www.revportpneumol.org
SPECIAL
ARTICLE
Understanding
COPD:
A
vision
on
phenotypes,
comorbidities
and
treatment
approach
E.
Fragoso
a,
S.
André
b,
J.P.
Boleo-Tomé
c,
V.
Areias
d,e,
J.
Munhá
f,
J.
Cardoso
g,h,∗,
on
behalf
of
GI
DPOC-Grupo
de
Interesse
na
Doenc
¸a
Pulmonar
Obstrutiva
Crónica
aPulmonologyDepartment,HospitaldeSantaMaria,CentroHospitalarLisboaNorte,EPE(CHLN),Lisbon,Portugal bPulmonologyDepartment,HospitalEgasMoniz,CentroHospitalardeLisboaOcidental,EPE(CHLO),Lisbon,Portugal cPulmonologyDepartment,HospitalProf.DoutorFernandodaFonseca,EPE,Amadora,Portugal
dPulmonologyDepartment,HospitaldeFaro,CentroHospitalardoAlgarve,EPE,Faro,Portugal eDepartmentofBiomedicalSciencesandMedicine,AlgarveUniversity,Portugal
fPulmonologyDepartment,CentroHospitalardoBarlaventoAlgarvio,EPE,Portimão,Portugal
gPulmonologyDepartment,HospitaldeSantaMarta,CentroHospitalardeLisboaCentral,EPE(CHLC),Lisbon,Portugal hNovaMedicalSchool,NovaUniversity,Lisbon,Portugal
Received17September2015;accepted2December2015
Availableonline27January2016
KEYWORDS COPD; Phenotypes; Riskfactors; Modifiablerisk factors; Symptoms; Severity; Comorbidities; Exacerbations
Abstract ChronicObstructivePulmonaryDisease(COPD)phenotypeshavebecomeincreasingly recognizedasimportantforgroupingpatientswithsimilarpresentationand/orbehavior,within the heterogeneity ofthe disease. The primary aimof identifyingphenotypes is to provide patientswiththebesthealthcarepossible,tailoringthetherapeuticapproachtoeachpatient. However,theidentificationofspecificphenotypeshasbeenhinderedbyseveralfactorssuch aswhichspecificattributesarerelevant,whichdiscriminantfeaturesshouldbeusedfor assign-ingpatientstospecificphenotypes,andhowrelevantaretheytothetherapeuticapproach, prognostic and clinical outcome. Moreover, the definition ofphenotype is still not consen-sual. Comorbidities, risk factors, modifiable risk factorsand disease severity, although not phenotypes,haveimpactacrossallCOPDphenotypes.
Althoughtherearesomeidentifiedphenotypesthatarefairlyconsensual,manyothershave beenproposed,butcurrentlylackvalidation.The on-goingdebateaboutwhichinstruments andtestsshouldbeusedintheidentificationanddefinitionofphenotypeshascontributedto thisuncertainty.
In thispaper,theauthors reviewpresentknowledgeregardingCOPDphenotyping,discuss theroleofphenotypesandcomorbiditiesontheseverityofCOPD,proposenewphenotypes
∗Correspondingauthor.
E-mailaddresses:[email protected](E.Fragoso),[email protected](S.André),[email protected](J.P.Boleo-Tomé), [email protected](V.Areias),[email protected](J.Munhá),[email protected](J.Cardoso).
http://dx.doi.org/10.1016/j.rppnen.2015.12.001
2173-5115/©2016SociedadePortuguesadePneumologia.PublishedbyElsevierEspaña,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
andsuggestaphenotype-basedpharmacologicaltherapeuticapproach.Theauthorsconclude thatapatient-tailoredtreatmentapproach,whichtakesintoaccounteachpatient’sspecific attributesandspecificities,shouldbepursued.
© 2016 Sociedade Portuguesa de Pneumologia. Published by Elsevier España, S.L.U. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a com-plex,multicomponent,heterogeneousdisease.Theclassical COPDclassificationhasbeenbasedonForcedExpiratory Vol-umeinthefirstsecond (FEV1), butthisaloneis nolonger accepted as a single parameter to define severity or to guidetreatment.1TheupdatedGlobalInitiativeforChronic
ObstructiveLungDisease(GOLD)recommendationspropose treatment approachbased on twoadditional parameters, symptomsandexacerbations,whichmaystillbeinsufficient toreflecttheheterogeneityofCOPD.Thereisarealneedto identifyspecificattributesinordertogroupthe heteroge-neousCOPDpopulationintodifferentphenotypes,andguide a patient oriented therapeutic approach. Several pheno-typeshavealreadybeenproposed,2---21buttheunderstanding
ofwhichattributesdefinewhichgroupsofpatientsremains achallenge.
Itisrecognizedthatfuturestudiesshouldfocuson estab-lishingsimple algorithms based on the most discriminant featuresforassigningpatientstospecificphenotypes.Such algorithms have tobe tested in validationcohorts before theycanbeusedinclinicalpractice.4Hanetal.proposea
schematoidentifycandidatephenotypesandvalidatethem oncetheirrelevancetoclinicaloutcomesisestablished.6
COPD patients frequently have several
comorbidities6,14,15,18,22,23 that should be actively sought
for andduly addressed therapeutically.Some associations between comorbidities and phenotypeshave been identi-fied,andalthoughtheyarerelevanttotheoverallseverity andrisk,theirrealimpactonCOPDisnotclearlyestablished. Inthispaper,theauthorsreviewpresentknowledgeand acceptedcriteriafor thesecrucialaspectsofthedisease, proposedefinitionsforphenotypingCOPD,discusstheroleof phenotypesandcomorbiditiesontheseverityofCOPD,and suggestatherapeuticapproachforconsensualphenotypes.
Phenotypes,
risk
factors
and
severity
Phenotypes
WiththerecognitionthatFEV1isnotsufficientto
character-izeandclassifyCOPDpatients,theconceptofphenotypes re-emerged,andthetraditionalconceptof‘‘bluebloaters’’ and‘‘pink puffers’’,abandonedin the past, isnow being replacedbyavarietyofdifferentphenotypes.24 The
phen-otypingprocess emergesasa consequence of the clinical need to group patients with similar presentation and/or behavior,withintheheterogeneityofthedisease,inorder toprovide themwiththebesthealth carepossible, tailo-ringthetherapeutic approachtoeach patientinterms of
symptoms control, disease progression, health status and qualityoflife.
Hanetal.6proposedthefollowingphenotypedefinition:
‘‘asingleorcombinationofdiseaseattributesthatdescribe differencesbetweenindividualswithCOPDastheyrelateto clinicallymeaningful outcomes(symptoms,exacerbations, responsetotherapy,rateofdiseaseprogression,ordeath)’’. Itfollowsfromthisdefinitionthatpatientsmaybeclassified intodistinct prognosticand therapeuticsubgroups. Mirav-itllesetal.25simplifythisdefinitionbysayingthat‘‘theterm
COPDphenotypeisreservedforthedifferentclinicaltypes that have therapeutic impactand areidentified in COPD patients’’.Salzman proposesthatan outcomecanalsobe included,24andsomeauthorssuggestthat,dependingonthe
context, someCOPD features,e.g., dyspneaor exacerba-tions,couldbeconsideredbothoutcomesandphenotypes.26
Weproposethataphenotypeisanattributeorasetof attributesthatcanbeclinicallycharacterized,issomewhat stableovertime,anddefinearelevantgroupofindividuals, bothintermsoftherapeuticandprognosticimplications.
