w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Incidence
of
anismus
in
fecal
incontinence
patients
evaluated
at
a
Coloproctology
service
夽
Larissa
Sokol
Rotta
a,
Doryane
Maria
dos
Reis
Lima
a,b,c,d,∗,
Dayanne
Alba
Chiumento
a,
Univaldo
Etsuo
Sagae
a,c,e,faFaculdadeAssisGurgacz(FAG),Cascavel,PR,Brazil
bUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
cGastroclínicaCascavel,Cascavel,PR,Brazil
dSectorofAnorectalPhysiology,GastroclínicaCascavel,Cascavel,PR,Brazil
eUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
fUniversidadeEstadualdoOestedoParaná(UNIOESTE),Cascavel,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14May2014 Accepted3March2015 Availableonline27May2015
Keywords:
Fecalincontinence Pelvicfloor Manometry
a
b
s
t
r
a
c
t
Introduction:Fecalincontinenceisdefinedasalossofbladderandbowelcontrol.Anismusis characterizedbyaparadoxicalcontractionorinappropriaterelaxationofpelvicfloor mus-cleswhiletryingtoevacuate,beingusuallyassociatedwithconstipation(60%).However, anismuscanbepresentin46%ofpatientswithfecalincontinence.
Objective:Toanalyzetheincidenceofanismusinpatientsdiagnosedwithfecalincontinence inanoutpatientColoproctologyClinicofParaná.
Methodology:Aretrospectivestudyof66patientsdiagnosedwithfecalincontinenceat Colo-proctologyClinic,HospitalSãoLucas,fromFebruary2012toOctober2013.Patientswere evaluatedbyclinicalhistoryandexaminationbyanorectalelectromanometry.
Results:Themeanageofparticipantswas56years.Regardingtheevaluationbyanorectal electromanometry,meanrestingpressure,contractionpressureandsustainedcontraction pressurewere,respectively,35.18mmHg,90.53mmHgand58mmHg.Anismuswasseenin 42.42%ofpatients.
Conclusion: Throughthisstudy,itcanbeinferredthattheincidenceofanismushasa rel-evantimpactonpatientsdiagnosedwithfecalincontinence.Ourresultscorroboratethe importanceoftheconcomitantmanagementofanorectalcontinencemechanismchanges, inordertoemphasizetheclinicalbenefitsandimprovedqualityoflifeforpatientswith fecalincontinence.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
夽
ThisstudywasconductedatGastroclínicaCascavelandFaculdadeAssisGurgacz(FAG),Cascavel,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.M.d.R.Lima).
http://dx.doi.org/10.1016/j.jcol.2015.03.001
Incidência
de
anismus
em
pacientes
com
incontinência
fecal
avaliados
em
um
servic¸o
de
coloproctologia
Palavras-chave:
Incontinênciafecal Assoalhopélvico Manometria
r
e
s
u
m
o
Introduc¸ão: Incontinênciafecal(IF)édefinidacomoaperdadocontroleesfincteriano.O anismuscaracteriza-secomocontrac¸ãoparadoxalourelaxamentoinadequadoda muscu-laturadoassoalhopélvicoduranteatentativadeevacuar,estandogeralmenteassociadoà obstipac¸ãointestinal(60%).Noentanto,podeestarpresenteem46%dospacientescomIF.
Objetivo: Analisaraincidênciadeanismusempacientesdiagnosticadoscomincontinência fecalemumambulatóriodeColoproctologiadoParaná.
Metodologia: Estudoretrospectivoenvolvendo66pacientescomincontinênciafecal diag-nosticadosentrefevereirode2012eoutubrode2013.Ospacientesforamavaliadospela históriaclínicaepeloexamedeeletromanometriaanorretal(EMAR).
Resultados: Aidademédiadosindivíduosestudadosfoide56anos.Quantoàavaliac¸ãoda eletromanometriaanorretal,asmédiasdapressãoderepouso,decontrac¸ãoedecontrac¸ão sustentadaforam,respectivamente,35,18mmHg,90,53mmHge58mmHg.Anismusfoi evi-denciadoem42,42%dospacientes.
