SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Evaluation
of
epidural
blockade
as
therapy
for
patients
with
sciatica
secondary
to
lumbar
disc
herniation
夽
Rogerio
Carlos
Sanfelice
Nunes
a,∗,
Elenir
Rose
Jardim
Cury
Pontes
b,
Izaias
Pereira
da
Costa
caUniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil
bUniversidadeFederaldeMatoGrossodoSul(UFMS),CentrodeCiênciasBiológicasedaSaúde,ProgramadePós-Graduac¸ãoemSaúdee
DesenvolvimentonaRegiãoCentro-Oeste,CampoGrande,MS,Brazil
cUniversidadeFederaldeMatoGrossodoSul(UFMS),FaculdadedeMedicina,DepartamentodeClínicaMédica,CampoGrande,MS,
Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5August2015 Accepted25September2015 Availableonline27June2016
Keywords:
Intervertebraldiscdisplacement Lumbarpain
Nerveblock
a
b
s
t
r
a
c
t
Objective:Sciaticpainsecondarytolumbardischerniationisacomplexconditionthatis oftenhighlylimiting.Thecausesofpainindischerniationaremultifactorial.Two physio-pathologicalmechanismsareinvolvedindiscogenicpain:mechanicaldeformationofnerve rootsandabiochemicalinflammatorycomponentresultingfromcontactbetweenthe inter-vertebraldiscandneuraltissue,bywayofthenucleuspulposus.Theaimofthisstudywas toevaluatetheefficacyandsafetyofepiduralblockadeastherapyforbulginglumbardisc herniation.
Methods:Aclinicalstudywasconductedbasedonaretrospectiveandprospectivesurvey. Theblockadeconsistedofinterlaminarpunctureandbolusdrugdelivery.Thenumberof proceduresvariedaccordingtotheclinicalresponse,asdeterminedthroughweekly eval-uationsandthen30,90,and180daysafterthefinalsession.Atotalof124patientswho receivedonetofiveblockadeswereevaluated.
Results:Thesuccessrate(definingsuccessasareductioninsciaticpainofatleast80%)was 75.8%.
Conclusion:Theresultsdemonstratedthetherapeuticactionofepiduralblockadeoverthe shortterm,i.e.incasesofacutepain,thusshowingthatintenseandexcruciatingsciaticpain canberelievedthroughthistechnique.Becauseofthemultifactorialgenesisofsciaticaand thedifficultiesencounteredbyhealthcareprofessionalsintreatingthiscondition,epidural
夽
StudyconductedatClínicadeDor,CampoGrande,MS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.C.Nunes).
http://dx.doi.org/10.1016/j.rboe.2015.09.014
blockade canbecome partof therapeutic arsenal available. This procedureis situated betweenconservativetreatmentwithaneminentlyclinicalfocusandsurgicalapproaches. ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
do
bloqueio
epidural
como
terapêutica
em
pacientes
com
ciatalgia
secundária
a
herniac¸ão
discal
lombar
Palavras-chave:
Deslocamentododisco intervertebral
Dorlombar Bloqueionervoso
r
e
s
u
m
o
Objetivo: Adorciáticasecundáriaahérniadiscallombarécondic¸ãocomplexae,muitas vezes,intensamentelimitante.Ascausasdedornaherniac¸ãodiscalsãomultifatoriais. Nadordiscogênicaháenvolvimentodedoismecanismosfisiopatológicos:adeformac¸ão mecânicadasraízesnervosaseocomponentebioquímicoinflamatório,queresultado con-tatododiscointervertebral,atravésdonúcleopulposo,comotecidoneural.Oobjetivodesta investigac¸ãofoiverificaraeficáciaeaseguranc¸adobloqueioepiduralcomoterapêuticaem hérniasdiscaislombaresprotrusas.
