LONG-TERM OUTCOMES OF SYMPTOMATIC
ELECTRODIAGNOSED CARPAL TUNNEL SYNDROME
Joao Aris Kouyoumdjian
1, Maria P.A. Morita
2, Amalia F.P. Molina
3,
Dirce M.T. Zanetta
4, Adriana K. Sato
3, Carlos E.D. Rocha
6, Claudia C. Fasanella
6ABSTRACT - This study was done to evaluate the long-term patient’s satisfaction after carpal tunnel syndrome (CTS) electrodiagnostic done between 1989 and 1994 (5 to 10 years follow-up). Mail contact was made to 528 consecutive cases with a questionnaire to be filled; 165 patients responded after 19 exclusions. CTS severity was graded from 0 (incipient) to 4 (severe) after a combination of median sensory distal latency, sensory median-radial latency difference and amplitude of the median compound muscle action potential. Current symptoms (“cure”, improved, unchanged or worsed) and the therapy utilized, either surgical or conservative, were analyzed to the initial CTS severity, age and duration of symptomatology. Surgical release was done in 114 cases (69%). Patient’s satisfaction after surgical and non-surgical were respectively, 77.6% and 16% (“cure”), 13.6% and 52% (much improved), 5.4% and 9.3% (little improved), 2.7% and 16% (unchanged), 0.7% and 6.7% (worsed). The frequency of “cure” versus unchanged/worsed or “cure”/much improved versus unchanged/worsed was highly significative (Fisher, P-value < 0.001) and was not influenced by the CTS electrophysiological severity. There was no relationship between the outcome after surgery and duration of symptomatology, age or CTS severity. Conservative benefice was more prevalent in those with shorter symptomatology and older age; the majority of conservative failure cases had mild initial CTS. We concluded the excellent surgical benefice described by patients and the absence of any predictive factors based on CTS severity, age or duration of symptomatology for outcome.
KEY WORDS: carpal tunnel syndrome, median nerve, compression neuropathy, electrodiagnosis, nerve conduction.
Síndrome do túnel do carpo: avaliação evolutiva de longo prazo após confirmação eletrodiagnóstica Síndrome do túnel do carpo: avaliação evolutiva de longo prazo após confirmação eletrodiagnósticaSíndrome do túnel do carpo: avaliação evolutiva de longo prazo após confirmação eletrodiagnóstica Síndrome do túnel do carpo: avaliação evolutiva de longo prazo após confirmação eletrodiagnóstica Síndrome do túnel do carpo: avaliação evolutiva de longo prazo após confirmação eletrodiagnóstica
RESUMO - O presente estudo tem por objetivo avaliar a terapia utilizada e o grau de satisfação dos pacientes que tiveram diagnóstico eletrofisiológico de síndrome do túnel do carpo (STC) entre 1989 e 1994 (528 casos); foram respondidas 184 cartas entre 528 enviadas (34,8%) sendo utilizadas 165. A gravidade do STC foi classificada de 0 a 4 de acordo com uma combinação de valores de latência distal sensitiva e amplitude do potencial de ação muscular composto do nervo mediano e diferença de latência sensitiva mediano/radial. As questões foram relativas a sintomatologia atual e terapêutica utilizada, cirúrgica ou conservadora. As respostas foram correlacionadas ao estudo de condução nervosa inicial, idade e tempo de sintomatologia. Os pacientes submetidos a cirurgia somaram 69% (114 casos). O benefício cirúrgico e não cirúrgico foi respectivamente de 77,6% e 16% (“cura”); 13,6% e 52% (melhora acentuada); 5,4% e 9,3% (melhora leve); 2,7% e 16% (inalterado); 0,7% e 6,7% (piora). A freqüência de “cura” versus inalterado/pior ou “cura”/melhora acentuada versus igual/ pior foi significativa, maior no grupo cirúrgico (teste de Fisher, valor de P < 0,001), e não foi influenciada pelo padrão eletrofisiológico inicial. Não houve relação entre melhora ou piora após cirurgia e tempo de sintomatologia, idade ou gravidade eletrofisiológica iniciais. Os casos com melhora sem cirurgia tiveram menor tempo de sintomatologia e idade mais avançada. Os casos sem melhora após tratamento conservador apresentavam padrão eletrofisiológico leve em sua maioria. Conclui-se o excelente benefício cirúrgico para STC e a ausência de fatores preditivos definidos baseados na gravidade eletrofisiológica, idade e tempo de sintomatologia iniciais.
