Arq Neuropsiquiat r 2002;60(4):889-899
JUVENILE DERM ATOM YOSITIS
Clinical, laborat orial, hist ological, t herapeut ical and
evolut ive paramet ers of 35 pat ient s
Adriana M aluf Elias Sallum
1, M aria Helena Bit t encurt Kiss
2, Silvana Sachet t i
3,
M aria Bernadat e Dut ra Resende
4, Kelly Crist ina M out inho
5, M ary de Souza Carvalho
6,
Clovis Art hur Almeida Silva
7, Suely Kazue Nagahashi M arie
8ABSTRACT - This st udy w as based on a prospect ive and a ret rospect ive analysis of 35 pat ient s w ho met Bohan and Pet er crit eria for juvenile dermat omyosit is diagnosis.The mean follow -up t ime w as t hree years t en mont hs. Calcinosis w as present in five (14.28 %) pat ient s, cut aneous ulcers in four (11.42%), and syst emic involvement in nine (27.71%) pat ient s. All pat ient s present ed alt erat ions in t he serum levels of muscle enzymes, and all of them w ere submitted to muscle biopsy as a diagnostic procedure. Nine (25.71%) patients received corticotherapy prior t o and 26 (74.28%) aft er t he muscle biopsy. Chloroquine, met hot rexat e, cyclosporine, cyclophosphamide and int ravenous immunoglobulin w ere used in pat ient s w it h poor response t o cort icot herapy. Cont inuat ion of cut aneous manifest at ions w as observed in 4 (11.43%) pat ient s, laborat orial act ivit y in 1 (2.85%), cut aneous and laborat orial act ivit ies in 3 (8.57%). Ten (28.57%) pat ient s w ere out of act ivit y, and 17 (48.57%) in remission at st udy end-point , on M arch 2002. Tw o (5.71%) pat ient s died.
KEY WORDS: juvenile dermat omyosit is, clinical findings, muscle biopsy, t reat ment , evolut ion, out come.
Dermatomiosite juvenil: parâmetros clínicos, laboratoriais, histológicos, terapêuticos e evolutivos de 35 pacientes
RESUM O - Est e est udo foi baseado na análise prospect iva e ret rospect iva de 35 pacient es que preencheram os crit érios diagnóst icos de Bohan e Pet er de dermat omiosit e juvenil. O t empo médio de seguiment o foi de 3 anos e 10 meses. Foi observado calcinose em 5 (14,28%) pacientes, úlcera cutânea em 4 (11,42%) e envolvimento sistêmico em 9 (22,71%). Todos os pacientes apresentavam alterações nos níveis séricos das enzimas musculares e t odos foram submet idos a biópsia muscular como procediment o diagnóst ico. Nove (25,71%) pacient es receberam cort icot erapia ant es e 26 (74,28%) depois da realização da biópsia muscular. Foram ut ilizados cloroquina, met ot rexat o, ciclosporina, ciclofosfamida e imunoglobulina endovenosa em t odos os pacient es que não apresent aram boa respost a ao cort icóide. Houve manut enção das manifest ações cut âneas em 4 (11,43%) pacient es, at ividade laborat orial em 1 (2,85%), at ividades cut ânea e laborat orial em 3 (8,57%). Dez (28,57%) pacient es est avam fora de at ividade e 17 (48,57%) em remissão por ocasião do t érmino do est udo em março de 2002. Dois (5,71%) pacient es faleceram.
PALAVRAS-CHAVE: dermatomiosite juvenil, achados clínicos, biópsia muscular, tratamento, evolução, prognóstico.
Pediat ric Rheumat ology Unit of Pediat ric Depart ment , Neurology Depart ament , Laborat ory of Neurological Invest igat ion, Universit y of São Paulo M edical School (USPM S), São Paulo SP, Brazil: 1M D, Post -graduat e st udent of Pediat ric Depart ment , USPM S; 2M D, PhD, Associat e Professor of Pediat rics, Children’s Inst it ut e, USPM S; 3M D, PhD, Head of Pediat ric Rheumat ology Unit , Sant a Casa de M isericórdia of São Paulo M edical School; 4M D, Post -graduat e st udent , Depart ment of Neurology, USPM S; 5Graduat e st udent ; 6M D, PhD; Neurology Depart ment , Clinical Hospit al, USPM S; 7M D, PhD, Head of Pediat ric Rheumat ology Unit , Children’s Inst it ut e, USPM S; 8M D, PhD, Associat e Professor, Head of t he Laborat ory of Neuromuscular Diseases, Depart ment of Neurology, USPM S. Grant from FAPESP 98/16290-6. Received 10 April 2002, received in final form 2 July 2002. Accept ed 17 July 2002.
Dra.Suely Kazue Nagahashi M arie - Faculdade de M edicina da Universidade de São Paulo - Depart ament o de Neurologia - Laborat ório de M iopat ias e Biologia M olecular - Avenida Dr. Arnaldo 455 sala 4110 - 01246-903 São Paulo SP - Brasil. FAX: 11 30614036. E-mail: [email protected].
Dermat omyosit is is a rare mult isyst em disease, w hose et iology is unknow n, charact erized by a vas-culit is t hat affect s skin and muscles1-3. M ost st udies
suggest t hat juvenile dermat omyosit is (JDM ) is au-t oimmune in paau-t hogenesis and resulau-t s from a vascu-lopat hy. Bot h cell-mediat e immunit y t o muscle ant
i-gens and immune-complex disease may play roles in pathogenesis1. Dermatomyositis is one of a
eri-890 Arq Neuropsiquiat r 2002;60(4)
zat ion of t his group of diseases is based on muscular involvement , associat ion of clinical manifest at ions, hist ological alt erat ions, response t o cort icot herapy and prognosis4,5.