Métodos: Empreendeu-seum ensaioclínico combaseem levantamentoretrospectivoe prospectivo.Obloqueiofoifeitoporpunc¸ãointerlaminarcomadministrac¸ãodefármacos embolo.Onúmerodeprocedimentosvariouconformeaevoluc¸ãoclínica,comavaliac¸ões semanais e, finalmente, aos30, 90 e 180dias da última sessão. Foram avaliados124 pacientes,quereceberamdeumacincobloqueios.
Resultados: Ataxadesucesso(consideradocomoreduc¸ãodenomínimo80%nadorciática) foide75,8%.
Conclusão: Osresultadosrevelaramaac¸ãoterapêuticadobloqueioepiduralemcurtoprazo –ouseja,nadoraguda–edemonstraramqueadorciáticaintensaeexcruciantepode seraliviadacomessatécnica.Agênesemultifatorialdaciatalgiaeasdificuldades encon-tradaspelosprofissionaisemseutratamentopermitemqueobloqueioepiduralintegreo arsenalterapêuticodisponível.Oprocedimentoinsere-seentreotratamentoconservador, eminentementeclínico,eocirúrgico.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The1stBrazilianConsensusonlowbackpainandsciatica1 classifieslowbackpainaccordingtomechanic-degenerative causes and non-mechanical causes (inflammatory, infec-tious,metabolic,andpsychosomatic;fibromyalgia,myofascial syndrome).Mechanic-degenerativecausesinvolvestructural, biomechanical, or vascular changes, or an interaction of these.2–4
Thegreatvariabilityofclinicalpresentationsreflectsthe location ofpain at various levels.1 Lumbar pain that radi-atestothedistalendofthelowerlimbandworsensaftera Valsalvamaneuverindicateaneurologicalorigin;painthat radiatestothebuttocksorposteriorthighandchangewith movementofthelumbarspinearelikelytohaveamechanical origin.Althoughvascularcausesshouldalsobeinvestigated (claudication,temperatureabnormalities,color,etc.),5 prop-erlycharacterizedsciaticatendstobethemainindicatorof discherniation.6
Discherniationresultsfrombiomechanicalfactors, degen-erativechanges,andsituationsthatincreasethepressureon the disc –developments that may or may notproveto be symptomatic.
Therelationshipbetweendiscdegenerativeprocess, dis-placement ofnuclearmaterial, andlow backpain remains controversial, although disc herniation tends to resolve spontaneouslywithinthefirst month.7,8 Throughmagnetic resonanceimaging,discdegenerationshavebeenevidenced in 34% of individuals aged 20–39 years, in 59% of those aged 40–50 years, and in 93% of those aged 60–80 years. Nonetheless,itisdifficulttoattributelowbackpaintothese findings.9
Inmechanic-degenerativelowbackpain,epiduralblocks aregaininggroundinthenon-surgicalarsenal.Giventhe mul-tifactorialgenesisofsciatica,partlyrelatedtoinflammatory processesduetothepresenceofdegenerativediscmaterial intheepiduralspace,theinjectionofananti-inflammatory medicationnearthesiteoforiginofpainisanindicated pro-cedure.
Thisstudy aimedto verify the effectiveness and safety ofepiduralblocksastherapyinprotrudinglumbardisc her-niations;estimate thesuccessrate ofthe epiduralblockin protruding herniations; verify the association between the resultofepiduralblockandthevariablesgender,age, num-berofblocks,anduseofadjuvantmedication;andcompare thepercentageofpain reductionafter30,90,and 180days ofmonitoring,forthefollowingvariables:resultofepidural blocks,numberofblocks,andtheuseofadjuvantmedication.
Materials
and
methods
This was a clinical trial based on a retrospective (patient recordsandinitialinterviews)andprospectivesurvey (inter-viewsafterthestartoftreatment).
Inclusion criteria comprised patients aged ≥18 years; withbackpainthatradiatedtotheposteriorthigh, extend-ing to the corresponding lower limb; pain whose pathway wascompatible withtheaffected rootand associatedwith sensory-subjective changes; and imaging exam diagnosing lumbar degenerative disc disease like protruding hernia-tion. The exclusion criteria comprised previous surgery, chronic/inflammatory degenerative diseases, extruded or migrateddischerniation,localorsystemicinfectiousdiseases, neoplasms,and chronicpainsecondarytoepiduralfibrosis (post-laminectomysyndrome).
