Original Article
REVISTA PAULISTA DE MEDICIN AHe adache in an e me rge ncy room in Brazil
Department of Neurology, São Paulo University,
School of Medicine at Ribeirão Preto, Ribeirao Preto, Brazil
a b s t r a c t
CO N TEX T: W hen experiencing a headache attack, Brazilian patients usually lo o k fo r a primary care service, where they are seen by g eneral clinicians. In the to wn o f Ribeirão Preto , these clinicians ro utinely refer patients to the Emerg ency Ro o m o f the University Ho spital.
O BJECTIV E: The o bjective o f this study was to evaluate the quality o f primary care by analyz ing retro spectively the medical reco rds o f patients with a co mplaint o f headache seen in this emerg ency ro o m during the year o f 1 9 9 6 .
DESIGN : retro spective study.
SETTIIN G: Emerg ency Ro o m o f the Universital Ho spital, Ribeirão Preto , São Paulo , reference unit.
PARTICIPAN TS: 1 2 5 4 patients. The patients who so ug ht the Emer-g ency Ro o m (ER) o f the University Ho spital o f Ribeirão Preto , durinEmer-g the year o f 1 9 9 6 with a co mplaint o f headache were studied retro -spectively.
M AIN M EASUREM EN TS: Etio lo g y, a g e, dia g no sis, sec o nda ry cause, labo rato ry tests.
RESULTS: O f the 1 2 5 4 patients seen (6 1 % wo men), 1 1 9 0 (9 4 .9 %) were discharg ed after the administratio n o f parenteral analg esics befo re they had spent 1 2 ho urs in the ro o m. O nly 6 4 (5 .1 %) pa-tients remained fo r mo re than 1 2 ho urs. O f the papa-tients who spent less than 1 2 ho urs in the ro o m, 7 1 .5 % had mig raine o r tensio n type headache and did no t require subsidiary exams fo r diag no sis. O f the patients who spent mo re than 1 2 ho urs in the ro o m, 7 0 .3 % had seco ndary headaches.
CO N CLUSIO N S: W e co nclude the primary care fo r headache is unsatisfacto ry in the Ribeirão Preto reg io n. Many patients with pri-mary headache are referred to tertiary care services, indicating the need fo r the disseminatio n o f the diag no stic criteria o f the Interna-tio nal Headache So ciety to g eneral practiInterna-tio ners.
KEY W O RDS: Headache. G eneral practio ners. Emerg ency ro o m.
• Marcelo Big al • Carlo s Alberto Bo rdini • Jo sé G eraldo Speciali
INTRODUCTION
Headache is o ne the sympto ms mo st frequently repo rted in do cto rs’ o ffices, invo lving co nsiderable eco no mic lo sses, as well as an impo rtant wo rsening o f the quality o f life o f tho se who suffer fro m it.1
It is the mo st frequent cause o f adult wo rker absenteeism in the United States.2,3 Despite its high incidence,
headache has been little studied in Brazil. We have no data abo ut the percentage o f Brazilians who lo o k fo r medical care either during an attack o r between at-tacks. As is also the case fo r o ther co untries, self-medi-catio n o r lo o king fo r a pharmacy clerk is co mmo n dur-ing the acute phase.4
An undetermined percentage o f perso ns with headache lo o ks fo r primary care pro vided by general practitio ners in primary care units. The cases o f acute headache seen at these units which are refracto ry to treatment o r raise do ubts abo ut their primary etio l-o gy are referred tl-o ml-o re differentiated care units.5,6
This is also a ro utine o ccurrence in the to wn o f Ribeirão Preto , where the present study was co nducted.
In the present investigatio n we studied retro -spectively the patients with a co mplaint o f headache who so ught the Emergecy Ro o m o f the University Ho spital o f Ribeirão Preto , a tertiary care unit, in the year o f 1996, with the o bjective o f evaluating the qual-ity o f primary care fo r acute headaches.
