www.jped.com.br
ORIGINAL
ARTICLE
Effects
of
programmed
physical
activity
on
body
composition
in
post-pubertal
schoolchildren
夽
Edson
dos
Santos
Farias
a,b,c,∗,
Ezequiel
Moreira
Gonc
¸alves
b,d,
André
Moreno
Morcillo
e,
Gil
Guerra-Júnior
d,e,
Olga
Maria
Silverio
Amancio
aaDepartmentofPediatrics,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil bFaculdadedeCiênciasMédicas(FCM),UniversidadeEstadualdeCampinas(UNICAMP),SãoPaulo,SP,Brazil
cUniversidadeFederaldeRondônia(UNIR),Pioneiro,RO,Brazil
dLaboratoryofGrowthandBodyComposition,CentrodeInvestigac¸ãoemPediatria(CIPED),FaculdadedeCiênciasMédicas,
UniversidadeEstadualdeCampinas(UNICAMP),SãoPaulo,SP,Brazil
eDepartmentofPediatrics,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(UNICAMP),SãoPaulo,SP,Brazil
Received22October2013;accepted5June2014 Availableonline13October2014
KEYWORDS Motoractivity; Schoolhealth; Bodycomposition; Overweight; Obesity
Abstract
Objective: To assess body composition modifications in post-pubertal schoolchildren after practiceofaphysicalactivityprogramduringoneschoolyear.
Methods: Thesampleconsistedof386studentsagedbetween15and17yearsanddividedinto twogroups:thestudygroup(SG)comprised195studentsandthecontrolgroup(CG),191.The SGwassubmittedtoaphysicalactivityprogramandtheCGattendedconventionalphysical educationclasses.Bodycompositionwasassessedusingbodymassindex(BMI),percentageof bodyfat(%BF),fatmass(FM),andleanmass(LM).
Results: A positive effect ofthe physical activity program on body composition inthe SG (p<0.001)wasobserved,aswellasontheinteractiontimexgroupinallthevariablesanalyzed inbothgenders.Areductionin%BF(meanofdifferences=-5.58%)andwaistcircumference (-2.33cm),aswellasanincreaseinLM(+2.05kg)wereobservedintheSGforbothgenders, whereastheoppositewasobservedintheCG.
Conclusion: Thepractice ofprogrammedphysicalactivitypromotes significantreductionof bodyfatinpost-pubertalschoolchildren.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:FariasES,Gonc¸alvesEM,MorcilloAM,Guerra-JúniorG,AmancioOM.EffectsofProgrammedphysicalactivity
onbodycompositioninpost-pubertalschoolchildren.JPediatr(RioJ).2015;91:122---9.
∗Correspondingauthor.
E-mails:[email protected],[email protected](E.d.S.Farias). http://dx.doi.org/10.1016/j.jped.2014.06.004
Effectsofprogrammedphysicalactivityinschoolchildren 123
PALAVRAS-CHAVE Atividademotora; Saúdeescolar; Composic¸ãocorporal; Sobrepeso;
Obesidade
Efeitodaatividadefísicaprogramadasobreacomposic¸ãocorporalemescolares
pós-púberes
Resumo
Objetivo: Verificar asmodificac¸õesdacomposic¸ãocorporal deescolarespós-púberesapósa práticadaatividadefísicaprogramadaduranteumanoletivo.
Método: Amostracompostade386alunos,divididosemdoisgrupos:estudo195econtrole191, comidadeentre15e17anos,ogrupoestudo(GE)submetidoàatividadefísicaprogramada eogrupocontrole(GC)aaulasconvencionaisdeeducac¸ãofísica.Acomposic¸ãocorporalfoi avaliadapeloíndicedemassacorporal(IMC),percentualdegordura(%G)emassagorda(MG) emagra(MM).
Resultados: Foipossívelobservarum efeitopositivodoprogramadeatividadefísicasobrea composic¸ão corporal noGE (p<0,001) dogrupoe dainterac¸ãotempo x grupoem todas as variáveisanalisadasemambosossexos.Foiobservadasreduc¸õesna%G(médiadasdiferenc¸as =-5,58%)enoperímetrodacintura(-2,33cm),aumentodaMM(+2,05kg)noGEemambosos sexos,ocontráriofoiobservadonoGC.
Conclusão: Apráticadeatividadefísicaprogramadapromovereduc¸ãosignificativadegordura corporalemescolarespós-púberes.