Conclusão: Atravésdesteestudo,foipossívelinferirqueaincidênciadeanismusérelevante empacientesdiagnosticadoscomincontinênciafecal,concorrendoassimpararessaltara importânciadomanejoconcomitantedasalterac¸õesdomecanismodecontinência anorre-tal,afimdesalientarosbenefíciosclínicoseamelhoranaqualidadedevidadospacientes comincontinênciafecal.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Fecal incontinence (FI) is defined as the loss of sphincter control or an inability in delaying an evacuation in situ-ations where the patient is not in a proper condition for suchaction,resultinginanunexpectedlossofgasorliquid and/orsolidfeces.1 Itsexactincidenceinthe populationis
unknown,butisestimatedthatFIaffects0.1–18%of individ-uals.Thesefiguresundoubtedlyareunderestimationsand,in part,thisisduetopatients’difficultyinreportingtheirclinical complaints.2,3
Thisconditionisconsideredaspartofacomplex etiopatho-genesisandphysiology.Itisknown thatthemechanismof analcontinencedependsonananalsphincterandpelvicfloor muscles’integratedaction,4presenceofrecto-analinhibitory
reflex,rectalability,sensitivityandcompliance,stool consis-tencyandboweltransittime.2Thus,conditionsordiseases
thatchangeanyofthesemechanisms,withlossof physiolog-icalcontrolofevacuation, mayleadtoafecalincontinence status. Traumatic causes are most common;among them, obstetricinjuryisanimportantfactoramongwomen.5
Theevaluationofanincontinentpatientbeginswitha thor-ough medicalhistoryand physicalexamination.2 Basedon
patient’sclinicalhistory,oneshoulddeterminethedegreeofFI withtheuseofavailablegradingscales,amongwhichthemost usedistheJorge-WexnerFecalIncontinenceScore.5Thisscore
classifiesincontinencefrom0to20,basedonthefrequencyof episodesofincontinenceproducinggasandliquidand/orsolid stools,aswellasonchangesinqualityoflife,whereineachof thesecriteriaaregradedfrom0to4(1,seldom;2,sometimes; 3,weekly;4,daily).6
Alongside the medical history – the primary diagnostic method–thecoloproctologistcanuse aseriesofanorectal examsthathelptounderstandthiscondition.Amongthese, anorectalelectromanometry(AREM),animportantfunctional methodforFIevaluation,7standsout,consideringthatAREM
measuresrestandcontractionpressuresandfunctionalanal canalsize,capacityand compliance,aswell asasurveyof rectum-anal inhibitoryreflex.Furthermore,AREMpromotes an interpretation of the synchronization of sensitive and motoranalcanalcomponents.8
Thus,itisknownthattheanalsphincterfunction assess-mentiscriticalforadiagnosisandtherapeuticapproachfor fecalincontinence;inthisscenario,AREMiscriticalforthis assessment.9
Ontheother hand,anismus,orpelvicfloordyssynergia, canbedefinedasaparadoxicalcontractionorinappropriate relaxationofpelvicfloormuscleswhiletheindividualistrying toevacuate,orasaninadequatepropulsiveforce.10Anismus
manifests itself asa failure in normalrelaxation ofpelvic floor muscles duringdefecation, and this can beassessed by an anorectal electromyography (AREM) test, defecogra-phy, nuclear magnetic resonance and dynamic anorectal ultrasound.11,12 This syndrome is usually associated with
constipation,11,13,14inwhichanismuscanbefoundin60%of
thesepatientsand,incontrast,in46%ofpatientswithfecal incontinence.14
AccordingtoChiarioni etal.,15 theuse ofbiofeedbackis
normalization ofrectal pressure functions and pelvicfloor contractions.16
Thesuccessofthisapproachisattributedtothe restora-tionofanormaldefecationdynamics.17Moststudiesonpelvic
floorre-educationtherapyshowedgoodefficiency,including improvementinrectalsphincterfunctionandinrectal sensi-tivity,psychologicalimprovementandabetterqualityoflife forpatientswithFIandanismus.18
Objective
This study aims to analyze the incidence of anismus in patientsdiagnosedwithfecalincontinencyinanoutpatient ColoproctologyClinicofParaná.