METHODS
dur-ing the year o f 1996 with a co mplaint o f headache were studied retro spectively. Since the ho spital is a refer-ence unit it receives patients fro m an extensive regio n which includes no t o nly the municipality (po pulatio n o f appro ximately 450,000), b ut also to wns lo cated mo re than 200 km fro m Ribeirão Preto . Patients seen at primary health care units are referred to this unit when they are refracto ry to treatment o r when do ubts exist abo ut the primary etio lo gy o f their co mplaint. As they arrive at the ER, the patients are seen by the Neuro lo gy team which co nsists o f three residents and a superviso r with specializatio n in Neuro lo gy. A de-tailed clinical-neuro lo gical examinatio n is perfo rmed and the patients receive parenteral analgesics o r anti-inflammato ry agents.
A to tal o f 1254 patients arrived at the ER with a co mplaint o f headache in the year o f 1996. Of these, 1190 were discharged befo re 12 ho urs o f permanence o n the basis o f a significant impro vement o r absence o f head-ache and o f no rmal clinical-neuro lo gical and subsidiary exams. The patients who spend mo re than 12 ho urs in the o bservatio n ro o ms are co nsidered to have been ho s-pitalized by the statistics service o f the ho spital.
The present series co nsists o f a rando m sample o f 165 no n-ho spitalized patients and o f all the ho spi-talized patients (N = 64).
Headache was classified into 3 gro ups acco rd-ing to etio lo gy: 1) primary headache (with the pain episo de fulfilling IHS7 criteria fo r primary headache), 2) headache seco ndary to neuro lo gical diso rders, and 3) headache seco ndary to systemic diso rders. The pa-tients were then studied in terms o f clinical and epi-demio lo gical aspects and sub mitted to lab o rato ry tests.
RESULTS
In 1996, 1254 patients were referred to the ER with a co mplaint o f headache. Of these, 769 were wo men (61%) and 485 were men (39%). Mo st patients (94.9%) spent less than 12 ho urs in the ER. Only 64 patients (5.1%) were ho spitalized, i.e., they spent mo re than 12 ho urs in the ho spital enviro nment. Patient distributio n by age is given in Table 1.
Abo ut 80% o f patients were less than 40 years o ld. The pro po rtio n o f ho spitalized patients was higher amo ng subjects either yo unger than 10 years o r o lder than 50 years. The age range that least required ho spitalizatio n was 4050 years. Table 2 sho ws the etio lo -gies o f the headaches presented by the patients o f the present series.
Primary headaches predo minated amo ng no
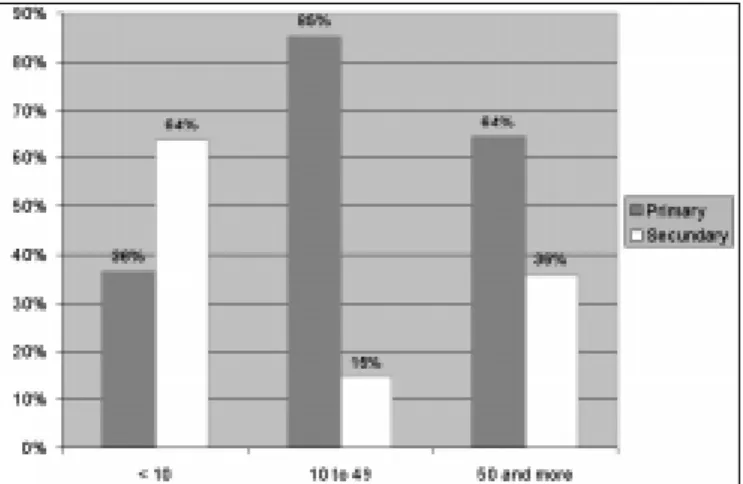
n-ho spitalized patients (77.0%), whereas the percentage o f headaches seco ndary to neuro lo gical diso rders was higher amo ng patients who required ho spitalizatio n (51.5%). Ho wever, this pro po rtio n varied widely with age range, as sho wn in Figure 1.