Riskfactors
The latest GOLD guidelines contemplate the cross-combination of two distinct dimensions: a symptom dimension,assessedbytheModifiedMedicalResearch Coun-cil Dyspnea Scale (mMRC) or the COPD Assessment Test (CAT),andariskdimension,assessedbyFEV1andfrequency
of exacerbations. Patients are classified as A, B, C, or D dependingonthecombinationofthesethreeparameters.25
However,differentpatientsexistwithintheriskdimension, giventhatariskassessmentbasedonthedegreeofairflow obstructionisdifferentfromariskassessmentbasedonthe occurrenceofexacerbations.Moreover,exacerbationshave differenttypes,severityandpresentations,andarenot pre-dictiveofthesamerisk.Also,patientsmayhavesymptoms and risk that are independent of the respiratory disease, namelythepresenceofsignificantcomorbidities.
Thus,risk and symptoms shouldbe considered vectors or dimensions of COPD, which can be present in several phenotypes.
Some factors can be present in several phenotypes andmodify thedevelopmentandclinical course ofCOPD. In this view, comorbidities would be modifying factors since they both change over time and can exist across allphenotypes,27 andsowouldinflammation28 andgenetic
polymorphisms,11,29sincetheymodifytheexpressionof
rec-ognized phenotypes. However,noprecise definitionexists formodifyingfactorsinCOPD.
In COPD, the most consensual modifiable risk factor (or behavior) is smoking. Other modifiable behaviors that impact COPD are Body Mass Index (BMI)30 and physical
activity.31 Environmentalexposure suchasexposure toair
pollutioncanbemodifiablebutcanhardlybeconsidereda behavior. Furthermore,it canbe arguedthat professional exposureisconsideredamodifiableriskfactor,asforsome patientsitcontributestoworseningofthediseaseanditcan beinterrupted.
Severity
Historically,assessment ofCOPDseveritywasbasedsolely on FEV1. Currently, and although spirometry is required
to establish a diagnosis of COPD, it is considered insuf-ficient to describe COPD severity.1,15,32 A comprehensive
assessment of COPD including symptom assessment using validatedquestionnairessuchasmMRC,theClinicalCOPD Questionnaire (CCQ)33 and CAT,34 degree of airflow
limi-tation, riskof exacerbations, existenceof comorbidities,1
overallimpactofCOPDinapatient’sQualityofLife(QoL), and exercise tolerance35 and levels of physical activity,
is nowrecommended.The latter isparticularly important because the amount of physical activity a patient takes and their functional status predict exacerbations, hospi-talizations,and mortality.31 Indeed, theUPLIFT study has
shown that although FEV1 did not differ between
treat-ment groups (long-acting muscarinicantagonist [LAMA] vs placebo),healthstatus,timetofirstexacerbationandtime to exacerbationresulting in hospital admission were bet-ter in the LAMA group,36 strongly suggesting that FEV
1
perseis notsufficient todeterminedisease severity.The TORCHstudy showed that FEV1 declined faster in current
smokers,patients withalowerbody massindex,patients withmoderatedisease,andpatientswhoexacerbatedmore frequently,37 also suggesting that comorbidities might be
majordeterminantsofdiseaseseverity.18
COPD severityisdifferent fromCOPDactivity.Severity hasbeen proposedasa conceptthatshouldberelatedto lossoforganfunctionthateventuallyimpactsonfunctional impairmentandprognosis,whereasCOPDactivityrelatesto theactivationlevel ofthecellularmechanismsunderlying diseaseprogression.26
We propose that disease severityshould bedefinedby mortalityrisk,dailyimpactofthediseaseandlossoforgan function.
Identifying
phenotypes
in
COPD
Detailed questionnaire data and pulmonary function tests have been proposed todifferentiate between COPD phenotypes.12 Multidimensional indexes built to
strat-ify risk/severity are not useful in identifying different phenotypes. Nevertheless, functional measurements of severity that correlate with mortality in COPD, such as FEV1,theratioofinspiratorycapacitytototallungcapacity
(IC/TLC), the diffusing capacity of the lung for carbon monoxide (DLCO), 6-min walking distance, and maximum O2 consumption or maximum watts on exercise testing,
may help in identifying phenotypes. Although it is not diagnostic, bronchodilator responsiveness can be useful in the distinction between asthma and COPD, and in the definition of the mixed asthma-COPD (ACOS) phenotype. However,pulmonaryfunctiontestsdonotidentifysubsets thatrespondtoparticulartherapies.24
Imaging techniques, such as Computed Tomogra-phy (CT),6,12,38---42 high-resolution computed tomography
(HRCT)16,43 and magnetic resonance imaging (MRI)39 have
been suggested to be of clinical use in discriminating betweensome COPD phenotypes,and maybe novel tools thatwillallowforamoreaccuratediagnosisandhelpguide clinical management.39,40 The usefulness of these
tech-niquesis stilldebatable, sinceit is recognizedthat there arefactorsnoteasilyassessedbycurrenttechniques.41
We propose that a combination of questionnaires, objective parameters such as pulmonary function tests, includingIC/TLC, 6-minwalkingdistance, exercisetesting and thoracic CT, should be able to discriminate between phenotypes.
Mostclinicallyrelevantphenotypes
The most consensual or most clinically relevant pheno-types are the non-exacerbator phenotype,14 the ACOS
phenotype,8,12,14,15,17 the exacerbator with
emphy-sema phenotype,8,12,14,16 the exacerbator with chronic
bronchitis,8,12,14,16,18 and the frequent exacerbator.2,6,7,23
However, even these most consensual phenotypes may not be easy to manage, since considerable overlap has been described between COPD phenotypes with chronic bronchitis,emphysema or asthma, which has therapeutic consequences.12ACOPD-bronchiectasisclinicalphenotype20
hasalsobeen suggested.TheSpanishguidelinesrecognize theneed toidentify bronchiectasis and chronic bronchial infectionin patientswiththeexacerbatorphenotypewith chronic bronchitis, but do not support them as clinical phenotypeswiththeirownclinicalrelevance forthe time being.14
We agree with the less symptomatic non-exacerbator, the exacerbator with emphysema, the exacerbator with chronicbronchitis, andACOSphenotypes asbeing fourof themostclinicallyrelevantphenotypes,propose the addi-tionofthesymptomaticnon-exacerbatorwithemphysema asaclinicallyrelevantphenotype,andfurtherproposethat theCOPD-bronchiectasisshouldbeconsideredanimportant clinicalphenotypewithitsownclinicalrelevance---Fig.1.
Otherpotentialphenotypes
Several other COPD phenotypes have been
proposed,3---5,10,11,13,21 but it remains unclear if these
are actually specific phenotypes. The proposed fast decliner phenotype19 can only be identified over time
and not a priori and thus it is difficult to include as a clinical phenotype. The combined pulmonary fibrosis and emphysema syndrome9 is another potential, albeit not
consensual,phenotype, in which imagingis pivotal. Since many aspects of COPD clinical phenotypes are related to inflammation,28 it has been proposed that the presence
of systemic inflammation may represent a unique COPD phenotype,6andpatientswithsubstantialsystemic
inflam-mation and relevant comorbidities might form specific phenotypes that lead tomodified treatment strategies.18
However, this is not consensual.27 Therefore, systemic
inflammationandcomorbiditieswouldbemodifyingfactors andnotphenotypes.Currentsmokerscouldalsorepresent
Chronic respiratory symptoms in patients with risk factors for COPD
FEV 1/FVC post-BD <70% → COPD
History of exacerbations
≥2/year
(or≥1 hospitalization) (no hospitalizations)<2/year
Wheezing as a dominant feature Symptom variabilty
Significnt response to bronchodilation Sputum or peripheral eosinophilia
Past history of bronchial asthma
Overlap asthma-COPD (mixed phenotype)
Scarce symptoms
Severe lung overinflation (IC/TLC<25%)
End-stage lung disease: Chronic respiratory failure Heavily symptomatic (marked exercise intolerance) Optional: Thoracic CT showing thickened bronchial walls, large/ small-airways mucoid impaction Cough and phlegm most of the days for 3 consecutive months during 2 years Thoracic CT: Emphysema-predominant pattern Thoracic CT: Significant bronchiectasis
Relatively preserved lung function
Other features
Non exacerbator Exacerbator
Exacerbator with
emphysema Less symptomatic
Comorbidities Symptomatic (usually emphysematous) COPD-bronchiectasis Exacerbator with chronic bronchitis Phenotype?