©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Physicalactivitycanhaveitsmostsignificanteffectonthe prevention,ratherthanonthetreatment ofobesity.That wastheconclusionoftheauthorsofastudyconductedfor fifteen weekswith obesepatients whowalked45minutes fivedaysaweek.Fortheauthors,thefactorsthatleadto obesityarefamilyinfluence,caloricdietshighinfats,and insufficientenergyexpenditure.1
The problemfor those treating obesity is that,shortly after the end of treatment, conditions return to previ-ous proportions. This is probably due to non-adherence to regular physical activity habits or unhealthy diet, or both.2
Theapproachforpreventingandtreatingexcessweight in children and adolescents involves changes in lifestyle, includingdietandphysical activity,notonly inrelationto thechild or adolescent, butalsoin relation tothefamily andtotheschoolanditssurroundings.
Some studies have addressed the effects of interven-tionprogramsinsideandoutsidetheschoolonbodyweight controlandhealthofchildrenandadolescentswithexcess weight. An eight-month intervention program conducted in 18 schools in the Netherlands included an individual educational program consisting of 11 biology and physi-cal education classes to induce changes in energy intake and expenditure, additional physical education classes, and changes in school cafeterias. After the intervention period, significant positive changes in body composition of the adolescents submitted to the intervention were observed.3
Therefore, physical activity can produce significant changes in body composition and lean mass (LM), and is animportantfactorinthecontrolofexcessweightin chil-drenandadolescents,leadingtoadecreaseinpsychosocial disorders,depression,isolation,lowself-esteem,andlater
exerting a positive influence on hypertension, diabetes, andcardiovasculardisease.4Ameta-analysisevaluatingthe treatmentofpediatricobesityevidencedthelimitedeffects of short-term drug interventions and changes in lifestyle (less than six months of treatment).5 Nevertheless, stud-iesonlong-terminterventions(morethan12months)have shown promising results of physical activity influence on lifestylechanges in and,consequently, bodycomposition, bothforpreventionandtreatmentofexcessweightin chil-drenandadolescents.6,7
Therefore,thisstudy aimedtoinvestigate thechanges inbodycompositioninpost-pubertalschoolchildrenaftera programmedphysical activityinterventionimplementedin physicaleducationclassesduringoneschoolyear.
Methods
This was a simple randomized clinical trial conducted by pairing grades/classes of post-pubertal schoolchildren attendingthefirsttothethirdyearofhighschoolof Colé-gio Meta, Rio Branco, AC, Brazil, aged 15 to 17 years, during the 2011 school year. This study was approved by theEthicsCommitteeofUniversidadeFederaldeSãoPaulo (Edict1073/10)andbytheprincipaloftheschool,afteran informedconsent was obtained from the schoolchildren’s parentsorguardians.
Exclusioncriteria
Samplingprocedures
thepopulation ofpost-pubertalschoolchildren enrolledin highschoolin2011consistedof567studentsdistributedin 10classes(first,second,andthirdyears).Thestratification processoccurredbysimpledrawing(simplerandomization) ingrades/classes, dividedintotwo strata (study[SG] and control[CG]),pairingfiveclasses foreach group,totaling 283 and 284 students in each stratum. This number was reducedduetotheevents thatledtothe lossof181 stu-dents.Thefinalstudypopulationconsistedof386students, 195intheSGand191intheCG,estimatingaprobabilityof typeIerror(␣)of0.05andaprobabilityoftypeIIerror() of80%.
Intervention
bothgroupshadtwophysicaleducationclassesweekly, last-ing60minuteseach. Eachclasshad 83physical education classes, totaling 415 annual classes. Students in the CG performed the usual physical activity at school, such as recreationandgamesthroughexercises,calisthenics, learn-ingthe fundamentalsof sports, andsports activities. The studentsinthe SGunderwentprogrammedphysical activ-ity withheart rate monitoring, consisting of three parts: aerobicactivity(exercisesforflexibility,muscularstrength, jumping rope, walking, alternating running, continuous jumping, recreational games), lasting 30minutes; sports games(volleyball,soccer,handball),lasting20minutes;and withstretching,lasting10minutes.
Measurements
theheartrate(HR)ofeachstudentwasmonitoredthrougha heartratemonitor(PM25-Beurer,BeurerGmbH,Germany). Exerciseintensitywasbasedonindications for the appro-priatelevelofphysicalactivitytoachievebestfat-burning efficiency,whichcomprisestherangeof>55%maximumHR (HRmax).8HRmeasurementwasperformedthrougha follow-uprecord,accordingtothefollowingcriteria:theHRofthe studentbeingmonitoredwasrecordedevery10minutes dur-inga60-minuteclass;allstudentswereregularlymonitored throughoutthecourseofstudy.Whennecessary, interven-tionswereperformedduringtheactivitiesinordertocontrol exercise intensity, aiming at keeping the exercise within theindividual target zone of > 55% HRmax as long as
pos-sible.