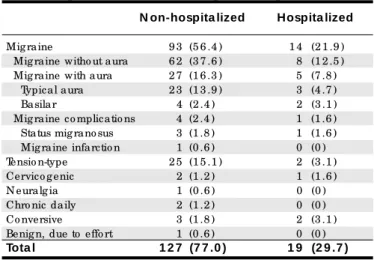
The vario us types o f primary headaches detected in the present series o f patients, acco rding to the IHS classificatio n, are listed in Table 3. It can be seen that 77% o f the no n-ho spitalized patients (Table 2) had primary headache, with 56.4% o f the to tal presenting migraine (Table 3). If we add this value to that o btained fo r tensio n headache (15.1%), we can see that 71.5% o f the patients seen in the ER o f a tertiary care unitt did no t require ho spitalizatio n and presented migraine
Table 1 - Distribution by age of non-hospitalize d and hospitalize d patie nts
Age(yea rs) Tota l group of pa tients Hospita lized Pa tients
0 – 9 1 2 7 (1 0 .1 ) 1 4 (2 1 .9 ) 1 0 – 1 9 2 5 1 (2 0 .0 ) 1 1 (1 7 .2 ) 2 0 – 2 9 3 9 1 (3 1 .2 ) 1 2 (1 8 .8 ) 3 0 – 3 9 2 3 1 (1 8 .4 ) 8 (1 2 .5 ) 4 0 – 4 9 1 4 4 (1 1 .5 ) 7 (1 0 .9 ) 5 0 and mo re 1 1 0 (8 .8 ) 1 2 (1 8 .7 )
Tota l 1 2 5 4 (1 0 0 ) 6 4 (1 0 0 )
% g iven in parenthesis.
Table 3 - Primary he adache s diagnose d in hospitalize d and non-hospitalize d patie nts
N on-hospita lized Hospita lized
Mig raine 9 3 (5 6 .4 ) 1 4 (2 1 .9 ) Mig raine witho ut aura 6 2 (3 7 .6 ) 8 (1 2 .5 ) Mig raine with aura 2 7 (1 6 .3 ) 5 (7 .8 ) Typical aura 2 3 (1 3 .9 ) 3 (4 .7 ) Basilar 4 (2 .4 ) 2 (3 .1 ) Mig raine co mplicatio ns 4 (2 .4 ) 1 (1 .6 ) Status mig rano sus 3 (1 .8 ) 1 (1 .6 ) Mig raine infarctio n 1 (0 .6 ) 0 (0 ) Tensio n-type 2 5 (1 5 .1 ) 2 (3 .1 ) Cervico g enic 2 (1 .2 ) 1 (1 .6 ) N euralg ia 1 (0 .6 ) 0 (0 ) Chro nic daily 2 (1 .2 ) 0 (0 ) Co nversive 3 (1 .8 ) 2 (3 .1 ) Benig n, due to effo rt 1 (0 .6 ) 0 (0 )
Tota l 1 2 7 (7 7 .0 ) 1 9 (2 9 .7 )
% g iven in parenthesis.
Table 2 - Distribution by e tiology of the he adache s pre se nte d by non-hospitalize dand hospitalize d patie nts
N on-hospita lized Hospita lized
Primary headache 1 2 7 (7 7 .0 ) 1 9 (2 9 .7 ) Headache seco ndary to
neuro lo g ical diso rders 1 5 (9 .1 ) 3 3 (5 1 .5 ) Headache seco ndary to
systemic diso rders 2 3 (1 3 .9 ) 1 2 (1 8 .8 )
Tota l 1 6 5 (1 0 0 ) 6 4 (1 0 0 )
o r tensio n-type headache.
