H VM BI OFLUX
H u m a n & V e t e r in a r y M e dicin e
I n t e r n a t ion a l Jou r n a l of t h e Bioflu x Socie t y
Pa ce a n d sot a lol – t h re e ca se r e por t s of t he
be ne fit s a nd pot e n t ia l h a za rds a ssocia t e d w it h
sot a lol a d m in ist r a t ion in sinu s n ode dysfu nct ion
1
Ştefan H. Roşianu
,
2Anca D. Buzoianu,
3Adela Roşianu
, and
1Radu
Căpâlnean
u
1
Depart m ent of Cardiology, Heart I nst it ut e “ Niculae St ancioiu” , “ I uliu Haţieganu” Univ ersit y of Medicine and Pharm acy , Cluj –Napoca, Cluj , Rom ânia; 2Depart m ent of Pharm acology and Toxicology , „Iuliu Haţieganu” University of Medicine and Pharmacy,
Cluj - Napoca, Cluj , Rom ânia; 3Heart I nst it ut e “ Niculae St ancioiu” , Cluj - Napoca, Cluj , Rom ânia. Corresponding author: Ş. H. Roşianu,dr.rosianu@gm ail.com
Abst r a ct. The sinus node dysfunct ion is associat ed wit h conduct ion syst em disease and supr avent r icular t achyar r hyt hm ias ( at r ial fibr illat ion and at r ial flut t er ) . The only effect ive t r eat m ent for pat ient s wit h chr onic sym pt om at ic sinus node dysfunct ion is pacem aker t her apy. I n t achy- br ady syndr om e pat ient s, in addit ion t o pacem aker t her apy, t he phar m acological t r eat m ent is necessar y t o avoid t achycar dia episodes. Because of t he fr equent par oxysm al at r ial fibr illat ion episodes a good choice t o m aint ain t he sinus r hyt hm is r epr esent ed by sot alol. This ar t icle will pr esent t hr ee pat ient s t hat pr ovide exam ples of beneficial effect s of sot alol and also on t he r isk of sever e adver se event s in som e cases.
Ke y w or ds: sinus node dysfunct ion, at r ial fibr illat ion, sot alol, pacem aker t her apy.
I n t r odu ct ion. The sinus node dy sfunct ion ( SND) or sick sinus sy ndrom e refers t o
abnorm alit ies in sinus node im pulse form at ion and propagat ion, and includes sinus brady cardia, sinus pause or arrest , chronot ropic incom pet ence, and sinoat rial exit block. SND is associat ed wit h conduct ion sy st em disease and suprav ent ricular t achy arrhy t hm ias ( at rial fibrillat ion and at rial flut t er) , nam ed “ t achy-brady sy ndrom e”( Epst ein et al 2008) .
SND is m ore prev alent in elderly pat ient s relat ed t o senescence of sinus node, oft en accom panied wit h senescence of t he at rium and conduct ion sy st em ( Dobrzy nski et al 2007) .
At rial fibrillat ion ( AF) is t he m ost com m on serious arrhy t hm ia wit h a prev alence est im at ed at 2.2 m illion people in t he Unit ed St at es and 4.5 m illion in t he European Union ( Chugh et al 2001; Fust er et al 2006) . I t s incidence also increases progressiv ely w it h age ( Tse et al 2005) . AF is associat ed wit h heart failure, hem ody nam ic im pairm ent and sy m pt om s affect ing qualit y of life. Pat ient s hav e an increased risk of art erial t hrom boem bolic ev ent s, including st rok e, result ing in significant m orbidit y, m ort alit y and cost s ( Glot zer et al 2003; Flak er et al 2005) .
The only effect iv e t reat m ent for pat ient s wit h chronic sy m pt om at ic SND is pacem ak er t herapy . Many st udies indicat e t hat right at rial pacing decreases t he incidence of AF, w hen com pared w it h pacing of t he v ent ricle, and it represent s t he opt im al pacing m ode ( Rosenqv ist et al 1986; Andersen et al 1997; Lam as et al 2002) .