Clinical features, complete pulmonary function test (PFT) , thoracic CT scan, additional assessments (sputum cytology, complete blodd count)
Figure1 Proposedmostclinicallyrelevantphenotypes.
a different phenotype, but since they must be identified across all phenotypes and intensive smoking cessation strategiesmustbeadopted intheseindividuals,27 smoking
would bea modifiable risk factor, or behavior, and not a phenotype.COPDseverityisnotaphenotypicfeaturesince itcanbeaconsequenceofaspecificclinicalphenotype.26
Undoubtedly,theissueofwhichclinicalphenotypesactually existwarrantsfurtherdiscussion.
Finally,itmustbeemphasizedthatcomorbidities, respi-ratoryfailureandend-stagediseasehaveimpactacrossall COPDphenotypes.
Risk
factors
---
significant
comorbidities
The presence of significant comorbidities is perhaps one of the most important modifying risk factors for sever-ity in COPD. They contribute to the overall severity in individual patients,18,44 have a major impact on quality
of life,23 increase the risk of certain causes of mortality
and of all-cause mortality3,15,23 and are major causes of
hospitalization,14,23especiallycardiovasculardisease(CVD)
and cancer.3,15,45 They should always be considered as a
very important feature in all patients, regardless of the stageorgrade.
Althoughtheprevalenceofdifferentcomorbiditiesvaries withtheGOLDstage,46availableevidencedoesnotsupport
arelationshipbetweencomorbiditiesandGOLDgroups. Dys-pnea,health status,exacerbationsandcomorbiditiessuch as chronic heart failure anddepression are markedly dif-ferentamongsubjects withthesame GOLDclassification, underscoring the need for a multidimensionalassessment ofCOPDpatients.3Metabolicandcardiovascular
comorbidi-ties appear relatively unrelated to the degree of airflow limitation.4
Comorbidities can be associated with any clinical phenotype27 andshouldbeconsideredinacomprehensive
therapeutic approach. A few recent studies have investi-gatedassociationsbetweencomorbiditiesandspecificCOPD phenotypes,47---50 oridentifiednovel phenotypesassociated
withcomorbidities,3---5,21butresultsarestillscarceto
estab-lishassociationsordrawdefiniteconclusions.Theexistence of COPDis associated withhigher risk for other diseases, suchascardiovasculardiseaseandlungcancer,butwhether thisassociation is due tocommonrisk factorsor common disease pathways (e.g.,smoking), susceptibilitygenes, or impairedclearanceofcarcinogensisnotclear.18,23Giventhe
factthatmorethan50%ofCOPDpatientshavefourormore comorbidities,51itiscurrentlydifficulttoascertainwhether
COPDisadiseasedistinctfromitscomorbiditiesorwhether thesearepartofthespectrumofCOPDmanifestations.
Comorbidities in COPDshouldbemanaged inthe same wayasforallotherpatientswithoutCOPD.1Infact,there
is growingevidencethat someof thetreatmentsusedfor comorbidities,suchasbetablockers,mayhaveabeneficial effect on the course of COPD. The Spanish guidelines provide an outline of the most common comorbidities of COPD,withitsdiagnosis andtreatment.14 Finally,whether
treatmentofco-morbidconditionsaltersthenaturalhistory of COPD or whether treatment effectiveness of COPD is altered by the presence of a concomitant comorbidity awaitsfurtherstudy.6,52
Cardiovasculardisease
The most frequent comorbidities associated with COPD are those related to the cardiovascular system.1,15,53,54
TheLungHealthStudyreportedthatcardiovascularcauses accounted for 42% of first hospitalizations and 44% of second hospitalizations of patients with relatively mild COPD,whereas respiratorycauses accounted for only14% of hospitalizations.15 Hypertension seems to be the most
prevalent cardiovascular comorbidity1,53 across all GOLD
stages.46 COPD patients are at greater risk of
cardiovas-cularmortality,55 withatrialfibrillation/flutter,congestive
heartfailureandcoronaryarterydiseasehavingacombined prevalence of 58.9% and being strongly associated with increasedriskofdeath.53Moreover,heartfailureprevalence
is muchhigheramongpatients experiencing an exacerba-tion,andistheleadingcauseofhospitalizationanddeath inCOPD patients.54 Also,aworseningofheart failureis a
challengeinthedifferentialdiagnosisofanexacerbation.1
The presence of heart failure may bea confounding fac-toraswell,whentryingtoidentifyapatient’sphenotype. With respect torecurrent interstitial lung edema, it may be responsible for wheezing and dyspnea in the setting of chronic obstructivelung disease, thus misidentifying a patientashavingACOS.
Itshouldbenotedthatdifferentcardiovasculardiseases haveadifferentclinicalimpactonCOPD,andtheGOLD2015 guidelinespropose that fourseparate entities withinCVD shouldbeconsidered:ischemicheartdisease,heartfailure, atrialfibrillationandhypertension.1
Although the precise mechanisms by which COPD may be a risk factor for CVD are not fully understood, evi-dencehassuggestedthatairflowlimitationandparticularly hyperinflation affect cardiac function and gas exchange, and that inflammatory mediators in circulation may initi-ateorworsencomorbiditiessuchasischemicheartdisease
andheartfailure.1,15Hyperinflationdirectlyaffectscardiac
dimensions, diastolicfilling,systolicejection fractionand cardiacmass,thusbeingacrucialcomponentforsomeofthe mostrelevantclinicalaspectsofCOPD,dyspneaand exer-ciselimitation.56,57 Ontheother hand,tworecentreports
didnotfinddifferencesinlow-gradesystemicinflammation betweenfiveidentifiedcomorbidityclusters,oneofwhich wascardiovascular,51norconfirmedthatamore
inflamma-toryCOPDmaybeacoronaryheartdiseaseriskfactor.55One
possibleexplanationisthatinflammationisindirectly asso-ciatedwithcardiovascularrisk,influencingotherfactorsor comorbiditiesthatinturnincreasethecardiovascularrisk.
Cardiovascularcomorbiditiesshouldbetreatedaccording tousualguidelines,andbeta-blockersshouldnotbe with-heldfromthesepatients,althoughselectivebeta1-blockers
arepreferred.1 In fact, recent studies reported a
reduc-tionof theriskfor exacerbationsrelatedtobeta-blockers use. The use of statins to reduce exacerbations is more controversial, and recent studies have reported different results.58---61
WeagreethatCOPDpatientsshouldbeactivelytreated for cardiovascular comorbidities, toreduce CV exacerba-tionsandmortalityandthatcardioselective beta-blockers shouldbeusedifrecommendedfortheexisting cardiovas-cularcomorbidity.