Alt hough clinical, laborat orial, hist ological, t he-rapeut ical and evolut ive aspect s of t his disease have been analyzed in many previous st udies, t he majorit y of t hese st udies w ere carried out some years ago, and t herefore may not accurat ely reflect t he st at us of t he disease as it current ly st ands.
We describe clinical, laborat orial, t herapeut ical, hist ological and out come paramet ers of 35 pat ient s w it h JDM , based on a mean follow -up of 3 years 10 mont hs, ranging from one year nine mont hs t o t en years t hree mont hs.
M ETHOD
Pat ient select ion: Thirt y-five JDM pat ient s fulfilling Bo-han and Pet er crit eria6, at t ending t he Pediat ric
Rheuma-t ology UniRheuma-t aRheuma-t Rheuma-t he Children’s InsRheuma-t iRheuma-t uRheuma-t e of Rheuma-t he UniversiRheuma-t y of São Paulo M edical School and Sant a Casa de M isericórdia de São Paulo, have been st udied. The evaluat ion w as pros-pect ive from February/1999 t o M arch/2002 in 25 pat ient s, and ret rospect ive over t he period M arch/1991 t o M arch/ 2002 in 10 pat ient s. Bohan and Pet er6 suggest ed a
classi-ficat ion based upon t he presence or absence of five major crit eria for diagnosis, including symmet ric muscle w ea-kness, evidence of inflammat ory myosit is in muscle biopsy, elevat ion of serum muscle enzymes, elect romyographic evidence of inflammat ory myopat hy and dermat ological pat hognomonic feat ures of dermat omyosit is (heliot rope and Got t ron´ s papules). A diagnosis of JDM requires t he presence of the pathognomonic rash and three of the other crit eria1. A diagnosis of JDM is not excluded by t he failure
t o meet one or more crit eria1.
Clinical evaluat ion: The clinical paramet ers analyzed w ere cutaneous manifestations such as heliotrope, Gottron papulae, erit hem a m alar, palm ar, periungueal, and in t runk, skin ulcers and calcinosis; involvement of int ernal organs, and muscle involvement according t o t he scale est ablished by t he M edical Research Council (M RC) in 19437 w here: 0= no cont ract ions, I= flicker or t race of
cont ract ion, II= act ive movement w it h gravit y eliminat ed, III= active movement against gravity, IV= active movement against gravit y and resist ance, and V= normal pow er.
Laborat ory evaluat ion: Ant inuclear and ant Jo-1 ant i-bodies, eryt hrocyt e sediment at ion rat e, serum levels of t he muscle enzymes AST, ALT, DHL and CK w ere analyzed at t he t ime of t he biopsy.
Histopathological evaluation of skeletal muscle: M uscle biopsy specimens w ere obtained from brachial biceps mus-cle in all pat ient s and a t ot al of 37 musmus-cle fragment s w ere submit t ed t o hist opat hological analysis. Specimens 2 and
5 w ere from a boy w ho present ed persist ent at ypical cu-t aneous alcu-t eracu-t ion and w as resubmicu-t cu-t ed cu-t o muscle biopsy, w it h a 40-mont h int erval from t he first procedure. Ad-dit ionally, specimens 9 and 14 w ere from a girl present ing an at ypical associat ion w it h ment al ret ardat ion and w ho w as submit t ed t o a second biopsy for diagnost ic confir-mat ion aft er an 8-mont h int erval. M uscle biopsy w as per-formed before cort icot herapy in 26 pat ient s, and aft er t he int roduct ion of t he medicat ion in 9.
Routine standard histological and histochemical techni-ques w ere employed in muscle biopsies. Frozen sequent ial sect ions w ere st ained w it h hem at oxylin-eosin (H&E), modified Gomori t richrome, periodic acid Schiff, cyt och-rome C oxydase, NADH-t et razolium-reduct ase, succinat e dehydrogenase, adenosine t riphosphat ase pH 4.3 and 9.4, alkaline and acid phosphat ase. Each biopsy specimen w as coded and analyzed concomit ant ly by t w o invest igat ors (AM ES and SKNM ). Presence of int ernal nuclei, f ocal m yo f ib rillar lo ss, n ecro t ic f ib er, reg en erat in g f ib er, perivascular inflammat ion, endomysial inflammat ion, and increased connect ive t issue w as observed in all prepara-t ions. Degeneraprepara-t ive aspecprepara-t s w ere confirmed in acid phat ase react ion, regenerat ive aspect s in alkaline phos-phat ase and proliferat ion of connect ive t issue in modified Gomori st aining. These alt erat ions w ere analyzed semi-quant it at ively w here: (-)= absent ; (+ )= present in less t han 25% of t he analyzed fields; (+ + )= present in 50%; (+ + + )= present in 75%; (+ + + + )= present in 100%.
Therapeut ical evaluat ion: All pat ient s received cort i-cot herapy (prednisone or met ilprednisolone), and init ial t herapeut ical response w as analyzed at bet w een 4 t o 6 w eeks follow ing t he int roduct ion of medicat ion; response w as considered good, part ial or bad, based on t he impro-vement of muscle st rengt h and/or cut aneous lesions. Chlo-roquine, met hot rexat e, cyclosporine, cyclophosphamide and/or int ravenous immunoglobulin w ere administ ered t o all pat ient s t hat present ed part ial or bad init ial responses.
Evolution analysis: Cont inuat ion of clinical act ivit y w as considered w hen t here w as persist ent muscle w eakness or cut aneous act ivit y charact erized by eit her t he presence of eryt hem a, heliot rope, Got t ron papulae, cut aneous ulcers, or laborat orial act ivit y during w hich, increased serum levels of muscle enzymes w ere maint ained. Out of act ivit y w as deemed w hen t here w as an absence of symp-t oms and signs w isymp-t h consymp-t inued medicasymp-t ion and remissions w hen t he children present ed asympt omat ic w it hout me-dication. All patients w ere classified according to these dif-ferent clinical criteria at study end-point, on M arch 2002.