All ant iarrhy t hm ic drugs hav e pot ent ial proarrhyt hm ic effect s; t hese m ay range from sim ple sinus bradycardia t o fat al v ent ricular arrhy t hm ias especially in elderly pat ient s wit h ischem ic cardiac disease ( Podrid 2001) .
This art icle will focus on t he beneficial effect s of sot alol and also on t he risk of sev ere adv erse ev ent s in som e pat ient s.
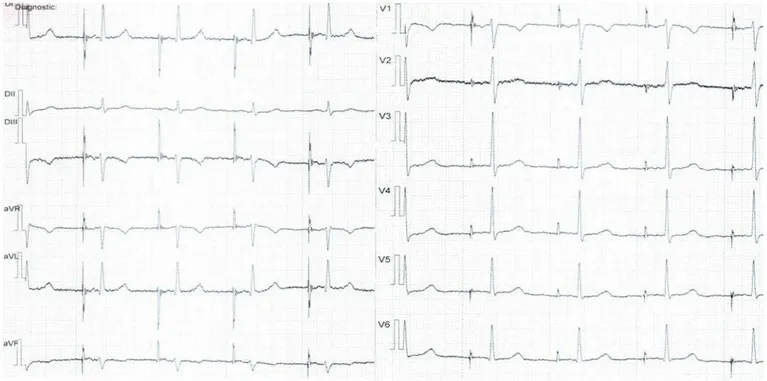
Ca se r e por t 1. The first case is a 62 y ear old fem ale pat ient diagnosed wit h sick sinus
sy ndrom e, sinus brady cardia ( 40 bpm ) and par ox y sm al AF, in w hich an AAI pacem ak er w as im plant ed and program m ed at 60 bpm . She receiv ed Sot alol 80 m g t wice daily in order t o prev ent AF. Aft er four y ears of t reat m ent t he AV node conduct ion is in t he norm al range and she is free of sy m pt om s, t he QTc int erv al w as 440 m sec ( Figure 1) .
Figure 1. M. A., 66 y ears old; EKG - AAI paced rhy t hm , 60 bpm , QTc= 440 m sec.
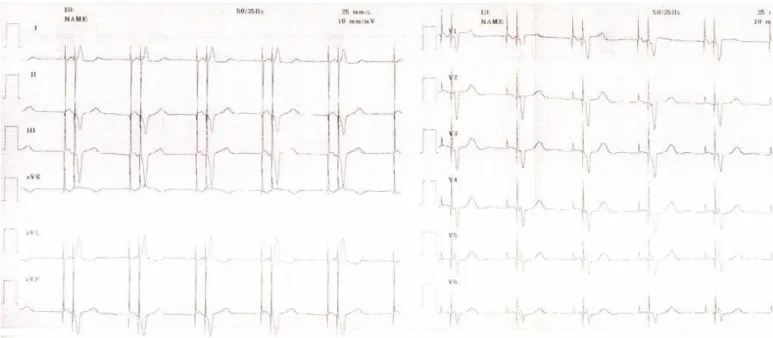
Ca se r e por t 2. The second case is a 71 y ears old m an diagnosed wit h sick sinus
Figure 2. A. I ., 73 y ears old; EKG - DDD paced rhy t hm , 60 bpm , QTc= 475m sec.
Ca se re por t 3 . The t hird case is sim ilar t o t he second one. This t im e it is a fem ale
pat ient, 60- y ear old, wit h a hist ory of sinus node dy sfunct ion, parox ysm al AF and at rial flut t er w hich w as regarded as inadequat ely cont rolled by ant iarrhy t hm ic drug t herapy. A com plex procedure of AF ablat ion by pulm onary v eins isolat ion and cavot ricuspidian ist hm us ablat ion w as perform ed in Decem ber 2007 in a cardiology hospit al in France. She also present ed a st rong fam ily hist ory of sinus node disease ( her m ot her and her older sist er bot h receiv ed a pacem ak er for sick sinus sy ndrom e) . Ov er t he nex t few m ont hs, she ex perienced recurrent dizzy spells, w hich becam e increasingly sev ere. She w as adm it t ed in our hospit al in Nov em ber 2008. The EKG rev ealed sev ere sinus brady cardia wit h a heart rat e of 38- 40 bpm and sinus pauses of m ore t han 3 seconds ( Figure 3) .
