EFFECTS OF MUSCLE RESPIRATORY EXERCISE
IN THE BIOMECHANICS OF SWALLOWING
OF NORMAL INDIVIDUALS
Efeitos do exercício muscular respiratório na biomecânica
da deglutição de indivíduos normais
João Rafael Sauzem Machado(1), Eduardo Matias dos Santos Steidl (1),
Diego Fernando Dorneles Bilheri(1), Mateus Trindade(2), Guilherme Lopes Weis(2),
Paulo Roberto Oliveira de Jesus(3), Marisa Bastos Pereira(4), Renata Mancopes(5)
(1) Universidade Federal de Santa Maria, RS – Brasil. 2) Serviço de Radiologia do Hospital Universitário de Santa
Maria, RS – Brasil.
(3) Serviço de Física Médica do Serviço de Radiologia do
Hos-pital Universitário de Santa Maria, RS – Brasil.
(4) Departamento de Fisioterapia e Reabilitação da
Universi-dade Federal de Santa Maria, RS – Brasil.
(5) Departamento de Fonoaudiologia da Universidade Federal
de Santa Maria, RS – Brasil.
Departamento de Fonoaudiologia - Programa de Pós-Gradua-ção em Distúrbios da ComunicaPós-Gradua-ção Humana da Universidade Federal de Santa Maria
Financial support: CAPES
Conlict of interest: non-existent
the coordination of many muscles and brain areas, mainly in the cortex and brainstem. Besides being the act of conducting food or substances in the oral cavity to the stomach, in a safe way (by protecting the airway against aspiration), it represents a temporal integration of events associated with
normal breathing1.In healthy subjects, breathing
is interrupted during swallowing. This act is known as preventive apnea, being it retained in expiratory
phase2. This mechanism is considered one of the
protective factors and the prevention of laryngeal aspiration, induced by increased resistance of the airways3.
The pharynx is an anatomical region which is common to respiratory and digestive functions. The pharyngeal stage of swallowing is inluenced indirectly by the dynamic action of hyolaryngeal complex and also by the pharynx, which acts in a
INTRODUCTION
Swallowing is a complex activity with inten
-tional and uninten-tional actions, which requires
ABSTRACT
Purpose: to analyze the efects of the respiratory exercise in the biomechanics of swallowing in nor
-mal subjects. Methods: the muscle respiratory’s exercise in normal subjects was administered for
seven consecutive days by the incentive spirometer low (three sets of ten repetitions for inspiration and expiration).The biomechanics of swallowing was evaluated by videoluoroscopy through temporal variables (pharyngeal transition time) and visuoperceptual (number of swallows, waste in the pyriform sinuses and valleculae, penetration/aspiration). For statistical analysis was used the Wilcoxon test, Equality of Two Proportions and Kappa. Results: were evaluated 16 young women with a mean age
of 21,2±3,4 years. In visuoperceptual variables was observed almost perfect agreement between eva
-luators (p<0,001) and in temporal variable (p=1,00). After the training period there was a signiicant reduction in the pharyngeal transition time (p=0,02). Conclusion: the use of incentive spirometer low
signiicantly inluence the biomechanics of swallowing, especially in reducing the pharyngeal transition
time.
KEYWORDS: Deglutition; Methods; Breathing Exercises; Fluoroscopy; Deglutition Disorders;
disease, cold symptoms and/or respiratory afections at the moment of evaluation, without complaints of swallowing and they were not smokers. 18 young people who started the study were evaluated, but 02 were not excluded once they did not present themselves in the corresponding period (one week after the irst evaluation) for reassessment after the exercises, resulting in a sample of 16 subjects.
The video luoroscopy of swallowing exam (VFSE) was carried out to analyze the biomechanics of swallowing, by using the supply of paste-like consistency in spoon with volume of 10ml, before and after respiratory muscle exercise.
