www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
REVIEW
ARTICLE
Low
birth
weight
and
obesity:
causal
or
casual
casual
association?
Adolfo
Monteiro
Ribeiro
∗,
Marília
de
Carvalho
Lima,
Pedro
Israel
Cabral
de
Lira,
Giselia
Alves
Pontes
da
Silva
UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received10June2014;accepted19September2014 Availableonline28June2015
KEYWORDS
Humandevelopment; Lowbirthweight; Nutrition; Obesity; Health; Disease
Abstract
Objective: Topresenttheconceptual foundationsthatexplainhow events occurringduring intrauterinelifemayinfluencebodydevelopment,emphasizingtheinterrelationbetweenlow birthweightandriskofobesitythroughoutlife.
Datasources: GoogleScholar,LibraryScientificElectronicOnline(SciELO),EBSCO,Scopus,and PubMedwerethedatabases.‘‘Catch-upgrowth’’,‘‘lifecoursehealth’’,‘‘disease’’,‘‘child’’, ‘‘development’’,‘‘earlylife’’,‘‘perinatalprogramming’’,‘‘epigenetics’’,‘‘breastfeeding’’, ‘‘smallbabysyndrome’’,‘‘phenotype’’,‘‘micronutrients’’,‘‘maternalnutrition’’,‘‘obesity’’, and‘‘adolescence’’wereisolatedorassociatedkeywordsforlocatingreviewsand epidemiolog-ical,interventionandexperimentalstudiespublishedbetween1934and2014,withcomplete textsinPortugueseandEnglish.Duplicatearticles,editorialsandreviewswereexcluded,as wellasapproachesofdiseasesdifferentfromobesity.
Datasynthesis: Within47 selected articles among 538 eligible ones, the thriftyphenotype hypothesis,theepigeneticmechanismsandthedevelopmentplasticitywereidentifiedas fun-damentalfactorstoexplainthemechanismsinvolvedinhealthanddiseasethroughoutlife.They admitthepossibilitythatbothcardiometaboliceventsandobesityoriginatefromintrauterine nutritionaldeficiency,which,associatedwithafoodsupplythatisexcessivetothemetabolic needsoftheorganisminearlylifestages,causesendocrinechanges.However,theremaybe phenotypicreprogrammingforlowbirthweightnewbornsfromadequatenutritionalsupply,thus overcomingarestrictiveintrauterineenvironment.Therefore,catch-upgrowthmayindicate recoveryfromintrauterineconstraint,whichisassociatedwithshort-termbenefitsorharmsin adulthood.
Conclusions: Dependingonthenutritionaladequacyinthefirstyearsoflife,developmental plasticitymayleadtophenotypereprogrammingandreducetheriskofobesity.
© 2015Sociedadede Pediatria de SãoPaulo. Published by Elsevier Editora Ltda.All rights reserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2014.09.007
∗Correspondingauthor.
E-mail:[email protected](A.M.Ribeiro).
PALAVRAS-CHAVE
Desenvolvimento humano;
Baixopesoaonascer; Nutric¸ão;
Obesidade; Saúde; Doenc¸a
Baixopesoaonascereobesidade:associac¸ãocausaloucasual?
Resumo
Objetivo: Apresentar as basesconceituais que explicam como eventos navidaintrauterina podeminfluenciarodesenvolvimentocorporaleenfatizarainterrelac¸ãoentrebaixopesoao nascereriscodeobesidadeaolongodavida.
Fontesdedados: GoogleScholar,ScientificElectronicLibratyOnline(SciELO),EBSCO,Scopus e PubMed foram asbases de dados. ‘‘Catch-up growth’’,‘‘lifecourse health’’, ‘‘disease’’, ‘‘child’’, ‘‘development’’, ‘‘early life’’, ‘‘perinatal programming’’, ‘‘epigenetics’’, ‘‘breastfeeding’’, ‘‘small baby syndrome’’, ‘‘phenotype’’, ‘‘micronutrients’’, ‘‘maternal nutrition’’, ‘‘obesity’’ e ‘‘adolescence’’ foram descritores isolados ou associados para localizar revisões, estudos epidemiológicos, de intervenc¸ão ou experimentais publicados entre1934e2014, comtextosintegrais, emportuguês einglês. Excluíram-seduplicidades, editoriais,resenhaseabordagensdedoenc¸adiferentedaobesidade.
Síntesedosdados: Nos47artigosselecionadosdentre538elegíveis,identificaram-seas hipóte-sesdofenótipopoupador,dosmecanismosepigenéticosedaplasticidadedodesenvolvimento como fundamentaispara explicarmecanismosenvolvidosnasaúdeenasdoenc¸asdurantea vida. Elasadmitem apossibilidadede eventoscardiometabólicoseobesidade teremorigem em deficiênciaintraúterodenutrientes que,associadosasuprimentoalimentarexcessivo às necessidadesmetabólicasnasfasesprecocesdavida,provocaalterac¸õesendócrinas.Todavia podehaverreprogramac¸ãofenotípicaquesupereambienterestritivointrauterinopara nasci-doscombaixopesoapartirdeofertanutricionaladequada.Assim,ocatch-upgrowthindicaria recuperac¸ãodarestric¸ãointrauterinaeseassociariaabenefíciosemcurtoprazoouprejuízos noadulto.