Lungcancer
Agrowing body of evidence supports COPD asa risk fac-torforlungcancer.62However,theincidenceoflungcancer
amongdifferentstagesofCOPDhasshowndifferentresults, withsome studies finding increased incidence withCOPD severity45 and others reporting the opposite.63 A possible
justificationforthesecontradictoryresultscouldberelated to the two proposed underlying mechanisms associating COPDtolungcancer:ifapatienthasgeneticorepigenetic riskfactorscommontobothdiseases,thenlungcancercould bemoreprevalentatlesssevereCOPDstages,andpatients inthemoreseverestageswouldnothavethepredisposing riskfactors;if,ontheotherhand,chronicinflammationis theculprit,then the worsethe COPDseverity, thehigher theprobabilityofdevelopinglungcancer.However,thetrue reasonforthesedifferentresultsawaitsfurtherstudies.
Earlylungcancerdiagnosisisofparamountimportance, andarecentstudysuggeststhatcurrentandformer smok-erswithCOPDmaybenefitfromlowerpack-yearthreshold forlungscreeningeligibility.64Apotentiallyinteresting
com-plementarytestwouldbetomonitorcirculatingtumorcells, whichhavebeenshowntobedetectedinpatientswithCOPD withoutclinicallydetectablelungcancer.65
LungcancerinCOPDpatientsshouldbetreatedaccording tolungcancerguidelines1.
Wepropose thatCOPD patientsshouldbescreened for lung cancer regardless of their smoking history, for early diagnosis.
Nutritionalanomalies,anxiety/depressionand metabolicpathologies
Nutritionalanomalies, metabolicdisturbancesand psycho-logical disorders arethree comorbidity clustersidentified
in COPD.51 The link between COPD and these and other
frequentcomorbiditiesmaybesystemicinflammation due to spillover,66 but this hypothesis remains to be fully
proven.52,67Depressionand/oranxietyarecommoninCOPD
and should be actively sought for, due to their associa-tionwithincreasedriskofexacerbationsandpoorerhealth status.1 LowerBMIis associated withahigher prevalence
ofacuteexacerbations46 andis anindependentriskfactor
formortalityandpoorprognosis.1PatientswithCOPD
fre-quentlyhave oneor severalcomponentsof themetabolic syndromeand/ortype2diabetes,andseveralmechanisms have been proposed to explain the link between COPD andmetabolicdisturbances.However,theyarestillpoorly understood.68 Osteoporosis isalso avery frequent
comor-bidityinCOPD,oftennotdiagnosedespeciallyinmen,and associatedwithpoorhealthstatusandprognosis.
Metabolic and psychological comorbidities should be treated according to the usual guidelines, with special attentiontoBMIinpatientswithsevereCOPD,whichshould notfallbelow21kg/m2.1
We agree that these comorbidities should be actively soughtfor,toallowearlytreatment.COPDpatientswill ben-efitfromamultidisciplinarytreatmentapproach,including nutritionalcounselingand psychologicor psychiatric ther-apy.
Assessing
severity
in
COPD
Thereis aneed for suitableinstruments toassessdisease severity,sothatmoreeffective therapeutic measurescan beapplied. Studies suggest that, although COPD patients withmoresevereairflowlimitationsuffermorerespiratory symptoms,worsequalityoflife andgreatercomorbidities thanthosewithmilderimpairment,lungfunctionalonedoes notadequatelyassesstheimpactofthedisease.35
Neverthe-less,FEV1hastobemeasuredsincespirometryisessential
forthediagnosisofCOPD,toevaluatethedegreeofairflow limitation,1 to monitor disease progression, and to guide
therapy.69 Alow FEV
1 is correlated withan increasedrisk
ofexacerbations1andpoorprognosis.69
Asfortheassessmentofotherparameters,severaltools and other tests are currently available, such as ques-tionnaires. The most comprehensive reliable and valid disease-specific health-related quality of life or health status questionnaires1,34 are the St. George’s Respiratory
Questionnaire (SGRQ)70 and the Chronic Respiratory
Dis-easeQuestionnaire(CRQ).71However,theyarebothlengthy
and have scoring algorithms that are too complexto use inroutineclinicalpractice.1,34 CAT34 or CCQ33 areshorter,
practical,easy touse measuresthat canbe completedin two minutes, and are considered suitable for a compre-hensiveassessmentofsymptoms.1Botharevalidtoassess
healthstatuscomparedtotheextensiveSGRQ,butpatients prefer the CCQ since it reflects their status better than CAT,asithasmoredetailsonbreathingproblems.72 mMRC
assesses only the impact of dyspnea, but it is simple to useandrecommended.1Theinformationprovidedbythese
questionnairesmaybetooscarcetoaccuratelyscoreCOPD severity,butallquestionnaireshavelimitationsandcannot extensivelyincludeallvariablesrelevant toassessdisease severity.Allthesescorescanbeusedbyeveryphysicianthat
dealswithCOPDpatients.Onereportadvisescautionwhen classifying patientsaccording totheGOLD groups,44 since
theclassificationobtained bythemMRCwasnotidentical totheoneobtainedusingCAT.73
Multicomponentindexesincorporateseveraldimensions of COPD.Thethreemost commonlyusedmulticomponent indices are BODE (BMI, FEV1, dyspnea and 6-min walking
distance),30BODEx(BMI,FEV
1,dyspneaandexacerbations)74
andADO (age,dyspnea andFEV1),75 andtheyareall
bet-terpredictors ofmortalityin COPDthanFEV1 alone.6The
BODEindexisconsideredtobethereferenceindex,thebest validatedandofwideruse.However,theneedtoperform the6-minutewalkingtestrendersitimpracticalinprimary care, andin thissetting it canbe replacedbythe BODEx index.74Bothindicesshowahighdegreeofcorrelationand
a similarprognosticcapacityfor predicting mortality.76 In
patientswithmoreseveredisease,theBODEindexshould always be used.14,76 BODE seemsto reflectCOPD severity
betterthanothermultidimensionalgradingsystems,butnot itsclinical heterogeneity.77 The ADO indexseemstohave
abettermedium-andlong-termpredictivereliabilitywhen comparedtootherindices,butafteradjustingforage,BODE andBODExhaveabetterprognosticreliability.14 Moreover,
and although ADO seems adequate to predict survival in COPDpatients,75itneedsvalidationsacrossawiderangeof
diseaseseverities.1TheBODEIndex,mBODE(BODEmodified
ingradingofwalkeddistance),e-BODE(BODEplus exacer-bations),BODExandtheADOindexareallbetterpredictors ofmortalityinCOPDthanFEV1alone.
Otherindexessuch asthe COPDPrognostic index,that predicts mortality, hospitalization, and exacerbation fre-quency, and the SAFE and DOSE (Dyspnea, Obstruction, Smoking,Exacerbation)indexes,whichalsopredict exacer-bations, may be useful6 as well. It has been questioned
whether prediction of mortality rates in patients using indexes such as BODE and ADO truly indicates patient-perceivedseverityandguidesappropriatetreatment,18 but
thisisdebatablesinceotherauthorsarguethat,being mea-surementsofdiseaseseverity,theyareusefulinestablishing prognosisandguidingtherapy.78
All the above mentioned questionnaires and multi-component indexes can be completed during physician appointments and are therefore subject to recall bias. Another problem inherent to the use of questionnaires is thepotentialtogenerateamountsofdatathatarenot pos-sible toprocessand interpretin duetime,thus rendering the effortuseless. A balanceis needed between the use-fulnessoftheinformation,thetimeittakestocollectand process,anditstrueimpactontherapeuticchoices.