The images were generated in Siemens equipment, Iconos R200, in the luoroscopy mode with 30 frames per second. On the other hand, the videos recorded in the capture software Zscan 6. This software has the following main technical characteristics: with mother image to 720x576; image resolution of 32Bits (32 million colors); JPEG image format with 1440 dpi; NTSC, PAL, SECAM (all standard) video system; video up to 720x576 with images in real time (30 frames per second (frames/s) AVI format and divX compressor, being able to record on DVD and CD. The mean value of
the dose generated in this procedure is 0.14 mR/
frame (2,1 mR/sec), these dose measurements were performed under conditions that reproduce the technical and patient positioning, by using a 4
cm aluminum simulator and Radcal electrometer,
9010 model with speciic ionization chamber for the procedures in luoroscopy of 60 cm3.
During VFSE, the subjects were evaluated in the sitting position, with lateral projection. The ield of videoluoroscopic image included the lips, oral cavity, cervical spine and proximal cervical esophagus.
The data collected through the VFSE were assessed by using temporal and visual-perceptual variables, as proposed by Baijens et al. (2011). The analyzed time variable was the pharyngeal transition time (PTT), expressed in seconds, which is deined by the moment of the glossopalatal junction opening until the closure of the upper esophageal
sphincter13. For the analysis, it was used the Movie
Maker® software, which allows the view of each frame in seconds.
The visual-perceptual variables were repre -sented on a numerical scale, as it is described
bellow14:
• Number of swallows (number of times that the
bolus is fragmented) 0 - one swallow; 1 - Two swallows; 2 - Three swallows; 3 - four or more swallows;
• Residue in vallecula (stasis of the bolus in
vallecula after complete swallowing): 0 - no contractile way in order to protect the airway during
the act of swallowing3. Steele et al.4 presented
corre-lations between vertical and horizontal movement of this complex during swallowing and the predictive value for biomechanical of swallowing disorders.
In this context, Troche et al.5 carried out a study
in which they demonstrated the importance of respi
-ratory muscle training, through the use of expi-ratory spirometry for the dysphagia rehabilitation in Parkinson patients. They veriied that there was an improvement in the function of swallowing, being it attributed to the improvement of the hyolaryngeal complex function, resulting in an increased airway protection during swallowing.
The incentive spirometry (IS) is a useful device for conducting spontaneous breathing, assisting in the lung re-expansion, increased permeability of the airways and strengthening the respiratory muscles, in addition to optimizing the mechanical work of venti
-lation and arterial oxygenation6. The exercises with
IS are a simple and safe way to perform breathing training, aiming at the improvement of lung volumes and at the prevention of respiratory complications in children, adults and elderly people7.
Among these, we can highlight the Respiron® IS, which emphasizes the deep inspiration up to total lung capacity, providing visual feedback7,8.
This type of IS facilitates deep breathing, stimulates high inspired volumes and prevents lung hypoventi
-lation6,9,10. However, even being a device that is used
for inspiratory muscle training, there is the possibility of being used in the training of expiration, with the purpose of improving expiratory muscle strength, lung capacity and expiratory lows11.
With this type of exercise, it is possible to observe the movement of the hyoid bone and hyolaryngeal complex, which plays an important role in orofacial motricity through the contractile structures that
are inserted in it12. Such structures may present
improved mobility and function, from the respiratory muscle training with the use of incentive spirometry5.
Thus, this study aimed to analyze the efects of breathing exercise in relation to the biomechanics of swallowing in normal subjects.
METHODS
It is a prospective, longitudinal study, previ
-ously approved by the Research Ethics Committee of the Federal University of Santa Maria, following the resolution 466/2012, the registrant 23676813.8.0000.5346. All participants signed an informed consent form, agreeing to participate in
the research.
Data were analyzed by a computer program named Statistical Package for Social Sciences (SPSS) - version 17. And, the Wilcoxon test and equality of two proportions were used to verify the signiicance of the variables before and after respi
-ratory muscle exercise.