Conclusões: Nadependênciadeadequac¸ãonutricionalnosprimeirosanosdevida,a plastici-dadedodesenvolvimentopodelevaràreprogramac¸ãofenotípicaereduziroriscodeobesidade. © 2015Sociedadede Pediatriade SãoPaulo. Publicado porElsevier Editora Ltda.Todosos direitosreservados.
Introduction
The knowledgeof theprocessesinvolved inhuman devel-opment contributes to the better understanding of the mechanismsassociatedwithhealthanddiseasethroughout life.1Toidentifythesemechanisms,whenandhowtheywork
isprobablythebestwaytopreventthediseaseonset.Only inrecentyearsseveraldiseasesthataffectadultshavebeen associatedwithintrauterineperiodevents.2---4
Althoughcomplementaryexaminationsprovide informa-tion that allows fetal development monitoring, obtaining data at birth provides better conditions for assessment, withadequacyofweightforgestationalagebeingthefirst measurement capable of providing information on fetal interactionwiththeintrauterineenvironment.5
The fetus reflects, throughnutrition, growthand body composition,thesupplies andthe energyit receivesfrom the mother, also expressing its dependence on placental function.6Thefetusalsoreceivesaflowofchemical
medi-ators, which informabout the maternal nutritional status and possibly the quality of the postnatal environment.3
Thisinformationcontributestodefinebodycompositionand size, aswell astostructure the endocrineand metabolic systems.7
The United Nations Children’s Fund8 reports that the
worldwideincidenceoflowbirthweightremainedat15%in theperiodof2008---2012,despitetheadvancesinprenatal care. The WorldHealth Organization9 confirms that more
than40millionchildrenyoungerthan5yearsareoverweight orobeseand,therefore,aresusceptibletoanincreasedrisk ofnoncommunicablediseases.Thesestatisticsreinforcethe importanceof considering the interrelationsbetween low birthweight andthe risk of obesity and itscomorbidities throughoutlife, consideringthat thisunderstanding isthe basisto establish earlyinterventions thatcan change the naturalhistoryofthisprocess.
Thisreviewaimedtodisclosetheconceptualand empir-icalfoundationsunderlyingtheunderstandingoftheeffect ofintrauterinelifeeventsonbodydevelopment, emphasiz-ingtheinterrelationbetweenlowbirthweightandobesity throughoutlife.
Method
Abstracts identified in the databases (SciELO=75; Google scholar=9; EBSCO
=312; pubMed=112; Scopus=30 (n=538)
Full articles assessed for eligibility (n=208)
Excluded abstracts n=10 for duplicity n=189 for subject n=30 for language
n=69 lack of access to full-text n=22 book reviews
n=10 editorials
Full articles excluded n=118 restricted to intrauterine development n=15 Central topic of obesity
n=28 No intrauterine development theory approach
Articles with assessed eligibility (n=47)
Articles included in the review (n=47)
Selection
Eligibility
Inclusion
Identification
Figure1 Flowchartofarticleselectionforthereview.
Inclusion criteria comprised review articles, epidemi-ological, experimental or intervention studies published between 1934 and 2014, with full texts in Portuguese or English,addressingaspectsofintrauterinedevelopmentand itsassociationwithobesity.Abstractsorarticlespublished induplicatewereexcluded,aswellasthoseaddressing diag-nosisortreatmentofspecificdiseasesratherthanobesity, editorialsandreviews.
Abstractsthatmettheinclusioncriteriawerereviewed bytwo independentreviewers whohad knowledgeof the centralthemeofthereview,toattainconsensualdefinition ofthearticlesthatwouldbereadinfull.
Results
A total of 538 abstracts were found, of which 330 were excluded, resulting in the analysis of the full texts of 208articles.Afterapplyingtheinclusionandexclusion crite-ria, the sample comprised 47 eligible articles that were included in the review (Fig. 1) and which were used to preparetheglossarydescribedinTable1.
Firstevidenceandthethriftyphenotype hypothesis
Theinfluenceoffactorspresentinearlylifewasidentifiedin reportsthatanalyzedthemortalityratefromallcausesin theUK andSweden, from1845to1925, at theage range of 10---100 years, which originated the hypothesis that a changeintheenvironmentcouldhelpreducemortality.10,11
Failure to prove the hypothesis motivated the inclusion of the age group 5---10 years in the mortality study. This time,anassociationwasobservedbetweenimprovementin
livingconditionsofchildrenandadolescentsanddecreasein overallmortalityrateinbothcountries,suggestingthatthe improvementofenvironmentalconditionsduringpregnancy couldhaveadirecteffectonthehealthofchildreninthe youngeragegroups.11
Studiescarriedoutinequines12demonstratedthe
influ-ence of the maternal body on the fetus, regardless of the genetic factor. Fetuses of large animals implanted in the uterus of small species resulted in foals that were smallerthanexpected,aswellasfetusesgeneratedinsmall equines showed greater development when implanted in largemares.