Socioeconomic level was assessed through a question-naire,using the classification of the Brazilian Association ofResearchCompanies(ABEP),9dividingthestudents into ClassA(upperclass)andB(medium-upperclass).
Maturationstagewasself-assessedthroughphotographs andwrittendescriptionofthefivestagesofbreast develop-mentforfemales(B1-B5)andgonadsformales(G1-G5), accordingtoMarshall&Tanner,10,11inwhichstudentswere askedtochoosethepicturethatmostaccuratelyreflected their own stage of development. Males were considered post-pubertalatG5andfemalesatB4withmenarche.
Ageatmenarchewasassessedbyaprospectivemethod throughtwodirectquestions:‘‘a)Haveyouever menstru-ated?’’;andb) ‘‘If so,doyou rememberthe day, month,
andyearyoumenstruatedforthefirsttime?’’Ifatleastthe month andyearofmenarche couldberecalled,the infor-mationwasconsideredvalid;otherwise,thesubjectwould beexcludedfromthestudy.
Theprocedureforquestionnairesapplicationwasalways thesame.The researcherandtheclassteacherwereboth inthe classroom,each questionwasreadandthestudent (respondent)answered.Sexualmaturationassessmentwas performedinaprivateroom.
Bodycompositionwasassessedthroughmeasurementsof weight(kg),height(cm),subscapular(SSSF,mm)andtriceps skinfold(TSF,mm),sumofskinfolds(2SF),andwaist cir-cumference(WC,cm),accordingtothestandardizationby Petroski.12
Based on weight and height measurements, the body massindex(BMI)wascalculatedasweight(kg)/height(m2).
Subsequently,excessweightwasdefinedbasedontheWorld Health Organization (WHO) recommendations,considering assuch(overweightandobesity)thosestudentswithZ-score ≥1.0.13
Thepercentageofbodyfat(%BF)wascalculatedbased onequationsdevelopedbySlaughteretal.,14usingTSFand SSSF andtaking intoaccountgender, ethnicity(whiteand black),andsexualmaturation.
Behnke&Wilmore’sformulawasusedtocalculatethefat mass(FM,kg) andLM(kg):15 FM=weight(kg)x(%BF/100) andLM=weight-FM.
Datawereanalyzed using PASWsoftwarefor Windows, release18.0 (SPSSInc.,IBMCompany, Chicago,USA).The chi-squaredtestwasusedtoverifytheassociationbetween SGandCGregardingage,gender,andsocioeconomicgroup. ThenonparametricMann-Whitneytestwasappliedto com-pareagesbetweenthetwogroups.Thedependentvariables (weight, height, BMI, SSSF, TSF, %BF, LM, FM, and WC) were not normally distributed after assessment by the Kolmogorov-Smirnov test. Data were transformed by the Blom formula and the standardized scores resulting from this transformation werenormally distributed. Forpaired samples,Student’st-testwasusedforcomparisonsbetween pre-andpost-momentswithineachvariablebetweenthe SGandCGandwithineachgroup.
Mauchly’stestwasusedforanalysisofsphericity.Analysis ofvarianceforrepeatedmeasureswasperformedforintra andinter-groupcomparisonsofbodycomposition.Asthese variables (FM,LM, andWC) differedsignificantly between groups atthepre-interventionmoment,comparisonswere adjustedforbaselinevalues,whichwereusedascovariates. The posthocBonferroni test wasusedtoidentify specific differencesinvariablesofwhichFvalueswerehigherthan the established statistical significance criterion (p<0.05). The chi-squared test was used to compare the associa-tionsbetweenexcessweight(overweightandobesity)and non-obeseschoolchildrenbetweentheassessments.The sig-nificancelevelwassetat5%.