RESULTS
Arq Neuropsiquiat r 2002;60(4) 891
male (26 females and 9 males). All pat ient s fulfilled Bohan and Pet er crit eria for dermat omyosit is, w it h t he p resence of charact erist ic cut aneous lesion (Got t ron´ s papules and/or heliot rope), in addit ion t o t hree ot her crit eria. It w as not ew ort hy t hat cut a-neous and subcut aa-neous involvement w as severe in four (11.42%), presenting cutaneous ulcer, w hile four ot her pat ient s had calcinosis. Gast roint est inal t ract involvement w as observed in six (17.14%) pat ient s, w hereas f ive p resent ed p ulm onary involvem ent (14.28%), and t hree (8.57%) present ed cardiac in-volvement . The majorit y of t he pat ient s present ed some degree of muscle w eakness, according t o t he M RC scale, w it h t he except ion of 3 pat ient s (cases 2/ 5, 14 and 21) w it h normal muscle st rengt h, in w hom JDM diagnosis w as est ablished w it h t he associat ion of ot her signs (Table 1).
Laborat orial charact erist ics: The ant inuclear an-t ibody w as posian-t ive in 14 (40%) paan-t ienan-t s, in conan-t rasan-t t o t he negat ivit y of t he ant i-Jo-1 ant ibody in all pa-t ienpa-t s, even in pa-t hose presenpa-t ing pulmonary involve-ment . The eryt hrocyt e sediinvolve-ment at ion rat e w as posi-t ive in five (14.28%) paposi-t ienposi-t s.
All pat ient s present ed at least one of t he muscle serum enzyme altered. The serum levels of CK compa-red t o serum levels of LDH, AST and ALT are show n in Graph 1. Int erest ingly, a normal range of CK w as observed in 31.5%, in cont rast t o 3%, 17% and 29% of normal values for ALT, LDH and AST, respect ively. A similar percent age of pat ient s present ed CK levels
w hich w ere either normal, 5 times normal or up to 15 times normal, w hereas a higher percentage of patients presented 5 times normal level of LDH, AST and ALT.
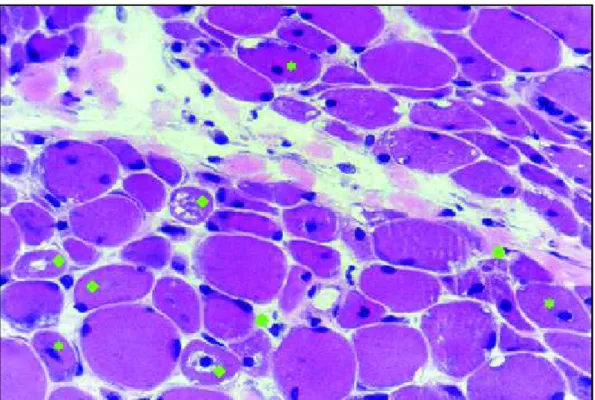
Hist opat hological f indings f or skelet al muscle (Table 1): M orphological alt erat ions on muscle fibers including miofibrillar loss, necrot ic fibers, regenera-t ing fibers w ere observed in all cases excepregenera-t four (Fig 2). Degenerat ing aspect s of muscle fibers w ere not ed in all specimens and bet t er demonst rat ed in acid phosphat ase react ion (Fig 3).
The mean t ime up t o t he biopsy w as 11 mont hs (± 16 mont hs 15 days) w it h median of 4 mont hs, ranging from 1 t o 64 mont hs. Five pat ient s had t heir biopsies performed more t han one year aft er disease onset , including t he t w o pat ient s submit t ed t o a se-cond biopsy. M orphological alterations in muscle bio-psies of t hese pat ient s w ere markedly slight , ran-ging f rom absent , t o 50% of t he analyzed f ields (+ + ), in concordance t o t he moderat e muscle w ea-kness t o normal muscle st rengt h observed. Their CK levels w ere also normal, except in Case 9/14, w hich present ed 25 t imes t he normal level at first biopsy, d ecr easi n g t o 3 t i m es at t h e seco n d b i o p sy performed 8 mont hs lat er. It is not ew ort hy t hat in spit e of t he marked CK level increase in t he lat t er case, t he muscles’ st ruct ural alt erat ions, including m u scle f ib er m o rp h o lo g ical d eran g em en t an d presence of inflammat ory infilt rat ion, w ere negli-gible. M oreover, t he perifascicular at rophy w as only dem onst rat ed in t he second biopsy. The t w o
8
9
2
A
rq
N
e
u
ro
p
si
q
u
ia
tr
2
0
0
2
;6
0
(4
)
Table 1. Clinical, laborat orial and skelet al muscule biopsy f indings in 37 muscle specimens of 35 pat ient s of juvenile dermat omyosit is.
