O R I G I N A L A R T I C L E UDC: 617.51:616.28-089 DOI: 10.2298/VSP1305463R
The use of total ossicular replacement prosthesis after radical
tympanomastoidectomy
Upotreba totalne osikularne proteze nakon radikalne trepanacije
temporalne kosti
Dejan Ranþiü
Ear, Nose and Throat Clinic, Clinical Center Niš, Niš, Serbia, Faculty of Medicine, University of Niš, Niš, Serbia
Abstract
Background/Aim. This paper presents our operative method for hearing recovery after the previous radical tym-panomasto-idectomy, radical trepanation of the temporal bone (trepanatio radicalis ossis temporalis – TROT) in eight pa-tients submitted to operations for giant cholesteatotoma.
Methods. All the patients were admitted to our clinic after TROT. There were no signs of cholesteatoma or infection. The patients refused any stent implantations or any hearing aids due to possible aesthetic problems. The described pro-cedure developed in two steps. The first one was to restore the destroyed cavum tympany and to covert with chondro-perichondral new membrane with a pin-like “guide” as col-lumela. The second step was to insert a TORP (total os-sicular replacement prosthesis) after guide excision. Re-sults. After the first operation (stage one) there were no in-fections in the operated area nor chondroperichondral graft rejection. Postoperative audiometry (6 to 8 weeks) was done to demonstrate the improvement of air conduction. Three months following the first, the second (stage two) operation was performed and 2.5 to 3 months after this operation even greater audiometry revealed hearing improvement in air- and bone-conduction. The patients were dismissed from
the hospital 2 days after each procedure without any com-plications. They did not experience any dizziness, vomiting nor a severe pain. Three months after the second operative stage, otoscopic findings were very good. The audiometry findings after a 3-months period (after stage one) and 3 months after final TORP insertion was done for each of the patients. After one year, the audiometric curve was the same. Clinical and audiometry follow up demonstrated a hearing recovery and closure of air bone gap (ABG) to val-ues of 5 to 15 dB. Conclusion. The use of TORP after radical tympanomastoidectomy is feasible. The first step of the procedure is the fixation of a neomembrane. A stabi-lized neomembrane is essential for light overpressure on the prosthesis and this is important for optimal or better con-ductivity. A better hearing recovery is confirmed with audi-ometric findings and ABG reduction to 5–15 dB. This method could be performed in all patients (with good bone-conduction) after radical tympanomastoidectomy for better hearing.
Key words:
chaolesteatoma; otologic surgical procedures; hearing loss, conductive; ossicular replacement; prostheses and implants; reconstructive surgical procedures.
Apstrakt
Uvod/Cilj. Ovaj rad predstavlja naš operativni metod za oporavak sluha nakon radikalne timpanomastoidektomije ranije, radikalne trepanacije temporalne kosti (lat. trepanatio radicalis ossis temporalis – TROT) kod osam bolesnika koji su bili ranije operisani zbog džinovskih holesteatoma. Metode.
Svi bolesnici primljeni su u kliniku nakon TROT. Nije bilo znakova holesteatoma ni infekcije. Bolesnici su odbijali bilo kakvu implantaciju ili slušno pomagalo koje bi izazvalo es-tetski problem. Opisana procedura se odvijala u dve faze. Prvo, restauriran je uništeni prostor srednjeg uva i prepokri-ven hondroperihondralnom neomembranom sa „vodiÿem“ nalik na trn, kao kolumelom. Druga faza bila je insercija
to-talne osikularne proteze (TORP) nakon ekscizije „vodiÿa“.