Thestudyincludedallpatientswhowereattendedtoin 2012atapaincliniclocatedinCampoGrande,MS,Braziland mettheinclusioncriteria.Patientswereretrospectivelyand prospectivelyevaluatedat30,90,and180daysafter receiv-inganepiduralblock.Theywere clinicallyevaluatedbythe sameexaminer,bothbeforeandafterthestartoftreatment usingthevisualanaloguescale(VAS),11andunderwentsimple radiography andmagneticresonance imagingorcomputed tomography.
Allblocks,madebythesameanesthesiologist,followeda protocol.Aninterlaminarpunctureperformedatthesite indi-catedbytheimagingtests;needlebevelfacedthesideofthe lesion.Thefollowingwereadministeredinbolus:0.5% bupiva-caine(2mL),methylprednisolone(80mg),clonidine(30–75g,
accordingtoageandclinicalconditions),morphine(1mg),and salinesolutionqs(10mL).Patientwassitting,and,when possi-ble,placedinlateraldecubitus.Incaseofpainmanifestation, themostconvenientantalgicpositionwasadopted.Then,a 15-minuterestfollowed.Incaseofcompleteabolitionofpain, theprocedurewasnotrepeated.Incaseofpartial improve-ment,theprocedurewasrepeatedseventotendaysafterthe initialprocedure.Incaseofpartialclinicalimprovement,new blockswereperformed(uptofive).
Weeklyserialclinicalassessmentswereperformedduring theproceduresandat30,90,and180daysofthelast(oronly) block,followingthesameguidelines.Atsuchtimes,general andspecificphysicalexaminationswereperformed,andthe VASwasusedbythepatientandbythephysician.
Tocomparethe proportionsofpatientswith orwithout pain reduction afterblock (outcome) and the independent variables(gender,age,numberofblocks,andadjuvant medi-cation),thechi-squaredtestandthechi-squaredtestfortrend
wereused.Therelativeriskswerecalculatedwiththeir95% confidenceintervals.
Friedman’s test for paired samples was used to com-pare the percentages of reductionof sciatica between the monitoringperiods(30, 90,and 180days).Forthe variables epiduralblockoutcome,numberofblocks,andadjuvant med-ication, theKruskal–Wallis (threeindependentgroups) and Mann–Whitney(twogroups)testswereused.
A5%significancelevelwasadopted.Epi-Info,version7,12 andBio-Stat,version5.313wereusedforstatisticalanalysis.
The study was approved by the Ethics Committee on Human Research of the Universidade Federal do Mato Grosso doSul(Protocol No.2234, CAAE No. 0359.0.049.000-11,November9,2011).Informedconsentsweresignedbythe participants,andallotherethicalrequirementsweremet.
Results
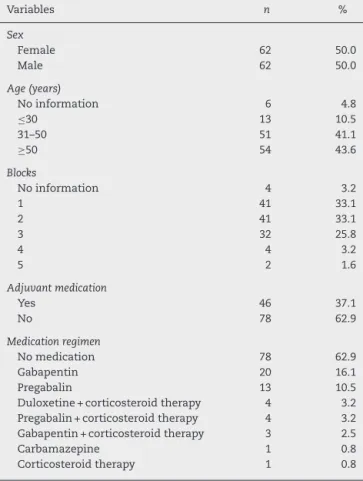
Ofthe129selectedpatientswithlumbardischerniation,five leftthestudy,resultingin124patients(62menand62women), mostofthemwereabove30yearsold(Table1;range:18–79 years;mean:50±14years).Ofthistotal,66.2%receivedoneor twoblocks(range:1–5;mean:2±1).
Adjuvant medication was administered to 37.1% of patients, predominantly gabapentin and pregabalin. Corti-costeroid therapy, alone or in combination with another
Table1–Patientswithlumbardischerniation,according totheassessedvariables.