PALAVRAS-CHAVE: síndrome do túnel do carpo, nervo mediano, neuropatia compressiva, eletroneuromiografia, condução nervosa.
Electromyography Laboratory, Clinical Neurophysiology, Department of Neurological Sciences, State Medical School, São Jose do Rio Preto SP, Brazil: 1Associate-Professor (MD, PhD); 2Assistent-Professor (MD, MSc); 3Postgraduate student (MD, Department of Epidemiology
and Social Medicine; 4Associate-Professor (MD, PhD); 6Resident (MD).
Received 16 July 2002, received in final form 10 October 2002. Accepted 30 October 2002.
Carpal tunnel syndrome (CTS) is the most com-mon entrapment neuropathy in the upper limbs1,21,21,21,21,2.
Prospective population-based studies have shown that the prevalence of electrophysiologically confir-med CTS in the Netherlands in 1985 was 5.8% in women and 0.6% in men33333; in another survey
perfor-med in southern Sweden in 199944444, the authors found
a 2.7% prevalence of symptomatic subjects with cli-nically and electrophysiologically confirmed CTS.
Early diagnosis and treatment are important be-cause delay can result in irreversible median nerve damage with persistent symptoms and permanent disability11111.Non-surgical treatment includes: 1.
avoi-ding the activity precipitating the condition; 2. splin-ting the wrist; 3. local steroid injection; 4. short cour-se of either oral steroids or nonsteroidal anti-inflam-matory drugs; 5. trial of diuretics especially when the symptoms are perimenstrual11111. The surgical
treat-ment of median nerve compression in carpal tunnel, first described in the 1940s (cited by Nancollas et al.55555) is one of the most common and widely accepted
surgical procedure and the only approach that can offer the possibility of a definitive cure6,76,76,76,76,7.
Electro-diagnosis is very sensitive and specific for the diag-nosis and several studies have reported sensitivity in the range of 80 to 92%88888 and most physicians rely on
this method for clinical suspicion confirmation. The present study was carried out in order to ana-lyze through mail response, patient’s satisfaction af-ter 5 to 10 years follow-up of CTS electrodiagnosed.
METHOD 1. Patients
From September to November 1999, 528 letters were sent, corresponding to 1989-1994 consecutive CTS electro-diagnosed patients by reviewing a computer database of the Electromyography Laboratory (EMG Lab), State Medical School, Sao Jose do Rio Preto, Sao Paulo, Brazil. All patients had a clinically confirmed diagnosis of CTS, including hand paraesthesia, numbness, and pain mainly at night; isolated pain was not considered. All patients had bilateral nerve conduction studies (upper limbs, sensory and motor) in-cluding at least median and ulnar ones. Age, gender and duration of symptoms were obtained from the patient’s notes in the EMG Lab.
2. Electrophysiology (nerve conduction studies) All patients had bilateral nerve conduction studies using either ATI 9000 (ATI, São Paulo, Brasil) or Cantata (Dantec, Skovlunde, Denmark) eletromyography machine. Palmar temperatures were maintained above 31°C (digital ther-mometer, Braile Biomedica, Sao Jose do Rio Preto, SP, Bra-sil). Electrophysiological techniques are described as fol-lows; sensory latencies were measured to the onset.