Klini-ÿkim i audiometrijskim praýenjem ustanovljen je slušni opo-ravak od 5 do 15 dB i zatvaranje vazdušno-koštanog proce-pa (air bone gap – ABG). Zakljuÿak. Primena TORP posle radikalne timpanomastoidektomije je moguýa. Prva faza ovog postupka jeste fiksiranje nove membrane. Stabilna no-va membrana no-važna je za blagi nadpritisak na protezu zbog optimalne ili bolje provodljivosti. Bolji sluh potvrdili su au-diometrijski nalazi i smanjenje ABG za 5–15 dB. Ova
me-toda mogla bi se koristiti kod svih bolesnika sa dobrim ko-štanim provoĀenjem posle timpanomastoidektomije za po-stizanje boljeg sluha.
Kljuÿne reÿi:
holesteatom; hirurgija, otološka, procedure; sluh, konduktivni gubitak; slušne košÿice, proteze; proteze i implantati; hirurgija, rekonstruktivna, procedure.
Introduction
By definition, radical trepanation of the temporal bone (trepanatio radicalis ossis temporalis – TROT) includes mastoidectomy, antrotomy, cleansing whole middle ear and closure of the Eustachian tube 1. This operation is also known as radical tympanomastoidectomy. This procedure is often indicated in patients with huge cholesteatoma proc-esses or tumors in middle ear and mastoid region. After TROT the frequency of hearing impairment was high 2.
There are many attempts to improve hearing thereaf-ter3–5. In case of partial defects in ossicular chain, there are different types of tympanoossiculoplasty with partial or total prosthesis in use 6. If there is no ossicle, a total prosthesis must be used.
The cost of these procedures is very high in developing countries and young individuals experience some aesthetic problems in accepting hearing aids.
The aim of this study was to present our original two-step operative method that can help in hearing recovery in patients who refused a hearing aids, and to demonstrate functional results using this method which is a combination of the known methods in otosurgery.
Method
All the 8 patients were admitted to the University Hos-pital with poor hearing in the previously operated ear.
The 8 patients were of both sexes, different age (from 13 to 57 years). All the patients had previously been operated on for cholesteatoma and everyone had made radical timpa-nomastoidectomy, with the epitelized postoperative cavity, and no signs of infection and recurrence of cholesteatoma. All the patients had preserved bone conductivity and con-ductivity air significantly decreased (about 45 dB air-bone gap-ABG). The studied group of patients refused visible hearing aids or implants, and accepted the proposed surgical treatment, although they had been submited to radical tym-panomastoidectomy 3–9 years ago.
Including factors for this type of surgery were: already underwent radical timpanomastoidectomy; no signs of infec-tion and recurrence of cholesteatoma in the postoperative pe-riod; good (preserved) bone conductivity (15–20 dB), ABG greater than 40 dB and the wish to improve hearing without visible hearing aids (for aesthetic reasons). The patients with radical timpanomastoidectomy who wanted total assicular replacement prosthesis (TORP) implantation were not treated due to (excluding factors): suspected infection or recurrence
of cholesteatoma, the lack of preserved bone conduction and small ABG and/or the existence of sensorineural hypacusis.
Our patients were followed clinically and audiometri-caly prior to surgery, after the first phase (about 3 months) and after the set TORP prosthesis (3 months and a year later).
Clinical findings were very good in the years following radical operation. Mastoid CT showed no signs of rest/residual cholesteatoma. There were no recidives of cho-lesteatoma and no signs of infection. Pure tone audiometric examination showed insufficient air conduction. Audiometri-cal examination showed a reduction in air conduction. The patients and their families refused any surgical procedure along with the use of visible hearing aids.
At admission otoscopic findings revealed a wide postop-erative cavity after radical mastoidectomy with good epitheli-zation. There were no signs of infection, nor residual choleste-atoma. Audiometrical findings showed a satisfied bone-conduction (BC) (approx. 25–30 dB in whole frequencies) and poor air-conduction (AC) (approx. 45–55 dB) in the same range.
Inclusion criteria for this method was good postopera-tive bone-conduction (BC) (less than 40 dB) and poor air conduction (AC) (more than 65 dB),
After preoperative planning, the operation was per-formed in two steps. Both operations were perper-formed in gen-eral endotracheal anesthesia.