In order to ensure the agreement among
evalu-ators, the Wilcoxon Test was applied for the temporal variable and the Kappa for the visual-perceptual variable. For the degree of agreement among evalu
-ators, the Landis and Koch classiication17, being
found that: <0.00 poor agreement; 0.00 to 0.19 poor agreement; 0.20 to 0.39 weak agreement; 0.40 to
0.59 moderate agreement; 0.60 to 0.79 substantial
agreement; 0.80 to 1.00 almost perfect agreement. Results were expressed as mean ± standard deviation and percentage considering statistically signiicant p values <0.05.
RESULTS
The sample consisted of 16 young adults, with a mean age of 21.2 ± 3.4 years. Table 1 presents the variables which were veriied and analyzed before the application of respiratory muscle exercise. stasis; 1 - residue illed until 50% of the vallecula;
2 - residue illed more than 50% of the vallecula.
• Residue in piriform sinus (stasis of the bolus in
piriform sinus after complete swallowing): 0 - no
stasis; 1 - mild to moderate stasis; 2 - Severe
stasis, illing the piriform sinus.
• Penetration/Aspiration: 0 - Normal; 1 -
penetration; 2 - aspiration.
The variables were analyzed by two blinded evaluators, with ive years of experience regarding VFSE analysis.
The training with breathing exercise was carried out at home, with previous recommendations given by a physiotherapist, through IS in Respiron® low for a period of seven consecutive days. For the inspiratory training all participants had to perform three sets of ten daily repetitions, starting from functional residual capacity (FRC) until reaching the inspiratory capacity (IC) and hold the ball for a period of ive to eight seconds15.
On the other hand for the expiratory training, Respiron® was used upside down. Each participant was asked to perform three sets of ten daily repeti
-tions, starting from IC until reaching FRC, with one minute of rest between each inspiratory and expiratory series16.
Table 1 – Characterization of the biomechanics of swallowing of the study sample Subject Age Number of
swallowing PTT
Post- swallowing VL Residue
Post-swallowing
PS Residue P/A
1 24 0 0,53 0 0 0
2 25 2 1,17 0 0 0
3 22 0 0,75 1 0 0
4 24 0 0,43 0 0 0
5 20 1 0,57 1 0 0
6 18 0 0,37 0 0 0
7 19 1 0,63 0 0 0
8 30 1 0,57 0 0 0
9 19 1 0,43 0 0 0
10 19 1 0,54 0 0 0
11 18 1 0,40 0 0 0
12 19 0 0,63 0 0 0
13 24 0 0,73 0 0 0
14 21 0 0,50 1 0 0
15 18 0 0,83 0 0 0
16 20 0 0,63 0 0 0
adults, none had episodes of penetration and/or
aspiration.
In the analysis of the evaluators, we observed that for PTT variable the evaluators obtained 100% agreement (p = 1.00), which indicates an almost perfect agreement. The agreement indexes of the visual-perceptual variables are shown in Table 2:
Considering the time variable, it is possible to
verify that PTT occurred at 0.62 ± 0.19 seconds – on average. On the other hand, for the visual-perceptual variables, it was observed that most subjects had only one swallow (56.2%), 81.2% showed no residue in vallecula and only 6.2% in piriform sinuses. Since this is a sample which is composed of healthy young
Table 2 – Agreement among evaluators visual-perceptual variables pre and post and respiratory muscle exercise
Variables Kappa P
Number of swallowing Pre 1,00 <0,001
Post 1,00 <0,001
Post- swallowing VL Residue Pre 1,00 <0,001
Post 1,00 <0,001
Post-swallowing PS Residue Pre 1,00 <0,001
Post 1,00 <0,001
P/A Pre 1,00 <0,001
Post 1,00 <0,001
P/A – penetration/aspiration, PS - piriform sinuses, PTT - pharyngeal transition time, VL - vallecula.
