www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Evaluation
of
postural
balance
in
mild
cognitive
impairment
through
a
three-dimensional
electromagnetic
system
夽
,
夽夽
Ana
Paula
Oliveira
Borges
a,b,∗,
José
Ailton
Oliveira
Carneiro
c,d,
José
Eduardo
Zaia
e,f,
Antonio
Adilton
Oliveira
Carneiro
g,h,
Osvaldo
Massaiti
Takayanagui
a,iaFaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),RibeirãoPreto,SP,Brazil bUniversidadedeFranca(UNIFRAN),Franca,SP,Brazil
cClinicalMedicine,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),RibeirãoPreto,SP,Brazil dUniversidadeEstadualdoSudoestedaBahia(UESB),Jequié,BA,Brazil
eBiologicalSciences,UniversidadeEstadualPaulista‘‘JúliodeMesquitaFilho’’(UNESP),SãoPaulo,SP,Brazil fMaster’sandDoctoratePrograminHealthPromotion,UniversidadedeFranca(UNIFRAN),Franca,SP,Brazil gUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
hDepartmentofPhysicsandMathematics,FaculdadedeFilosofia,CiênciaseLetrasdeRibeirãoPreto,UniversidadedeSãoPaulo
(FFCLRP-USP),RibeirãoPreto,SP,Brazil
iDepartmentofNeurosciencesandBehavioralSciences,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo
(FMRP-USP),RibeirãoPreto,SP,Brazil
Received8June2015;accepted17August2015 Availableonline23December2015
KEYWORDS Elderly; Mildcognitive impairment; Posturalbalance; Sensorydeprivation
Abstract
Introduction:Elderlypeoplewithcognitiveimpairmentareatgreaterriskforfalls;thus,an understandingoftheearlieststagesofcognitivedeclineisnecessary.
Objective: Tocompareposturalbalancebetweenelderlypeoplewithandwithoutmild cogni-tiveimpairmentusingathree-dimensionalsystem.
Methods:Thirty elderly people with mild cognitive impairment and thirty healthy elderly subjectswereselected.Staticposturographywasperformedusingthree-dimensional electro-magnetic equipmentandthefollowingparameterswereevaluated:maximumdisplacement, mean speed and total trajectory.Open- and closed-eyestabilometric variablecomparisons betweengroupsandwithineachgroupwerecarriedout,andarelationshipbetweentheMini MentalStateExaminationandthetotaltrajectoryofallelderlysubjectswasdetermined.
夽 Pleasecitethisarticleas:BorgesAPO,CarneiroJAO,ZaiaJE,CarneiroAAO,TakayanaguiOM.Evaluationofposturalbalanceinmild
cognitiveimpairmentthroughathree-dimensionalelectromagneticsystem.BrazJOtorhinolaryngol.2016;82:433---41.
夽夽Institution:DepartmentofPhysicsandMathematics,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),
RibeirãoPreto,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](A.P.O.Borges). http://dx.doi.org/10.1016/j.bjorl.2015.08.023
Results:Theanalysisamongopen-andclosed-eyeconditionsshowedasignificantdifference inmaximumanteroposteriordisplacementinthecontrolgroupandasignificantdifferencein all stabilometric variables inthe mild cognitive impairmentgroup. A significant difference between thegroups inallvariablesinthe closed-eyeconditionwas observed.There wasa strongcorrelationbetweencognitiveperformanceandtotaltrajectory.
Conclusion:Evaluations showed decrease in balance in elderly peoplewith mild cognitive impairment.Presenceofanteroposteriordisplacementcanbeanearlysignofpostural con-trolimpairment,andtheevaluationwith visualrestriction canbeuseful indetectingsmall posturalinstabilities.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Idoso;
Comprometimento cognitivoleve; Equilíbriopostural; Privac¸ãosensorial
Avaliac¸ãodoequilíbriocorporalnocomprometimentocognitivoleveatravésde sistemaeletromagnéticotridimensional
Resumo
Introduc¸ão:Idososcomalterac¸ãocognitivaapresentammaiorriscodequedas;assim,é impor-tantecompreenderasprimeirasfasesdodeclíniocognitivo.
