, AndersonK,etal.InternationalUniformresponsecriteriafor multiplemyeloma.Leukemia.2006;20(9):1467–73.
12.ZouD,AnG,ZhuG,WangJ,ShiL,MengH,etal.Secondary monoclonalgammopathyofundeterminedsignificanceis frequentlyassociatedwithhighresponserateandsuperior survivalinpatientswithplasmacelldyscrasias.BiolBlood MarrowTransplant.2014;20(3):319–25.
13.TovarN,deLarreaCF,ArósteguiJI,CibeiraMT,Rosi ˜nolL, RoviraM,etal.Naturalhistoryandprognosticimpactof oligoclonalhumoralresponseinpatientswithmultiple myelomaafterautologousstemcelltransplantation: long-termresultsfromasingleinstitution.Haematologica. 2013;98(7):1142–6.
14.AlexanianR,WeberD,GiraltS,DimopoulosM,DelasalleK, SmithT,etal.Impactofcompleteremissionwithintensive therapyinpatientswithresponsivemultiplemyeloma.Bone MarrowTransplant.2001;27(10):1037–43.
15.Martinez-LopezJ,BladeJ,MateosMV,GrandeC,AlegreA, García-Lara ˜naJ,etal.Long-termprognosticsignificanceof responseinmultiplemyelomaafterstemcell
transplantation.Blood.2011;118(3):529–34.