Figure 3. C. V., 58 y ears old; EKG - sinus rhy t hm , sinus pause of 3 sec.
y ear lat er she present ed frequent episodes of rapid palpit at ions. The Holt er m onit or show ed episodes of poly m orphic nonsust ained v ent ricular t achy cardia ( Figure 4) associat ed wit h sot alol adm inist rat ion, w hich w as discont inued and she w as st art ed on propranolol. The QTc int erv al w as sev erely prolonged 540 m sec. Unt il t he lat est cont rol in Decem ber 2010 she didn’t ex perienced new recurrent episodes of rapid palpit at ions.
Figure 4. C. V., 59 y ears old; t elem et ry m onit oring show ing poly m orphic nonsust ained v ent ricular t achy cardia.
D iscussion. These t hree cases prov ide ex am ples of t he benefit s and pot ent ial hazards
associat ed wit h t he sot alol adm inist rat ion.
I n pat ient s w it h SND and norm al at riovent ricular ( AV) conduct ion, phy siological pacing can be accom plished wit h eit her a single cham ber at rial pacem ak er AAI / R or a dual cham ber pacem ak er DDD/ R. For dual cham ber dev ices hav e been dev eloped new algorit hm s in order t o m inim ize v ent ricular st im ulat ion. How ev er, a single- cham ber at rial pacem ak er in AAI m ode is an accept able t herapy in pat ient s wit h SND and norm al AV conduct ion as t he ov erall incidence of com plet e heart block is very low . I n pat ient s wit h SND and k now n AV conduct ion abnorm alit y ( including bundle branch block and bifascicular block ) , a DDD pacem ak er should be used because of t he high risk of AV block ( Brandt et al 1992) . I n t he first case present ed, t he AAI pacing w as enough because t he AV int erv al ( conduct ion) rem ained const ant during t he five years of follow- up. The ot her t w o cases needed DDD pacem ak ers due t o adv anced age ( Case 2) and t o first degree AV block ( Case 3) .
The AF recov ery t o sinus rhy t hm will result in hem ody nam ic im prov em ent s by rest orat ion of at rial sy st ole and im provem ent of v ent ricular filling at rest and during ex ercise ( Ueshim a et al 1993; Yigit et al 2003; Singh et al 2005, 2006) . I n pat ient s wit h SND low heart rat es will facilit at e at rial ect opies, w hich if are v ery early can induce parox y sm al AF (Wallm ann et al 2003) . For t his reason rapid at rial pacing significant ly decreases t he rat e of AF recurrence ( Flam m ang et al 2005) . Also, t here are ret rospect iv e st udies indicat ing t hat right at rial pacing decreases t he incidence of AF com pared wit h pacing in t he v ent ricle ( Rosenqvist et al 1996) . Andersen et al ( 1997) dem onst rat ed significant benefit for single cham ber right at rial pacing vs. single cham ber right v ent ricular pacing in pat ient s wit h sick sinus sy ndrom e, wit h a decreased incidence of AF, t hrom boem bolic ev ent s, congest iv e heart failure and im prov ed surviv al, especially aft er long- t erm follow - up.
Sot alol, by his high degree of bet a- adrenorecept or blocking effect ( sy nergist ic wit h at rial pacing) , reduces t he at rial ect opies and m aint ains t he sinus rhy t hm ( Plew an et al 2001) . But t his ß- adrenergic blocking act ivit y t hrough t he sinus brady cardia m ay represent a m aj or lim it at ion concerning t he use of sot alol in pat ient s wit h SND or AV block unprot ect ed by a back up pacem ak er. Cont rary t o t his sit uat ion, in pat ient s w it h pacem ak er, sot alol can be used for it s class I I I effect s in order t o prev ent t he AF recurrence. I n our pat ient s t he double st rat egy “pace and sot alol” m anaged t o m aint ain free of suprav ent ricular arrhy t hm ias ( especially AF) along t he follow- up period.
sy m pt om at ic paroxy sm al AF wit h a low but definit e risk of sev ere side- effect s ( Pat t en et al 2004) .