Variables n %
Sex
Female 62 50.0
Male 62 50.0
Age(years)
Noinformation 6 4.8
≤30 13 10.5
31–50 51 41.1
≥50 54 43.6
Blocks
Noinformation 4 3.2
1 41 33.1
2 41 33.1
3 32 25.8
4 4 3.2
5 2 1.6
Adjuvantmedication
Yes 46 37.1
No 78 62.9
Medicationregimen
Nomedication 78 62.9
Gabapentin 20 16.1
Pregabalin 13 10.5
Duloxetine+corticosteroidtherapy 4 3.2 Pregabalin+corticosteroidtherapy 4 3.2 Gabapentin+corticosteroidtherapy 3 2.5
Carbamazepine 1 0.8
Corticosteroidtherapy 1 0.8
100 80 60 40 20 0 Failure Success 1 block 2 blocks 3 blocks 4 or 5 blocks Non-medicated Medicated
Percentage of lumbar pain reduction
180
90 30
Fig.1–Painreductioninpatientswithlumbardisc herniation,accordingtotheassessedvariablesanddays elapsedafterepiduralblock.CampoGrande,MS,2012 (n=124).
medication,wasseldomused(criterion:partialimprovement associatedwithinterruptionofepiduralblocks).
Consideringthenumberofblocksandtimeelapsedsince last(oronly)block(Table2),weobservedthat,at30-day follow-up,mostpatientshadhadoneblock(35.7%);at90-day,two blocks(35.2%);andat180-day,threeblocks(36.8%).Clinically, longertreatmentperiodsrequiremoreblocks.
Success rate (≥80% reduction in sciatica) was of 75.8% (95% CI: 68.3–83.3%). Failure rate was of 24.2% – in 8.9%, blockwasineffective,butwithoutsubsequentsurgerybecause patientsabandonedtheprotocol,optedformedicaltherapyor acupuncture,amongotherapproaches;12.9%receivedsurgery duetoadverseclinicaloutcomesafterblockages;and2.4%had recurrenceafterreductionof95–100%ofpainwiththeblock.
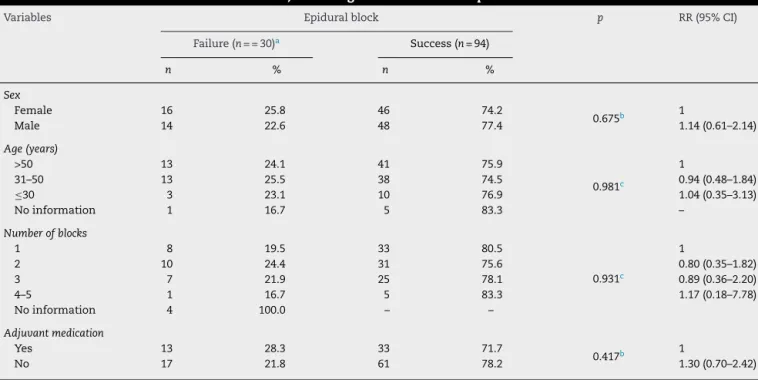
There was nosignificant association betweenfailure or successofthetechniqueandsex,age,numberofblocks,and useofadjuvantmedication(Table3).
At 90-day post-block follow-up, the percentage of pain reductionincreasedwhencomparedwith30-daypost-block (Fig.1).Patientswhodidnotreceiveadjuvantmedicationhad ahigherpercentageofsciaticareductionaftertheprocedure. At30-dayfollow-up,asmallerpercentageofpain reduc-tionwasobservedinpatientssubmittedtotwoblocks(Fig.1). Forthe90- and180-dayfollow-ups,thisdifference wasnot significant.