Inthecontextoftheseideas,Neel13published
observa-tionsontheeffectsof maternalnutritionaldeprivationon the fetus. The author theorized that fetuses developed a typeofmetabolismaimedatconservingenergy,withinsulin resistancebeingimportant,whichwouldberelatedtoa ran-domgeneticmutation.13Thepreponderanceofthis‘‘thrifty
genotype’’wouldlastandwouldbepassedontofuture gen-erations,andthus,theabundantconsumptionoffoodwould leadtoobesitybyexcessiveaccumulationofreserves.
The effect of food shortages during the German siege of the Netherlands in World War II14 made women suffer
the impact of malnutrition during pregnancy. The analy-sisofthisnaturalexperimentraisedquestionsaboutNeel’s hypothesis,13asnutrientdeprivationledtodifferenteffects
thanthoseexpected.Fetusesthatsufferedmalnutritionin the first trimester developed obesity in adulthood, while nutritionalrestriction afterthe initialphaseof pregnancy wasnotassociatedwiththesameeffect.Evenifonewould admittheimportanceofenvironmentalstimuliinthe occur-renceofobesity,thegeneticfactorcouldnotbeignored.
ANorwegianstudy15 reinforcedtheimportanceof
Table1 Glossaryoftermsandconceptsusedinthisreview.
Terms Concepts
Catch-upgrowth Periodofrapidweightgain and/oraccelerationingrowth ratethatoccursaftera slowdownperiod
Epigenetics Studyofalterationsingene expressionthatcanbe transmittedtooffspringanddo notimplyinDNAsequence alterations
Thriftyphenotype hypothesis
Whenthefetalenvironmentis poorfromanutritionalpointof view,thefetalbodygoes throughaprogrammingprocess inwhichthereisprotectionfor thedevelopmentofsome organs(brain,heart);however, itleadstometabolicchanges thatmayimpactonlater stagesoflife
Phenotypicplasticity Thecapacityoftheorganism todevelopseveralphenotypes fromasinglegenotype,in responsetodifferent environmentalstimuli Fetalprogramming Structuralandfunctional
changesthatoccurinthefetal bodyinresponsetostimuli thatoccuratcriticalperiodsof development
Predictiveadaptive responses
Aprocessthroughwhichthe body,intheearlystagesof development,predictsthe environmentitwillbeexposed tointhefuturebymodifying itselfphenotypically,basedon theperceptionof
environmentalstimuli
Consideringthegenerationofindividualsbornbetween1896 and1925,itwasverifiedthatincreasedmortalityinadults occurredincountieswithhigherinfantmortality,withrisk factorsbeingincreasedbloodcholesterolandahigh-fatdiet consumption, as well as individuals’ social status, smok-ingandtypeofnutrition.Regardingthecontributionofthe high-fatdiettohighcholesterollevels,thestudyidentified differentbehaviorsaccording tothesocioeconomic status of individuals. The ones who had previously experienced povertyhadincreasedcholesterolrelatedtoahigh-fatdiet, which did not occur with those with a financially stable life.15 These findings provided the basis for the
hypothe-sisthatthedeprivationperiodcontributedforindividualsto develop‘‘fat intolerance’’,beingexposedtoahigherrisk ofdeathwhentheyreceivedanabundantdiet.
Inadditiontothehypothesesoffatintoleranceandthe ‘‘thriftygenotype’’, a cohortin Hertfordshire16,17
demon-stratedanassociationbetweenlowbirthweightanddeath fromcoronaryheart diseaseinadulthood. Riskfactorsfor
cardiovascularandmetabolicdiseasesweremorefrequent among those born with low birth weight.17 Additionally,
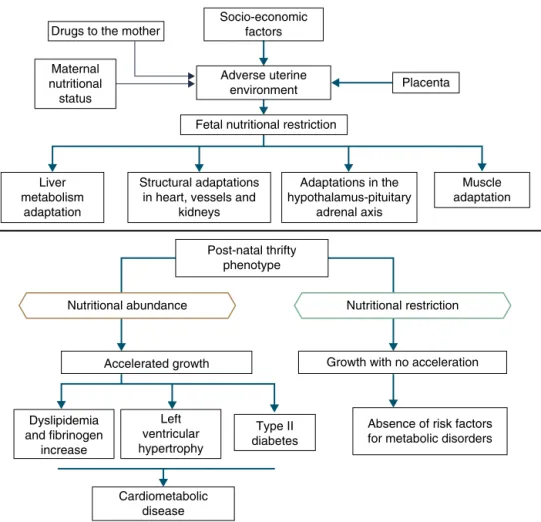
Barker16proposedthatthefetusrespondswithgrowth
retar-dationwhenthereis anutrientdeficitin itsenvironment, whichisassociatedwithdecreased insulinsensitivity, pro-vidingbetter survival circumstances. This adaptation also predicts,inadultlife,maintenanceofanenvironmentwith lowsupplyofnutrients.Ifthissituationdoesnotoccur,the abundantsupplyoffoodcreatesanimbalancethatcanlead tocardiometabolicdiseases.Thiscontextledtothethrifty phenotypehypothesis,16andsubsequently,tothepredictive
adaptiveresponse,3whicharedepictedinFig.2.