After local infiltration, through retroauricular incision, the whole epithelized cavity was exposed. The first step of operation was performed through several phases.
At the beginning of operation, de-epithelization of the common cavity after radical trepanation of the temporal bone was performed (Figure 1). Special attention was paid not to
injure the footplate of stapes, promontorium (the first turn of the cochlea) and the facial nerve. The identification and re-opening of the Eustachian tube was of great importance (Figure 2). The aspiration or probe of the Eustachian tube was necessary. Identification of sticky, transparent secret confirmed the right and proper tube position (Figure 3).
Fig. 2 – Identification of the closed Eustachian tube and its opening.
Fig. 3 – Aspiration or a probe into the auditory tube.
Creating a neomembrane was the next step of the pro-cedure to prepare a chondro-peri-chondrial graft from tragus tissue. After the incision on the external ridge of tragus and the exposure of cartilage, a semilunar excision was per-formed. The excised cartilage was separated in the shape of butterfly wings to be used as a neomembrane. One half of the cartilage was trimmed in order to reduce volume and thick-ness. On another part a triangular semiexcision was per-formed where the base of the triangle was fixed to the carti-lage. This triangular cartilage part was seen as a “guide“ (Figure 4).
Fig. 4 – Creation of a neomembrane.
It was important to secure an adequate positioning of the neomembrane with the cartilaginous “guide”. Two marks should be followed: interiorly, above the tubal orifitium and posteriorly, on the facial ridge of temporal bone. The “guide” was positioned in such a way to touch the base of stapes (Figure 5). This “guide” enabled sound conduction and pre-vented collapsing of the neomembrane. The “guide” will fa-cilitate the identification of the stapes footplate and easy ap-plication of a prosthesis.
Fig. 5 – A “guide” must touch the base of the stapes.
At the end of the first step we performed the closure of a neocavum tympani and tamponade of the external auditory canal. The closure was very delicate. The peripheral part of the chondro-perichondrial flap must be fixed under the planned excision during deepithelization and the posterior part must lie on the facial ridge on the anterior part (Figure 6). Good fixation of this kind of graft insured a good aeration and good neomembane elasticity.
Fig. 6 – Closure of the neocavum.
At the end of this procedure the postoperative course was uneventful. Bandages were changed on the third postoperative day. The patients were dismissed from hospital after 6 days.
Three months postoperatively, audiometry showed bet-ter air- and bone-conduction.
probably originates from the Eustachian tube. Also the tip of the “guide” was epithelized at the footplate of stapes. A proximal part of “guide”, fixed to the neomembrane, was cut with micro-scissors and totally removed. A small scratch on the stapes footplate was made. A TORP, model Aerial-Vario by “Kurz“ (Germany) was used. The TORP was subse-quently placed in standard manner.
The second step of the proposed operation was shortly performed in three parts.
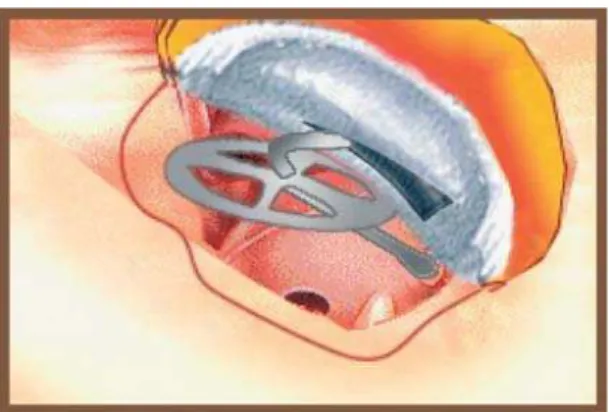
The first part comprised of preparing a tympanomeatal flap 5 mm from the fixed neomembrane border which was very slightly pushed up until the “guide” was exposed. The second part was the removal of the “guide” (Figures 7 and 8). The trapezoid space which remained after removing the „guide“ was very suitable for the placement of the upper part of TORP. The third part was the insertion of TORP in its place.