Pure class I I I ant iarrhy t hm ic agent s are charact erized by t heir act ion pot ent ial durat ion–prolonging effect ast he sole elect rophy siological m echanism . Besides t his effect t he sot alol and am iodarone possess also addit ional elect rophy siologicaleffect s ( Hohnloser et al 1994; Singh 1994) .
All ant iarrhy t hm ic drugs hav e pot ent ial proarrhyt hm ic effect s w hich m ay range from sim ple sinus brady cardia t o fat al v ent ricular arrhy t hm ias ( especially in pat ient s wit h significant st ruct ural heart disease) and m ight ex ceed t he benefit of t he drug ( Wellens et al 1992) . Class I a dr ugs and class I I I ant iarrhy t hm ic drugs induce early aft er-depolarizat ions and det erm ine poly m orphic v ent ricular t achy cardia ( Borggrefe et al 1992) .
The QT int erv al is prolonged by a v ariet y of drugs. The class I I I ant iarrhy t hm ics are t he m aj or ex am ples and ex ert t heir t herapeut ic effect by affect ing pot assium ion channels, reducing out w ard, repolarizing current and prolonging act ion pot ent ial durat ion and t he QT int erv al respect iv ely . These drugs are used for conv ersion and m aint enance of sinus rhy t hm in pat ient s wit h recurrent AF and t hey m ay induce a pot ent ially fat al arrhy t hm ia - t orsade de point es ( TDP) ( Jack m an et al 1998) . The incidence of t his form of proarrhy t hm ia is ranging bet w een 1.8 – 4.8% for d,l- sot alol ( Lehm ann et al 1996; Hav erk am p et al 1997) . Thed- sot alol m ay be less lik ely t o prov ok e TDP com paredwit h
d, l- sot alol because of t he lack of drug- associat ed brady cardia ( Touboul 1993) . How ev er t he ex act incidence of TDP induced by d- sot alol is not y et est ablished. The lik elihood of occurrence increases wit h t he use of higher doses ( Hohnloser et al 1992; McNeil et al 1993) . I n sev eral st udies, t he aut hors dem onst rat ed t hat sot alol w as m ore effect iv e t han placebo in m aint aining sinus rhy t hm and TDP did not dev elop if drug doses w ere adj ust ed t o renal funct ion and t he QT int erv al w as m onit ored ( Brachm ann et al 1993; Bendit t et al 1999) . The reduct ion of out w ard current s and t he enhancem ent of inw ard current s during phase 2 and 3 of t he act ion pot ent ial det erm ine it s prolongat ion in t he v ent ricular m y ocy t es, w hich in t urn prolongs t he QT int erv al on t he EKG. The v ent ricular repolarizat ion is det erm ined by t he int rinsic t ransm ural het erogeneit y in t he densit y of t he v arious ion channels. The reduct ion of out w ard current and t he increase in inw ard current facilit at es t he dev elopm ent of early aft erdepolarizat ions due t o react iv at ion of t he L- t y pe calcium current and t o act iv at ion of t he sodium - calcium exchange current during t he act ion pot ent ial plat eau ( Burashnik ov et al 1998; Visw anat han et al 1999) . A m ark ed increase in dispersion of repolarizat ion increases t he lik elihood t hat early aft erdepolarizat ion-induced ex t rasyst oles will t rigger reent ry and TDP ( Verduy n et al 1997; Ant zelevit ch et al 1999) .