Situations relatedto birth weightalterations reinforce its importance as an indicative marker of intrauterine environmentand predictor of cardiometabolicdiseases in adolescence and adulthood.18---20 Thus, birth weight may
haveaconstitutionaloriginorbesecondarytointrauterine nutritionaldeprivation,whichleadstofetalgrowth restric-tion. It is acknowledged that low birth weight newborns undergotheinfluenceofdifferentmechanismsofadaptation toextra-uterineenvironment,amongwhicharetheincrease in carbohydrate metabolism and the consequent increase inadiposity,increasing thefuturerisk of chronic diseases suchas insulin resistance, obesity and type 2 diabetes.19
Thesemechanismsleadtohighlevelsof leptin,secondary toincreasedresistancelevelofitsreceptors,relatedtolack ofsatietyinearlylife,whichisassociatedwithobesityand metabolic disorders in adolescence and adulthood, when thesenewborns are exposedto a nutritionalenvironment withexcessivenutritionalofferintheearlyyearsoflife.20
Whenleavingthissituationofrestrictedgrowth,dueto hormonalor nutritional issues, to another with adequate supplyofnutrients,acceleratedgrowthrecoverymayoccur toachievethegeneticallydeterminedpotential,21whichis
theso-calledcatch-upgrowth.22
Catch-up growth can be definedas the rateof weight gainand/or growththatis higherthanthe statistical lim-its of normality for age and maturity that occurs during a defined period of time, following a transient period of growth inhibition.21 Catch-up growth is a physiological
process related to size recovery of a body subjected to restriction,sothatitcanreachtheadequatesizeforage, gender and degree of maturity, depending on the action of the somatotropic axis, with an increase in hormone receptors.21
Thisrecovery,resultingfromunfavorableconditionsfor growthduringtheprenatalandearlypostnatalperiods,can influence the risk of developing cardiometabolic diseases throughout life.23,24 However,short-term growth recovery
offers advantages for neurodevelopment, particularly for children born with very low birth weight, and also con-tributes to increased resistance to infections. Hence the question of identifying whether the benefits of increased growth velocity can occur without adverse metabolic consequences.18
It is accepted that a catch-up growth >0.67 standard deviations wouldbeassociated withcentralobesity25 and
Cardiometabolic disease
Type II diabetes
Absence of risk factors for metabolic disorders Growth with no acceleration
Nutritional restriction Nutritional abundance
Accelerated growth
Left ventricular hypertrophy Dyslipidemia
and fibrinogen increase Liver metabolism
adaptation
Post-natal thrifty phenotype Structural adaptations
in heart, vessels and kidneys
Muscle adaptation Placenta
Socio-economic factors Drugs to the mother
Maternal nutritional status
Adverse uterine environment
Fetal nutritional restriction
Adaptations in the hypothalamus-pituitary
adrenal axis
Figure2 Thethriftyphenotypehypothesisandpredictiveadaptiveresponse.
agreaterdegree thanwell-nourishedchildrenor theones whoareexcessivelyfed.Thus,hyperinsulinemiasecondary toinsulinresistance couldbethe keyexplanationfor the genesisofmetabolicsyndrome.26
Insulin resistancein preterm infants is associated with hypersecretion of growth hormone and reduced levels of IGF-1,whichpersistfor3monthsafterbirthintheabsence ofadequatenutritionalsupply.Thisalteredendocrine sta-tus favorsreductionof subcutaneous adiposetissue, with relativevisceral adiposity, a markerof insulin resistance, dyslipidemia,andthepresenceofothermetabolicsyndrome components.27
Despitetheseobservations,itisnotclearwhether cen-tral obesity, rather than subcutaneous fat, is a function ofprematurity, of beingborn smallfor gestationalage or ofcatch-up growth.Studies have shown that infants with growthrestrictionatbirthhavereducedsubcutaneousfat, butmaintainlevelsofabdominalfatsimilartothoseof new-bornsthatareadequateforgestationalage.28Acohortstudy
carried out to investigate the association between fetal andearlypostnatalgrowthandmetabolicand anthropomet-ricalterationsshowedthatcatch-upgrowthwasassociated withthefetalgrowthpattern, regardlessof birth weight, and was related to higher insulin sensitivity and lower concentrationsof leptin atbirth. Therefore,thecatch-up growth would promote the recovery of body size and fat storeswithout deleteriousconsequences tothemetabolic profileandbodycomposition,afteroneyearofage.29
A recent review30 was performed to search evidence
on the association between low weight, insulin resis-tance and type 2 diabetes in adults, considering body composition andmetabolic pathways. The empirical basis shows a multifactorial association and points out that, in some children and adults who were born preterm, insulin resistance andincreased abdominaladiposity orig-inate from the variation of the glucocorticoid receptor gene.Higherconcentrationsofglucocorticoidsactivatethe hypothalamic-pituitary-adrenalaxis, promotingthe intake ofpalatablefoods,which activatethepleasurecentersof the brainandtrigger greater accumulation ofadipocytes. Thus, adults whowere born preterm may have increased sensitivity to stressors, leading to an overproduction of glucocorticoids,stimulatingtheomentalpopulationof pre-adipocytes,withincreasedabdominalfatdeposition.