Objetivo:Compararoequilíbriocorporalentreidososcomesemcomprometimentocognitivo leveatravésdeumsistematridimensional.
Método: Trinta idosos com comprometimento cognitivo leve e 30 idosos saudáveis foram selecionados.A posturografiaestáticafoirealizada utilizando equipamentoeletromagnético tridimensional,eforamavaliadososparâmetrosdeslocamentomáximo,velocidademédiae trajetóriatotal. Foirealizadacomparac¸ãodasvariáveis estabilométricascomolhoaberto e olho fechado intragrupo eintergrupos, e foiestabelecida arelac¸ão entreo MiniExame do EstadoMentaleatrajetóriatotaldetodososidosos.
Resultados: Aanáliseentreolhoabertoeolhofechadonogrupodecontroleevidenciouuma diferenc¸asignificativanodeslocamentoanteroposteriormáximo;nogrupocom comprometi-mentocognitivoleve,houvediferenc¸asignificativaemtodasasvariáveisestabilométricas.Foi observadadiferenc¸asignificativaentreosgrupos emtodasasvariáveisnacondic¸ãodeolho fechado.Houvefortecorrelac¸ãoentredesempenhocognitivoetrajetóriatotal.
Conclusão:As avaliac¸ões evidenciaram diminuic¸ão do equilíbrio nos idosos com compro-metimento cognitivo leve. O deslocamento anteroposterior pode ser um sinal precoce de comprometimentodocontrolepostural, eaavaliac¸ão comrestric¸ãovisual podeser útilna detecc¸ãodepequenasinstabilidadesposturais.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Thepresence of cognitiveimpairmentis amajorrisk fac-torforchangesinmotorperformanceandbodybalance.1---4 Studiesshowthattheincidenceoffallsinpeoplewith cog-nitive impairmentis estimated tobe twice theincidence in cognitively intact elderly people.5 A good approach to reducetheriskoffallsinthispopulationistogainan under-standingoftheearlystagesofcognitivedecline.
Mild cognitive impairment (MCI) is a clinical condition definedbyclinical,cognitiveandfunctionalcriteria.Inthis entity,there occursa greater cognitive declinethan that expected for an individual’s age and level of education, butthatdeclinedoes notinterferesignificantlywithdaily functionalactivities.6
Elderlypeople with MCI areat increased risk not only forconversiontodementia,butalsoforadeclinein mobil-ity and for suffering falls. Boyle et al.7 suggested that thesemotorchangesmayprecedethediagnosisofcognitive decline.Althoughthemechanismthatleadstoanincreased riskoffallsinpeoplesufferingcognitiveimpairmentisnot yetcompletelyunderstood,itisknownthatdeficienciesin cognitiveskillscanreduceattentionpaidtoposturalskills. Thus,MCIisanopportunitytointerveneinthetrajectoryof cognitiveandfunctionaldeclineintheelderly.8
Among the latest technologies usedin studies of body sway, the three-dimensional system of electromagnetic sensors detects smallbody movements, allowing a direct investigationofmotionkinematics,andhasalowercostand greaterportabilitythantheforceplatform.10---17
During the aging process, a number of changes occur in motor,sensory andcognitivesystems, thatresultin an increaseofbodysway.1,2Onewaytoassessthecontribution ofsensorysystemsinposturalcontrolisbymanipulatingthis informationduringstance.18
Inthissense,thebodyswayevaluationindifferent sen-sory conditions can be useful in detecting imbalance in elderlypatientswithMCI.Theaimofthisstudywasto com-parethestaticbodybalanceinelderlypopulationswithand without MCI,usingdatafroma three-dimensionalsystem, underopen-andclosed-eyeconditions.
Methods
Participants
Thisisacross-sectional,descriptiveandcomparativestudy. Two groups of 30 elderly subjects were defined: control group(elderlypeoplewithoutcognitiveimpairment)anda groupwithMCI.