Pat ient s w ho dev elop drug-induced long QT sy ndrom e m ay hav e subt le genet ic defect s w hich m ak e t hem m ore suscept ible t o arrhy t hm ias w hen drugs t hat can cause prolonged QT int erv als are adm inist rat ed. The acquired abnorm al QT prolongat ion m ay be due t o a reduced repolarizat ion reserv e and t he TDP’s occurrence secondary t o a repolarizat ion prolonging drug represent s a pat ient - specific response ( pat ient s w ho dev elop new episodes of TDP aft er ex posure t o anot her repolarizat ion prolonging drug different from t he init ial one w ho caused t he arrhy t hm ia) ( Hav erk am p et al 2000) . This response specific t o each pat ient does not necessarily im ply an abnorm al QT prolongat ion and TDP ev ery t im e w hen he/ she is ex posed t o a repolarizat ion prolonging st im ulus and t he int erv als bet w een t he init iat ion of t he t herapy and t he occurrence of arr hy t hm ia are highly v ariable. St udies of congenit ally long QT sy ndrom es ( LQTS) dem onst rat ed a genet ic het erogeneit y w hich im plies m ult iple genes ( Keat ing et al 2001) . These genet ic st udies hav e ident ified fam ilies wit h v ery low penet rance ( individuals wit h genet ic m ut at ions but wit hout clinical phenot y pe) and suggest ed t hat such individuals m ay be at increased risk for TDP during t he adm inist rat ion of QT- prolonging drugs ( Donger et al 1997; Priori et al 1999; Napolit ano et al 2000; Sest i et al 2000; Yang et al 2002) . Furt herm ore t he HERG gene w as ident ified not only in LQTS disease but also as t he predom inant t arget of m ost drugs inducingTDP ( Sanguinet t i et al 1995) .
w it h frequent poly m orphic v ent ricular t achy cardia considered a m aj or com plicat ion of t he sot alol t herapy . Aft er sot alol discont inuat ion she w as free of v ent ricular arrhy t hm ias. Furt herm ore, her paced QRS com plex w as v ery large ( 200 m sec) v s. her nat iv e QRS ( 100 m sec) t hat can be ex plained by o possible cardiom y opat hy or by depolarizat ion t roubles in t he left v ent ricular m ass. Also t he fam ily burden of SND m ay suggest a genet ic predisposit ion or a possible channelopat hy.
I n conclusion, t he “ pace and sot alol” st rat egy is a good t herapeut ic alt ernat iv e in pat ient s wit h SND in order t o m aint ain t he sinus rhy t hm . Nev ert heless, alt hough t he sot alol is generally w ell t olerat edby t he m aj orit y of pat ient s, t he need for individualized careful dose t it rat ion and t he QT int erv al m onit oring, part icularly in pat ient s wit h st ruct ural heart disease, is required by t he observ at ion of drug- associat ed serious arrhy t hm ic adverse ev ent s.
Re fe r en ce s
Andersen H. R., Nielsen J. C., Thom sen P. E., Thuesen L., Mort ensen P. T., Vest erlund T., et al, 1997 Long- t erm follow - up of pat ient sfrom a random ised t rial of at rial v ersus v ent ricular pacing for sick- sinus sy ndrom e. Lancet 3 5 0: 1210–1216.
Ant zelevit ch C., Shim izu W., Yan G. X., Sicouri S., Weissenburger J., Nest erenk o V. V., et al, 1999 The M cell: I t s cont ribut ion t o t he ECG and t o norm al and abnorm al elect rical funct ion of t he heart . J Cardiov asc Elect rophy siol 1 0: 1124–52.
Bendit t D. G., William s J. H., Jin J., Deering T. F., Zuck er R., Brow ne K., et al, 1999 Maint enance of sinus rhy t hm w it h oral d,l- sot alol t herapy in pat ient s wit h sy m pt om at ic at rial fibrillat ion and/ or at rial flut t er. Am J Cardiol 8 4: 270- 7.
Borggrefe M., Haverk am p W., Shenasa M., Hindrick s G., Breit hardt G., 1992 How t o ev aluat e class I I I ant iarrhy t hm ic drug efficacy clinically : t he benefit s and short com ings of t he inv asiv e approach. J Cardiov asc Pharm acol 2 0( suppl 1) : 32- 40. Brachm ann J., Schöls W., Beyer T., Mont ero M., Enders B., Kübler W., 1993 Acut e and
chronic ant iarrhy t hm ic effect s of d- sot alol in pat ient s wit h sust ained v ent ricular t achy arrhy t hm ias. Eur Heart J 1 4( suppl I I ) : 85- 87.
Brandt J., Anderson H., Fåhraeus T., Schüller H., 1992 Nat ural hist ory of sinus node disease t reat ed wit h at rial pacing in 213 pat ient s: im plicat ions for select ion of st im ulat ion m ode. J Am Coll Cardiol 2 0( 3) : 633- 639.