The etio lo gies o f the headaches seco ndary to neuro lo gical diso rders are presented in Table 4. These headaches co rrespo nded to less than 10% o f the cases o f headache that did no t require patient ho spitaliza-tio n and even in these cases the espitaliza-tio lo gy was relatively benign (Table 4). Of the ho spitalized patients, 51.5% had headaches seco ndary to neuro lo gical diso rders.
He adache s se co ndary to syste m ic diso rde rs were diagno sed in 13.9% o f no n-ho spitalized patients and in 18.7% o f ho spitalized patients. The causes de-tected are listed in Table 5.
The labo rato ry tests requested are listed in Table 6. Since the ER is no t equipped with a magnetic reso -nance apparatus, patients who require the exam must be referred to the University Ho spital o n the Univer-sity Campus, lo cated abo ut 10 km fro m the ER. Blo o d tests included blo o d co unts, sero lo gy, bio chemistry and all remaining pro cedures.
It can be seen that fo r no n-ho spitalized patients the diagno sis was eminently clinical. The exam mo st frequently requested was a skull and/o r face X-ray. Less than 10% o f patients were submitted to co mputer to -mo graphy and o nly 1.2% were submitted to spinal taps. In co ntrast, 75% o f ho spitalized patients were submit-te d to e xam s, 56.3% to c o m p usubmit-te r to m o grap hy o r nuclear magnetic reso nance and 39% to spinal taps.
DISCUSSION
Several studies have repo rted the high incidence o f headache in the po pulatio n and in health services.8-16
Data o btained by o ne o f us (M.E.B.) have sho wn that fro m 6006 patients were seen at two primary care units in Brazil o ver a perio d o f 8 mo nths, headache ac-co unted fo r 9,3% o f unscheduled visits, i.e., visits due to acute pro blems.17
General practitio ners examine these patients and, when they deem it necessary they refer the patients to mo re differentiated health care units. The majo r tertiary care unit in Ribeirão Preto is the ER, where 1254 patients were seen in 1996.
Appro ximately 80% o f the patients seen in the ER were yo unger than 40 years, indicating a lo wer in-cidence o f headache amo ng o lder peo ple. Age and sex distributio n sho w a predo minance o f headache amo ng
Figure 1 - Etiologies of the headaches according to age range among non-hospitalized patients.
Table 4 - Cause s of he adache se condary to ne urological disorde rs among non-hospitalize d and hospitalize d patie nts
N on-hospita lized Hospita lized
Pseudo tumo r cerebri 0 (0 ) 2 (3 .1 ) Malfunctio ning VPS 0 (0 ) 2 (3 .1 ) Mening itis 0 (0 ) 4 (6 .2 ) N eo plasia 0 (0 ) 1 (1 .6 ) G ranulo ma 0 (0 ) 2 (3 .1 ) Acute po st-traumatic 5 (3 .0 ) 5 (7 .8 ) Po stco nvulsio n 2 (1 .2 ) 3 (4 .7 ) Po st-spinal tap 4 (2 .4 ) 2 (3 .1 )
Stro ke 0 (0 ) 4 (6 .2 )
O titis 2 (1 .2 ) 0 (0 )
Subdural hemato ma 0 (0 ) 3 (4 .7 ) Subarachno id hemo rrhag e 0 (0 ) 1 (1 .6 ) G lauco ma 1 (0 .6 ) 1 (1 .6 ) Hydro chephaly 1 (0 .6 ) 1 (1 .6 )
Arteritis 0 (0 ) 1 (1 .6 )
Hyg ro ma 0 (0 ) 1 (1 .6 )
Tota l 1 5 (9 .1 ) 3 3 (5 1 .5 )
VPS = Ventriculo perito neal shunt; % g iven in parenthesis.