1- Median distal sensory latency (routine). The stimulation delivered on median nerve at wrist activate antidromic sensory action potentials at the second digit; we used a fixed 14 cm distance from the ring recording electrodes that were placed around the proximal (recording, cathode) and distal (reference, anode) interphalangeal joints. The absolute latency value was defined as abnormal when equal or greater than 3.0 ms (46.6 m/s)99999. Prolongation of
the distal sensory latency or absence of the sensory nerve action potential in CTS has been reported in 53% to 98% of cases77777.
2 - Median motor distal latency (MDL). Median nerve stimulation was delivered at wrist in order to activate the compound muscular action potential (CMAP) at the thenar eminence; we used a fixed 8 cm distance from the disc recording electrodes that were placed over the belly of the Abductor Pollicis Brevis (APB) muscle (recording, ca-thode) and just distal to the metacarpophalangeal joint (reference, anode). The absolute latency value was defined as abnormal when equal or greater than 4.25 ms99999 and
amplitude of the CMAP less than 4.0 mV. Prolonged MDL to the APB in other series of CTS vary from 29% to 81%1010101010.
3 - Sensory median-radial difference (MR). Median nerve stimulation was delivered at wrist in order to activate antidromic sensory action potentials at the thumb; we used an approximately 10 cm distance from the ring recording electrodes around the thumb. Radial nerve stimulation was delivered at the lateral edge of the radius in the distal forearm at the same line used for median nerve stimula-tion; the recording ring electrodes around the thumb were the same. The latency difference was defined as abnormal when equal or greater than 0.40 ms1111111111. Prolongation of
MR in CTS has been reported in 58% to 100% of cases1010101010.
Percutaneous stimuli were delivered until supramaximal response obtained; pulse duration were 0.05/0.1 ms for sensory nerve stimulation and 0.2/0.5 ms for motor nerve stimulation; filters were set at 20 Hz and 2 kHz; the sweep speed was set at 1 ms per division; one-centimeter disc recording, either platinum or disposable electrodes, were used for motor and ring electrodes for sensory nerve stu-dies; either disposable or Velcro around the forearm were used as ground.
3. Questionnaire
A questionnaire was sent to each patient including a pre-paid returned envelope with the following questions: 1. How are the symptoms now (complete relief “cure”, improved “much better”, improved “little”, unchanged, or worsed). 2. What kind of treatment was done (surgical or conservative, either by splinting the wrist, local steroid injection, use of drugs medicines or others). 3. Surgeon specialty. 4. Date and side of carpal release.
RESULTS
Of the 528 cases in the initial sample, 184 letters (34.8%) were returned with a complete question-naire done, 123 (23.3%) were returned without res-ponse (address do not matched) and the remaining 221 (41.9%) with no response at all; 89.4% was fe-male (472 cases) and 10.6% fe-male (56 cases). A total of 19 patients were excluded after incorrect res-ponses, death, carpal release before electro-physiological evaluation and evidence of polyneu-ropathy based on conduction abnormalities in nerves other than the median. The records of the remaining 165 patients, 158 female (95.8%) and 7 male (4.2%), were retained for final analysis and form the basis of this study. Surgery release was done in 114/165 pa-tients (69.1%) corresponding to 147/222 hands (66.2%). Non-surgical procedures were done in 51/ 165 patients (30.9%) corresponding to 75 hands (33.8%). Correct medical specialty was obtained in 109 from 114 surgical cases corresponding to 48.7% ortho-paedic surgery, 22% neurosurgery, 17.4% vascular surgery, 11% plastic surgery and 0.9% general surgery.