Burashnik ov A., Ant zelevit ch C., 1998 Accelerat ion- induced act ion pot ent ial prolongat ion and early aft erdepolarizat ions. J Cardiov asc Elect rophy siol 9: 934–948.
Chugh S. S., Black shear J. L., Shen W. K., Ham m ill S. C., Gersh B. J., 2001 Epidem iology and nat ural hist ory of at rial fibrillat ion: clinical im plicat ions. J Am Coll Cardiol
3 7: 371–378.
Dobrzy nsk i H., Boy et t M. R., Anderson R. H., 2007 New insight s int o pacem ak er act ivit y : prom ot ing underst anding of sick sinus y ndrom e. Circulat ion 1 1 5( 14) : 1921- 1932. Donger C., Denj oy I ., Bert het M., Ney roud N., Cruaud C., Bennaceur M., et al. 1997
KVLQT1 C- t erm inal m issense m ut at ion causes a form e frust e. Circulat ion 9 6: 2778– 2781.
Epst ein A. E., DiMarco J. P., Ellenbogen K. A., Est es N. A. 3rd, Freedm an R. A., Get t es L. S., et al, 2008 ACC/ AHA/ HRS 2008 Guidelines for Device- Based Therapy of Cardiac Rhy t hm Abnorm alit ies: a report of t he Am erican College of Cardiology / Am erican Heart Associat ion Task Force on Pract ice Guidelines ( Writ ing Com m it t ee t o Revise t he ACC/ AHA/ NASPE 2002 Guideline Updat e for I m plant at ion of Cardiac Pacem ak ers and Ant iarrhy t hm ia Devices) dev eloped in collaborat ion wit h t he Am erican Associat ion for Thoracic Surgery and Societ y of Thoracic Surgeons. J Am Coll Cardiol 5 1( 21) : e1- 62.
Flaker G. C., Belew K., Beck m an K., Vidaillet H., Kron J., Safford R., et al, 2005 Asy m pt om at ic at rial fibrillat ion: dem ographic feat ures and prognost ic inform at ion from t he At rial Fibrillat ion Follow- up I nv est igat ion of Rhy t hm Managem ent ( AFFI RM) st udy . Am Heart J 1 4 9: 657–663.
recurrence assessed by reliable elect rogram s: t he prefib pilot st udy . Europace
7: 482–489.
Fust er V., Ry den L. E., Cannom D. S., et al, 2006 ACC/ AHA/ ESC 2006 Guidelines for t he Managem ent of Pat ient s wit h At rial Fibrillat ion: a report of t he Am erican College of Cardiology / Am erican Heart Associat ion Task Force on Pract ice Guidelines and t he European Societ y of Cardiology Com m it t ee for Pract ice Guidelines (Writ ing Com m it t ee t o Revise t he 2001 Guidelines for t he Managem ent of Pat ient s Wit h At rial Fibrillat ion) : dev eloped in collaborat ion wit h t he European Heart Rhy t hm Associat ion and t he Heart Rhy t hm Societ y . Circulat ion 1 1 4: 257–354.
Glot zer T. V., Hellk am p A. S., Zim m erm an J., Sw eeney M. O., Yee R., Marinchak R., et al, 2003 At rial high rat e episodes det ect ed by pacem ak er diagnost ics predict deat h and st rok e: report of t he At rial Diagnost ics Ancillary St udy of t he MOde Select ion Trial ( MOST) . Circulat ion 1 0 7: 1614–1619.
Hav erk am p W., Breit hardt G., Cam m A. J., Janse M. J., Rosen M. R., Ant zelevit ch C., et al, 2000 The pot ent ial for QT prolongat ion and pro- arrhy t hm ia by non- ant i-arrhy t hm ic drugs: clinical and regulat ory im plicat ions: report on a policy conference of t he European Societ y of Cardiology. Cardiov asc Res 4 7: 219–233.
Hav erk am p W., Mart inez R. A., Hief C., Lam m ers A., Mühlenk am p S., Wicht er T., et al, 1997 Efficacy and safet y of d,l- sot alol in pat ient s w it h v ent ricular t achy cardia and in surv iv ors of cardiac arrest . J Am Coll Cardiol 3 0: 487–495.