We veriied that the Kappa values were high and signiicant, showing that in the analysis of visual-perceptual variables the evaluators were 100% identical, which indicates an almost perfect
agreement.
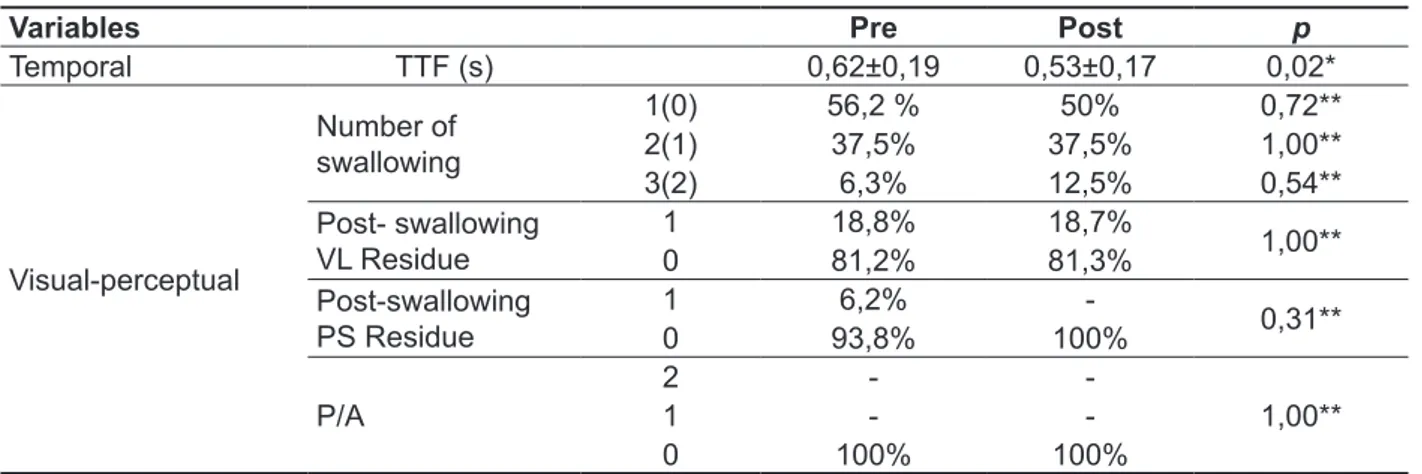
Table 3 presents the values related to swallowing biomechanics variables. They were analyzed before and after respiratory muscle exercise with Respiron®.
Table 3 – Variables analyzed pre and post respiratory muscle exercise
Variables Pre Post p
Temporal TTF (s) 0,62±0,19 0,53±0,17 0,02*
Visual-perceptual
Number of swallowing
1(0) 56,2 % 50% 0,72** 2(1) 37,5% 37,5% 1,00** 3(2) 6,3% 12,5% 0,54**
Post- swallowing
VL Residue 10 18,8%81,2% 18,7%81,3% 1,00**
Post-swallowing
PS Residue
1 6,2%
-0,31**
0 93,8% 100%
P/A
2 -
-1,00**
1 -
-0 100% 100%
to carry out TME with supportive equipment was reduced, with similar use to Respiron®, in parkin
-sonian subjects. In this work, the achievement of better performance and handling of laryngopha
-ryngeal structures was attributed to the increase in mobility of these structures, induced by muscle training and consequent strength gain. In this sense, no studies with large population samples were found. However, various studies have demonstrated signiicant gains in strength level of the respiratory muscles with the use of IR by Respiron®7,26,27 low.
Person et al.28 demonstrated in this regard, in a
study which was carried out in order to evaluate the efectiveness of maneuvers for swallowing in the activation of hyolaryngeal complex, through analysis of functional magnetic resonance imaging, favoring greater muscle coordination and gain in its ability to perform strength. These indings reinforce the idea
that it can be used in order to do muscle training
that primarily afects the capabilities of the rib cage to generate strength to increase the respiratory system functionality. But these indings also showed that, in a secondary way, their execution with suction or blowing action interferes with the mobility of the hyolaryngeal complex and pharyngeal transit.