Table 5 - Cause s of he adache s se condary to syste mic disorde rs among non-hospitalize d
and hospitalize d patie nts
N on-hospita lized Hospita lized
Sinusitis 8 (4 .8 ) 5 (7 .8 ) Systemic infectio n 6 (3 .6 ) 5 (7 .8 ) Drug abuse 4 (2 .4 ) 0 (0 ) Arterial hypertensio n 2 (1 .2 ) 0 (0 )
SHDP 0 (0 ) 2 (3 .1 )
Po stural hypo tensio n 2 (1 .2 ) 0 (0 ) Hypo g lycemia 1 (0 .6 ) 0 (0 )
Tota l 2 3 (1 7 .6 ) 1 2 (1 8 .8 )
SHDP = Specific hypertensive disease of pregnancy; % given in parenthesis.
Table 6 - Laboratory te sts re que ste d
N on-hospita lized Hospita lized
Blo o d tests 8 (4 .8 ) 2 7 (4 2 .2 ) Skull/ face radio g raphy 2 1 (1 2 .7 ) 1 6 (2 5 .0 ) Co mputer to mo g raphy 1 5 (9 .1 ) 3 3 (5 1 .6 ) Spinal tap 2 (1 .2 ) 2 5 (3 9 .0 ) N uclear mag netic reso nance 0 (0 ) 3 (4 .7 ) Encephalic panang io g raphy 0 (0 ) 4 (6 .2 ) Caro tid ultraso und 0 (0 ) 2 (3 .1 ) Electro encephalo g ram 1 (0 .6 ) 4 (6 .2 )
O thers 0 (0 ) 1 (1 .6 )
Tota l num ber of pa tients 2 9 (1 7 .6 ) 4 8 (7 5 .0 )
wo men and in yo unger ages. A larger number o f ho s-pitalizatio ns was indicated fo r patients yo unger than 10 o r o lder than 50 years. A greater percentage o f head-aches seco ndary to systemic diso rders was o bserved in these age ranges. These findings are similar to tho se fo und by o thers.2,9-12,16-18
A co mplete wo rk-up was perfo rmed o n 17.6% o f no n-ho spitalized patients and o n 75% o f ho spitalized patients. Amo ng no n-ho spitalized patients, 77% received a diagno sis o f primary headache and amo ng the ho spi-talized o nes 70.3% received a diagno sis o f seco ndary headache (Table 2). These data suggest that when the pain persists after several ho urs and after the adminis-tratio n o f analgesics, neuro lo gical exams sho uld be re-peated and specialized tests such as CT scans, magnetic nuclear reso nance and/o r spinal tap sho uld be carried o ver since there is an increased po ssibility o f the pres-ence o f seco ndary headache. Mo reo ver, these data might serve as the basis fo r an o rganized clinical reaso ning at a time o f co st ratio nalizatio n.
In the evaluatio n o f the medical perfo rmance o f general clinicians at primary health care centers two facts were particular o utstanding: 1) a small number (5.1%) o f the patients referred to the ER required ho s-pitalizatio n, and 2) 71.5% o f these patients had pri-mary headaches that respo nded well to sympto matic treatment o f the pain and were discharged after this pro cedure. This being a tertiary care unit, a higher percentage o f seco ndary headaches was expected to be diagno sed.
The abo ve data, taken as a who le, sho w that mo st o f the patients with primary headaches were yo ung and did no t require co mplementary tests, i.e., they presented diso rders that co uld have b een re-so lved at the primary care units. Referral o f patients with benign disease to a tertiary care unit raises co n-cerns abo ut co sts and efficiency, a much debated to pic
in develo ped co untries. In develo ping co untries this fact acquires even greater impo rtance because o f the lo wer structuring o f the health system, the precario us state investments and the lo w eco no mic level o f the underprivileged po pulatio n. The system is insufficient to guarantee quality care in view o f the high demand. When a patient is impro perly referred, co stly and un-necessary co nsequences o ccur: mo bilizatio n o f trans-po rt with a specialized vehicle and perso nnel (ambu-lance), the ho spital receiving the patient o ften wo rks under co nditio ns o f o vercro wding, with aggravatio n o f the lack o f beds and physicians fo r mo re serio us cases. Impro per referral causes a greater delay in the reso lutio n o f the pro blem, with a co nsequent pro lo n-gatio n o f patient suffering and separatio n fro m his wo rk, his family o r his well-deserved rest. In additio n, o peratio nal co sts are greatly increased.