Thesamplecalculationwascarriedoutbasedonasurvey ofthenumberofconsultationsandonpreviousstudies con-ductedintheoutpatientclinic,aswellasinestimatesbased ontheliterature,throughthestatisticalprogramG*Power 3.1®;anindicativesampleofat least27subjectsforeach groupwasobtained.
Participants intheMCI groupwereselectedsubsequent tomultidisciplinaryassessmentatouroutpatientclinic,and thecontrolgroupparticipantswereselectedfromother clin-icaldepartmentsfromthehospital.
Todefinethediagnosticgroups,theMCIgroupwas com-posedofelderlysubjectswithaclinicaldiagnosisaccording to criteriadeveloped by Petersen et al.19 These patients shouldshowsomecognitiveimpairment,withpredominance of mnemonic function (amnestic-type MCI), but without compromising their functional capacity. MCI patients also shouldshowabsenceofdementiabytheInternational Clas-sificationof Diseases10thedition(ICD-10)criteria,by the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV), through changes in the battery of neu-ropsychological tests, and by a Clinical Dementia Rating (CDR)=0.5.The controlgroupshouldnotexhibitevidence of cognitive or functional impairment, according to their clinicalandneuropsychologicalevaluation.20
Individualsofbothgenders,aged65---75years,matched forage,andwithaminimumoffouryearsofformal educa-tionwereincludedinourtwogroups.Elderlysubjectsusing metal devicesor a pacemaker inside the body, exhibiting memorychangessecondarytootherdegenerativediseases, withseverecardiovasculardisorder,anon-correctedvisual or hearing impairment, prior musculoskeletal and neuro-logicalchangesthatwouldinfluencethesubject’sbalance, vestibulardisorders,complaintsofdizzinessand/orvertigo, or the useof psychotropicdrugs were excludedfrom this study.Inaddition,individualswithasignificantdecreasein dailyactivities, history offalls (definedasan unexpected
eventinwhichthesubjectwillbepositionedontheground oronalowerlevelthanhis/herownlevel),21andambulatory deviceuserswerealsoexcludedfromthisstudy.
Afterthe approvalof this researchby theInstitutional EthicsCommittee(number5,156/2010), allsubjectswere informed about the evaluations and signed a free and informedconsentform.
Proceduresandinstruments
Atfirst,wecollectedpersonalandanthropometric informa-tion,aswellasinformationongeneralstateofhealthand cognitive performance by applying the Mini Mental State Examination(MMSE). An assessment of physical and func-tional performance was carried out, in order to become awareofthefunctionalaspectsoftheelderlyandtoexclude the possibility that potential sensory and motor deficits wouldcompromisethestaticbodybalancetest. Withthis in mind,the participants were submitted tothe Freiburg testof visual acuity(modified version),22 theDix-Hallpike maneuver23 and the Short Physical Performance Battery (SPPB),24 and a tuning forkwas bilaterallyapplied tothe mastoidprocess.
The static body balance was evaluated using the Polhemus® Patriotthree-dimensionalelectromagnetic sen-sorsystem(Fig.1).The positionandspatialorientationof the elderly were recorded in real time by plotting their movements in the anteroposterior, mediolateral and ver-tical axes (positions x, y, z and orientation angles , ϕ,
) betweenthe receiversensorattached onthesubject’s skinonthesacralregion(nearthecenterofmass),andthe transmittersensor,whichwasplacedonasupportuncoupled fromtheparticipant’sbody,atadistanceofapproximately 40cmandatthesameheightasthereceiversensor.10---14The dataacquiredbythesystemweretransferredtoanotebook viaanUSBinterface andwithaLabView 8.0environment throughaspecificsoftware.Samplingacquisitionfrequency wasof100Hz.