Toanalyzetheassociationbetweenlowbirthweightand hypertension development in adulthood, Huxley et al.,31
in a meta-analysis, compared 18 articles submitted by researchersthatcorroboratedthethriftyphenotype hypoth-esiswith37 studiesfromother researchers.Although this meta-analysis31 did not show an association between low
birth weight and hypertension in adults, it did not rule out the adaptive hypotheses, and other aspects of late expression of intrauterinelife determinants started tobe investigated. The hypotheses were based on the idea of conservation,which didnotseem torepresenttheoverall process.Observations fromthebeginningoflifesuggested a muchwider andwidespread phenomenon, in which the patternofdevelopmentcouldbemodifiedinanydirection, dependingonthestimulus.32,33
Theepigeneticexplanation,thethriftyphenotype andcardiometabolicdiseases
Basedonthepossibilitythatthephenotypecangenerate dif-ferentgenotypeunderdifferentenvironmentalconditions, that is, phenotypic plasticity, Gluckman et al.34
enunci-atedthehypothesis ofan ‘‘adaptivepredictiveresponse’’ totheenvironment. Thedevelopmentplasticitywould be evokedbyenvironmentalalterationsearlyinlife, generat-inganadaptivephenotypicresponse,ofwhichadvantages wouldmanifestonlyinlaterstages.Therefore,the pheno-typicplasticitymighthavegrantedadvantagestothehuman species to face environments with nutritional restriction or high-energy expenditure.However, when submitted to a differentnutritional environment than theprogrammed one, individuals would have exacerbated responses and develop diseases in adulthood.34 The ‘‘predictive
adap-tive response’’ will be an adaptive advantage when the ‘‘prediction’’ about the environment is correct (match) and may determine a disadvantage when it is wrong (mismatch),34characterizingplasticity.
Plasticity can trigger differentresponses with immedi-ateexpression,suchasnutritionalrestrictionstothefetus, which reacts with a decrease in its nutritional reserves, decreased anabolism, plasma insulin, insulin-like growth factor 1 (IGF-1), and blood flow diversion to protect the heartandbrain.Theseimmediateadaptationstothe restric-tiveenvironmentallowadequatesurvival,butresultinlow birthweight,increasedriskofmorbidityandmortality, cog-nitiveimpairment,andpersistentgrowthdeficit.35
Responsesaimedatensuringsurvivalcan,however,lead toadaptive errors.Maternal hyperglycemia in early preg-nancy can contribute to embryopathy, by leading to the reductionofmyo-inositol,whichisessentialforembryonic developmentduringgastrulationandtheneurulationstages. Myo-inositoldeficiencyseemstodisturbthe phosphoinosi-tidesystem,whichleadstoabnormalitiesinthearachidonic acid---prostaglandinpathwaysandincreaseinreactive oxy-gensubstances.36Thischainofeventsisresponsibleforfetal
cardiovascular abnormalities, suchas transposition of the great vessels, ventricular septal defects, hypoplastic left heartsyndrome,anddextrocardia.37Increasedmaternal
gly-catedhemoglobinisassociatedwithembryonicalterations in 66% of fetuses, but whenlower than 9.5%, itdoes not alterembryogenesis,36 characterizingdisruption,3inwhich
ahormonecantriggeranundesirableeffectontheresponse processtoenvironmentaladaptation.
Although thefetaland postnatalorganismshave adap-tiveresponsestoarestrictiveintrauterineenvironmentina continuousmanner,theirdevelopmenthas‘‘plasticity win-dows’’,i.e.,thepossibilityofinterferencewiththeadaptive programming, correcting inappropriate responses.38 This
hypothesis is corroborated by an experimental study comparing offspring with growth retardation, born to malnourishedratsduringpregnancy,totheoffspringof well-nourished rats, after feeding a hypercaloric diet to the offspringwithoutIUGRandleptintothosewithIUGR. The authorsverifiedthatgrowthinthetwogroups didnot dif-ferandconcludedthattheincreaseinleptinconcentration signaledthepresenceofanadequateamountofadipose tis-sueintheoffspringorganismand,therefore,ofnutritional reserves.38
The adaptive continuity toenvironmental changes and ‘‘windowsofopportunity’’areexplainedbytheepigenetic theory,i.e.,thepossibilitythatenvironmentalfactors inter-ferewithgeneexpression.Predictiveadaptiveresponsesare modulated by covalent modifications of deoxyribonucleic acidandhistones,whicharenecessaryforthephenomenon ofgene transcription,namely the synthesis ofribonucleic acidforproteinsynthesis.39
Evidencesuggeststhatthefetalperiodismoresensitive fortheoccurrenceof epigeneticvariationsthat will influ-encecellandtissuegeneticexpression,sexualdimorphism andtheriskoftriggeringdisordersthatwillmanifestlater inlife.40Anexampleoftheinfluenceofepigeneticsonthe
earlyneonatalperiodistheeffectofhigh-fatdietsduring pregnancy,41i.e.,overeatingintheoffspringandincreased
expression of orexigenic peptides promotingincrease and deregulationofneonatalleptin.