Sex Age at Time up t o Signs & M uscle CK Perifascicular Focal myofibrillar Necrot ic Regenerat ing Perivascular Endomysial Increased
onset biopsy (mo) sympt oms st rengt h at rophy loss fibers fibers inflammat ion inflammat ion connect ive t issue
1 F 6y3mo 1 II 711 P + + + + + + + + +
-2 M 3y1m o 24 CCa V 71 p + + + + + + +
-3 F 7y 2 IV 1785 p + + + + + + + + + + + + + + + +
4 F 9y11mo 4 PG I 1051 p + + + + + + + + + + + + + + + + + +
5 M 3y1m o 64 C V 33 p + + + + + + +
6 F 3y8mo 4 II 141 p + + + + + + + + + + + + + +
7 F 9y6mo 3 P III 1281 p + + + + + + +
8 M 8y8m o 24 C IV 33 p + + - + +
-9 F 4y8mo 36 III 4365 p - - - + - +
10 M 1y6mo 4 UCCaG II 240 p + + - + + +
11 F 5y6mo 4 UPG IV 358 p + + + + + +
12 M 9y 18 III 197 p + + + + + + + +
13 F 5y8m o 3 IV 636 p + - + + -
-14 F 4y8m o 44 V 503 p - - + + + +
15 F 4y6m o 12 III 371 p + + + + + + + +
16 F 9y9m o 4 IV 57 p - - - + -
-17 M 7y8mo 1 III 2168 p + + + + + + + + + + + + + + +
-18 F 1y5mo 12 III 2488 p + + + + + + + + + + + + + + +
19 F 9y1m o 2 UPG III 34 p + + + + + +
-20 F 8y8mo 3 IV 5022 p + + + + + +
-21 F 8y1m o 1 V 138 p - - - + -
-22 F 9y 4 III 1874 p + + + + + + + +
23 F 7y11mo 9 U III 507 p + + + + + + + + + + + + + + +
24 F 1y5mo 2 III 358 p + + + + + + + + + + + +
25 F 10y6mo 2 Ca III 113 p + + + + + + + + + + +
26 F 6y10mo 2 G III 1173 p - - -
-27 F 8y 6 IV 734 p - + + + + + + + +
-28 F 5y8m o 4 PG II 605 p + + + + + + + + + + + +
29 F 2y4mo 2 IV 2670 p + + + + + + + + +
30 M 11y 36 C IV 88 p + - - + -
-31 M 8y6mo 1 II 1269 p + - - + -
-32 F 9y1mo 1 IV 1147 p + + + + +
-33 F 12y8mo 3 III 11640 p + + + + + + + + + + +
34 M 7y 8 IV 504 p + + - + + + +
-35 F 13y 6 III 378 p + + + + + + + + + + +
-36 F 6y 4 III 92 p + + + + + + + + + + + + + + +
37 M 4y 3 IV 205 p + - + + + +
A
rq
N
e
u
ro
p
si
q
u
ia
tr
2
0
0
2
;6
0
(4
)
8
9
3
Table 2. Treat ment administ ered t o each of 35 JDM pat ient s, init ial response t o cort icot herapy, f ollow t ime and out come at t he st udy end-point .
Case
Cort icot herapy Init ial response Chloroquine M et hot rexat e Cyclosporine Cyclophosphamide IV IgG Follow up t ime Out come at st udy end-point
before bx aft er bx (4 -6w ) (mo)
1 + part ial + + 77 out of act ivit y
2 + part ial + 130 laborat orial and cut aneous act ivit y
3 + good 72 remission
4 + good 70 out of act ivit y
5 + part ial + 130 laborat orial and cut aneous act ivit y
6 + part ial + 58 remission
7 + bad + + + + 56 out of act ivit y
8 + part ial + + 102 remission
9 + good 51 out of act ivit y
10 + part ial + + + 49 out of act ivit y
11 + bad + + + + + 46 deat h
12 + good 15 remission
13 + part ial + 46 remission
14 + good 51 out of act ivit y
15 + part ial + 41 out of act ivit y
16 + part ial + 38 remission
17 + part ial + 39 remission
18 + part ial + 39 out of act ivit y
19 + good 38 out of act ivit y
20 + good 38 laborat orial and cut aneous act ivit y
21 + good 36 cut aneous act ivit y
22 + no adherence - deat h
23 + part ial + + 35 cut aneous act ivit y
24 + part ial + 35 cut aneous act ivit y
25 + good 36 laborat orial act ivit y
26 + part ial + 33 remission
27 + part ial + 29 remission
28 + bad + + 30 out of act ivit y
29 + good 28 remission
30 + part ial + 29 remission
31 + good 39 remission
32 + good 26 remission
33 + part ial + 25 cut aneous act ivit y
34 + good 24 remission
35 + good 22 remission
36 + good 21 remission
37 + good 21 remission
894 Arq Neuropsiquiat r 2002;60(4)
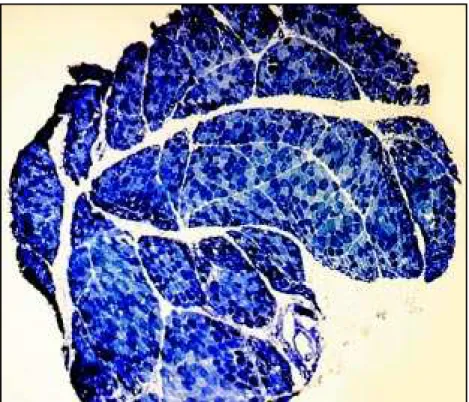
Fig 1. Transversal sect ion of f rozen skelet al m u scle, 5µ o f t h ick n ess, h ist o ch em ical preparat ion of NADH, 40x. All t he f ascicles in t he f ragment show perif ascicular at rophy charact erized by muscle f ibers w it h decre-ased diameter distributed at periphery of the f ascicle.
quent ial biopsies performed in anot her case (2/5) w it h a 40-mont h t ime int erval show ed few differen-ces bet w een t hem. In t he second biopsy, an increase in connect ive t issue and a slight decrease in perivas-cular inflammat ion, w hich had been scant from t he out set , w ere observed.
30 biopsies w ere performed on pat ient s during t heir first 12 mont hs of sympt oms, and among t hem 5 biopsies w ere carried out in t he first mont h, 6 in t he second mont h, 5 in t he t hird mont h, 8 in t he fourt h mont h, 2 in t hesixt h mont h and 4 bet w een t he sevent h and t w elft h mont hs of disease onset . Alt hough t he number of cases in each t ime int erval w as t oo small t o permit st at ist ical analysis, t he mus-cle lesion and inflammat ory infilt rat ion w ere more evident in t he group w it h less t han one year of dise-ase. 40% of biopsies performed in t he first mont h present ed muscle alt erat ion for more t han 50% (+ + ) of fields st udied, w hereas t he frequency of muscle lesions increased t o 67% - 100% of cases in subse-quent t ime int ervals up t o 12 mont hs.