Results
Effectsofprogrammedphysicalactivityinschoolchildren 125
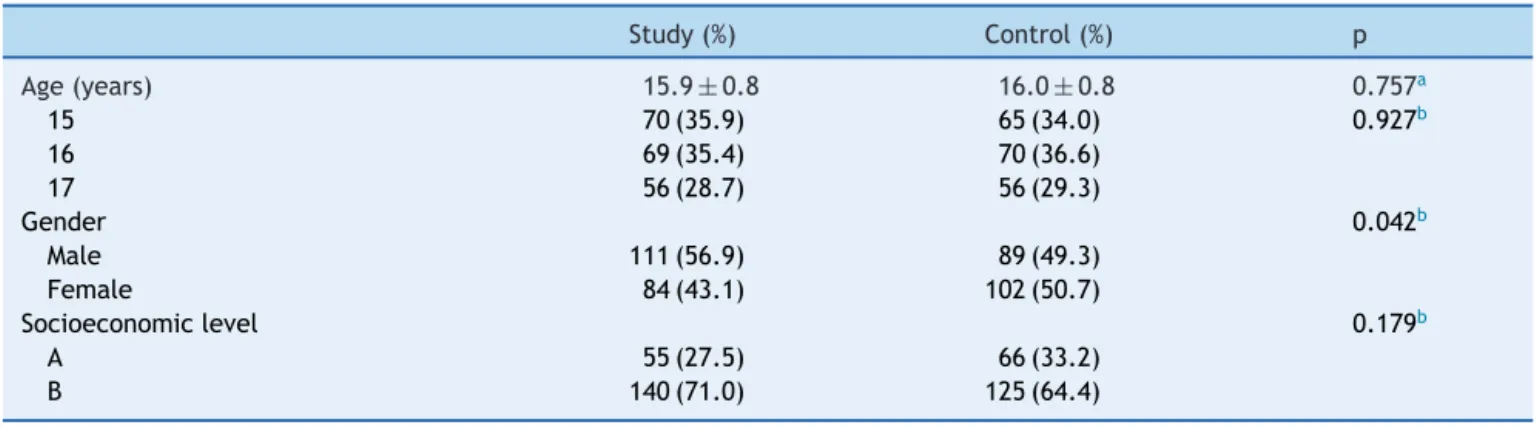
Table1 Characteristicsofschoolchildreninthestudyandcontrolgroups.
Study(%) Control(%) p
Age(years) 15.9±0.8 16.0±0.8 0.757a
15 70(35.9) 65(34.0) 0.927b
16 69(35.4) 70(36.6)
17 56(28.7) 56(29.3)
Gender 0.042b
Male 111(56.9) 89(49.3)
Female 84(43.1) 102(50.7)
Socioeconomiclevel 0.179b
A 55(27.5) 66(33.2)
B 140(71.0) 125(64.4)
a Mann-Whitneytest.
b Chi-squaredtest.
(Table1).Table2showsthegeneralcharacteristicsof the groupsinthepre-interventionperiod.Malesubjectsinthe CGweresignificantlytaller,heavier,andhadmoreleanbody mass(p<0.01),whencomparedtoindividualsintheSG.In contrast,malesintheSGhadhigherlevelsofadiposity,with significantlyhighervaluesinthe2SFandtheamountof rel-ativeandabsolutebodyfat.Comparisonsbetweenfemale subjects fromboth groups showed the opposite behavior, in which the control group had a higher amount of body fat(2SF,%BF,andfatmass),whereasthestudygrouphad higherLM.
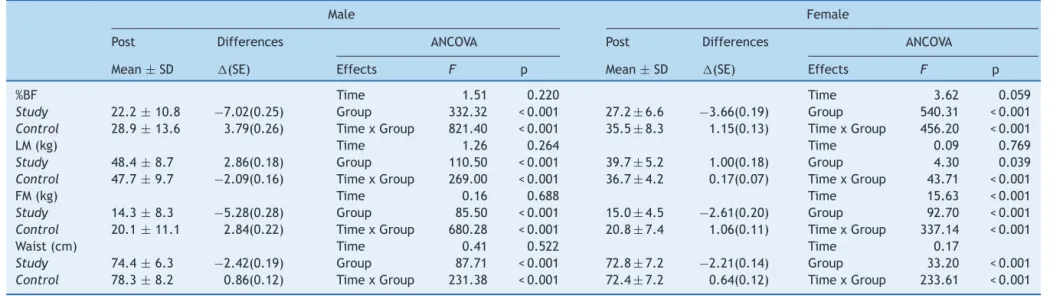
Apositiveeffectofthephysicalactivityprogramonbody compositionofadolescentsinthegroupswasobserved, ver-ified by thesignificant effect(p<0.001) of thegroup and theofinteractiontimexgroupinallvariablesanalyzedin both genders. Reductions in bodyfat (%BF andtotal) and WC,aswellasanincreaseinLMwereobservedintheSGin bothgenders,whereastheoppositewasobservedintheCG (Table3).
Table 4shows the frequency ofcases of excessweight (overweight and obesity) according toBMI z-score in the studyandcontrolgroupsbeforeandaftertheintervention.