There arecurrently noseverity scores adapted to the knownclinicalphenotypesthatcanbeusedtoguide treat-ment. It wouldcertainly be desirable tohave scores that better predict severity in different clinical phenotypes, anditcanbeexpected,giventheheterogeneityofCOPD, that multiple variableswillbe needed for differentCOPD subtypes.19We propose the combination of several
instru-mentstoassessseverityinCOPD:
• FEV1isessential.
• mMRCshouldbeusedtoassesstheimpactofdyspneaon thepatient’sdailylife.
• BODEx can beused ina primary care setting butBODE mustbeusedformoreadvanceddisease,inarespiratory caresetting.
• BothCAT andCCQ arebetterin definingsymptoms,but CAThastheaddedadvantageofassessingdiseaseimpact. • ADOmayalsobeusedincombinationwiththeabove,but
notasastand-aloneindex.
CurrentchallengesregardingCOPDseverityand theroleofexacerbations
SeveralaspectsofCOPDseverityarecurrentlybeing chal-lenged,andthefirstis,perhaps,theroleofexacerbations intheclinicalevolutionofCOPD.
Anexacerbationcanbedefinedas:
• ‘‘an event that leads a care provider to prescribe antibiotics or corticosteroids (or both) or that leads to hospitalization(severeexacerbation)’’;7
• ‘‘aneventthatoftenoccurs,wherethereisarapidand sustainedworseningofsymptomsbeyondnormal day-to-dayvariations’’;32
• ‘‘an acute event characterized by a worsening of the patient’srespiratorysymptomsthatisbeyondnormal day-to-dayvariationsandleadstoachangeinmedication’’.1
Any oftheabove definitionspose challengesfor usein clinicalphenotypingandseverityevaluation.Howlongmust changesinsymptomsbesustainedbeforebeing character-ized as an exacerbation, is it two to three days or less? Moreover,andalthoughtheGOLDdefinitionstates:‘‘leads toachangeinmedication,’’thecriteriainvokedby health-careproviders tojudgewhen toaltermedicationremains unclear. Are these changes in medication quantitative or qualitativeorboth?Importantly,patient-recordedincreases in symptoms that appear tobe exacerbations outnumber thosethatcausethemtopresentformedicalattention.In addition,eventswithworseningsymptomsthatdonotlead patientstoseekadditionalcaremayalsoimpactprognosis.6
Whichclinicalorbiochemicalmarkerscanorshouldbeused to identify or grade severity of exacerbations? These are unfortunatelyunresolvedquestions.
Nevertheless,andregardlessofthedefinition,itis recog-nizedthatexacerbationscontributetotheoverallseverity in individual patients, are associated with an increased mortality,79 the risk of exacerbations increases asairflow
limitationworsens,andhospitalizationforaCOPD exacer-bationisassociatedwithapoorerprognosisandincreased riskofdeath.1
Another important issue is that assessment of disease severity as envisaged in GOLD does not seem adequate. TheGOLDABCDclassificationresultsinveryheterogeneous populations,80 and does not reflectdisease progressionor
mortalityrisk,81,82 assomestudies have shown thatGOLD
B patients may be at a higher mortality risk than GOLD C patients.83 GOLD anticipates that lung function can be
expected toworsen over time,1 but does not specifically
state thatpatients mayswitchbetween GOLDcategories, althoughan analysisfromtheECLIPSEstudyreportedthat patientsmayindeedswitchbetweenanyGOLDcategories.82
Itdoesnotdefinedyspneaasafactorforworseprognosis,
includes subsets of patients defined by low lung function withpatientsdefinedbyfrequentexacerbations,anddoes not value the presence of respiratory failure, which has importantprognosticandtherapeuticimplications.
ThenoninclusionintheGOLDreportofrespiratory fail-ureasacriterionfor diseaseseverity1 canhaveimpactin
clinical practice. Respiratory failure has been historically considered the hallmark of end-stage COPD, and thus, is intrinsically a severity criterion. On the other hand, is it a severity criterion only in the context of end-stage dis-ease, or should respiratory failure bea severity criterion independentofend-stagedisease?
Finally, a patient with COPD is considered to be well controlled who, during follow-up, shows minimal or no symptoms,has had noacute exacerbations sincethe last follow-upvisit, andnoimpairmentin QoLwhile receiving the current treatment.76 Therefore, in the same manner
as severity assessment, disease control should be multi-component.Thereis aneedtointerveneinthesymptoms andbeyond the symptoms,namely usingpharmacological andnon-pharmacologicalapproachesthatreduce therisk, whichmeans,controlthesymptomsandcontrolthedisease beyondthesymptoms.
We acknowledge that GOLD is useful in terms of gen-eralrecommendationsandpublichealth,butdoesnottake intoaccounttheseveralphenotypes,andisnotsufficientto assessmortalityrisk.
Phenotype-based
therapeutic
approach
Information regarding specific therapeutic approaches dependingonthephenotypeisgrowing.TheCanadian guide-lines propose treatment based on frequent or infrequent exacerbations15 and GOLD proposes treatment based on
the risk and symptoms.1 The Spanish guideline proposes
treatmentof COPDbased onfourclinical phenotypesand diseaseseverity.14 Bothphysiologic measures and
patient-reported outcome questionnaires will help identify these patientphenotypesandallowforoptimalpharmacological treatmenttobeimplemented.31
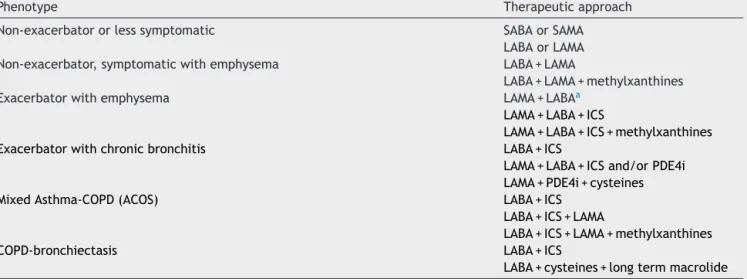
We suggest a phenotype-based pharmacological ther-apeutic approach, considering the six most clinically relevantphenotypeswehaveproposed---Table1.The non-exacerbator and less symptomatic phenotype may start with a bronchodilator that, over time, will preferably bea long-acting medication. In the strongly symptomatic non-exacerbatorwithemphysematheaimshouldbe max-imumbronchodilation.The exacerbatorphenotypeshould be treated first with a long-acting bronchodilator or an associationofbronchodilators,tocontrolsymptoms.Ifnot controlled,atrialofinhaledcorticosteroid(ICS)association is recommended. The ACOS phenotypeshould be treated withLABA/ICSas firstoption. Whenever an ICS is recom-mended, the risk of increased bacterial load84 should be
takenintoconsideration.SpecificICSdruganddoseshould also be appropriately chosen since there is no evidence thatahigherdoseproducesbetterresultsandtheavailable molecules are not equivalent.18,84 The chronic bronchitis
phenotype, if not controlled with the proposed previous treatment, can be treated with a phosphodiesterase-4-inhibitor (PDE4i --- currently not available in Portugal),
Table1 Proposedphenotype-basedpharmacologicaltherapeuticapproach.