In order to establish a signal pattern and obtain reli-able data, the baseline shift of the Polhemus equipment
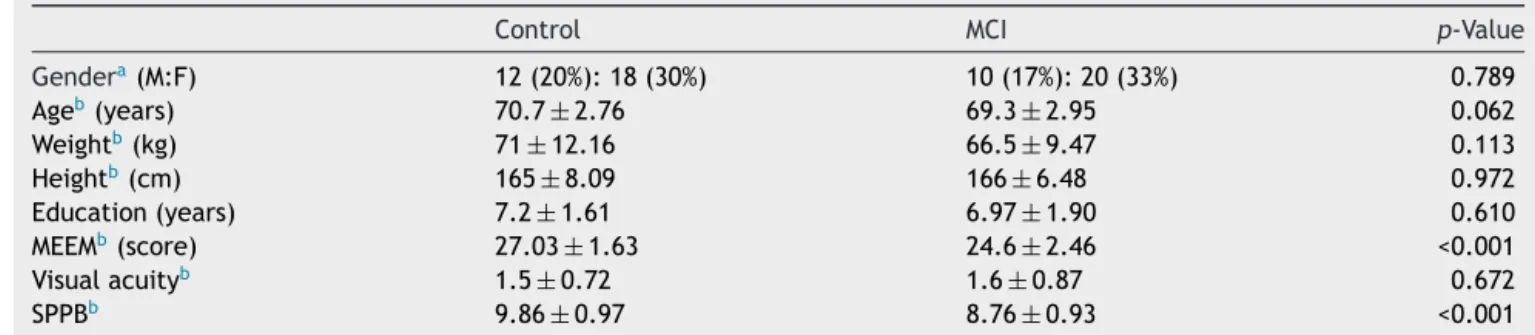
Table1 Demographicandanthropometriccharacteristics,MMSEscores,andphysicalandfunctionalcharacterizationin diag-nosticgroups.
Control MCI p-Value
Gendera(M:F) 12(20%):18(30%) 10(17%):20(33%) 0.789
Ageb(years) 70.7±2.76 69.3±2.95 0.062
Weightb(kg) 71±12.16 66.5±9.47 0.113
Heightb(cm) 165±8.09 166±6.48 0.972
Education(years) 7.2±1.61 6.97±1.90 0.610 MEEMb(score) 27.03
±1.63 24.6±2.46 <0.001 Visualacuityb 1.5±0.72 1.6±0.87 0.672
SPPBb 9.86
±0.97 8.76±0.93 <0.001
MCI,mildcognitiveimpairment;MMSE,MiniMentalStateExamination;SPPB,ShortPhysicalPerformanceBattery. aCardinalnumbersandpercentages.
b Mean
±standarddeviation.
wasverifiedandtheequipmentwascalibratedpriortothe evaluationbymovingthecoilofthesensor5cmforwardon aflatsurface.Consideringthatthethree-dimensional sys-temworks asa motion sensor, it should detect the same previouslyknowndisplacement.
Duringbodyswayassessment,theparticipantsremained in an orthostatic position,with bipedal support and with theirarms placedalongside the body,withbare feetin a side-by-sidepositionandparalleltothewidthofthepelvis, onawoodenplatform measuring1cm×50cm×50cmand keeping a distance of about 12cm between their heels duringtheevaluation.25 Additionally,allparticipantswere instructedtostandstillasmuchastheycouldandnotmove theirarms.Duringthetest,nocommunicationwasallowed. Thetestwasconductedintwosensoryconditionsfor60s foreachpositioninthefollowingorder:openeyes(OE)and closedeyes(CE)condition.InOEcondition,allparticipants wereinstructedtomaintaintheireyesfixedatapointplaced ateyelevelandatadistanceofonemeter.
Thebodyswayparameters(stabilometricvariables) ana-lyzedwere:maximumanteroposterior(AP)andmediolateral (ML) displacement, total trajectory, and total average speed.10---17Avariable/heightcalculationwasperformedfor statisticalanalysis, withdatacorrection for heightof the elderlysubjects.
Statisticalanalysis
To check sample homogeneity, we applied the Kolmogorov---Smirnov test. The comparisons of anthro-pometric, demographic, educational, and physical and functionalvariablesandMMSEscoresbetweencontroland MCI groups were carried out using the Student’s t test. ThegenderratioineachgroupwasverifiedbytheFischer Test. To compare stabilometric variables for OE and CE conditionswithineachgroup,theWilcoxontestwasused, andforthecomparisonbetweengroups,theMann---Whitney test was applied. Spearman coefficient was used to test the correlation between the variables with and without adjustment for the height of participants and between MMSE scores and total trajectory in those two sensory conditions.Statistical analyseswereconductedusingSPSS software(SPSSfor Windows,version16.0,SPSSInc.,USA), considering a 5% significance level. For preparation of
chartsweusedthestatisticalpackageOrigin®,version6.0 (Mi-crocalOrigin®,6.0,USA).