Methodology
Thisisaretrospectivestudyinvolving66patientswithfecal incontinence that were clinically evaluated and had been diagnosedbyJorge-WexnerFecalIncontinenceScore6 atan
outpatientColoproctologyclinicinthestateofParanáfrom February2012toOctober2013.
Thestudyincludedpatientsofbothgenders,agedbetween 18 and 75 years, with a Jorge-Wexner Fecal Incontinence Score>8.Then,selectedpatientswereanalyzedaccordingto resultsofananorectalelectromanometry(AREM)testfound intheclinicdatabase.AREMwasperformedwiththepatient in left lateral decubitus, without previous rectal prepara-tion,usingacontinuouswaterperfusion,8-channelDynamed eletromanometer.Theexaminationswereperformedbytwo proctologists (DL and GK). The pressures were measured along the length of the functional anal canal, using only thehigh-pressureandstatictractionzone.Intheanalysisof AREMresults,thestudyendpointsincludedrestingpressure (RP)(40–70mmHg),contractionpressure(CP)(100–200mmHg), sustainedcontractionpressure(SCP),rectosphinctericreflex (RSR) (present or absent), rectal sensitivity (10–50mL), rec-talcapacity(180–300mL)andskeletalmuscleevaluationwith straining(presenceorabsenceofanismus).Presenceof anis-muswasconsideredwhenthestrainingepisoderesultedin anincreaseofpressureofsphinctermusclesinrelationto res-tingpressure.Allparameterswereevaluatedinaminimumof threetimes.
Duringtheclinicalhistory,presenceofvaginalbirthsand anorectalsurgerieswasalsoevaluated.
Patients who had a Jorge-Wexner Fecal Incontinence Score <8, patients with neoplasia, patients with prior or current history of radiotherapy, neurological disorders and presenceofaninflammatory-infectiouscondition were ex-cluded.
After an individual analysis of variables, patients were divided into2groups: Group1–patients withFIand with anismus;andGroup2–patientswithFIandwithoutanismus. Then,resting(RP)andcontraction(CP)pressuresfromAREM werecomparedbetweengroups.
Theinformationinthisstudywasobtainedina confiden-tialmannerwithrespecttotheperiodofpatients’assessment and data analysis. Statistical analysis was performed by
100
75
25
0
Without anismus
Resting pressure
With anismus
50
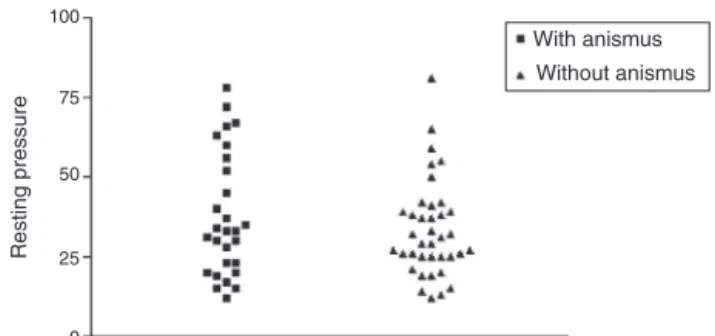
Fig.1–ComparisonofRPmeansbetweengroupsof patients:FIwithanismus×FIwithoutanismus(p=0.4013).
applyingtheStudent’sttestusingPrism5.0platformfor com-parison of study variables. This study was submitted and approved by the Research Ethics Committee of Faculdade AssisGurgaczthroughPlataformaBrasil,anationwide,unified database(opinionnumber:643983).
Results
Thestudiedgroup consistedof66patients diagnosedwith fecalincontinence:63women(95.45%)and3men(4.55%)with ameanageof56(29–75)years.Astowomen,56(84.84%)had ahistoryofvaginalbirthand13(19.69%)underwentanorectal surgery.
As to the assessment of anorectal electromanometry (AREM),meanRPwas35.18(12–81)mmHg;3patients(4.50%) presentedwithrestinghypertoniaand47(71.20%)withresting hypotonia.Ontheotherhand,duringCPevaluation,themean forthisvariablewas90.53(17–217)mmHg;2(3.03%)patients showedhypertoniccontractionand43(65.15%)hypotonic con-traction.SCPhadameanof58(16–157)mmHg.