Phenotype Therapeuticapproach
Non-exacerbatororlesssymptomatic SABAorSAMA LABAorLAMA Non-exacerbator,symptomaticwithemphysema LABA+LAMA
LABA+LAMA+methylxanthines Exacerbatorwithemphysema LAMA+LABAa
LAMA+LABA+ICS
LAMA+LABA+ICS+methylxanthines
Exacerbatorwithchronicbronchitis LABA+ICS
LAMA+LABA+ICSand/orPDE4i
LAMA+PDE4i+cysteines
MixedAsthma-COPD(ACOS) LABA+ICS
LABA+ICS+LAMA
LABA+ICS+LAMA+methylxanthines
COPD-bronchiectasis LABA+ICS
LABA+cysteines+longtermmacrolide
COPD---ChronicObstructivePulmonaryDisease;ACOS---Asthma-COPDOverlapSyndrome;SABA---short-actingbetaagonist;SAMA--- short-actingmuscarinicantagonist;LABA---long-acting2-agonist;LAMA---long-actingmuscarinicantagonist;ICS---inhaledcorticosteroid; PDE4i--- phosphodiesterase-4-inhibitor.
aAlternativelyincaseofanaïvepatient,caninitiateLAMAorLABAmonotherapy,withashort-termfollow-up,andincaseof non-control,shouldprogresstoLABA+LAMA.
mucoactivedrugs(acetylcysteine,erdosteine)and,if con-sideredineffective,alsowithlong-termoralantibiotics(e.g. azythromycin). In the COPD-bronchiectasis phenotype, a long-termoralantibioticshouldbeconsideredandinhaled antibioticscouldalsobeuseful inpatients withend-stage disease.
All phenotypes will benefit from non-pharmacological measuressuchassmokingcessation,influenzaand pneumo-coccalvaccination,minimumof150min/weekofmoderate tointense physical activity, and pulmonary rehabilitation programs.
The proposed phenotype-based pharmacological ther-apeutic approach should be interpreted as a general recommendation,assometreatment optionsarebasedon expertopinion.Werecommendpatienteducation,including correct inhalation technique, prompt recognition of exa-cerbations,andadoptionofhealthylifestyles.Westrongly recommendthattreatmentshouldbepatient-orientedand notCOPD-oriented.Apatient-tailoredtreatmentapproach, whichtakesintoaccounteach patient’sspecificattributes andspecificities,shouldbepursued.
Ethical
disclosures
Protection of human and animal subjects.The authors
declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethatnopatient dataappearinthisarticle.
Right to privacy and informed consent.The authors
declarethatnopatientdataappearinthisarticle.
Conflict
of
interest
The authors declare collaborating and receiving fees frompharmaceuticalcompaniesotherthanNovartiseither through participation in advisory board or consultancy meetings, congress symposia, clinical trial conduct or investigator-initiatedtrials.
Role
of
funding
source
Funding for thispaperwasprovided byNovartis Portugal. Fundingwasusedtoaccessallnecessaryscientific bibliog-raphyandcovermeetingexpenses.NovartisPortugalhadno roleinthecollection,analysisandinterpretationofdata,in thewritingofthepaperandinthedecisiontosubmitthe paperforpublication.
Acknowledgements
The authors wishtothankNovartis Portugalfor the fund-ingfor this paper,whichwasusedtoaccessallnecessary scientificbibliographyandcovermeetingexpenses.
References
1.GlobalInitiativeforChronicObstructiveLungDisease.Global Strategy for the Diagnosis, Management and Prevention of ChronicObstructivePulmonaryDisease(revised2015). 2.BeehKM,Glaab T,Stowasser S,SchmidtH, FabbriLM,Rabe
KF,etal.Characterisationofexacerbationriskandexacerbator phenotypesinthePOET-COPDtrial.RespirRes.2013;14:116. 3.BurgelPR,PaillasseurJL,CaillaudD,Tillie-LeblondI,ChanezP,
EscamillaR,etal.ClinicalCOPDphenotypes:anovelapproach usingprincipalcomponentandclusteranalyses.EurRespirJ. 2010;36:531---9.
4.BurgelPR,PaillasseurJL,PeeneB,DusserD,RocheN,Coolen J,et al. Twodistinct chronic obstructive pulmonary disease (COPD)phenotypesareassociatedwithhighriskofmortality. PLoSONE.2012;7:e51048.
5.CampPG,Ramirez-VenegasA,SansoresRH,AlvaLF,McDougall JE, SinDD, et al. COPD phenotypes in biomass smoke- ver-sus tobacco smoke-exposed Mexican women. Eur Respir J. 2014;43:725---34.
6.HanMK,AgustiA,CalverleyPM,CelliBR,CrinerG,CurtisJL, etal.Chronicobstructivepulmonarydiseasephenotypes:the futureofCOPD.AmJRespirCritCareMed.2010;182:598---604. 7.Hurst JR, Vestbo J, Anzueto A, Locantore N, Mullerova H, Tal-Singer R, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128---38.
8.Izquierdo-Alonso JL, Rodriguez-Gonzalezmoro JM, de Lucas-RamosP,UnzuetaI,RiberaX,AntonE,etal.Prevalenceand characteristicsofthreeclinicalphenotypesofchronic obstruc-tivepulmonarydisease(COPD).RespirMed.2013;107:724---31. 9.JankowichMD, Rounds SI. Combined pulmonary fibrosis and
emphysemasyndrome:areview.Chest.2012;141:222---31. 10.KimWD,LingSH,CoxsonHO,EnglishJC,YeeJ,LevyRD,etal.
Theassociationbetweensmallairwayobstructionand emphy-semaphenotypesinCOPD.Chest.2007;131:1372---8.
11.KimWJ,HoffmanE,ReillyJ,HershC,DemeoD,WashkoG,etal. AssociationofCOPDcandidategeneswithcomputed tomogra-phyemphysemaand airway phenotypes insevereCOPD.Eur RespirJ.2011;37:39---43.
12.MarshSE,Travers J,WeatherallM,WilliamsMV,AldingtonS, ShirtcliffePM,etal.ProportionalclassificationsofCOPD phen-otypes.Thorax.2008;63:761---7.
13.MatkovicZ,MiravitllesM.ChronicbronchialinfectioninCOPD. Isthereaninfectivephenotype?RespirMed.2013;107:10---22. 14.Miravitlles M,Soler-CatalunaJJ, Calle M,Molina J, Almagro
P,QuintanoJA,etal.SpanishguidelineforCOPD(GesEPOC). Update2014.ArchBronconeumol.2014;50Suppl.1:1---16. 15.O’DonnellDE,AaronS,BourbeauJ,HernandezP,MarciniukDD,
BalterM,etal.CanadianThoracicSocietyrecommendationsfor managementofchronicobstructivepulmonarydisease---2007 update.CanRespirJ.2007;14Suppl.B:5B---32B.
16.Paoletti M, Camiciottoli G, Meoni E, Bigazzi F, Cestelli L, PistolesiM,etal.Explorativedataanalysistechniquesand unsu-pervisedclusteringmethodstosupportclinicalassessmentof ChronicObstructivePulmonaryDisease(COPD)phenotypes.J BiomedInform.2009;42:1013---21.
17.PatalanoF,BanerjiD,D’AndreaP,FogelR,AltmanP,Colthorpe P.AddressingunmetneedsinthetreatmentofCOPD.EurRespir Rev.2014;23:333---44.
18.RabeKF,WedzichaJA.Controversiesintreatmentofchronic obstructivepulmonarydisease.Lancet.2011;378:1038---47. 19.RossiA,ZanardiE.Epluribusplurima:multidimensionalindices
andclinicalphenotypesinCOPD.RespirRes.2011;12:152. 20.StockleyRA.Bronchiectasiswithchronicobstructivepulmonary
disease:associationora furtherphenotype?AmJRespirCrit CareMed.2013;187:786---8.