Results
InTable1,onecanseethattherewasnosignificant differ-encebetweenthediagnosticgroupsregardinggender,age, weight,height,andeducation;ontheotherhand,therewas asignificant differencein MMSEscores, anditcanalsobe observed that the elderly fromthe control group showed bettercognitiveperformance.Allelderlysubjectshadtheir proprioceptivesensitivitypreserved,anegativeresponseto Dix-Hallpike maneuver, preserved visual acuity preserved andtheymanagedtorealizetheSPPBtest.
Table 2 shows variables of body sway in groups in OE andCEconditions,andthecomparisonsbetweenintra-and intergroups’ sensoryconditions. The analysisbetween OE andCEinthecontrolgrouponlyshowedasignificant differ-enceinmaximum APdisplacement (p<0.01),while inthe MCI groupa significant differenceamongallstabilometric variableswasdetected(p<0.001).
When the comparison between groups was analyzed, therewasnosignificant difference betweenthe variables (p>0.05) in OE condition. In CE condition, we observed significant differences between groups for all variables (p<0.01).In thisstudy,variablescorrected for heightare notpresented,becauseoftheirstrongcorrelation(r:0.91; p<0.001)withuncorrectedvariables.
Fig.2shows statokinesiogram graphs,representing the total60-strajectoryofbodyswayinAPversustheMLaxisfor ahealthysubjectversusanelderlyMCIofthesamegender andwithhomogeneityofanthropometricvaluesindifferent sensoryconditions.By analyzing thesecharts onecan see thatthelesssensoryinformationtheelderlyhas,thegreater thebodyoscillation.
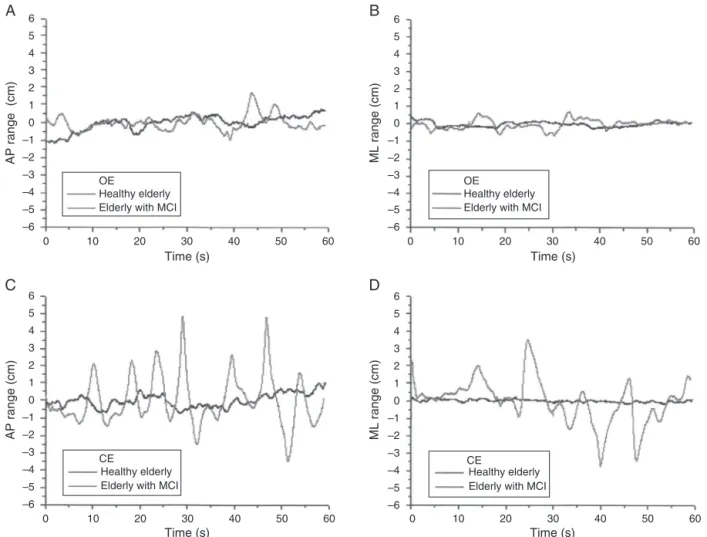
Fig.3 shows the stabilogramof the same elderly sub-jectsindifferentsensoryconditions.Thegraphshows the rangesofbodyswayinrelationtotheacquisitiontimeinAP andMLaxes.Stabilogramsallowtheidentificationofthose test periods in which the individual has obtained greater oscillationpeaks(higherriskoffalls).
Table2 Parametersofbodyswayofthetwostudygroups indifferentsensoryconditions.