General patient’s satisfaction
Patient satisfaction after surgery: complete relief “cure” in 114 hands (77.6%), improved “much bet-ter” in 20 hands (13.6%), improved “little” in 8 hands (5.4%), unchanged in 4 hands (2.7%) and worsed in 1 hand (0.7%). The mean period between surgery and questionnaire response (follow-up) was 70
mon-ths for complete relief “cure” group and 72 monmon-ths for unchanged/worsed group. Patient satisfaction after non-surgical procedures: complete relief “cure” in 12 hands (16%), improved “much better” in 39 hands (52%), improved “little” in 7 hands (9.3%), unchanged in 12 hands (16%) and worsed in 5 hands (6.7%). A comparison between surgical and non-sur-gical cases in the complete relief “cure” group (114 versus 12 hands or 77.6% versus 16%) and un-changed/worsed groups (5 versus 17 hands) revealed P < 0.001, Fisher-test.
Age and patient’s satisfaction
The mean age of patients that underwent CTS released (surgical) in the complete relief “cure” group was 46 (24-70) years against 44 (39-58) years in the unchanged/worsed one. The mean age of patients that had non-surgical procedures in the complete relief “cure” group was 61 (48-79) years against 50 (30-83) years in the unchanged/worsed one.
Duration of symptomatology and patient’s satisfaction
The mean duration of symptomatology of pa-tients that underwent CTS released (surgical) in the complete relief “cure” group was 43 (1-120) months against 50 (1-120) months in the unchanged/worsed one. The mean duration of symptomatology of pa-tients that had non-surgical procedures in the com-plete relief “cure” group was 8 (1-48) months against 26 (1-120) months in the unchanged/worsed one.
Nerve conduction studies severity and patient’s satisfaction
The nerve conduction severity of patients that un-derwent CTS released (surgical) in the complete relief “cure” group (114 hands) was as follows: group 0 (7 hands, 6.1%), group 1 (74 hands, 64.9%), group 2 (17 hands, 14.9%), group 3 (9 hands, 7.9%) and
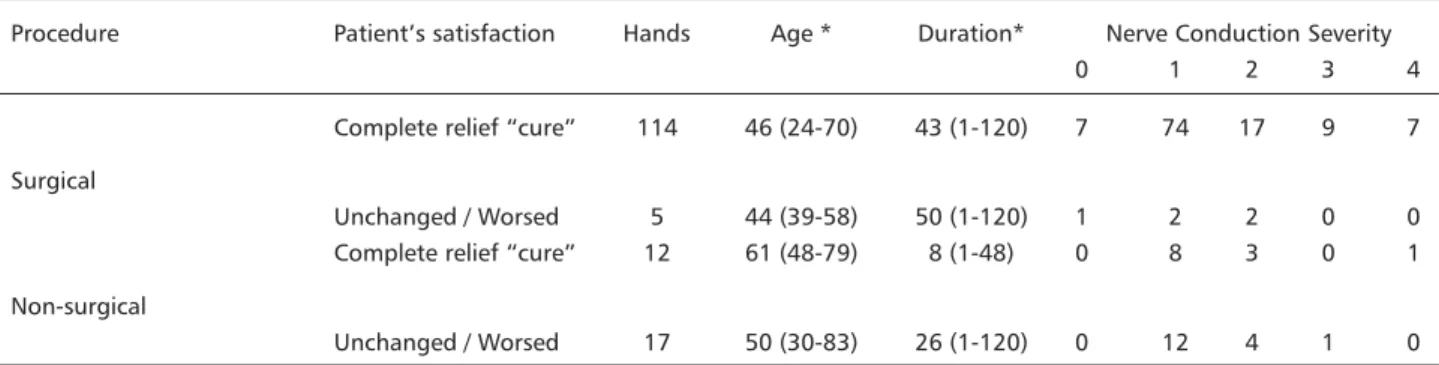
Table 1. Summary of the results of patient’s satisfaction after surgical and non-surgical CTS treatment.