21.ToraldoDM,DeNuccioF,GaballoA,NicolardiG.Useofcluster analysistodescribedesaturatorphenotypesinCOPD: correla-tionsbetweenpulmonaryfunctiontestsandnocturnaloxygen desaturation.IntJChronObstructPulmDis.2011;6:551---61. 22.OmachiTA,YelinEH,KatzPP,BlancPD,EisnerMD.TheCOPD
severityscore:adynamicpredictiontoolforhealth-care uti-lization.COPD.2008;5:339---46.
23.GlobalInitiativeforChronicObstructiveLungDisease.Global Strategy for the Diagnosis, Management and Prevention of ChronicObstructivePulmonaryDisease(revised2011). 24.SalzmanSH.Whichpulmonaryfunctiontestsbestdifferentiate
betweenCOPDphenotypes?RespirCare.2012;57:50---7, discus-sion58-60.
25.MiravitllesM,CalleM,Soler-CatalunaJJ.Clinicalphenotypesof COPD:identification,definitionandimplicationsforguidelines. ArchBronconeumol.2012;48:86---98.
26.SobradilloP,Garcia-AymerichJ,AgustiA.Clinicalphenotypes ofCOPD.ArchBronconeumol.2010;46Suppl.11:8---11. 27.Miravitlles M, Soler-CatalunaJJ, CalleM, Soriano JB.
Treat-mentofCOPDbyclinicalphenotypes:puttingoldevidenceinto clinicalpractice.EurRespirJ.2013;41:1252---6.
28.Perez T, Mal H, Aguilaniu B, Brillet PY, ChaouatA, Louis R, etal.,COPDandinflammation:statementfromaFrenchexpert group. Phenotypes related to inflammation. Rev Mal Respir. 2011;28:192---215.
29.KaparianosA,SampsonasF,LykourasD,EfremidisG,Drakatos P,KarkouliasK,etal.AssociationofET-1genepolymorphisms withCOPDphenotypesinaCaucasianpopulation.MonaldiArch ChestDis.2011;75:126---31.
30.CelliBR, CoteCG,MarinJM,CasanovaC,Montesde OcaM, Mendez RA,et al.Thebody-massindex, airflowobstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonarydisease.NEnglJMed.2004;350:1005---12.
31.vanderMolenT,MiravitllesM,KocksJW.COPDmanagement: roleofsymptomassessmentinroutineclinicalpractice.IntJ ChronObstructPulmDis.2013;8:461---71.
32.National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adultsin primary and sec-ondary care(partialupdate);2010. http://www.nice.org.uk/ guidance/CG101
33.vander Molen T, Willemse BW, SchokkerS, ten HackenNH, PostmaDS,JuniperEF.Development,validityand responsive-ness of the Clinical COPD Questionnaire. Health Qual Life Outcomes.2003;1:13.
34.JonesPW,HardingG,BerryP,WiklundI,ChenWH,KlineLeidy N.Developmentand firstvalidation oftheCOPD Assessment Test.EurRespirJ.2009;34:648---54.
35.Dransfield MT, Bailey W, Crater G, Emmett A, O’Dell DM, YawnB.Diseaseseverityandsymptomsamongpatients receiv-ing monotherapy for COPD. Prim Care Respir J. 2011;20: 46---53.
36.DecramerM,CelliB,KestenS,LystigT, MehraS,TashkinDP. Effect oftiotropium onoutcomes inpatientswithmoderate chronic obstructive pulmonary disease (UPLIFT): a prespeci-fiedsubgroupanalysisofarandomisedcontrolledtrial.Lancet. 2009;374:1171---8.
37.CelliBR, ThomasNE,AndersonJA, FergusonGT, JenkinsCR, JonesPW,etal.Effectofpharmacotherapyonrateofdecline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med. 2008;178:332---8.
38.Bragman FJ, McClellandJR, ModatM,OurselintS, HurstJR, HawkesDJ.Multi-scaleanalysisofimagingfeaturesanditsuse inthestudyofCOPDexacerbationsusceptiblephenotypes.Med ImageComputComputAssistInterv.2014;17:417---24.
39.FanL,XiaY,GuanY,ZhangTF,LiuSY.Characteristicfeaturesof pulmonaryfunctiontest,CTvolumeanalysisandMRperfusion imaginginCOPDpatientswithdifferentHRCTphenotypes.Clin RespirJ.2014;8:45---54.
40.Galban CJ, HanMK,BoesJL, Chughtai KA, Meyer CR, John-sonTD,etal.Computedtomography-basedbiomarkerprovides uniquesignaturefordiagnosisofCOPDphenotypesanddisease progression.NatMed.2012;18:1711---5.
41.HanselNN, WashkoGR, ForemanMG, HanMK, HoffmanEA, DeMeoDL,etal.RacialdifferencesinCTphenotypesinCOPD. COPD.2013;10:20---7.
42.MohamedHoeseinFA,SchmidtM,MetsOM,GietemaHA, Lam-mers JW,Zanen P,et al. Discriminating dominant computed tomographyphenotypesinsmokerswithoutorwithmildCOPD. RespirMed.2014;108:136---43.
43.Kitaguchi Y,Fujimoto K,Kubo K, HondaT.Characteristicsof COPDphenotypesclassifiedaccordingtothefindingsofHRCT. RespirMed.2006;100:1742---52.
44.GlobalInitiativeforChronicObstructiveLungDisease.Pocket Guide for COPD Diagnosis, Management and Prevention (updated2014).
45.SinDD,AnthonisenNR,SorianoJB,AgustiAG.MortalityinCOPD: roleofcomorbidities.EurRespirJ.2006;28:1245---57.
46.Fumagalli G, Fabiani F, Forte S, Napolitano M, Marinelli P, PalangeP,etal.INDACOproject:apilotstudyonincidenceof comorbiditiesinCOPDpatientsreferredtopneumologyunits. MultidiscipRespirMed.2013;8:28.
47.ChubachiS,NakamuraH,SasakiM,HaraguchiM,MiyazakiM, TakahashiS,etal.PolymorphismofLRP5geneandemphysema severityareassociatedwithosteoporosisinJapanesepatients withoratriskforCOPD.Respirology.2015;20:286---95. 48.Garcia-RioF,SorianoJB,MiravitllesM,MunozL,Duran-Tauleria
E,SanchezG,etal.Impactofobesityontheclinicalprofileof apopulation-basedsamplewithchronicobstructivepulmonary disease.PLOSONE.2014;9:e105220.
49.Martinez CH, HanMK. Contribution of the environment and comorbiditiestochronicobstructivepulmonarydisease pheno-types.MedClinNorthAm.2012;96:713---27.
50.McGarveyL,LeeAJ,RobertsJ,Gruffydd-JonesK,McKnightE, HaughneyJ.Characterisationofthefrequentexacerbator phe-notypeinCOPDpatientsinalargeUKprimarycarepopulation. RespirMed.2014.
51.VanfleterenLE,SpruitMA,GroenenM,GaffronS,vanEmpel VP, BruijnzeelPL, et al. Clusters ofcomorbidities based on validatedobjectivemeasurementsandsystemicinflammation inpatientswithchronicobstructivepulmonarydisease.AmJ RespirCritCareMed.2013;187:728---35.
52.DecramerM,JanssensW.Chronicobstructivepulmonarydisease andcomorbidities.LancetRespirMed.2013;1:73---83. 53.DivoM,CoteC,deTorresJP,CasanovaC,MarinJM,Pinto-Plata
V,etal. Comorbiditiesand riskofmortalityinpatientswith chronicobstructivepulmonarydisease. AmJRespirCritCare Med.2012;186:155---61.