Posturalsway
OE CE p-Valuea
MaxAPdispl(cm)
Control 1.45±0.42 1.92±0.81 <0.01 MCI 1.61±0.40 6.04±1.89 <0.001
p-Valueb 0.062 <0.001 MaxMLdispl(cm)
Control 0.93±0.43 1.25±1.11 0.070 MCI 1.08±0.28 4.36±2.24 <0.001
p-Valueb 0.084 <0.001 Totaltrajectory(cm)
Control 65.04±31.98 68.14±29.17 0.199 MCI 65.53±40.57 117.17±35.43 <0.001
p-Valueb 0.517 <0.001 Totavspeed(cm/s)
Control 1.07±0.56 1.15±0.49 0.264 MCI 1.09±0.38 1.97±0.60 <0.01
p-Valueb 0.451 <0.01
MCI,mildcognitiveimpairment;MaxAPdispl,maximum antero-posteriordisplacement; MaxMLdispl, maximummediolateral displacement;Totavspeed,totalaveragespeed;OE,openeyes; CE,closedeyes.
a p-ValuesinthecolumnaccordingtopairedWilcoxontest. b p-ValuesinlinesaccordingtoMann---Whitneytest.
to the finding of a significant correlation (OE: r −0.65; p<0.01andCE:r:−0.92;p<0.01);and,astheMMSEvalue increased,thevalue ofthetotaltrajectorydiminishedfor theentiresample.
Discussion
Although much research has been devoted to the study of falls in elderly patients with dementia (mostly with
Azheimer’s Disease), few studies have addressed elderly people with MCI. Consequently, the incidence of falls in thispopulationandtheirriskfactorsremainpoorlydefined. In this study, the static postural control of subjects in a standingposition and its changes in the presence of MCI wereexamined.Traditionally,thestandingpositionhasbeen quantifiedusingcharacteristics of bodysway andchanges inthepressurecenter.Recently,however,new technologi-caldevicesforthisevaluationhavebeenevaluated.Tothe extent of ourknowledge, thiswas the firststudy to ana-lyzestaticbodybalanceinelderlypeoplewithMCIusinga three-dimensionalsysteminsensoryconditionsOEandCE, andtheanalysisof ourfindingsrevealed poorerbody bal-anceinthatgroup,inagreementwithotherposturographic studiesconductedinthispopulation.26,27
For the conduction of this study, 60 elderly subjects wereselected. The proportions of men and women were similarinbothgroups; thus,thedifferencesthatcouldbe observedbetweengroupswouldnotbeattributedto differ-encesingenderdistribution.Otherstudiesutilizedasimilar design.3,4,26 The age distributionwas homogeneousin our groups;thus,the effectofthis variableintheresults was controlled,sinceageisaknownriskfactor forfalls. Also, significantdifferencesbetweenthegroupsregarding anthro-pometricvariableswerenotobserved.
The analysis of static body balance in different visual conditionsenabled an analysis of the impact of vision to maintain the balance in both groups studied. We could observethattherewasnosignificantdifferencein stabilo-metricvariablesbetweencontrols versustheMCIgroupin terms of OE condition, in which all elderly subjects have usedthethreesensorysystemstomaintainbalance. How-ever,inCEcondition,asignificantdifferencebetweenthese groupsinallstabilometricvariableswasobserved,andthe MCIgroupshowedincreasedbodyswaycomparedtothe con-trolgroup,indicatingthattheMCIgroupneededmorevisual informationtomaintainbalance.