From this, it is possible to conclude that the
decline in the PTT of the bolus of pasty consistency in the sample subjected to the respiratory training through incentive may be related to an increase in the mobility of the hyolaryngeal complex. In this case, the increase in this mobility may have occurred due to the training and strength gain of muscle structures of this complex. For Pilz et al.29,
any damage at this muscle strength, however minimal, represents a potential risk for penetration and/or laryngotracheal aspiration.
CONCLUSION
The use of IS seemed to produce efects on biomechanics of swallowing, especially in the time variable PTT, which decreased leading to better eiciency of swallowing, in the studied sample. In
relation to the visual-perceptual variables there
was a signiicant change in the residue in piriform sinuses variable, being eliminated any residue in the post training. And the number of swallow variable there was a slight increase in this amount when
comparing pre and post intervention.
It was possible to notice that the limitations found during the development of the study as the inability to perform spatial variable measures, in order to check the movement of the hyoid bone. This happens once there is no speciic software for this type of analysis. In addition, the authors suggest instrumental measurements that would evaluate
DISCUSSION
The agreement among evaluaters in this study was high and signiicant, demonstrating high reliability in the results found by the applied scale. As described in the study of Baijens et al.14, in which
evaluators obtained almost perfect agreement
regarding visual-perceptual variables among
intra-evaluators (0.8 to 1.0).
Although it is possible to determine the physi
-ology of swallowing, its dynamics may vary in some aspects in each individual, making it diicult to deine the normative data. Some authors consider the value of 17.5 seconds for normal swallowing - for pasty consistency, and that since the opening of the oral cavity to receive the food until the last pass of it through the upper esophagus.
It is also possible to ind a time of 4 seconds for liquid consistency17. However, the identiication of a
reference to the location of the pharyngeal phase iring is still an object of study, beyond the time of its phases. The study of temporal measures, through objective data, does not present a consensus about their reference values18-20 yet, ranging from 0.7 to
1.0 second21. Vale-Prodomo22 veriied that the time
of the mean time of the pharyngeal phase is 0.71
seconds.
In this study, it was observed in the studied sample, a mean of PTT even lower than those ones proposed by the literature before the application of the respiratory training (0.62 ± 0.19 seconds). These data are important in order to contribute to the establishment of normal parameters that allow the formation of a control to other studies with young adults of similar age and gender.
In relation to the efects of the breathing exercise on swallowing biomechanics, no signiicant diference on the PTT was noticed, reducing it about 0.09 seconds after the training. Studies that have used IS by low on the analyzed variables were not found in the literature up till now. However, previous studies that used expiratory muscle training (TME), by means of incentive spirometer with pressure linear load, showed satisfactory results on the biomechanics of swallowing.
Studies have shown that TME improves the vertical movement of the hyoid bone because it favors a greater activation and strength of submental muscles, which results in better laryngeal elevation and opening of the upper esophageal sphincter22-24.
Pitts et al.25 still state that a greater mobility of the
hyoid obtained by TME promotes muscle coordi
-nation of the structures related to swallowing, which
also causes an increase in subglottic pressure.
Troche et al.5 reported that the airway protection
were not found in the literature, which limited the theoretical study and discussion of this study. Thus, we suggest further studies addressing the use of IS related to the biomechanics of swallowing.
laryngeal sensitivity, together with the evaluation of respiratory muscle strength before and after using IS to establish correlations between these evaluations.
Studies that have used the Respiron® and its efects on swallowing or treatment of dysphagia
REFERENCES
1. Chaves RD, Carvalho CRF, Cukier A, Stelmach R, Andrade CRF. Sintomas indicativos de disfagia em portadores de DPOC. J Bras Pneumol. 2011;37(2):176-83.