Regarding block treatment duration, 14 patients were assessed at 30 days: 14.3% were successful in reducing
2
80
12
12 11 7
0 10 20 30 40 50 60 70 80 90
180 Days 90 Days
30 Days
Treatment duration
Number of patients
Success Failure
Fig.2–Patientswithlumbardischerniation,accordingto durationofthetreatmentwithepiduralblockandoutcome. CampoGrande,MS,2012(n=124).
sciatica;inthe91reevaluatedat90days,an87.9%successrate wasobserved;inthe19reassessedat180days,a63.2%rateof successfuloutcomesafterlastblockwasobserved(Fig.2).
Discussion
Painduetolumbardiscdisease,morespecificallylumbardisc herniation,radiatesalongthelowerlimbandtheinjurednerve rootpathway,withsensoryand/ormotordeficitssecondaryto neuraldysfunctionofthatroot.14Itspathophysiologyinvolves both mechanical(compression ofthelumbarroot)15,16 and biochemical/inflammatorycauses.17
Althoughmechanicalfactorshavebeeninvestigatedsince the description of this condition as an intervertebral disc disease by Mixter,18 inflammatory factors have recently beenthesubjectofrigorousresearchinmanyexperimental studies.14,19–21
Thereisevidenceofimmunesystemimpairmentinthe reactionbetweennerverootandexposednucleuspulposus. Theglycosphingolipid(GSL)arecellularcomponentsof cer-taintypesofcentralandperipheralnervoussystemcells.22,23 Astudyondischerniationafterdiscectomyindicatedthe pres-enceofanti-GSLantibodiesathighratesin54%ofpatients. Innon-operatedpatientswithacutesciatica,highrateswere observedin71%ofpatients.24
Therefore, compression-related mechanical, inflamma-tory,andimmunecomponentsareinvolvedinthegenesisof sciatica
Table2–Patientswithlumbardischerniation,accordingtothenumberofepiduralblocksandtimeelapsedfromthelast (oronly)block.
Blocks 30days(n=14) 90days(n=91) 180days(n=19)
N % N % N %
Noinformation 4 28.6 – – – –
1 5 35.7 30 33.0 6 31.6
2 4 28.6 32 35.2 5 26.3
3 1 7.1 24 26.4 7 36.8
4 – – 3 3.3 1 5.3
5 – – 2 2.1 – –
Table3–Patientswithlumbardischerniation,accordingtotheoutcomeofepiduralblockandassessedvariables.
Variables Epiduralblock p RR(95%CI)
Failure(n==30)a Success(n=94)
n % n %
Sex
Female 16 25.8 46 74.2
0.675b 1
Male 14 22.6 48 77.4 1.14(0.61–2.14)
Age(years)
>50 13 24.1 41 75.9
0.981c
1
31–50 13 25.5 38 74.5 0.94(0.48–1.84)
≤30 3 23.1 10 76.9 1.04(0.35–3.13)
Noinformation 1 16.7 5 83.3 –
Numberofblocks
1 8 19.5 33 80.5
0.931c
1
2 10 24.4 31 75.6 0.80(0.35–1.82)
3 7 21.9 25 78.1 0.89(0.36–2.20)
4–5 1 16.7 5 83.3 1.17(0.18–7.78)
Noinformation 4 100.0 – –
Adjuvantmedication
Yes 13 28.3 33 71.7
0.417b 1
No 17 21.8 61 78.2 1.30(0.70–2.42)
Ifp≤0.05,statisticallysignificantdifference.Thecategory“noinformation,”whenpresent,wasremovedfromthetestcalculation.
Source:Hospitalfiles,2012(n=124).
a <80%reductioninlumbarpainaftertheblock. b Chi-squaredtest.
c Chi-squaredtestfortrend.
Thepathophysiology of sciatica is characterizedby the factthatthenucleuspulposus,whichcausesinflammation, causestheinvolvementofkeyinflammatorymediatorsand leadstodemyelination,rootganglionischemia,andincreased endoneural pressure, with consequent reduction of nerve stimulusspeed.24Thisinflammatoryreactionisfollowedby theimmuneresponse.