Perifascicular at rophy w as det ect ed in all cases, independent of evolut ion t ime, being present even in t he first mont h of t he disease (Fig 1). Int erest ingly, slight proliferat ion of connect ive t issue w as observed even in t he first mont h since t he onset of sympt oms. Surprisingly, st riking inf lam m at ory inf ilt rat ion (+ + /+ + + /+ + + + ), eit her endom ysial or perivas-cular, w as observed in 5 out of 9 pat ient s w ho had been t reat ed w it h cort icot herapy before t he biopsy
procedure. Coincident ally, t he great majorit y (4/5) w ere female pat ient s.
No relation w as observed betw een degree of mor-phological muscle lesion, degree of inflammat ory in-filt rat ion and CK serum level. Similarly, no associat ion w as found concerning CK level and evolut ion t ime interval up to biopsy and degree of muscle w eakness.
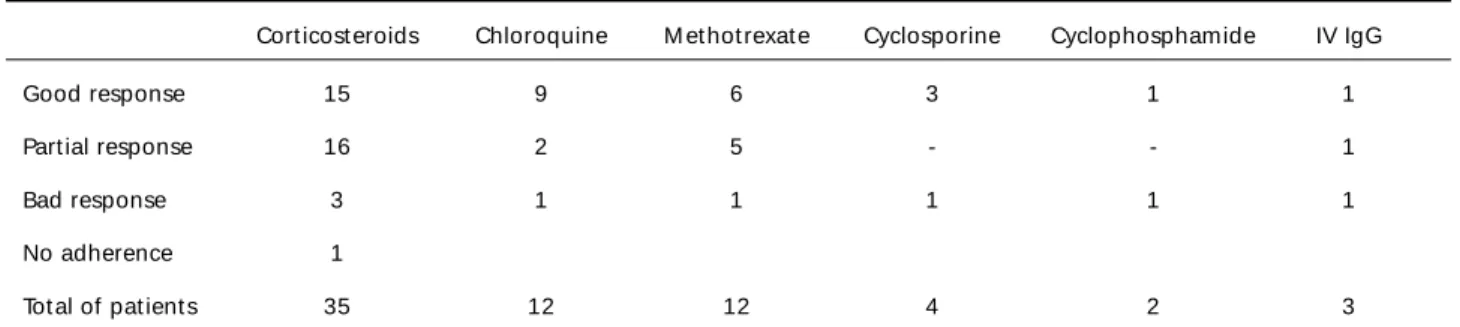
Therapeutical and evolutional characteristics: All patients received corticotherapy, 9 (25.71%) patients received therapy prior to muscle biopsy, and 26 (74.28%) patients after it. 15 patients presented initial good ponse needing no complementary therapy. Partial res-ponse w as observed in 16 patients, and bad resres-ponse in 3, w hom received additional associated therapy w ith Ch lo ro q u in e (12 p at ien t s), M et h o t rexat e (12), Cyclosporine (4), Cyclophosphamide (2) and intrave-nous Immunoglobulin (3). The medication adminis-tered to each patient, along w ith corresponding initial therapeutical status and outcomes at study end-point (M arch 2002), are listed in Tables 2 and 3.
Arq Neu ro p siq u iat r 2002;60(4) 8 9 5
Fig 2. Transversal section of frozen skeletal muscle, 5µ of thickness, histological preparation of hematoxilin-eosin, 400x. Note the marked morphological alterations in the majority of muscle fibers characterized by the presence of internal nuclei ( ), focal myofibrillar losses w ith vacuolization ( ) and necrotic fibers ( ).
Fig 3. Transversal section of frozen skeletal muscle, 5µ of thickness, histochemical preparation of acid phosphatase, 200x. Red reaction in muscle fibers and vessels represent lisossomal activity distributed mainly at the periphery of fascicles.
The analysis of outcom es at study end-point revea-led continuation of clinical activity associated to cuta-neous manifestations in 4 (11.43%) patients, laborato-rial activity in 1 (2.85%), cutaneous and laboratolaborato-rial activities in 3 (8.57%), out of activity in 10 (28.57%), and
896 Arq Neuropsiquiat r 2002;60(4)
Table 3. Therapeut ical response in 35 JDM pat ient s.
Cort icost eroids Chloroquine M et hot rexat e Cyclosporine Cyclophosphamide IV IgG
Good response 15 9 6 3 1 1
Part ial response 16 2 5 - - 1
Bad response 3 1 1 1 1 1
No adherence 1
Tot al of pat ient s 35 12 12 4 2 3
IV IgG, int ravenous Immunoglobulin G.
No relapses w ere observed am ong pat ient s in rem issio n , f o llo w -u p b ein g f o r 37 m o n t h s o n average. 11 out of 17 pat ient s in remission had more t han 2 years of follow -up.
Among 13 pat ient s present ing syst emic involve-ment , 8 pat ient s (61.5%) present ed good out comes, independent of t he CK level, degree of muscle st ren-gt h or inflammat ory infilt rat ion in muscle biopsy.
DISCUSSION
JDM makes up approximat ely 5% of annual visit s t o Pediat ric Rheumat ology reference cent ers4. In our
experience, JDM ranks fourt h among rheumat ologic diseases, aft er rheumat ic fever, juvenile rheumat oid art hrit is and syst emic lupus eryt hemat osus8. It has
been est imat ed t hat about one t hird of t he 1000 or so cases published in t he w orld lit erat ure, w ere in t he pediat ric age group (under 16 years)9.