There was no significant difference in the excess weight group(>0.176)inthepre-test.Therewasasignificant dif-ferenceinthepost-test,withadecreaseinthenumberof casesofexcessweight(<0.001).
Discussion
Thestudypopulationconsistedofpost-pubertal schoolchil-dren,consideringthatduringpubertychangesdonotalways occurin suchagradual manner duetometabolic adapta-tionsgeneratedduringthetrainingprocess,andmainlydue tochangesingrowthandbodycomposition,characteristic ofthegrowthspurt.
When comparingaccordingtogender, themales inthe SGshowedasignificantreductioninthevariables%BFand FM,as well as an increase in LM, confirming that during puberty,thehormonalinfluenceandthelessactivelifestyle givefemalesatendencytohigherfataccumulation,16i.e., whileinfemalesthereisamoremarkedincreaseinFMdue totheactionofprogesteroneandestrogen,inmalesthere isanincreaseinLMduetotestosterone.17
Table 2 General characteristicsof the groups in the pre-interventionperiod. Valuesare expressed as mean ± standard deviation.
Male Female Total
Study Control Study Control Study Control
Weight(kg) 65.1±11.7 67.1±10.0a 56.3±8.1 56.3±8.4 61.3±11.2 61.3±10.6 Height(cm) 171.8±7.9 173.4±6.4a 161.4±6.1 161.1±5.3 167.3±8.8 166.8±8.5 BMI(kg/m2) 21.9±3.2 22.3±2.9 21.6±2.8 21.6±2.8 21.8±3.0 21.9±2.9
zBMI 0.4±1.0 0.3±0.9 0.3±0.8 0.2±0.9 0.3±0.9 0.3±0.9
2SF(mm) 36.3±13.4a 31.6±15.0a 39.4±12.7a 45.7±14.6a 37.6±13.1 39.1±16.4
%BF 29.2±11.1a 25.1±12.6a 30.9±7.4a 34.3±8.5a 29.9±9.7 30.0±11.5 LM(kg) 45.5±8.9a 49.8±9.6a 38.7±5.6b 36.5±4.4b 42.6±8.3 42.7±9.9 FM(kg) 19.5±9.7b 17.3±9.9b 17.6±5.9b 19.8±7.2b 18.7±8.3 18.6±8.6 Waist(cm) 76.9±7.2 77.4±8.0 76.1±7.5b 74.4±8.2b 75.0±7.9a 71.8±7.5a
BMI,bodymassindex;zBMI,z-scoreofbodymassindex;2SF,sumofskinfolds;%BF,percentageofbodyfat;LM,leanmass;FM,fat
mass.
a Statisticallysignificantdifferencesbetweenthestudyandcontrolgroups,p<0.01,Student’st-testforindependentsamples(Blom
transformation).
b Statisticallysignificantdifferencesbetweenthestudyandcontrolgroups,p<0.05,Student’st-testforindependentsamples(Blom
Farias
ES
et
al.
Table3 Comparisonofbodycompositioninchildrenaftertheinterventionperiod.
Male Female
Post Differences ANCOVA Post Differences ANCOVA
Mean±SD (SE) Effects F p Mean±SD (SE) Effects F p
%BF Time 1.51 0.220 Time 3.62 0.059
Study 22.2±10.8 −7.02(0.25) Group 332.32 <0.001 27.2±6.6 −3.66(0.19) Group 540.31 <0.001 Control 28.9±13.6 3.79(0.26) TimexGroup 821.40 <0.001 35.5±8.3 1.15(0.13) TimexGroup 456.20 <0.001
LM(kg) Time 1.26 0.264 Time 0.09 0.769
Study 48.4±8.7 2.86(0.18) Group 110.50 <0.001 39.7±5.2 1.00(0.18) Group 4.30 0.039 Control 47.7±9.7 −2.09(0.16) TimexGroup 269.00 <0.001 36.7±4.2 0.17(0.07) TimexGroup 43.71 <0.001
FM(kg) Time 0.16 0.688 Time 15.63 <0.001
Study 14.3±8.3 −5.28(0.28) Group 85.50 <0.001 15.0±4.5 −2.61(0.20) Group 92.70 <0.001 Control 20.1±11.1 2.84(0.22) TimexGroup 680.28 <0.001 20.8±7.4 1.06(0.11) TimexGroup 337.14 <0.001
Waist(cm) Time 0.41 0.522 Time 0.17
Study 74.4±6.3 −2.42(0.19) Group 87.71 <0.001 72.8±7.2 −2.21(0.14) Group 33.20 <0.001 Control 78.3±8.2 0.86(0.12) TimexGroup 231.38 <0.001 72.4±7.2 0.64(0.12) TimexGroup 233.61 <0.001
Effectsofprogrammedphysicalactivityinschoolchildren 127
Table4 Numberofschoolchildrenintheexcessweight(overweightandobesity)andnon-obesestudygroupinthepre-and post-interventionperiods.