Fig. 7 – A prosthesis in the place.
Fig. 8 – A prosthesis in the place (intraoperatively).
The statistical methods used in the study were the ANOVA to the chosen significance level and the Dunnett’s test to compare the mean values of the groups. Regression analysis and the significance of differences in the level of air and bone conductivity was performed by ANOVA followed by Dunnett post hoc multiple comparison tests using SPSS software Version 11.5.
Results
After the first operation (stage one) there were no in-fections in the operated area nor chondroperichondral
graft rejection. Postoperative audiometry (6 to 8 weeks) was done to demonstrate the improvement of air conduc-tion.
Three months following the first, the second (stage two) operation was performed and 2.5 to 3 months after this operation even greater audiometry revealed hearing im-provement in AC and BC (Table 1).
Table 1 Air conduction (AC) and bone conduction (BC) preoperatively (Pre OP) and after total ossicular
replacement prosthesis (TORP)
Conductivity Pre OP (dB) After TORP (dB) p AC 68.93 r 10.21 45.6 r 8.71 < 0.0001 BC 40.07 r 8.16 34.28 r 7.85 < 0.0001
The patients were dismissed from the hospital 2 days after each procedure without any complications. They did not experience any dizziness, vomiting nor a severe pain.
Three months after the second operative stage, oto-scopic findings were very good. The audiometry findings after period a 3-months (after stage one) and 3 months after final TORP insertion was done for each of the patients (Fig-ures 9–11).
Fig. 9 – Puretone audiometry preoperatively (PreOP), after stage one (“cavum parvum” – “CP”) and 3 months after the total ossicular replacemnet prosthesis (TORP) insertion.
After one year, the audiometric curve was the same.
Discussion
For the presented patients, the use of this operative mo-dality was based on their wish to improve their hearing, but specifically without the use of any visible hearing aid. This method was developed out of the need to recover hearing in patients with hearing impairment after radical trepanation of temporal bone. It should not be forgotten that for a patient with childhood cholesteatoma this process has some special characteristics 7.
AC BC
Fig. 10 – Puretone audiometry findings: the average for all the patients for air conduction (AC) and bone conduction (BC) preoperatively ( ), after stage one ( ) and 3 months after the surgery ( )
AC – Air conduction properatively (Pre OP), after stage 1 (cavum parvum - CP) and three months after prosthesis insertion (TORP).
BC – bone conduction properatively (Pre OP), after stage 1 (cavum parvum - CP) and three months after prosthesis insertion (TORP).
Fig. 11 – Benefit in air conduction and bone conduction (diagrams show a better conduction in all levels even with tympanoplasty with the “guide”)
Considering different types of tympanoplasty and reported success8, 12, 13 with different ossicular prosthesis 14, 15 the right question is: Who are the suitable candidates and why to use this prosthesis? The patients had good BC but poor AC.
The “Aerial-Vario” prosthesis, in comparison with other prothesis 16 has two characteristics which are very important considering its application in this case. First, the usable length (from the footplate up to a neomembrane) can be easily defined by rolling the upper plate up and down intraoperatively in 0.25 mm increments. Second, the elasticity of a neomembrane (chondroperichondral graft) allows better conductivity.
There are several issues that should be resolved in order to perform this procedure. The problem of a closed tube with a small diameter should be solved by using a diamond burr to make it wider. Finding of a “sticky” tubal secret is a proof that the tubal lumen was found. Curettage of tympanal part of tube should support microvascular and epithelial invasion in „ca-vum par„ca-vum“ (it is expected after 3 months which is the rea-son why the second step should be delayed for this period).