JDM is different from t he adult form of dermat o-myosit is. The clinical present at ion in children is more frequent ly insidious and may be dominat ed by cons-t icons-t ucons-t ional sym p cons-t om s of f acons-t ig ue, m alaise, f ever, anorexia and w eight loss. Addit ionally, children have more oft en a mult isyst em vasculit is, w hich may in-volve t he skin, gast roint est inal mucosa, heart , and ret ina. Children w it h longst anding, unt reat ed dise-ase, w ith generalized cutaneous vasculitis, frequently develop calcinosis. The associat ion of malignancy w it h t he developm ent of m yosit is has been w ell described in adult s, but only rarely report ed in chil-dren . Once remission is achieved, chilchil-dren appear to return to normal muscle strength and function, mo-re fmo-requently than adults w ith dermatomyositis10-12.
Out come depends on t he precocit y of diagnosis and t reat ment . Predict ive paramet ers t o guide t he correct t herapeut ical approach, and for prognosis, are st ill lacking in JDM .
Therefore, t his st udy w as designed t o describe clinical, laborat orial, and hist ological findings, and
t o correlat e t hem t o early response t o t he t herapy adopt ed and t o longst anding out come feat ures, in 35 JDM pat ient s.
Age and gender distribution: It w as previously re-ported that the most common age for onset of JDM w as 6 years for boys, w ith tw o peaks of 6 years and 10 years for girls, w ith an overall average of 7 years for disease onset1. The mean age of disease onset in
our study was in accordance with these reports, being 6 years 10 months on average, 6 years for boys, with peaks of 4 years 10 months and 9 years 6 months for girls.
A female predominance has been described in most of t he rheumat ic diseases in childhood, as w as observed in t he present st udy w it h a female t o male proport ion of 2.8:1.
Clinical findings: All pat ient s in t his st udy fulfilled t h ese d iag n o st ic cr it er ia. An asso ciat io n w it h w idespread vasculit is has also been made in t his chil-dhood disease. In fact, 34% of our patients presented systemic involvement including gastrointestinal tract, cardiac, respirat ory and more severe cut aneous alt e-rat ions, t han predict ed w it hin t he diagnost ic crit eria.
JDM may be associat ed w it h mot or dysfunct ion of t he ent ire gast roint est inal t ract . Abnormal eso-phageal mot or funct ion is a complicat ion of t he di-sease and esophageal sym pt om s are f requent ly present . Small and large bow el involvement has also been docum ent ed13. Our pat ient s present ed
eso-phageal gastric reflux, dysphagia and upper digestive t ract bleeding.
There are few report s in t he lit erat ure on cardiac involvement in JDM1. A few pat ient s have cardiac
m urm urs or pericardial f rict ion rubs and a high proport ion show ECG changes14. In t his st udy, t hree
Arq Neuropsiquiat r 2002;60(4) 897
Lungs may be affect ed in JDM , primarily or t hro-ugh com plicat ions of m uscle w eakness15. In t his
st udy, aspirat ive pneumonia w as present in t w o pa-t ienpa-t s and inpa-t erspa-t ipa-t ial disease in pa-t hree papa-t ienpa-t s. The pat hological mechanisms of int erst it ial lung disease remain unknow n. There is evidence t hat bot h cell mediat ed and humoral immunit y play a role in t he pat hogenesis of t his lesion. M ore recent ly, t he role of t he ant i-Jo-I ant ibody has been highlight ed15 in
associat ion w it h pulmonary int erst it ial disease. Ho-w ever, t he ant i-Jo-I ant ibody Ho-w as negat ive in all pa-t ienpa-t s in pa-t his spa-t udy, even in pa-t hose papa-t ienpa-t s w ipa-t h in-terstitial disease, w hich corroborates previous reports describing t he rarit y of it s presence in childhood.
Dystrophic calcification is tw o or three times more f requent in JDM t han in adult derm at om yosit is, occurring in 40% to 75% of children w ith JDM16. The
calcification occurs in the interstitial of muscle or in the subcutaneous tissue, and it is readily visible on X-ray. Nodules of calcium may be ext ruded t hrough perforations in the skin. We found a lesser incidence of calcinosis in our casuistic (11%) than seen previously.
Skin ulcerat ion may be considered among t he sys-t emic angiopasys-t hy referred sys-t o by Banker and Vicsys-t or17,
w here necrot izing vasculit is has been ident ified. The same pat hological condit ion has been described in skelet al muscle, subcut aneous t issue and gast t est inal t ract , result ing in muscle infarct ion, gast roin-t esroin-t inal ulceraroin-t ion, bleeding and perforaroin-t ion, cons-t icons-t ucons-t ing one of cons-t he major causes of deacons-t h18. Few
pa-t ienpa-t s in pa-t he presenpa-t spa-t udy presenpa-t ed skin ulcerapa-t ion (11%), how ever it w as present in one of t he 2 fat al cases, being part of t he syst emic angiopat hy t hat lead t o deat h.
Alt hough muscle w eakness is one of t he crit eria for diagnosis of inflammat ory myopat hy, it is not easy t o assess t his alt erat ion object ively. The st rengt h of muscles may be graded according t o t heir abilit y t o act against gravit y and resist ance offered by an exam iner, as proposed by t he w ell-know n M RC grading syst em . How ever, such a syst em has t he disadvant age of being subject ive, depending on exa-miner impression. M oreover, about 40% of ext remit y muscles such as rot at ors and muscles moving fingers and t oes, are not significant ly affect ed by gravit y. A careful examinat ion of muscle st rengt h, t aking int o acco u n t t h ese d if f icu lt ies, d ep ict ed o n ly t h ree pat ient s w it h normal muscle pow er from our cases. A bet t er, non-invasive met hod of assessing muscle funct ion is necessary t o permit correlat ion of t his paramet er t o ot her findings, t hus permit t ing a bet t er search for predict ive fact ors of evolut ion in JDM19.