Pre
Study Control Total
n(%) n(%) n(%) pa
Non-Obese 135(69.2) 144(75.4) 279(72.3)
Excessweight 60(30.8) 47(24.6) 107(27.7) 0.176
Total 195(100.0) 191(100.0) 386(100.0)
Post
Non-Obese 190(97.4) 145(75.9) 335(86.8)
Excessweight 05(2.6) 46(24.1) 51(13.2) <0.001
Total 195(100.0) 191(100.0) 386(100.0)
a Chi-squaredtest.
The programmed physical activity in the SG led to changesinthevariablesofbodycompositionnotobservedin theCG,i.e.,asignificantdecreaseinbodyadiposity, repre-sentedby2SF,%BF,andFM.Similarresultshavealsobeen observedbyotherauthors.18,19
Thereisnodoubtregardingthebenefitsofphysical activ-ityforhealth.EstimatesoftheWorldHealthReportindicate thatapproximately3%oftheglobalburdenofheartdisease and10%ofstrokesareduetophysicalinactivity.20Thesame documentindicatesthatphysicalinactivityisamongtheten leadingcausesofmorbidityanddisabilityinthedeveloped world.TheWHOestimatesthatapproximatelytwomillion deathsworldwidearecausedbyphysicalinactivity.21
Basedonthereviewofmorethan850articles,itis rec-ommendedthatindividualsofschoolage(6-18years)should practice60minutesormoreofmoderatetovigorousphysical activityeverydayoftheweek.22
Despite all the benefits provided by regular physical activity,theWHOreportof200223 statedthataround17% of theworldpopulation practicesnophysical activity and approximately60%donotmeetthecriteriatobeconsidered physicallyactive(150minutesaweek).
As demonstrated by meta-analyses,6,24 several studies have sought toinvestigate the effectof physical training onimprovingthepreventionofexcessweightanddifferent components of body composition in children and adoles-cents.
Thepresentstudyobservedasignificantdecreasein%BF andFMintheSGwhencomparedtotheCG,demonstrating thata physicalactivity programwithfrequency,duration, andintensitycontrolpromotedgreaterenergyexpenditure andusedbodyfatasthemainsubstrate,25,26 resultingina significantreductionofFMduringoneschoolyear.
Theprogrammedphysicalactivity,withfrequency, dura-tion, and intensity control, was of utmost importance to achievepositiveresults.Harrisetal.,24 inameta-analysis that evaluated the effect of interventions with physi-cal activity on FM in schoolchildren, demonstrated that whentheinterventionlastedmorethanthreemonthsand wascombinedwithnutritionaleducation,theresultswere moresignificantregardingFMreduction.Thisindicatesthat strategiestoreduceandpreventexcessweightshouldfocus onadequate food intakeand caloricexpenditure through
motoractivity,aspectsthatshouldbeconsideredwhen plan-ningpublicpoliciesinhealthcare.
Thechangesobservedin2SF,%BF,andFMintheSGare similartoliteratureresultsinadolescents.3Physicalactivity aloneproducesa modestreductionin bodyfat, butwhen physical activityis performed in a controlledmanner and withincreasedintensity,itcanpromoteasignificant reduc-tionin fat oxidation, both visceral and subcutaneous,27,28 mainlywhen theindividualis overweight.It is well docu-mentedthatphysicalactivityhelpsburningbodyfat.3,29
Theintensityofphysical activityappearstobedirectly related to fat loss, as higher-intensity activity results in greater calorie burn, leading tosignificant fat reduction. Exerciseintensityaffectsthemagnitudeofthepost-activity metabolicrateincreasemorethanthedurationofthe exer-cise.Therefore,thephysicalactivityintensityshouldalways beincreasing,astheinsufficientlyactiveand/orsedentary individualisnotabletoperformatthebeginningoftraining ahigh-intensityactivitytoproduceaprolongedincreasein post-physicalactivityenergyexpenditure.27Physicalactivity intensityisa keyfactor toachievebetteroutcomes,both inphysicalconditioning andreductionbodyfat.Thus,the intensity of the programmed physical activity may be an explanationfor the differenceof what occurred between theSGandCG,andthisintensitywaseffectiveinreducing bodyfatintheSG.