Neomembrane creation differs from other cartilage and/or perichondral grafts 17–20.. It uses a tragal cartilage-perichondral “butterfly-like” graft 21. Its surface and shape
are large enough to cover a future neocavum 15. One half of the cartilage that was orientated posteriorly was of full thick-ness, and that was orientated interiorly was trimmed to the half of its full thickness. One half of the cartilage had been removed to enable better elasticity due to the weight and volume of the graft.
Considerating that patients with chronical otitis could have a tubal dysfunction, the cartilage “guide” (triangular pin-like cartilage part) was used for two reasons. First, to prevent collapsing of the neomembrane and second, for sound conducting effect (columella effect). In case that auditory tube is blocked (mucous, edema, infection) the pin-like guide preserves a constant distance between a neomem-brane and the footplate of stapes, preventing neomemneomem-brane collapse in case of negative pressure. Additionally pine-like “guide” serves as a columella to established/reestablish re-newed cochlear activity to sound stimulation.
The mastoid cavity was not filled or closed because of the ability to view a mastoid part. Of course, filling of mas-toid cavity is possible with bone dust or commercial prepa-rations22–24 as in any “wall-down” tympanoplasty.
The second stage is simple – to cut out the “guide”, re-move it and position a TORP in its place. It is very useful to make 25, a small incision on the stapes footplate to prevent dislocation or migration of the prosthesis. For this reason, the upper part of a prosthesis was placed in an empty triangular space inside of a neomembrane.
Before the first stage, the audiometrical findings showed 25–39 dB of BC and 55 dB of AC. The air-bone conduction gap was 30 dB. Two months after the first stage ABG was 10–20 dB (depending of frequencies). It showed a better value range between 250 Hz and 2 kHz. At this time, BC also showed increased values from 5 dB. It could have been a sign that the cochlear activity was getting better. Af-ter 3 months, the second stage was performed. Three months after the second stage, audiometry showed BC of 20–25 dB; and AC of 30–35 dB; ABG was 5–15 dB.
With the use of TORP, ABG closure was ex-pected 12, 13, 16. A surprising fact was that the bone conduction
was improving. This study sheds a new light on recovery pro-cesses in the cochlea. The reason for it may be found in a bet-ter and more permanent stimulation of cochlea. This is a very good procedure for hearing recovery for patients with good bone-conduction. Compared to other implantable systems it is cheaper and it is followed by good audimetrical findings.
In this case no visible hearing aids were used that was a very significant fact. The cost of the procedure (cheaper than other methods) should not be neglected either.
Conclusion
The use of TORP after radical tympanomastoidectomy is feasible. The first step of the procedure is fixation of a neomembrane. A stabilized neomembrane is essential for light overpressure on the prosthesis and this is important for optimal or better conductivity.
A better hearing recovery is confirmed with audi-ometric findings and ABG reduction to 5–15 dB.
This method could be performed in all patients (with good bone-conduction) after radical tympanomastoidectomy for better hearing.
R E F E R E N C E S
1. Becker W, Naumann HH, Pfaltz CR. Ear, nose and throat diseases Stuttgart: Thieme; 1989.
2. Ragheb SM, Gantz BJ, McCabe BF. Hearing results after choles-teatoma surgery: the Iowa experience. Laryngoscope 1987; 97(11): 1254î63.
3. Federspil PA.Bone anchored hearing aids (BAHA). HNO 2009; 57(3): 216î22. (German)
4. Colletti V, Carner M, Colletti L. TORP vs round window implant for hearing restoration of patients with extensive ossicular chain defect. Acta Otolaryngol 2009; 129(4): 449î52.
5. Kiratzidis T, Arnold W, Iliades T.Veria operation updated. I. The trans-canal wall cochlear implantation. ORL J Otorhinolaryngol Relat Spec 2002; 64(6): 406î12.
6. Schmerber S, Troussier J, Dumas G, Lavieille JP, Nguyen DQ. Hearing results with the titanium ossicular replacement prosthe-sis. Eur Arch Otorhinolaryngol 2006; 263(4): 347î54.