Thederegulation isimportant,becauseleptin isoneof thefirsthormones synthesized duringembryonic develop-mentbytheplacenta,byadipocytesofwhiteadiposetissue, livercells,cartilaginousstructuresandheart muscle.This molecule acts on neurogenesis, axonal growth, dendritic proliferation,synapse formation,23 in the developmentof
neurologicalpathwaystosatiety,hungerandthermal regu-lation,whichbeginsinintrauterinelifeandiscompletedin thefirstmonthsoflife,whensuppliedbybreastmilk.42
During the first pregnancy trimester, leptin synthesis occursin the placenta, triggering a cascadeof transcrip-tionfactorsinpre-adipocytes,contributingtotheformation ofwhiteadiposetissue,whichbecomesthemainsourceof leptinsynthesis.Thismolecule,bycrossingtheblood---brain barrier, contributes to the development of several brain regions,amongthemthehypothalamus,wheretheir recep-torsarelocated.23 The leptin-receptorbindingisessential
toindicatethe need for nutrient intake andthe increase inenergyreserves inadipose tissue.When leptin concen-trations in the hypothalamus are reduced due to binding tothereceptors,thefeelingofsatietyis triggeredbythe activation of anorexigenic neurons. Thus, the phenotypic alterationof leptin receptors, characterizing leptin resis-tance,results in the persistenceof thefeeling of hunger andpromotesingestionoflargequantitiesofnutrientsand adiposetissuehypertrophy.24
Cardiometabolic diseases Body composition of
child/adolescent/adult
Catch-up Delivery variables
Breastfeeding Placenta variables
Development of the fetus, body composition, metabolic processes
Paternal genetic variable Social and natural environment
Maternal, socioeconomic, demographic, behavioral, biological and
gestational variables
Diet in childhood
Physical activity
Lifestyle
Diet
Development of newborn - body composition - metabolic processes
Figure3 Explanatorymodel---cardiometabolicdiseases.
wellas innewborns withIUGR submitted toexcess nutri-entintake or whose mothers were fed lipid-richdiets. In contrast,whenduringpregnancyandlactation,the moth-ersreceivebalanceddiets,or whenfetuseswithIUGR are submittedtorestrictive dietsduring thelactation period, theyshownormalgrowthoftheadiposetissue,butdevelop post-weaning hyperphagia, attributed to phosphorylation deregulationofhypothalamicleptinreceptors,reductionin anorexigenicreceptorsandreductioninpermeabilityofthe blood---brainbarriertothismolecule.24
Epidemiologicalresearch18hascorroboratedthe
hypoth-esis of adaptive predictive response,33 by demonstrating
that an abundant food supply contributes to catch-up growth.However,itisalsoconfirmedwhenthereisabsence of abdominal obesity, with normal neurodevelopment, in children receiving adequate nutrition, but not in excess. Thesignificance ofthenutrition ofthenewborn hasbeen debated,43 especially for preterm ones, because there is
moreorganicplasticityearlyinlife.Thus,adequate inter-ventionsshortlyafterbirthhaveplasticityasthepossibility forcorrectionofdevelopmentaldelay,maintainingthe ben-efitsbycumulativeeffect.Asageincreases,withthedecline inplasticity,nutritionthatis adequatetothebody’sneed willmakethechild’sbodycompositionreachthelevelofa childborntoterm,atthesameage.Similarly,excess nutri-tion,alsoduetoplasticity,willresultindeleteriouseffects thatwillmanifestthroughoutlife.
Onemustconsider4theprocessesbywhichthequantity
andqualityofnutrientssuppliedtothefetusandtheembryo aredetermined,duetotheirpermanenteffectson devel-opment,a processcalled nutritional programming, which depends onboth maternal characteristics (before, during andafterpregnancy),andfetalnutritionalstatus.
Among the maternal andenvironmental characteristics that affect the fetal and newborn development are the
socioeconomicandnutritionalstatuses,withdirecteffect, andmaternaleducation,withanindirecteffect.Nepalese infants born with low birth weight more frequently had motherswithloworverylowsocioeconomiclevel,low edu-cational leveland inadequatenutrition,factors thatwere associated withlower level of prenatalmedical care.44 A
population-based cohortfollowed between 1961and 2000 disclosed that, in four decades, in the United Kingdom, socioeconomic inequalities still determined a higher fre-quency of low birth weight or premature births among mothersfromthelowersocioeconomicclasses,evenafter adjustingformaternalage.44
Amongthedemographicandsocialfactorsarethe mater-nal variables, suchas age extremes (<20 and >30 years), loweducationallevel,parity,shortinterbirthinterval,drug use,45 and short stature.46 Breastfeeding is also
consid-ered,givenitsweaktomoderateprotectiveeffectonadult obesity. Breastfeeding, by meeting the newborn’s needs, reduces therisk of insulin resistanceand increased intra-abdominal adiposity, and provides leptin concentrations capableofmodulatingthehunger---satietymechanism.47
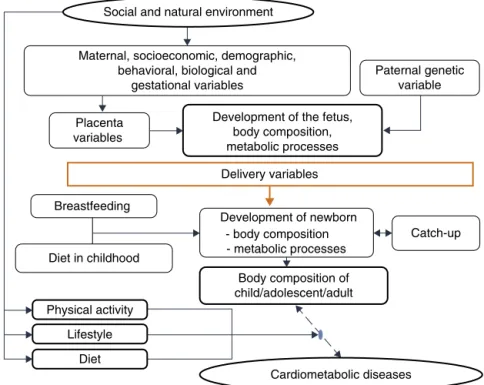
Thisevidenceisconsistentwiththehypothesisaccepted by Gluckmanet al.,3 which affirmsthatnaturedirects its
effortstoreproduction.Thus,iftherearesignsofa threat-eningpostnatalenvironment,thefetusisbornprematurely or smaller than expected,and in a nutrient-rich environ-ment, unlike the planned trajectory, develops metabolic disease,inamultifactorialprocessinwhichmanymaternal andfetalfactorsinteract(Fig.3).