Theuseofcorticosteroidsassociatedwithlocal anesthet-icsattheepiduralsiteiscommoninseveralreferencecenters forthetreatmentofradiculopathy.25,26InBrazil,theprocedure hasspreadfromtheideasofJohnBonicaapudCastro.27 Mul-timodalanalgesiaisrecognizedasthemostadequateforthe treatmentofsciatica.28
Lumbarpuncture(bothmedianandparamedian)is prefer-abletosacralpunctureduetoloweranatomicalvariation,as wellasgreater easeoflocation anddepositionofthe solu-tionclosertotheinjury.29Useoffluoroscopyiscontroversial. CannonandAprill26indicate theoccurrenceofroute diver-sionin18–52%ofcases,dependingontherouteusedandthe experienceoftheprofessional.AccordingtoJohnsonetal.,30 resultsarepositiveinapproximately 95%ofcases,without usingcontrastandfluoroscopy.
Whenthedesiredeffectisachievedwithasingle proce-dure,theneedforrepetitionbecomesunlikely.31Nonetheless, there are patients who do not present an initial satisfac-toryresponse,butrespondtoasecondorthirdprocedure.26 SwerdlowandSayle-Creer32postulatethatthesolutionshould remaininplaceformorethantwoweeks.Chenetal.33 sup-portedthetwo-weekrangeofvalidity,butadmittedrepeating theprocedureinasmallerinterval iftheclinicalsettingso
requested.However,theydidnotagreewiththeideaof “stan-dardizing”aseriesofthreeblockswithoutintercurrentclinical evaluation,despitethefactthatexperienceshowsthe num-berofprocedurestobetypicallythreeorfour.Theseauthors indicatethatthereisnosupportforthisconductinthe litera-ture.
Inthepresentseries,asuccessrateof75.8%wasachieved – 12.9% of patients subsequently underwent surgery: one patienthadsignificanturinaryretentionforabout6hafterthe procedure,withnoassociatedanalgesicbenefit,andtwohad nosuccesswiththetechnique(punctureerrororduramater puncture),andprocedurewasaborted.Thesethreepatients wereincludedinthegroupthatwaslaterreferredtosurgery. Literatureindicatesthat10–15%ofpatientswithsciatica secondarytoadischerniationundergosurgery,34which cor-respondedwiththepresentfindings(Table3).
Inaccordancewithexistinginternationalprotocols, pos-itive results required two blocks, on average. Adjuvant medicationwasadministeredto37.1%ofthepatients(Table1). Epidural blockisconsidered tobesafe,presenting good cost-effectiveness and representing a minimally invasive treatmentforsciatica,particularlyinacutecases.This pro-cedureshouldbeusedinclinicalsituationsofpaincrisis,and italsoallowsfortheprognosisoffuturesurgery.35
Study
limitations
Thesamplesize(124patients)andtheselectionofsubjects (restrictedtothose who attended asinglecliniclocated in Campo Grande, Brazil, in the period investigated) can be consideredasinherentlimitationstothisstudy.For ethical reasons,thestudy didnotincludeacontrolgroup,inorder toavoiddeprivinganypatientsfromthetreatment adminis-tered.
Conclusions
Consideringthelimitationsofthisstudy,theprocedurewas proventobeeffective, asitprovidedrelief fromsciatica in 75.8%ofpatients,andsafe,asonlythreecases(2.4%)had tech-nicalproblems(bladderfunctiondisorderinonepunctureand errorintwo).
Bestclinicaloutcome(87.9%success)withthelargest num-berofpatients(91)wasobservedat90daysoffollow-up.
Therewas noassociation betweenepiduralblocks (suc-cess/failure) and the variables gender, age, number of procedures,anduseofadjuvantmedication.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CecinHA.Consensobrasileirosobrelombalgiase
lombociatalgias.SãoPaulo,Uberaba:SociedadeBrasileirade
Reumatologia,FaculdadedeMedicinadoTriânguloMineiro;
2000.
2. BassamBA.Lowbacksyndromes.Thechallengeofaccurate
diagnosisandmanagement.PostgradMed.1990;87(4):209–15.