This study demonstrated a significant increase in LM betweenthepre-andpost-interventionperiodsinboth gen-dersintheSG,andremainedwithoutasignificantdifference intheCG.Hardyetal.28showedthatastrengthtraining pro-grammaybeincludedinthetreatmentofadolescentswith excessweight,astheyresultinareductionof FM. Proba-blytheresultobservedintheSGwasaconsequenceofthe developmentofmusclestrengthactivity,withasignificant increaseinLM.ThisincreaseinLMwaspossiblyinfluencedby themusclestrengthworkoutofupperandlowerlimbswith increasedload.Therefore,musclestrengthactivitymaybe associated with the positive effect that the programmed physicalactivityhadonLM,directly,whichisinaccordance withthepreviousliteratureresults.29
disease.AsignificantdecreaseinWCwasobservedintheSG andmalegender.Thisresultisprobablyrelatedtothe differ-entfunctionalandmorphologicalcharacteristicsofthemale genderandthefactthattheyaremorephysicallyactive.
As expected, and as a consequence of the results observed in body composition variables, a significant decreasein thefrequency of excess weightwasobserved onlyintheSG.
Studiesontheeffectsofphysicalactivityinterventionon bodycomposition(weight,FMindex,skinfolds,%BF,FM,and waist)shouldbeinterpretedwithcaution,astheassessment ofthenutritionalstatususingtheseindicesduringpuberty hasshownmorphologicaldifferencesbetweenthegenders, mainlyduringthesexualmaturationstage.Changesinbody massmaybe typicalof acertainstageof maturationand nottheresultofdietaryintakeandphysicalactivitylevels. Theseindices,althoughtheydonotindicatebody compo-sition, are easy tomeasure, and the wide availability of dataonbodyheightandweight,inadditiontotheir associ-ationwithmorbidityandmortality,justifiestheiruseasan indicatorofnutritionalstatusinepidemiologicalstudies.30
Gonc¸alves etal.30 emphasize that,for epidemiologists, body composition changes have environmental explana-tions,‘‘as,inrecenttimes,itisveryunlikelythatsubstantial changes have occurred in the genetic characteristics of populations,whilechangesintheirhabitsoflifeappearto havebeenhuge.’’
Better adherence tophysical activity at school, rather thanaloneoringyms,canresultinfavorablestimulitothe overallhealthofchildren/adolescentsthroughmore effec-tiveprograms withmoreambitious targets thatstimulate theseyoung individualstoovercomeobstacles toattaina healthieradulthood,withfewerhealthproblemsrelatedto excessweight.
Therefore, it can be concluded that, in the SG, the regularpracticeofprogrammedphysicalactivity,with fre-quency,duration, andintensity control, conductedduring theschoolyear,resulted inasignificantreductionofbody fatinpost-pubertaladolescents.
Funding
CNPq(Conselho Nacionalde Desenvolvimento Científico e Tecnológico)---processn.475959/2010-8.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Thivel D,BlundellJE, DuchéP, Morio B.Acute exercise and subsequentnutritionaladaptations:whataboutobeseyouths? SportsMed.2012;42:607---13.
2.WangN,XuF,ZhengLQ,ZhangXG,LiY,SunGZ,etal.Effects oftelevisionviewingonbodyfatnessamongChinesechildren andadolescents.ChinMedJ(Engl).2012;125:1500---3.
3.SinghAS,ChinA,PawMJ,BrugJ,vanMechelenW.Short-term effectsofschool-basedweightgainpreventionamong adoles-cents.ArchPediatrAdolescMed.2007;161:565---71.
4.de Ferranti S, Mozaffarian D. The perfect storm: obesity, adipocyte dysfunction, and metabolic consequences. Clin Chem.2008;54:945---55.
5.McGovern L, Johnson JN, Paulo R, Hettinger A, Singhal V, KamathC,etal.Clinicalreview:treatmentofpediatricobesity: asystematicreviewandmeta-analysisofrandomizedtrials.J ClinEndocrinolMetab.2008;93:4600---5.
6.Farias ES, Paula F, Carvalho WR, Gonc¸alves EM, Baldin AD, Guerra-JúniorG.Influenceofprogrammedphysicalactivityon bodycompositionamongadolescentstudents.JPediatr(RioJ). 2009;85:28---34.
7.OrtegaFB,RuizJR,CastilloMJ,SjöströmM.Physicalfitnessin childhoodandadolescence:apowerfulmarkerofhealth.IntJ Obes(Lond).2008;32:1---11.