54.CavaillesA,Brinchault-RabinG,DixmierA,GoupilF,Gut-Gobert C,Marchand-AdamS,etal.ComorbiditiesofCOPD.EurRespir Rev.2013;22:454---75.
55.ParkerDR,LiuJ,RobertsMB,EatonCB.Isinflammatorychronic obstructive pulmonary disease a coronary heartdisease risk equivalent?AlongitudinalanalysisofthethirdNationalHealth andNutritionExaminationSurvey(NHANESIII),1988---1994.BMC PulmMed.2014;14:195.
56.WatzH,WaschkiB,MeyerT,KretschmarG,KirstenA,Claussen M, et al. Decreasing cardiac chamber sizes and associated heart dysfunction in COPD: role of hyperinflation. Chest. 2010;138:32---8.
57.Barr RG, Bluemke DA,AhmedFS, Carr JJ,Enright PL, Hoff-manEA,etal. Percentemphysema,airflowobstruction, and impaired left ventricular filling. N Engl J Med. 2010;362: 217---27.
58.WangMT,LoYW,TsaiCL,ChangLC,MaloneDC,ChuCL,etal. StatinuseandriskofCOPDexacerbationrequiring hospitaliza-tion.AmJMed.2013;126,598---606.e2.
59.IngebrigtsenTS,MarottJL,Nordestgaard BG,LangeP,Hallas J, VestboJ. Statinuseand exacerbationsinindividuals with chronicobstructivepulmonarydisease.Thorax.2015;70:33---40. 60.CrinerGJ,ConnettJE,AaronSD,AlbertRK,BaileyWC,Casaburi R, et al. Simvastatin for the preventionof exacerbationsin moderate-to-severeCOPD.NEnglJMed.2014;370:2201---10. 61.FruchterO,YiglaM,KramerMR.Lipidprofileand statinuse:
the paradox of survival afteracute exacerbation of chronic obstructivepulmonarydisease.AmJMedSci.2015.
62.HoughtonAM.MechanisticlinksbetweenCOPDandlungcancer. NatRevCancer.2013;13:233---45.
63.deTorresJP,MarinJM,CasanovaC,CoteC,CarrizoS, Cordoba-LanusE,etal.Lungcancerinpatientswithchronicobstructive pulmonary disease--- incidence and predicting factors. AmJ RespirCritCareMed.2011;184:913---9.
64.LowryKP,GazelleGS,GilmoreME,JohansonC,MunshiV,Choi SE,etal.Personalizingannuallungcancerscreeningforpatients withchronicobstructivepulmonarydisease:adecisionanalysis. Cancer.2015.
65.IlieM,HofmanV,Long-MiraE,SelvaE,VignaudJM,PadovaniB, etal.‘‘Sentinel’’circulatingtumorcellsallowearlydiagnosis oflungcancerinpatientswithchronicobstructivepulmonary disease.PLOSONE.2014;9:e111597.
66.BarnesPJ,CelliBR.Systemicmanifestationsandcomorbidities ofCOPD.EurRespirJ.2009;33:1165---85.
67.WoutersEF,ReynaertNL,DentenerMA,VernooyJH.Systemic andlocalinflammationinasthmaandchronicobstructive pul-monarydisease:is therea connection? ProcAmThoracSoc. 2009;6:638---47.
68.NaikD,JoshiA,PaulTV,ThomasN.Chronicobstructive pul-monarydiseaseandthemetabolicsyndrome:consequencesof adualthreat.IndianJEndocrinolMetab.2014;18:608---16. 69.Direcc¸ãoGeraldeSaúde.Normanr028/2011---Diagnósticoe
TratamentodaDoenc¸aPulmonarObstrutivaCrónica.Portugal; 2013.
70.JonesPW,QuirkFH,BaveystockCM.TheStGeorge’sRespiratory Questionnaire.RespirMed.1991;85Suppl.B:25---31,discussion 33-7.
71.GuyattGH,BermanLB,TownsendM,PugsleySO,ChambersLW. Ameasureofqualityoflifeforclinicaltrialsinchroniclung disease.Thorax.1987;42:773---8.
72.TsiligianniIG,vanderMolenT,MoraitakiD,LopezI,KocksJW, KaragiannisK,etal.AssessinghealthstatusinCOPD.A head-to-headcomparisonbetweentheCOPDassessmenttest(CAT) and the clinical COPD questionnaire (CCQ). BMC Pulm Med. 2012;12:20.
73.KimS, OhJ,Kim YI,BanHJ,Kwon YS,OhIJ, et al. Differ-encesinclassificationofCOPD groupusing COPDassessment test(CAT)ormodifiedMedicalResearchCouncil(mMRC) dys-pneascores:across-sectionalanalyses.BMCPulmMed.2013; 13:35.
74.Soler-CatalunaJJ,Martinez-GarciaMA,SanchezLS,TorderaMP, SanchezPR.SevereexacerbationsandBODEindex:two inde-pendentriskfactorsfordeathinmaleCOPDpatients.Respir Med.2009;103:692---9.
75.Puhan MA, Garcia-Aymerich J, Frey M, ter Riet G, Anto JM, Agusti AG, et al. Expansion of the prognostic assess-mentofpatientswithchronicobstructivepulmonarydisease: the updated BODE index and the ADO index. Lancet. 2009;374:704---11.
76.Molina Paris J. How can we define well-controlled chronic obstructive pulmonary disease? Expert Rev Respir Med. 2013;7:3---15.
77.CamiciottoliG,BigazziF,BartolucciM,CestelliL,PaolettiM, DiciottiS,et al.BODE-index, modifiedBODE-indexand ADO-score in chronic obstructive pulmonary disease: relationship withCOPD phenotypes and CT lung densitychanges. COPD. 2012;9:297---304.
78.AgustiA,CelliB.AvoidingconfusioninCOPD:fromriskfactorsto phenotypestomeasuresofdiseasecharacterisation.EurRespir J.2011;38:749---51.
79.MiravitllesM,IzquierdoI,HerrejonA,TorresJV,BaroE,Borja J,COPDseverityscoreasapredictoroffailureinexacerbations ofCOPD.TheESFERAstudy.RespirMed.2011;105:740---7. 80.Agusti A, Calverley PM, Celli B, Coxson HO, Edwards LD,
LomasDA,etal.CharacterisationofCOPDheterogeneityinthe ECLIPSEcohort.RespirRes.2010;11:122.
81.GoossensLM,LeimerI,MetzdorfN,BeckerK,Rutten-vanMolken MP.Doesthe 2013GOLDclassificationimprovetheability to
predictlungfunction decline,exacerbationsand mortality:a post-hocanalysisofthe4-yearUPLIFT trial.BMC PulmMed. 2014;14:163.
82.Agusti A, Edwards LD, Celli B, Macnee W, Calverley PM, MullerovaH,etal.Characteristics,stabilityand outcomesof the2011GOLDCOPDgroupsintheECLIPSEcohort.EurRespir J.2013;42:636---46.
83.LangeP,MarottJL,VestboJ,OlsenKR,IngebrigtsenTS,Dahl M,etal.Predictionoftheclinicalcourseofchronic obstruc-tivepulmonarydisease, usingthenewGOLDclassification: a studyofthegeneralpopulation.AmJRespirCritCareMed. 2012;186:975---81.
84.AgustiA,FabbriLM.InhaledsteroidsinCOPD:whenshouldthey beused?LancetRespirMed.2014;2:869---71.