2. Dozier TS, Brodsky MB, Michel Y, Walters BC, Martin-Harris B. Coordination of swallowing and respiration in normal sequential cup swallows. Laryngoscope. 2006;116(8):1489-93.
3. Costa M. Deglutição & Disfagia: bases morfofuncionais e videoluoroscópicas. Rio de Janeiro: Med Book; 2013.
4. Steele CM, Miller AJ. Sensory input pathways and mechanisms in swallowing: a review. Dysphagia.
2010;25:323-33.
5. Troche MS, Okaun MS, Rosenbek JC, Musson N, Fernandez HH, Rodriquez R et al.. Aspiration and swallowing in Parkinson disease and rehabilitation with EMST. Neurology. 2010;75:1912-9.
6. Romanini W, Muller AP, Carvalho KAT, Olandoski M, Faria-Neto JR, Mendes FL et al.. Os efeitos da
pressão positiva intermitente e do incentivador respiratório no pós-operatório de revascularização
miocárdica. Arq Bras Cardiol. 2007;89(2):105-10.
7. Lunardi AC, Porras DC, Barbosa R, Paisani DM, Silva CM, Tanaka C et al. Efect of volume-oriented versus low-oriented incentive spiromtry on chest wall volumes, inspiratory muscle activity, and thoracoabdominal synchrony in the elderly. Respir
Care. 2014;59(3):420-6.
8. Renault J, Costa-Val R, Rossetti MB, Houri Neto MA. Comparação entre Exercícios de Respiração Profunda e Espirometria de Incentivo no Pós – Operatório de Cirurgia de Revascularização
do Miocárdio. Rev Bras Cir Cardiovasc. 2009;24(2):165-72.
9. Azeredo AC. Fisioterapia respiratória do hospital geral. Rio de Janeiro: Manole; 2000.
10. Costa D. Fisioterapia Respiratória Básica. São Paulo: Atheneu; 1999.
11. Rosa R, Santos GK, Siqueira AB, Toneloto MGC. Inspirômetro de incentivo invertido como exercitador
da musculatura respiratória em indivíduos saudáveis. Rev Intellectus. 2013;25:177-97.
12. Deljo E, Filipovic M, Babacic R, Grabus J. Correlation analysis of the hyoid bone position in
relationto the cranial base, mandible and cervical
part of vertebra with particular reference to bimaxillary relations / teleroentgenogram analysis. Acta Inform Med. 2012;20(1):25-31.
RESUMO
Objetivo: analisar os efeitos do exercício respiratórios na biomecânica da deglutição de sujeitos
normais. Métodos: o exercício muscular respiratório em sujeitos normais foi aplicado por sete dias
consecutivos por meio de incentivador respiratório a luxo (três séries de dez repetições para inspi
-ração e expi-ração). A biomecânica da deglutição foi avaliada por videoluoroscopia, utilizando vari
-áveis temporais (tempo de transição faríngea) e visuoperceptuais (número de deglutições, resíduos em seios piriformes e valéculas, penetração/aspiração). Para análise estatística foi aplicado o Teste de Wilcoxon, Igualdade de Duas Proporções e Kappa. Resultados: foram avaliadas 16 jovens do
sexo feminino com média de idade de 21,2±3,4 anos. Nas variáveis visuoperceptuais observou-se concordância quase perfeita entre os avaliadores (p<0,001), bem como na temporal (p = 1,00). Após o período de treinamento houve redução no tempo de transição faríngea (p=0,02). Conclusão: o
uso de incentivador respiratório a luxo inluenciou signiicantemente na biomecânica da deglutição, principalmente na redução do tempo de transição faríngea.
DESCRITORES: Deglutição; Métodos; Exercício Respiratório; Fluoroscopia; Transtornos da
during swallow and expiratory pressure threshold training tasks. Dysphagia. 2007;22:108-16.