8.HusseyJ,BellC,BennettK,O’DwyerJ,GormleyJ.Relationship betweentheintensityofphysicalactivity,inactivity, cardiore-spiratoryfitnessandbodycompositionin7-10-year-oldDublin children.BrJSportsMed.2007;41:311---6.
9.Associac¸ãoNacionaldeEmpresasdePesquisa(ABEP).Critério
de classificac¸ão econômica --- Brasil [cited 7 Feb 2010].
Available from:
http://www.abep.org.br/mural/anep/04-12-97-cceb.htm
10.Marshall WA, Tanner JM. Variations in pattern of pubertal changesingirls.ArchDisChild.1969;44:291---303.
11.MarshallWA,TannerJM.Variationsinthepatternofpubertal changesinboys.ArchDisChild.1970;45:13---23.
12.PetroskiEL.org.Antropometria:técnicasepadronizac¸ões.3rd ed.PortoAlegre:Pallotti;2009.
13.deOnisM,OnyangoAW,BorghiE,SiyamA,NishidaC,Siekmann J.DevelopmentofaWHOgrowthreferenceforschool-aged chil-drenandadolescents.BullWorldHealthOrgan.2007;85:660---7.
14.SlaughterMH,LohmanTG,BoileauRA,HorswillCA,StillmanRJ, VanLoanMD,etal.Skinfoldequationsforestimationofbody fatnessinchildrenandyouth.HumBiol.1988;60:709---23.
15.BehnkeAR,WilmoreJH.Evaluationandregulationofbodybuild andcomposition.NewJersey:PrenticeHall;;1974.
16.DollmanJ,RidleyK,MagareyA,MartinM,HemphillE.Dietary intake,physicalactivity and TVviewingas mediators ofthe associationofsocioeconomicstatuswithbodycomposition:a cross-sectionalanalysisofAustralianyouth.IntJObes(Lond). 2007;31:45---52.
17.MalinaRM,Pe˜naReyesME,EisenmannJC,HortaL,RodriguesJ, MillerR.Height,massandskeletalmaturityofelitePortuguese soccerplayersaged11-16years.JSportsSci.2000;18:685---93.
18.DavisJN,VenturaEE, TungA,MunevarMA,HassonRE, Byrd-Williams C, et al. Effects of a randomized maintenance interventiononadiposity and metabolic riskfactors in over-weightminorityadolescents.PediatrObes.2012;7:16---27.
19.FriedrichRR,SchuchI,WagnerMB.Effectofinterventionson thebodymassindexofschool-agestudents.RevSaudePublica. 2012;46:551---60.
20.PhysicalActivityGuidelinesAdvisory Committee.In:Physical Activity Guidelines Advisory Committee Report. Washington, DC:U.S.DepartmentofHealthandHumanServices;2008.
21.WorldHealthOrganization(WHO).In:TheWorldHealthReport 2002: reducing risks, promoting healthy life. Geneva: WHO; 2002.
22.Strong WB, Malina RM, BlimkieCJ, Daniels SR, Dishman RK, GutinB,etal.Evidencebasedphysicalactivityforschool-age youth.JPediatr.2005;146:732---7.
23.WorldHealthAssembly57.17.In:Global strategyondietand physicalactivity.Geneva:WHO;2004.
24.HarrisKC, Kuramoto LK, Schulzer M, Retallack JE. Effect of school-basedphysicalactivityinterventionsonbodymassindex inchildren:ameta-analysis.CMAJ.2009;180:719---26.
Effectsofprogrammedphysicalactivityinschoolchildren 129
metabolicriskprofileofurbanAsianIndianadolescentsinNorth India.EurJClinNutr.2010;64:364---73.
26.Wright K, Norris K, Newman Giger J, Suro Z. Improv-ing healthy dietary behaviors, nutrition knowledge, and self-efficacy among underserved school children with par-ent and community involvement. Child Obes. 2012;8: 347---56.
27.KremerMM,ReichertFF,HallalPC.Intensityandduration of physicaleffortsinphysicaleducationclasses.RevSaude Pub-lica.2012;46:320---6.
28.Hardy OT, Wiecha J, Kim A, Salas C, Briceno R, Moody K, etal.Effectsofamulticomponentwellnessinterventionon dys-lipidemiaamongoverweightadolescents.JPediatrEndocrinol Metab.2012;25:79---82.
29.LottenbergSA,GlezerA,TurattiLA.Metabolicsyndrome: iden-tifyingtheriskfactors.JPediatr(RioJ).2007;83:S204---8.