Hohnloser S. H., Arendt s W., Quart B., 1992 I ncidence, t y pe, and dose- dependence of pro- arrhy t hm ic ev ent s during sot alol t herapy in pat ient s t reat ed for sust ained VT/ VF. PACE Pacing Clin Elect rophy siol 1 5: 551.
Hohnloser S. H., Woosley R. L., 1994 Sot alol. N Engl J Med 3 3 1: 31- 38.
Jack m an W. M., Friday K. J., Anderson J. L., Aliot E. M., Clark M., Lazarra R., 1988 The long QT sy ndrom es: a crit ical review, new clinical observ at ions and a unify ing hy pot hesis. Prog Cardiov asc Dis 3 1: 115- 172.
Keat ing M. T., Sanguinet t i M. C., 2001 Molecular and cellular m echanism s of cardiac arrhy t hm ias. Cell 1 0 4: 569–580.
Lam as G. A., Lee K. L., Sw eeney M. O., Silverm an R., Leon A., Yee R., et al, 2002 Vent ricular pacing or dual- cham ber pacing for sinus node dy sfunct ion. N Engl J Med
3 4 6: 1854–1862.
Lehm ann M. H., Hardy S., Archibald D., Quart B., McNeil D. J., 1996 Sex difference in risk of t orsade de point es wit h d,l- sot alol. Circulat ion 9 4: 2535–2541.
McNeil D. J., Davies R. O., Deit chm an D., 1993 Clinical safet y profile of sot alol in t he t reat m ent of arrhy t hm ias. Am J Cardiol 7 2: 44- 50A.
Napolit ano C., Schw art z P. J., Brow n A. M., Ronchet t i E., Bianchi L., Pinnav aia A., et al, 2000 Ev idence for a cardiac ion channel m ut at ion underlying drug-induced QT prolongat ion and life- t hreat ening arrhy t hm ias. J Cardiov asc Elect rophy siol 1 1: 691– 696.
Pat t en M., Maas R., Bauer P., et al, Lüderit z B., Sonnt ag F., Dluzniew ski M., 2004 Suppression of parox y sm al at rial t achy arrhy t hm ias – result s of t he SOPAT t rial. Eur Heart J 2 5: 1395–1404.
Plew an A., Lehm ann G., Ndrepepa G., Schreieck J., Alt E. U., Schom ig A., et al, 2001 Maint enance of sinus rhy t hm aft er elect rical cardiov ersion of persist ent at rial fibrillat ion; sot alol v s bisoprolol. Eur Heart J 2 2: 1504- 1510.
Podrid P., 2001 Pr oarrhy t hm ia, a serious com plicat ion of ant iarrhy t hm ic drugs. Curr Cardiol Rep 1( 4) : 289- 296.
Priori S. G., Napolit ano C., Schw art z P. J., 1999 Low penet rance in t he long- QT sy ndrom e: clinical im pact . Circulat ion 9 9: 529–533.
Rosenqv ist M., Brandt J., Schuller H., 1986 At rial v ersus v ent ricular pacing in sinus node disease: a t reat m ent com parison st udy. Am Heart J 1 1 1: 292–297.
Sest i F., Abbot t G. W., Wei J., Murray K. T., Sak sena S., Schw art z P. J., et al, 2000 A com m on poly m orphism associat ed wit h ant ibiot ic- induced cardiac arrhy t hm ia. Proc Nat l Acad Sci USA 9 7: 10613–10618.
Singh B. N., Singh S. N., Reda D. J., Tang C., Lopez B., Harris C. L., et al, 2005 Am iodarone v ersus sot alol for at rial fibrillat ion ( SAFE- T) . N Engl J Med 3 5 2: 1861-1872.
Singh B. N., 1994 Am iodarone: pharm acological, elect rophy siological, and clinical profile of an unusual ant iarrhy t hm ic com pound. I n: Elect ropharm acological Cont rol of Cardiac Arrhy t hm ias. Singh B. N., Wellens H. J. J., Hiraok a M. ( eds) , pp 497- 524, Fut ura Publishing Co, NY.
Singh S. N., Tang X. C., Singh B. N., Dorian P., Reda D. J., Harris C. L., et al, 2006 Qualit y of life and ex ercise perform ance in pat ient s in sinus rhy t hm v ersus persist ent at rial fibrillat ion. J Am Coll Cardiol 4 8: 721- 730.