Consideringallparticipants,65(98.48%)patientsexhibited rectosphinctericreflexand1(1.51%)didnotshowthisreflex duringAREM.Regarding rectalsensitivity,10(15.15%)and2 (3.03%) patients, respectively, had values above and below normalvalues(50and 20mL).Inrectalcapacityevaluation, 7(10.60%)and17(24.24%)patients,respectively,hadvalues aboveandbelowrecommendedlevels(300and160mL). Anis-muswasevidencedin28(42.42%)ofpatientsevaluatedwith fecalincontinence.
ThemeanrestingpressuresmeasuredbyAREMforpatients with FI with versus without anismus were, respectively, 37±19.29and33.37±15.01.WhenRPvaluesofthesegroups were compared (Fig. 1), there was no statistically signifi-cantdifference(p=0.4013).Themeancontraction pressures measured by AREMfor patients withFI withanismus ver-sus without anismus were, respectively, 99.39±45.63 and 84.00±48.15. When CP values of these groups were com-pared(Fig.2),therewasnostatisticallysignificantdifference in(p=0.8788).
Discussion
100 200 300 0 Without anismus Resting pressure With anismus
Fig.2–ComparisonofCPmeansbetweengroupsof patients:FIwithanismus×FIwithoutanismus(p=0.8788).
andresultinginlesserqualityoflife.Fecalcontinenceisthe resultofacoordinatedactivitybetweentherectumandanal sphincters,anddependsnotonlyofthesefactors,butalsoof rectalsensitivity,intestinaltransittime,stoolconsistencyand rectalreservoirconditions.19
Thepelvicfloordysfunctionsyndromewithoutanatomical changes,knownasanismus,ischaracterizedbytheabsence ofrelaxationorbyaparadoxical contractionofpelvicfloor musclesorspasmsofelevatormusclesofanus.21
This study aimed to analyze the incidence of anismus inpatients diagnosed with fecal incontinence, considering that,notwithstandingtherelationshipbetweenanismusand constipation,11,13,14anismuscanalsomanifestitselfinother
anorectaldisorders.Thus,patientswillobtainclinicalbenefits andanimprovedqualityoflifeifthemanagementofthese changes in anorectal continence mechanism is addressed concurrently.
Theincidence ofanismus followed the trend published inthe literature11,14; thepresent study foundacorrelation
betweenanismus and fecalincontinence in42.42%, which agreeswiththestudyofSchoutenetal.14
Stillinregardtotheevaluationofanorectal electromanom-etry(AREM),thestudyshowedthat71.20%ofpatientssuffered fromrestinghypotoniaand65.15%showedhypotoniaof con-traction,correspondingtothefindingsinthestudybyBalsamo etal.,8inwhichrestingandcontractionpressuresarelowerin
incontinentindividuals.
Theneedforacomprehensiveapproachofpatientswith fecal incontinence for pelvicfloor disorders is based on a constantpursueforclinicalimprovement.AccordingtoRao etal.,18patientsundergoingBiofeedbackforanismusandFI
treatmentexhibitedimprovedsphincterfunctionandrectal sensitivity,psychologicalimprovementandabetterqualityof life.
Thus,itcanbeinferredthatthepresentstudyshowed sim-ilarresultstothoseavailableincontemporaryliterature,for instance, inthe study bySchouten et al.,14 confirming the
relevanceofthediagnosisofanismusinFIpatients,sothat onecandesignanassociatedtherapeuticplanaimedat re-educationofpelvicfloormusclesandoptimizationofclinical response.
Conclusion
Through this study, we can infer the importance of the incidence of anismus in patients diagnosed with fecal
incontinence;andthatthedetectionoffunctionalchangesis importantforthetreatmentofpatientswithFI,sotheycanbe clinicallybenefitedandgetabetterqualityoflife.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BalsamoF,RamaciottiPR,PozzobonBH.Correlac¸ãoentre
achadosmanométricosesintomatologianaincontinência
fecal.RevBrasColoproctol.2011;31(1):39–43.
2.OliveiraL.Fecalincontinence.JBrasGastroenterol.
2006;6(1):35–7.