apprehendingseveralaspectsofbiologicalknowledge, espe-cially of the evolution theory, because it is through this viewthatone cancapture theimportanceof the interac-tionbetweengenotypeandtheenvironmentandtheseveral mechanismsusedbythebodytoadapttotheenvironment. Physicians,especiallypediatricians,haveakeyroleinthis scenario,astheycareforhumanbeingsatatimewhenthere aremoreopportunitiestoactandgeneratechanges,dueto developmentalplasticity.
Funding
Conselho Nacional de Desenvolvimento Científico e Tec-nológico (CNPq), for funding productivity grants given to PedroLira,MaríliaLimaandGiseliaAlves.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.HalfonN,LarsonK, LuM,TullisE,RussS. Lifecoursehealth development:past,presentandfuture.MaternChildHealthJ. 2014;18:344---65.
2.GluckmanPD,HansonMA,CooperC,ThornburgKL.Effectofin uteroandearly-lifeconditionsonadulthealthanddisease.N EnglJMed.2008;359:61---73.
3.GluckmanPD,HansonMA,BeedleAS.Earlylifeeventsandtheir consequencesforlaterdisease:alifehistoryandevolutionary perspective.AmJHumBiol.2007;19:1---19.
4.DesaiM,RossMG.Fetalprogrammingofadiposetissue:effects ofintrauterinegrowthrestrictionandmaternalobesity/high-fat diet.SeminReprodMed.2011;29:237---45.
5.Brasil--- Ministério daSaúde. In:Secretaria deVigilânciaem Saúde---departamentodeanálisedesituac¸ãoemsaúde.Saúde Brasil2006:umaanálisedasituac¸ãodesaúdenoBrasil.Brasília: MinistériodaSaúde;2006.
6.SuhagA,BerghellaV.Intrauterinegrowthrestriction(IUGR): eti-ologyanddiagnosis.CurrObstetGynecolRep.2013;2:102---11. 7.SymondsME,MendezMA,MeltzerHM,KoletzkoB,GodfreyK, ForsythS,etal.Earlylifenutritionalprogrammingofobesity: mother-childcohortstudies.AnnNutrMetab.2013;62:137---45.
8.UNICEF[homepageontheInternet].Lowbirthweight.Available
from: http://www.data.unicef.org/nutrition/low-birthweight
[accessed19.07.14].
9.World Health Organization. Obesity and overweight.
Avail-able from: http://www.who.int/mediacentre/factsheets/
fs311/en/[accessed19.07.14].
10.KermackWO,McKendrickAG,McKinlayPL.Death-ratesinGreat BritainandSweden:somegeneralregularitiesandtheir signifi-cance.Lancet.1934;31:698---703.
11.KermackWO,McKendrickAG,McKinlayPL.Death-ratesinGreat Britainand Sweden: expressionofspecific mortalityratesas productsoftwofactors,andsomeconsequencesthereof.JHyg (Lond).1934;4:433---57.
12.WaltonA, HammondJ. Thematernal effects ongrowth and conformationinshirehorse-shetlandponycrosses.ProcRSoc LondB.1938;125:311---35.
13.Neel JV. Diabetes mellitus: a ‘‘thrifty’’ genotype rendered detrimental by ‘‘progress’’? Am J Hum Genet. 1962;14: 353---62.
14.LumeyLH,PoppelFW Van.TheDutchFamine of1944---45as ahumanlaboratory:changesintheearlylifeenvironmentand
adulthealth.In:LumeyL,VaisermanA,editors.Earlylife nutri-tionandadulthealthanddevelopment:lessonsfromchanging dietarypatterns,famines,andexperimentalstudies.London: Nova;2013.p.59---76.
15.Forsdahl A. Arepoor livingconditions inchildhoodand ado-lescence an important risk factor for arteriosclerotic heart disease?BrJPrevSocMed.1977;31:91---5.
16.Barker DJ. The intrauterine origins of cardiovascular and obstructivelungdiseaseinadultlife.TheMarcDanielsLecture 1990.JRCollPhysiciansLond.1991;25:129---33.
17.HalesCN,BarkerDJ,ClarkPM,CoxLJ,FallC,OsmondC,etal. Fetalandinfantgrowthandimpairedglucosetoleranceatage 64.BMJ.1991;303:1019---22.
18.OngKE,LoosRJ.Rapidinfancyweightgainandsubsequent obe-sity:systematicreviewsandhopefulsuggestions.ActaPediatr. 2006;95:904---8.
19.HofmanPL,ReganF,JacksonWE,JefferiesC,KnightDB, Robin-sonEM,etal.Prematurebirthandlaterinsulinresistance.N EnglJMed.2004;351:2179---86.
20.OngKK, Dunger DB. Birth weight, infant growth and insulin resistance.EurJEndocrinol.2004;151Suppl.3:U131---9.