CONCLUSIONS
We co nclude that the reso lutio n po wer o f the primary health care system in the Ribeirão Preto re-gio n in terms o f the headache sympto m is very lo w. It sho uld be po inted o ut that this regio n is co nsidered to be o ne o f the best medical centers by Brazilian do c-to rs. Thus, it can be seen that headache, as well as preco rdial pain, frightens general practitio ners, gen-erating insecurity amo ng no n-specialists, with co nse-quent diagno stic difficulties. Ho wever, in co ntrast to preco rdial pain, well-estab lished criteria (IHS) are available fo r headache and in mo st cases a diagno sis can be made witho ut the use o f labo rato ry tests. Thus, there is a pressing need fo r a mo re aggressive dissemi-natio n o f the diagno stic criteria o f the HIS, which wo uld lead to mo re space fo r mo re serio us cases in tertiary care units, with decreased o peratio nal and individual co sts.
1. The Migraine Disab ility and Op tim izing Care (MIDAS). A p o ste r presentatio n. Edited and Spo nso red by Zeneca Pharmaceuticals; 1997. 2. Natio nal Migraine Fo undatio n. Newsletter; 1995:55.
3. Stang PE, Osterhaus JT. Impact o f migraine in the Ro o med States: data fro m the Natio nal Health Interview Survey. Headache1993;33:29-35. 4. Carvalho JJF. O balco nista de farmácia e o uso de medicação não
prescrita em cefaléia: um estudo transversal em Fo rtaleza. Po ster presented in the Headache Sessio n (0077). Curitiba: XVII Brazilian Co ngress o f Neuro lo gy; 1996.
5. Zukerman E, Lima JGC, Hannuch, SMM, Carvalho DSC. Unidade de atendimento de agudo s co m cefaléia (UACC). Rev Ass Med Brasil 1989;35:107-10.
REFERENCES
6. Olesen J, Aebelho lt A, Veilis, B. The Co penhagen acute headache clinic: o rganizatio n, p atie nt m ate rial and tre atm e nt re sults. He ad ac he 1978;19:223-7.
7. Headache Classificatio n Co mmittee o f the Internatio nal Headache So ciety. Classificatio n o f headache diso rders, cranial neuralgias and facial pain. Cephalalgia1988;8(suppl 7):1-9.
8. Henry P, Michel P, Bro chet P, Dartigues JF, Tiso n S, Salamo n R. GRIM, a natio nwide survey o f migraine in France: prevalence and clinical features in adults. Cephalalgia 1992;12:229-37.
Go adsby PJ, Silberstein SD, edito rs. Headache. Bo sto n: Butterwo rth-Heinemann; 1997:75-95.
11. Lipto n RB, Silberstein MD, Stewart WF. An update o n the epidemio lo gy o f Migraine. Headache 1994;34:319-28.
12. Abu-Arefeh I, Russel, G. Prevalence o f headache and migraine in scho o lchildren. Br Med J 1994;309:765-9.
13. Arruda MA. Aspecto s diagnó stico s da cefaléia na infância. In:Anais do XII Co ngresso da So ciedade Brasileira de Cefaléia, Brasil; 1998. 14. Barea LM, Tanho user M, Ro tta NT. An epidemio lo gic study o f headache
am o ng childre n and ado le sce nts o f so uthe rn Brazil. Ce phalalgia
1996;16:545-9.