3.AlsheikEH,CoyneT,HawesSK,MerikhiL,NaplesSP,
KanagarajanN,etal.FecalIncontinence:prevalence,severity
andqualityoflifedatafromanoutpatientgastroenterology
practice.GastrResPract.2012;2012:947694.
4.CirizaDeLosRíosC,RuizDeLeónSanJuanA,Díaz-Rubio
GarcíaM,TomásMorosE,GarcíaDuránF,Mu ˜nozYagüeT,
etal.Differencesinthepressureofcanalanalandrectal
sensitivityinpatientswithfecalincontinence,chronic
constipationandhealthysubjects.RevEspEnfermDig.
2010;102(12):683–90.
5.CarvalhoLP,CorletaOC,MallmannACM,KoshimizuRT,
SpolavoriA.Neuropatiapudenda:correlac¸ãocomdados
demográficos,índicedegravidadeeparâmetrospressóricos
empacientescomincontinênciafecal.ArqGastroenterol.
2002;39(3):139–46.
6.JorgeJMN,WexnerSD.Etiologyandmanagementoffecal
incontinence.DisColonRectum.1993;36(1):77–97.
7.VoderholzerWA,NeuhausDA,KlauserAG,TzavellaK,
SchindlbeckNE.Paradoxicalsphinctercontractionisrarely
indicativeofanismus.Gut.1997;41(2):258–62.
8.BalsamoF,FilhoPRR,PozzobonBHZ,CastroCAT,FormidaGJS.
Correlationbetweenmanometricfindingsand
symptomatologyinfecalincontinence.RevBrasColoproctol.
2011;31(1):39–43.
9.ArendMGP,FernandesWVB,ArendG.UsodoBiofeedbackna
incontinênciafecaledissinergiadoassoalhopélvico–relato
decaso.RevSaúdePesq.2009;2(3):433–6.
10.ViebigRG,FelixVN.Func¸ãoanorretalnormalealterada.São
Paulo:EditoraRedbStyle;2006.p.27.
11.CesarMAP,KlugWA,OrtizJA,BinFC,KapelhuchnikP.
Diagnosisoftheanismusthroughtheanorectalphysiology
tests.RevBrasColoproctol.2009;29(2):192–6.
12.Murad-RegadasSM,RegadasFS,RodriguesLV,SouzaMHLP,
LimaDMR,SilvaFRS,etal.Anovelproceduretoassess
anismususingthree-dimensionaldynamicanal
ultrasonography.ColorectalDis.2007;9:159–65.
13.KlauserAG,VoderholzerWA,HeinrichCA,SchindlbeckNE,
Müller-LissnerSA.Behavioralmodificationofcolonic
function.Canconstipationbelearned?DigDisSci.
1990;35(10):1271–5.
14.SchoutenWR,BrielJW,AuwerdaJJ,vanDamJH,GosselinkMJ,
GinaiAZ,etal.Anismus:factorfiction?DisColonRectum.
1997;40(9):1033–41.
15.ChiarioniG,FerriB,MorelliA,IantornoG,BassottiG.
Bio-feedbacktreatmentoffecalincontinence:wherearewe,
andwherearewegoing?WorldJGastroenterol.
2005;11(31):4771–5.
16.HeymenS,JonesKR,RingelY,ScarlettY,WhiteheadWE.
Biofeedbacktreatmentoffecalincontinence:acriticalreview.
17.WaldA,ChandraR,ChiponisD,GabelS.Anorectalfunction
andcontinencemechanismsinchildhoodencopresis.J
PediatrGastroenterolNutr.1986;5:346–51.
18.RaoSS,WelcherKD,PelsangRE.Effectsofbiofeedback
therapyonanorectalfunctioninobstructivedefecation.Dig
DisSci.1997;42(11):2197–205.
19.NortonC.Fecalincontinenceandbiofeedbacktherapy.Ther
GastroenterolClinNAm.2008;37(3):587–604.
20.NessW.Faecalincontinence:whatinfluencescare
andmanagementoptions?BrJNurs.2008;17(18):
1148–52.
21.RegadasFSP,Murad-RegadasSM.DistúrbiosFuncionais
doAssoalhoPélvico.AtlasdeUltra-sonografiaAnorretal
BieTridimensional.RiodeJaneiro:Revinter;2006.