7. Schraff SA, Strasnick B. Pediatric cholesteatoma: a retrospective review. Int J Pediatr Otorhinolaryngol 2006; 70(3): 385î93. 8. Lesinski SG. Reconstruction of hearing when malleus is absent:
TORP vs. homograft TMMI. Laryngoscope 1984; 94(11 Pt 1): 1443î6.
9. Siddiq MA, Raut VV. Early results of titanium ossiculoplasty using the Kurz titanium prosthesis - a UK perspective. J Laryn-gol Otol 2007; 121(6): 539î44.
10. Ho SY, Battista RA, Wiet RJ. Early results with titanium ossicular implants. Otol Neurotol 2003; 24(2): 149î52.
11. Vassbotn FS, Møller P, Silvola J. Short-term results using Kurz ti-tanium ossicular implants. Eur Arch Otorhinolaryngol 2007; 264(1): 21î5.
12. Schmerber S, Troussier J, Dumas G, Lavieille JP, Nguyen DQ. Hearing results with the titanium ossicular replacement prostheses. Eur Arch Otorhinolaryngol 2006; 263(4): 347î54.
13. Alaani A, Raut VV. Kurz titanium prosthesis ossiculoplasty-follow-up statistical analysis of factors affecting one year hearing results. Auris Nasus Larynx 2010; 37(2): 150î4.
14. Fisch U, May J, Linder T, Naumann IC. A new L-shaped titanium prosthesis for total reconstruction of the ossicular chain. Otol Neurotol 2004; 25(6): 891î902.
15. Hales NW, Shakir FA, Saunders JE. Titanium middle ear prosthe-ses in staged ossiculoplasty: does mass really matter? Am J Oto-laryngol 2007; 28(3): 164-7.
16. Schmerber S, Troussier J, Dumas G, Lavieille JP, Nguyen DQ. Hearing results with the titanium ossicular replacement prostheses. Eur Arch Otorhinolaryngol 2006; 263(4): 347î54.
17. Beutner D, Luers JC, Huttenbrink KB. Cartilage 'shoe': a new tech-nique for stabilisation of titanium total ossicular replacement prosthesis at centre of stapes footplate. J Laryngol Otol 2008; 122(7): 682î6.
18. Martin C, Timoshenko AP, Martin C, Bertholon P, Prades JM. Carti-lage and tympanoplasty. Acta Otorhinolaryngol Belg 2004; 58(4): 143î9.
19. Yung M. Cartilage tympanoplasty: literature review. J Laryngol Otol. 2008; 122(7): 663î72.
20. Chiossone E. "Three cartilages" technique in intact canal wall tympanoplasty to prevent recurrent cholesteatoma. Am J Otol 1985; 6(4): 326î30.
21. Ghanem MA, Monroy A, Alizade FS, Nicolau Y, Eavey RD. Butter-fly cartilage graft inlay tympanoplasty for large perforations. La-ryngoscope 2006; 116(10): 1813î6.
22. Leatherman BD, Dornhoffer JL. The use of demineralized bone matrix for mastoid cavity obliteration. Otol Neurotol 2004; 25(1): 22î5; discussion 25î6.
23. Magliulo G, Ronzoni R, Vingolo GM, Cristofari P. Reconstruction of old radical cavities. Am J Otol 1992; 13(3): 288î91.
24. Ikeda M, Yoshida S, Ikui A, Shigihara S. Canal wall down tympa-noplasty with canal reconstruction for middle-ear cholesteatoma: post-operative hearing, cholesteatoma recurrence, and status of re-aeration of reconstructed middle-ear cavity. J Laryngol Otol 2003; 117(4): 249î55.
25. Babighian GG, Albu S. Failures in stapedotomy for otosclerosis. Otolaryngol Head Neck Surg 2009; 141(3): 395î400.