Procedure Patient’s satisfaction Hands Age * Duration* Nerve Conduction Severity
0 1 2 3 4
Complete relief “cure” 114 46 (24-70) 43 (1-120) 7 74 17 9 7 Surgical
Unchanged / Worsed 5 44 (39-58) 50 (1-120) 1 2 2 0 0 Complete relief “cure” 12 61 (48-79) 8 (1-48) 0 8 3 0 1 Non-surgical
Unchanged / Worsed 17 50 (30-83) 26 (1-120) 0 12 4 1 0
group 4 (7 hands, 6.1%). On the other hand, the nerve conduction severity in the unchanged/worsed group (5 hands) after surgery was as follows: group 0 (1 hand), group 1 (2 hands), group 2 (2 hands), groups 3 and 4 (no hands).
The nerve conduction severity of patients that had non-surgical procedures in the complete relief “cure” group (12 hands) was as follows: group 0 (no hands), group 1 (8 hands, 66.6%), group 2 (3 hands, 25%), group 3 (no hands) and group 4 (1 hand, 8.3%). On the other hand, the nerve conduction severity in the unchanged/worsed group after non-surgical proce-dures (17 hands) was as follows: group 0 (no hands), group 1 (12 hands, 70.6%), group 2 (4 hands, 23.5%), group 3 (1 hand, 5.9%) and 4 (no hands). The main findings are summarized on Table 1.
DISCUSSION
Our results clearly showed the great surgical be-nefice in CTS treatment based on long-term patient’s satisfaction after confirmed electrodiagnosed cases when compared to non-surgical procedures, regardless surgery technique or surgeon specialty (P < 0.001, Fisher test, surgical versus non-surgical, complete relief “cure” versus unchanged/worsed). Non-surgical procedures either through medications or splints, avoiding activities precipitating the con-dition or many non-conventional referred ones like homeopathy, acupuncture or vitamins could not be measured ought to large variability on response or time of use. We could not find any relationship bet-ween the outcome after surgery and duration of sym-ptomatology, age or CTS electrodiagnostic severity prior to surgery. Conservative benefice was more pre-valent in those with shorter duration of sympto-matology and older age. The majority of conservative failure cases had mild initial CTS, pointing out the confusing attempt to predict results and benefices.
We used a similar model as did Cseuz et al.1212121212 in
1966 at Mayo Clinic. They described that the use of questionnaires to be answered and sent by mail for the interpretation of CTS recovery seemed admissible, since the manifestations of CTS are largely subjective and therefore best judged by the patient himself.
Our mean follow-up after CTS release was 71 months (5.9 years) comparable to the other series described by Cseuz et al. (3 years)1212121212, DeStefano et al.
(7.3 to 12 years)1313131313, Haupt et al. (5.5 years)1414141414, Nancollas
et al. (4.8 years)55555 and Thurston and Lam (18
months)1515151515. We found 91.2% complete relief “cure”
and improved “much better” (good results) after sur-gery, comparable to other series as Haupt et al. (86%)1414141414, Cseuz et al. (81%)1212121212, Thurston and Lam
(80%)1515151515, Nancollas et al. (87%)55555, Harris et al. (91.9%)1616161616
and DeStefano et al. (nearly 6 times more likely to have symptoms resolution)1313131313.
The duration of the symptoms had little bearing on the degree of recovery and those with poor results were clinically not different from those who had ob-tained good results from operation as also described by most series5,12,16,175,12,16,175,12,16,175,12,16,175,12,16,17. However, DeStefano et al.1313131313
found that duration of CTS was one of the strongest factors influencing the effectiveness of CTS surgery; nearly all surgical patients who had successful out-comes had resolution of their symptoms by 6-12 months after surgery.
Nerve conduction studies severity also failed as a factor determining prognosis and, even in severe ca-ses, subjective recovery could be found, as also described in others series5,12,145,12,145,12,145,12,145,12,14. It is possible that same
patients associate recovery with the disappearance of pain and paresthesia, and that mild residual sen-sory loss could be ignored by the patient and could explain the great benefice of surgery even in patients with severe electrodiagnosed CTS.1212121212 Mendelson and
Balla1818181818 describing a small series, showed a tendency
for patients with more severe symptoms to obtain better results from surgery.