Laboratorial and histopathological findings of ske-let al muscle: It has been st ressed t hat t he serum levels of muscle enzymes are import ant for diagnosis and f or monit oring t he ef f ect iveness of t herapy1.
How ever, CK levels w ere norm al in 31% of our patients, in spite of presenting muscle w eakness and/ or structural alterations and inflammatory infiltration in muscle biopsy. Unfort unat ely, t he degree of incre-ase in CK level did not also predict t he out come. The ot her muscle enzymes present ed similar behavior.
Ot her serum specific markers for myosit is have been considered, and ant ibody ant i-M i-2, an ant ibo-dy against cyt oplasmic ribonucleoprot ein evolved in t he t ranslat ion process, is one of t hese candidat es. How ever, in cont rast t o presence of ant i-M i-2 of up t o 95% in dermat omyosit is w it h classical cut aneous involvement , only 10-50% of cases of JDM present ed t his ant ibody. Therefore, most previous st udies do not recommend rout ine clinical t est ing for ant M i-2 since t he yield is likely t o be low. M oreover, it seems not t o be a prognost ic fact or20.
Other non-specific indicators of inflammation, such as erythrocyte sedimentation rate, tend to correlate w ith the degree of clinical inflammation, and have are useful in differentiating inflammatory myopathies from non-inflammat ory muscle disorders. How ever, t he reported results are also variable and likely to be low.
On t he ot her hand, muscle biopsy is import ant for est ablishing t he diagnosis of an inflammat ory myopat hy and for underst anding t he charact er of the inflammatory change, such as its distribution and t he degree of parenchyma involvement21. Alt hough
perifascicular atrophy may be present in other patho-logies as dyst rophies, it w as described as a frequent finding in definit e DEM22 and w as found in all cases
st udied here (Fig 1). Perif ascicular at rophy in t he present st udy w as observed as early as 1 mont h from t he onset of sympt oms and persist ed for at least 64 m ont hs of t he act ive disease. The inf lam m at ory infilt rat ion seems t o be more evident from bet w een t w o mont hs of disease onset and up t o one year, most ly in t he first six mont hs of t he disease. Aft er one year, t here is ap p arent ly a d ecrease in t he inflammat ory alt erat ions, even if unt reat ed.
898 Arq Neuropsiquiat r 2002;60(4)
Despit e muscle biopsy being a fundament al diag-nost ic t ool, it s hist ological analysis is insufficient as a prognost ic fact or. Fut ure biological markers, such as prot eins involved in t he pat hom echanism s of t issue lesions, may be st udied in muscle specimens by immunohist ochemical met hods t o guide t he best t herapeut ical approach23-25.
Therapeut ical and evolut ional charact erist ics: Treat m ent w it h cort icost eroids does im prove t he prognosis. The deat h rat e is reduced from around 33% t o less t han 10%26. The acut e st age, during
w hich t herapy is required, is generally self-limit ed and lasts for about tw o years27. Chloroquine has been
used as a st eroid-sparing agent , and as a drug t hat is ef f ect ive in t reat ing t he d erm at it is of JDM1.
Glucocorticoid resistance or dependence is the primary indication for the use of immunosupressive drugs1. It
is difficult to evaluate the efficacy of these drugs, since there have been no controlled trials in JDM treatment. How ever, some publications confirm the efficacy of corticotherapy, or other highly selective immunosup-pressive therapy, in the management of this disease during its acute phase. M ost authors agree that early diagnosis and early aggressive therapy, result either in reducing mortality or improving functional recovery28.
Thus, the 74% remission or out of activity achieved by our patients at the study end-point, also corroborates these reports. The high incidence (88%) of some extent of response t o cort icot herapy in our st udy, also confirms the efficacy of its use, and strongly suggests this as the drug of first choice.
The majorit y of fat alit ies occur w it hin t w o years of disease onset , according t o several report s29,
alt hough t here are several periods of increased vul-nerabilit y t o life-t hreat ening complicat ions, during t he init ial year of t reat ment . Gast roint est inal ulce-rat ion, hemorrhage and perfoulce-rat ion, and myocardial and respirat ory failure have been described as major causes of deat h in JDM30. Pulmonary involvement is
anot her import ant cause of morbidit y and mort alit y in JDM . Concordant ly, one of our cases present ed a fat al evolut ion ow ing t o complicat ions of mult isys-t emic involvemenisys-t . Non-adherence isys-t o isys-t reaisys-t menisys-t w as t he cause of our ot her fat al case. Lat er relapses w it h cort icost eroid t reat ment programs (prednisone do-ses < 15 mg) in t he first 24 mont hs aft er cessat ion of treatment have also been described31. Our patients
in rem ission, observed f or m ore t han 2 years on average, have not present ed relapses t o dat e. A lengt hier follow -up w ill permit furt her conclusions t o be draw n on t he out comes.
The present analysis of a represent at ive number of cases of JDM , a rare childhood m ult isyst em ic disease, permit t ed us t o conclude t hat :
1. Skelet al muscle involvement can be assessed by clinical evaluat ion, a qualit at ive met hod; by CK serum levels, not alw ays corresponding t o clinical or st ruct ural m uscle condit ion; and by m uscle biopsy, w it h perifascicular at rophy as a const ant finding.
2. Adequate diagnosis and therapy resulted in a 74% good out come w it hin a mean follow -up period of 3 years 10 mont hs.
3. None of t he p aram et ers analyzed , includ ing m uscle w eakness, m ult isyst em ic alt erat ion, CK level, degree of inf lam m at ory inf ilt rat ion and muscle fiber morphological alt erat ion, present ed predict ive value.