3. McQuayHJ,MooreRA.Epiduralcorticosteroidsforsciatica.In:
McQuayHJ,MooreRA,editors.Anevidence-basedresource
forpainrelief.NewYork:OxfordUniversityPress;1998.p.
216–8.
4. NachemsonAL,AnderssonGB.Classificationoflow-back
pain.ScandJWorkEnvironHealth.1982;8(2):134–6.
5. CoxJM.Dorlombar:mecanismo,diagnósticoetratamento.
6thed.SãoPaulo:Manole;2002.p.17–30,377–507.
6. DeyoRA,Tsui-WuYJ.Descriptiveepidemiologyoflow-back
painanditsrelatedmedicalcareintheUnitedStates.Spine
(PhilaPa1976).1987;12(3):264–8.
7. BozzaoA,GallucciM,MasciocchiC,AprileI,BarileA,
PassarielloR.Lumbardiskherniation:MRimaging
assessmentofnaturalhistoryinpatientstreatedwithout
surgery.Radiology.1992;185(1):135–41.
8. BodenSD,DavisDO,DinaTS,PatronasNJ,WieselSW.
Abnormalmagnetic-resonancescansofthelumbarspinein
asymptomaticsubjects.Aprospectiveinvestigation.JBone
JointSurgAm.1990;72(3):403–8.
9. NachemsonAL,JonssonE,editors.Neckandback:the
scientificevidenceofcauses,diagnosisandtreatment.
Philadelphia:LippincottWilliams&Wilkins;2000.
10.SouzaFAE,PereiraLV,HortenseP.Avaliac¸ãoemensurac¸ãoda
percepc¸ãodador.In:AlvesNetoO,CostaCMC,SiqueiraJTT,
TeixeiraMJ,editors.Dor:princípioseprática.PortoAlegre:
Artmed;2009.p.370–81.
11.CentersforDiseasesControlandPrevention(CDC).EpiInfo
2011:version7:programsforusebypublichealth
professionals.Atlanta:CDC;2011.
12.AyresM,AyresJM,AyresDL,SantosAAS.BioEstat:aplicac¸ões
estatísticasdasciênciasbio-médicas:versão5.0.Belém:
SociedadeMamirauá;2007.
13.OlmarkerK,StørksonR,BergeOG.Pathogenesisofsciatic
pain:astudyofspontaneousbehaviorinratsexposedto
experimentaldischerniation.Spine(PhilaPa1976).
2002;27(12):1312–7.
14.KawakamiM,WeinsteinJN,ChataniK,SprattKF,MellerST,
GebhartGF.Experimentallumbarradiculopathy.Behavioral
andhistologicchangesinamodelofradicularpainafter
spinalnerverootirritationwithchromicgutligaturesinthe
rat.Spine(PhilaPa1976).1994;19(16):1795–802.
15.WinkelsteinBA,WeinsteinJN,DeLeoJA.Theroleof
mechanicaldeformationinlumbarradiculopathy:aninvivo
model.Spine(PhilaPa1976).2002;27(1):27–33.
16.OlmarkerK,RydevikB,NordborgC.Autologousnucleus
pulposusinducesneurophysiologicandhistologicchanges
inporcinecaudaequinanerveroots.Spine(PhilaPa1976).
1993;18(11):1425–32.
17.MixterWJ.Ruptureofthelumbarintervertebraldisk:an
etiologicfactorforso-calledsciaticpain.AnnSurg.
1937;106(4):777–87.
18.OmarkerK,MyersRR.Pathogenesisofsciaticpain:roleof
herniatednucleuspulposusanddeformationofspinalnerve
rootanddorsalrootganglion.Pain.1998;78(2):99–105.
19.KawakamiM,TamakiT,MatsumotoT,KuribayashiK,
TakenakaT,ShinozakiM.Roleofleukocytesinradicularpain
secondarytoherniatednucleuspulposus.ClinOrthopRelat
Res.2000;376:268–77.