Open carpal tunnel release remains a safe and reliable treatment of CTS15 15 15 15 15 and the relief of pain was
often dramatic1717171717. Nerve conduction improves with
surgical treatment and correlates to an improvement in symptoms1818181818. Patients with post-operative
norma-lization of electrodiagnostic findings invariably im-proved clinically as well1414141414. The results of the
elec-trodiagnostic testing was not predictive of duration of symptoms13,1913,1913,1913,1913,19.
The present study as others indicates that the long-term postoperative results are very gratifying and we concluded the excellent surgical benefice des-cribed by patients and the absence of any predictive factors based on CTS severity, age or duration of symptomatology for outcome.
REFERENCES
1. Dawson DM, Hallett M, Wilbourn AJ. Entrapment neuropathies. 3.Ed., Philadelphia: Lippincott-Raven; 1999.
2. Stewart JD. Focal peripheral neuropathies. 3.Ed., Philadelphia: Lippincott Willians & Wilkins; 2000.
3. de Krom MC, Knipschild PG, Kester AD, Thijs CT, Boekkooi PF, Spaans F. Carpal tunnel syndrome: prevalence in the general population. J Clin Epidemiol 1992;45:373-376.
4. Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosen I. Prevalence of carpal tunnel syndrome in a general population. JAMA 1999;282:153-158.
6. Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter for carpal tunnel syndrome (summary statement). Neurology 1993;43:2406-2409.
7. Stevens JC. American Association of Electrodiagnostic Medicine minimonograph #26: the electrodiagnosis of carpal tunnel syndrome. Muscle Nerve 1997;20:1477-1486.
8. Andary MT, Werner RA. Electrodiagnosis in clinical decision making: carpal tun-nel syndrome. 1997 AAEM Course B: Using electrodiagnosis in clinical decision making. AAEM 20th Annual Continuing Education Courses 1997, San Diego. 9. Kouyoumdjian JA. Síndrome do túnel do carpo: correlação da
compa-ração de latência sensitiva mediano-radial com condução nervosa roti-na em 1059 mãos (668 casos). Arq Neuropsiquiatr 1999;57:208-215. 10. Jablecki CK, Andary MT, So YT, Wilkins DE, Willians FH. Literature
review of the usefulness of nerve conduction studies and electro-myography for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve 1993;16:1392-1414.
11. Johnson EW, Sipski M, Lammertse T. Median and radial sensory latencies to digit I: normal values and usefulness in carpal tunnel syndrome. Arch Phys Med Rehabil 1987;68:140-141.
12. Cseuz KA, Thomas JE, Lambert EH, Love JG, Lipscomb PR. Long-term results of operation for carpal tunnel syndrome. Mayo Clin Proc 1966;41:232-241.
13. DeStefano F, Nordstrom DL, Vierkant RA. Long-term symptom outcomes of carpal tunnel syndrome and its treatment. J Hand Surg 1997;22:200-210. 14. Haupt WF, Wintzer G, Schop A, Löttgen J, Pawlik G. Long-term results of carpal tunnel decompression: assessment of 60 cases. J Hand Surg (Br) 1993;18:471-474.
15. Thurston A, Lam N. Results of open carpal tunnel release: a comprehensive, retrospective study of 188 hands. Aust N Z Surg 1997;67:283-288. 16. Harris CM, Tanner E, Goldstein MN, Pettee DS. The surgical treatment
of the carpal tunnel syndrome correlated with preoperative nerve conduction studies. J Bone Joint Surg Am 1979;61:A93-98.
17. Hybbinette C-H, Mannerfelt L. The carpal tunnel syndrome. A retrospective study of 400 operated patients. Acta Orthop Scand 1975;46:610-620. 18. Mendelson B, Balla J. Results of surgical treatment of the carpal tunnel
syndrome. Proc Aust Assoc Neurol 1973;9:129-132.