23. Wheeler-Hegland KM, Rosenbek JC, Sapienza CM. SumentalsEMG and hyoid movement during Mendelsohn maneuver, efortful swallow, and expiratory muscle strength training. J Speech, Language, and Hearing Research. 2008;51:1072-87. 24. Laciuga H, Rosenbek JC, Davenport PW,
Sapienza CM. Functional outcomes associated
with expiratory muscle strength training: narrative review. J of Rehabilitation Research & Development.
2014;51(4):535-46.
25. Pitts T, Bolser D, Rosenbek J, Troche M, Okun MS, Sapienza C. Impact of expiratory muscle strength training on voluntary cough and swallow function in Parkinson disease. Chest. 2009;135:1301-8. 26. Oliveira M, Santos C, Oliveira C, Ribas D. Efeitos da técnica expansiva e incentivador respiratório na força da musculatura respiratória em idosos
institucionalizados. Fisioter Mov. 2013;26(1):133-40.
27. Souza HCM. Efeitos do treinamento muscular inspiratório sobre a função pulmonar em idosas [dissertação]. Recife (PE): Universidade Federal de
Pernambuco; 2013.
28. Pearson WG, Hindson DF, Langmore SE, Zumwalt AC. Evaluating swallowing muscles essential for hyolaryngeal elevation by using muscle functional magnetic resonance imaging. Int J Radiation Oncol Biol Phys. 2013;85(3):735-40. 29. Pilz W, BaijensL WJ, Passos VL, Verdonschot R, Wesseling F, Roodenburg N et al. Swallowing assessment in myotonic dystrophy type 1 using iberoptic endoscopic evaluation of swallowing
(FEES). Neuromuscul Disord. 2014;24(12):1054-62.
13. Kahrilas PJ, Lin S, Rademaker A, Logemann J. Impaired deglutitive airway protection: a videoluoroscopic analysis of severity and mechanism. Gastroenterology. 1997;113(5):1457-64.
14. Baijens LWJ, Speyer R, Passos VL, Pilz W, Roodengurg N, Clave P. Swallowing in Parkinson patients versus healthy controls:
reliability of measurements in videoluoroscopy. Gastroenterology Research and Practice 2011. Article ID 380682.
15. Ysayama L, Lopes LR, Silva AMO, Andreollo NA. A inluência do treinamento muscular respiratório
pré-operatório na recuperação de pacientes
submetidos à esofagectomia. Arq Bras Cir Dig. 2008;21(2):61-4.
16. Landis JR, Koch GG. The Measurement of Observer Agreement for Categorical Data.
Biometrics. 1977;33:159-74.
17. Padovani AR, Moraes DP, Mangili LD, Andrade CR. Protocolo fonoaudiológico de avaliação do risco para disfagia (PARD). Rev Soc Bras Fonoaudiol.
2007;12(3):199-205.
18. Stephen JR, Taves DH, Smith RC, Martin RE. Bolus location at the initiation of the pharyngeal stage of swallowing in healthy older adults. Dysphagia.
2005;20(4):266-72.
19. Takase EM. Avaliação da deglutição de
alimentos e cápsulas gelatinosas duras em adultos assintomáticos [dissertação]. São Paulo (SP): Universidade Estadual de Campinas; 2013.
20. Douglas CR. Fisiologia aplicada à Fonoaudiologia. 2ª Ed. Rio de Janeiro: Guanabara
Koogan; 2006.
21. Vale-Prodomo LP. Caracterização videoluoroscópica da fase faríngea da deglutição
[tese]. São Paulo (SP): Fundação Antonio Prudente; 2010.
22. Wheeler KM, Chiara T, Sapienza CM. Surface electromyographic activity of the submental muscles
http://dx.doi.org/10.1590/1982-0216201517621514
Received on: December 19, 2014 Accepted on: September 21, 2105
Mailing address:
João Rafael Sauzem Machado
Av. Roraima, 1000 - Centro de Ciências da Saúde -
Prédio 26-A, 2º andar, sala 1432 Santa Maria – RS – Brasil CEP: 97015-000