20.MurataY,NannmarkU,RydevikB,TakahashiK,OlmarkerK.
Nucleuspulposus-inducedapoptosisindorsalrootganglion
followingexperimentaldischerniationinrats.Spine(PhilaPa
1976).2006;31(4):382–90.
21.SullivanWJ,WillickSE,Chira-AdisaiW,ZuhoskyJ,Tyburski
M,DreyfussP,etal.Incidenceofintravascularuptakein
lumbarspinalinjectionprocedures.Spine(PhilaPa1976).
2000;25(4):481–6.
22.SvennerholmL,BoströmK,FredmanP,MånssonJE,
RosengrenB,RynmarkBM.Humanbraingangliosides:
developmentalchangesfromearlyfetalstagetoadvanced
age.BiochimBiophysActa.1989;1005(2):109–17.
23.BrisbyH,BalaguéF,SchaferD,SheikhzadehA,LekmanA,
NordinM,etal.Glycosphingolipidantibodiesinserumin
patientswithsciatica.Spine(PhilaPa1976).2002;27(4):
380–6.
24.VanniSMA.Injec¸ãosubaracnoideainadvertidadecorticoide
emtratamentodedorcrônicadacolunalombar:relatode
caso.RevBrasAnestesiol.2004;54(6):821–5.
25.CannonDT,AprillCN.Lumbosacralepiduralsteroid
injections.ArchPhysMedRehabil.2000;813(Suppl.1):S87–98.
26.CastroAB.TratamentodadornoBrasil:evoluc¸ãohistórica.
Curitiba:Maio;1999.
27.CarneiroAF,AlvesNetoO.Corticoidesespinais.In:AlvesNeto
O,CostaCMC,SiqueiraJTT,TeixeiraMJ,editors.Dor:
princípioseprática.PortoAlegre:Artmed;2009.p.1320–6.
28.ScottDB.Bloqueioperidural.In:RogersMC,TinkerJH,Covino
BC,LongneckerDE,editors.Princípiosepráticade
anestesiologia.RiodeJaneiro:GuanabaraKoogan;1993.p.
955–71.
29.JohnsonBA,SchellhasKP,PolleiSR.Epidurographyand
therapeuticepiduralinjections:technicalconsiderationsand
experiencewith5334cases.AJNRAmJNeuroradiol.
1999;20(4):697–705.
30.Gonc¸alvesBMV.Sobreousodecorticosteroidesporvia
Janeiro:UniversidadeFederaldoRiodeJaneiro; 1976.
31.SwerdlowM,Sayle-CreerWS.Astudyofextradural
medicationinthereliefofthelumbosciaticsyndrome.
Anaesthesia.1970;25(3):341–5.
32.ChenB,StitikTP,FoyePM,CastroCP,MehnertFJ.Epidural steroidinjections;2011.Availablefrom:http://emedicine.
medscape.com/article/325733-overview#showall[cited
24.09.12].
33.BushK,CowanN,KatzDE,GishenP.Thenaturalhistoryof
sciaticaassociatedwithdiscpathology.Aprospectivestudy
withclinicalandindependentradiologicfollow-up.Spine
(PhilaPa1976).1992;17(10):1205–12.
34.LoyTT.Epiduralsteroidinjectionforsciatica:ananalysisof
526consecutivecaseswithmeasurementsandthewhistle
test.JOrthopSurg(HongKong).2000;8(1):39–44.
35.RiewKD,YinY,GilulaL,BridwellKH,LenkeLG,LauryssenC,
etal.Theeffectofnerverootinjectionsontheneedfor
operativetreatmentoflumbarradicularpain:aprospective,
randomized,controlled,double-blindstudy.JBoneJointSurg
Am.2000;82(11):1589–93.
36.RiewKD,ParkJB,ChoYS,GilulaL,PatelA,LenkeLG,etal.
Nerverootblocksinthetreatmentoflumbarradicularpain:a
minimumfive-yearfollow-up.JBoneJointSurgAm.