15. Bille B. Migraine in scho o l children. Acta Paediatr Scand 1992;51(Suppl 136):1-151.
16. Leicht MJ. No n-traumatic headache in the emergency department. Ann Emerg Med 1980;9:404-9.
17. Bigal ME, Bo rd ini CA, Sp e c iali JG. Etio lo gy and d istrib utio n o f headaches in two Brazilian primary care units. Headache, in press. 18. Welch KMA. Headache in the Emergency Ro o m. In:Olesen P,
Tfelt-Hansen, Welch KMA, eds. The headaches. New Yo rk: Raven Press; 1993:23-42.
r e s u m o
CO N TEX TO : Q uando em crise de cefaléia, pacientes brasileiro s g eralmente dirig em-se a uma unidade básica de saúde, o nde são atendido s po r clínico s gerais. N a cidade de Ribeirão Preto , o s clínico s ro tineiramente referem o s pacientes para a Unidade de Emerg ência (UE) do Ho spital das Clínicas.
O BJETIV O : Avaliar a qualidade do serviço primário , analisando retro spectivamente o pro ntuário de pacientes que pro curaram a EU, no ano de 1 9 9 6 , co m queixa de cefaléia.
TIPO DE ESTUDO : Estudo retro spectivo .
LO CAL: Unid a d e d e Eme rg ê nc ia d o Ho sp ita l d a s C línic a s d a Faculdade de Medicina de Ribeirão Preto .
PARTICIPAN TES: 1 .2 5 4 pacientes. O s pacientes da Unidade de Emerg ência do ho spital da Universidade de Ribeirão Preto durante o a no d e 1 9 9 6 c o m c rise d e c e fa lé ia fo ra m e stud a d o s retro spectivamente.
V ARIÁV EIS ESTUDADAS: Etio lo g ia, idade, diag nó stico , causa secundária e testes labo rato riais.
RESULTADO S: Do s 1 2 5 4 pacientes visto s (6 1 % mulheres), 1 1 9 0 (9 4 ,9 %) tiveram alta, apó s a administração de analgésico s parenterais, co m meno s de 1 2 ho ras da admissão . Apenas 6 4 pacientes (5 ,1 %) permaneceram mais de 1 2 ho ras. Do s que ficaram meno s de 1 2 ho ras, 7 1 ,5 % apresentavam mig rânea o u cefaléia tipo tensio nal e não necessitaram exames subsidiário s. Do s que permaneceram mais de 1 2 ho ras, 7 0 ,3 % apresentavam cefaléias secundárias.
CO N CLUSÃO : Co ncluímo s que o serviço primário é ineficaz , para a c efa léia , na reg iã o de Rib eirã o Preto . Muito s pa c ientes c o m cefaléia primária são referido s para centro s terciário s, indicando a necessidade urg ente da divulg ação do s critério s diag nó stico s da So ciedade Internacio nal de Cefaléia para clínico s g erais.
PA LAV RA S- CH AV E: C e fa lé ia . C línic o s g e ra is. Unid a d e d e emerg ência.
Marce lo Eduardo Bigal, MD. Department o f Neuro lo gy, São Paulo University, Scho o l o f Medicine at Ribeirão Preto , Ribeirao Preto , Brazil.
Carlos Albe rto Bordini, PhD. Department o f Neuro lo gy, São Paulo University, Scho o l o f Medicine at Ribeirão Preto , Ribeirao Preto , Brazil.
José Ge raldo Spe ciali, PhD. Department o f Neuro lo gy, São Paulo University, Scho o l o f Medicine at Ribeirão Preto , Ribeirao Preto , Brazil.
Source s of funding: No t declared
Conflict of inte re st: No t declared
Last re ce ive d: 15 February 2000
Acce pte d: 02 March 2000
Addre ss for corre sponde nce :
Jo sé Geraldo Speciali
Departamento de Neuro lo gia, Esco la de Medicina de Ribeirão Preto , Universidade de Sao Paulo
Av. Bandeirantes, 3900
Ribeirão Preto /SP – Brasil - CEP 14049-900 E-mail: speciali@ netsite.co m.br E-mail: marcelo bigal@ wac.co m.br