21.Boersma B, Wit JM. Catch-up growth. Endocr Rev. 1997;18:646---61.
22.PraderA,TannerJM,vonHarnackG.Catch-upgrowthfollowing illnessorstarvation.Anexampleofdevelopmentalcanalization inman.JPediatr.1963;62:646---59.
23.Djiane J, Attig L. Role of leptin during perinatal metabolic programmingandobesity.JPhysiolPharmacol.2008;59Suppl. 1:55---63.
24.ParleeSD,MacDougaldOA.Maternalnutritionandriskof obe-sityinoffspring:theTrojanhorseofdevelopmentalplasticity. BiochimBophysicaActa.2014;1842:495---506.
25.BertottoML,ValmórbidaJ,BroiloMC,CampagnoloPD,Vitolo MR.Associationbetween weightgaininthefirst yearoflife withexcessweightand abdominaladiposityatprescholage. RevPaulPediatr.2012;30:507---12.
26.YeungMY.Postnatalgrowth,neurodevelopmentandaltered adi-posityafterpretermbirth-fromaclinicalnutritionperspective. ActaPediatr.2006;95:909---17.
27.Uthaya S, ThomasEL, HamiltonG, DoréCJ, Bell J, ModiN. Alteredadiposityafterextremelypretermbirth.PediatrRes. 2005;57:211---5.
28.Ibá˜nezL, OngK, DungerDB, ZegherF.Earlydevelopmentof adiposityandinsulinresistanceaftercatch-upweightgainin small-for-gestational-age.JCEM.2006;91:2153---8.
29.BeltrandJ,NicolescuR,KaguelidouF,VerkauskieneR,Sibony O,ChevenneD,etal.Catch-upgrowthfollowingfetalgrowth restriction promotes rapidrestoration of fat massbut with-out metabolic consequences atone year of age. PLoS ONE. 2009;4:E5343---50.
30.ThomasEL,AlSaudNB,DurighelG,FrostG,BellJD.Theeffect ofpretermbirthonadiposityandmetabolicpathwaysandthe implicationsforlaterlife.ClinLipidol.2012;7:275---88.
31.Huxley R, Neil A, Collins R. Unravelling the fetal origins hypothesis: is there really an inverse association between birthweightandsubsequentbloodpressure?Lancet.2002;360: 659---65.
32.GluckmanPD,HansonMA,SpencerHG,BatesonP. Environmen-talinfluencesduringdevelopmentandtheirlaterconsequences for healthanddisease:implicationsfor theinterpretationof empiricalstudies.ProcBiolSci.2005;272(1564):671---7.
33.GluckmanPD, Hanson MA. Thedevelopmentalorigins ofthe metabolicsyndrome.TrendsEndocrinolMetab.2004;15:183---7.
34.Gluckman PD, Hanson MA, Spencer HG. Predictive adap-tive responses and human evolution. Trends Ecol Evol. 2005;20:527---33.
36.Gilbert-Barness E. Teratogenic causesof malformations.Ann ClinLabSci.2010;40:99---114.
37.HornbergerLK.Maternaldiabetesandthefetalheart.Heart. 2006;92:1019---21.
38.Vickers M, GluckmanPD, Coveny A, Hofman PL, Cutfield W, GertlerA,etal.Neonatalleptintreatmentreverses develop-mentalprogramming.Endocrinology.2005;146:4211---6.
39.Fu Q, Yu X, Callaway CW, Lane RH, McKnight RA. Epige-netics: intrauterine growth retardation (IUGR) modifies the histone code along the rat hepatic IGF-1 gene. FASEB J. 2009;23:2438---49.
40.BogdarinaI,WelhamS,KingPJ,BurnsSP,ClarkAJ.Epigenetic modificationoftherenin---angiotensinsysteminthefetal pro-grammingofhypertension.CircRes.2007;100:520---6.
41.LeibowitzSF,ChangGQ,DourmashkinJT,YunR,JulienC,Pamy PP.Leptinsecretionafterahigh-fatmealinnormal-weightrats: strongpredictoroflong-termbodyfataccrualonahigh-fatdiet. AmJPhysiolEndocrinolMetab.2006;290:E258---67.
42.PicoC,PalouA.Perinatalprogrammingofobesity:an introduc-tiontothetopic.FrontPhysiol.2013;4:255.
43.Hanson M, Godfrey KM, Lillycrop KA, Burdge GC, Gluck-manPD.Developmental plasticity and developmentalorigins ofnon-communicabledisease: theoreticalconsiderationsand epigenetic mechanisms. Prog Biophys Mol Biol. 2011;106: 272---80.
44.KehindeOA,Njokanma OF,OlanrewajuD.Parental socioeco-nomic status and birth weight distribution of Nigerian term newbornbabies.NigerJPaed.2013;40:299---302.
45.Perez-Pereira M, Fernandez P, Gómez-Taibo M, Gonzalez L, TrisacJL, CasaresJ, et al. Neurobehavioraldevelopment of pretermandfulltermchildren:biomedicalandenvironmental influences.EarlyHumDev.2013;89:401---9.
46.AddoOY,SteinAD,FallCH,GiganteDP,GuntupalliAM,Horta BL,etal.Maternalheightandchildgrowthpatterns.JPediatr. 2013;163:549---54.