Touboul P., 1993 Elect rophy siologic propert ies of sot alol and d- sot alol: a current v iew. Eur Heart J 1 4( suppl H) : 24- 29.
Tse H. F., Lau C. P., 2005 Prev alence and clinical im plicat ions of at rial fibrillat ion episodes det ect ed by pacem aker in pat ient s wit h sick sinus síndrom e. Heart 9 1: 362–364. Ueshim a K., My ers J., Graet t inger W. F., At w ood J. E., Morris C. K., Kaw aguchi T., et al,
1993 Ex ercise and m orphologic com parison of chronic at rial fibrillat ion and norm al sinus rhy t hm . Am Heart J 1 2 6: 160- 161.
Verduy n S. C., Vos M. A., Van der Zande J., Van der Hulst F. F., Wellens H. J. J., 1997 Role of int erv ent ricular dispersion of repolarizat ion in acquired t orsade- de- point es arrhy t hm ias: rev ersal by m agnesium . Cardiov asc Res 3 4: 453–463.
Visw anat han P. C., Rudy Y., 1999 Pause induced early aft erdepolarizat ions in t he long QT sy ndrom e: a sim ulat ion st udy . Cardiov asc Res 4 2: 530–542.
Wallm ann D., Tuller D., Kucher N., Fuhrer J., Ar nold M., Delacret az E., 2003 Frequent at rial prem at ure cont ract ions as a surrogat e m ark er for parox y sm al at rial fibrillat ion in pat ient s wit h acut e ischaem ic st rok e. Heart 8 9: 1247- 1248.
Wellens H. J. J., Sm eet s J. L., Vos M., Gorgels A.P., 1992 Ant iarrhy t hm ic drug t reat m ent : need for cont inuous v igilance. Br Heart J 6 7: 25- 33.
Yang P., Kanki H., Drolet B., Yang T., Wei J., Visw anat han P. C., et al, 2002 Allelic v ariant s in long QT disease genes in pat ient s w it h drug- associat ed t orsades de point es. Circulat ion 1 0 5: 1943–1948.
Yigit Z., Ak dur H., Arabaci U., Gürses H. N., Güzelsoy D., 2003 Rest oring sinus rhy t hm im prov es excessive heart rat e response t o ex ercise in pat ient s wit h at rial fibrillat ion. Jpn Heart J 4 4: 73- 82.
Received: 16 June 2 011. Accept ed: 06 July 201 1. Published on line: 17 August 201 1. Aut hor s:
Ştefan H. Roşianu, Depar t m ent of Car diology, Heart Institute “Niculae Stancioiu”, “Iuliu Haţieganu” University
of Medicine and Phar m acy, 19- 2 1st Moţilor Street,
Cluj –Napoca, Cluj , Rom ânia, EU, em ail: dr .r osianu@gm ail.com
Anca D. Buzoianu, Depar t m ent of Phar m acology and Toxicolog y, „Iuliu Haţieganu” University of Medicine and Phar m acy, 13t h
Em il I sac St r eet , Cluj - Napoca, Cluj , Rom ânia, EU, em ail: ancabuzoianu@y ahoo.com
Adela Roşianu, Heart Institute “Niculae Stancioiu” 19- 21stMoţilor Street, Cluj- Napoca, Cluj , Rom ânia, EU,
em ail: adela.popa25@gm ail.com
Radu Căpâlneanu, Department of Cardiology, Heart Institute “Niculae Stancioiu”, “Iuliu Haţieganu” University of Medicine and Phar m acy, 19- 2 1stMoţilor Street, Cluj
- Napoca, Cluj , Rom ânia, EU, em ail: r adu.capalneanu@gm ail.com
How t o cit e t his ar t icle:
RoşianuŞ. H., Buzoianu A. D. , Roşianu A., Căpâlneanu R., 20 1 1 Pace and sot alol – t hr ee case r epor t s of t he
benefit s and pot ent ial hazar ds associat ed wit h sot alol adm inist r at ion in sinus node dysfu nct ion. HVM Bioflux