4. Furt her st udies are necessary aimed at finding b iolog ical m arkers t o select and g uid e new t herap eut ical ap p roaches f or t hose p at ient s present ing draw backs.
REFERENCES
1. Cassidy JT, Petty RE. Juvenile dermatomyositis. In Cassidy JT, Petty RE (Eds.). Textbook of pediatric rheumatology. 3 Ed. Philadelphia: Saunders, 1995:323-364.
2. A nsell BM. Juv enile d ermato myo sitis. Rheum Dis Clin N A m 1991;17:931-942.
3. Ansell BM. Juvenile dermatomyositis. J Rheumatol 1992;19:60-62. 4. Mastaglia FL, Ojeda VJ. Inflammatory myophaties: Part I. Ann Neurol
1985;17:215-227.
5. Mastaglia FL, Ojeda VJ. Inflammatory myophaties: Part II. Ann Neurol 1985;17:317-323.
6. Bohan A, Peter JB. Polymyositis and dermatomyositis. N Engl J Med 1975;13:344-347.
7. Medical Research Council. Aids to the investigation of peripheral nerve injuries. W ar Memo rand un No 7, 2.Ed . Lo nd o n: Her Majesty’ s Stationery Office, 1943.
8. Sogabe T. Dermato/ polimiosite juvenil: estudo das características clínico-laboratoriais em 40 crianças. Dissertação (Mestrado) Uni-versidade de São Paulo SP, 1993.
9. Bitnum S, Daeschner CW , Trav is LB, Do d g e W F, Ho p p s HC. Dermatomyositis. J Pediatr 1964;64:101-131.
10. Callen JP. Relationship of cancer to inflammatory muscle disease: dermatomyositis, polymyositis and inclusion body myositis. Rheum Dis Clin N Am 1994;20:943-953.
11. Caloew EE, Cavaliere MJ, Perez NM. Muscle pathology in juvenile dermatomyositis. São Paulo Med J 1997;115:1555-1559.
12. Rider L. Childhood myositis: newly recognized diversity. In Plotz P (moderator). Myositis: immunologic contributions to understanding cause, pathogenesis, and therapy. Ann Intern Med 1995;122:715-724. 13. Horow itz M, McNeil JD, Maddern GJ, Collins PJ, Shearman DJC.
Abnormalities of gastric and esophageal emptying in polymyositis and dermatomyositis. Gastroenterology 1986;90:434-439.
14. Dubowitz V. Inflammatory myopathies. In Dubowitz V (ed). Muscle disorders in childhood. 2.Ed. Philadelphia: Saunders, 1995:422-456. 15. Marie I, Hatro nP-Y, Hachulla E, Wallaert B, Micho n-Pasturel U,
Devulder B. Pulmonary involvement in polymiositis and in derma-tomyositis. J Rheumatol 1998;25:1336-1343.
16. Bow yer SL, Blane CE, Sullivan DB, Cassidy JT. Childhood derma-tomyositis: factors predicting functional outcome and development of dystrophic calcification. J Pediatr 1983;103:882-888.
17. Banker BQ, Victor M. Dermatomyositis (systemic angiopathy) of childhood. Medicine 1966;45:261-289.
Arq Neuropsiquiat r 2002;60(4) 899
19. Hoskimg GP, Bhat US, Dubowitz V, Edwards RHT. Measurements of muscle strength and performance in children with normal and diseased muscle. Arq Dis Child 1976;51:957-963.
20. Feldman BM, Reichlin M, Laxer RM, Targoff IN, Stein LD, Silverman ED. Clinical significance o f sp ecific auto antibo d ies in juv enile dermatomyositis. J Rheumatol 1996;23:1794-1797.
21. Dubowitz V. Histological and histochemical stains and reactions. In: Dubowtiz V (ed). Muscle biopsy: a practical approach. 2.Ed. London: Baillière Tindall, 1985:19-40.
22. Scola RH, Werneck LC, Prevenello DMS, Toderke EL, Iwamoto FM. Diagnosis of dermatomyositis and polymyositis: a study of 102 cases. Arq Neuropsiquiatr 2000;58:789-799.
23. Gonçalves FGP, Chimelli L, Sallum A ME, Marie SKN, Kiss MHB, Ferriani VPL. Immunohistological analysis of CD59 and membrane attack complex of complement in muscle in juvenile dermatomyositis. J Rheumatol 2002;29:1301-1307.
24. Sallum AME. Expressão das moléculas de adesão (ICAM-1 e VCAM-1) em tecido muscular de pacientes com dermatomiosite juvenil. Dissertação
(Mestrado) Faculdade de Medicina da Universidade de São Paulo, 2002. 25. Carvalho, AAS. Estudo imuno-histoquímico do complexo maior de
histo co mp atibilid ad e classe I nas d o enças neuro musculares. Importância no diagnóstico diferencial das miopatias inflamatórias. Tese (Doutorado), Universidade de São Paulo, São Paulo 1996. 26. Yo shio ka M, Okuno T, Mikaw a H. Pro gno sis and treatment o f
polymiositis with particular reference to steroid patients. Arch Dis Child 1985;60:236-244.
27. Miller JJ. Late progression in dermatomyositis in childhood. J Pediatr 1973;83:543-548.
28. Sullivan DB, Cassidy JT, Petty RE. Dermatomyositis in pediatric patient. Arthritis Rheum 1977;20:327-331.
29. Goel KM, Shanks RA. Dermatomyositis in childhood: review of eight cases. Arch Dis Child 1976;51:501-506.
30. Pachman LM, Cooke N. Juvenile dermatomyositis: a clinical and immunologic study. J Pediatr 1980;96:226-234.