StudiesusingposturographyinelderlypatientswithMCI are still limited. Shin et al.,3 Leandri et al.26 and Merlo etal.27 conductedsimilar research.The study by Leandri et al.26 drew attention to differences between MCI and
6
6 5
5 4
4 3
3 2
2 1
1 0
0
Anteroposterior (AP) cm
Mediolateral (ML) cm Mediolateral (ML) cm
Anteroposterior (AP) cm
–1
–1 –2
–2
A
B
Healthy elderly Elderly with MCI
CE OE
Healthy elderly Elderly with MCI
–3
–3 –4
–4 –5
–5 –6
–6 –6 –5 –4 –3 –2 –1 0 1 2 3 4 5 6
6
5
4
3
2
1
0
–1
–2
–3
–4
–5
–6
6
5
4
3
2
1
0
0 10 20 30
A
B
C
D
OE
Healthy elderly Elderly with MCI
OE
Healthy elderly Elderly with MCI
CE
Healthy elderly Elderly with MCI
CE
Healthy elderly Elderly with MCI 40
Time (s)
AP range (cm)
AP range (cm)
ML range (cm)
ML range (cm)
Time (s) Time (s) Time (s)
50 60 0 10 20 30 40 50 60
0 10 20 30 40 50 60
0 10 20 30 40 50 60
–1
–2
–3
–4
–5
–6
6
5
4
3 2
1
0
–1
–2
–3 –4
–5
–6
6 5
4
3
2
1
0
–1
–2
–3
–4
–5
–6 6
5
4
3 2
1
0
–1
–2
–3
–4
–5
–6
Figure3 Stabilogramfromahealthyelderlyandfromonewithmildcognitiveimpairment(MCI).Openeyes(OE)inan anteropos-terior(AP)direction.B,openeyes(OE)inamediolateral(ML)direction.C,eyesclosed(EC)inananteroposterior(AP)direction. D,eyesclosed(EC)inamediolateral(ML)direction.
Alzheimer’sdisease (AD) groups. These researchers found significant differences in AP displacement between con-trolandMCIgroups,andsubsequentlybetweenMCIandAD groups.Therewasnosignificant differenceinthevariable ‘‘MLdisplacement’’ between MCI andcontrol groups, but thisdifferenceoccurredbetweenMCIandADgroups.Thus, APdisplacementshowedasteadyincreaseamongthethree groupsassessed,showingthatearlychangesinthebalance ofelderlypeoplemayoccur,inparallelwithmotorchanges alreadyobservedinclinicaltrials.28---30
Taylor etal.31 showed thatolder women withMCI had moreriskfactorsfor falls thanhealthyelderly women,as wellasgreaterchangesinclinicaltrialsandanincreasein bodysway, especiallywithCE,whichcorroboratedstudies conducted by Franssen et al.,29 Boyle et al.32, and Liu-Ambroseetal.33 Thegreater bodysway inCEconditionin theMCIgroupcomparedwiththecontrolgroup,asobserved inthesestudies,confirmstheimportanceofvisionin main-tainingbodystability.Inourstudy,theabsenceofavisual cueresultedinhigherbodyswayintheMCIgroup, replicat-ingthefindingsfromthestudiescitedabove.Theseresults alsoindicatethatan overload mayoccurin other sensory
(vestibularandsomatosensory)systems,inordertomaintain balanceandpreventfalls.
After testing the multisensory integration ability of elderlypeoplewithMCIandAD,Wuetal.34observedthatthe reactiontimenotonlyofelderlypeoplewithAD,butalso of thosewithMCI, wasslower thaninhealthy individuals. Thisfindingsuggeststhatcognitivedeficitsfoundinelderly peoplewithMCI mayalreadyleadtoalowermultisensory integration, which reduces their functional performance comparedtohealthyelderlysubjects.
When comparing the same groups with OE and CE, subjectsbelongingtothecontrolgrouponlyshoweda signifi-cantdifferenceinmaximumAPdisplacement,whiletheMCI group showed significant differences for all stabilometric variablesassessed.
posture, studies have shown nodifferences in bodysway among healthy elderly people in the absence of vision, exceptinAPdisplacement.26,35---37
Sarabonetal.35andFujitaetal.37 showedimprovement in postural control efficiency according to age in healthy individuals,butobservednodifferencesinbodyswaywith OEandCEbetweengroupsofdifferentages.Theseresults contradict studies that highlight a high reliance onvisual informationintheelderlypopulation.38
Ontheotherhand,inolderadultswithMCIvisual infor-mation seems to play a greater role in controlling body balance, since the sensory compensation does not occur soefficiently,duetothelowersensoryintegration demon-stratedbysuchpatients.34Astheseelderlypeoplepresent withalowersomatosensory input intheir lowerlimbs,as wellasapossiblechangeinvestibularsystem,theirvisual system gets overloaded, and visual deprivation triggers a greater change of staticequilibrium.This resultwas con-firmedbyShinetal.3andLeandrietal.26instudiesinvolving elderlypeople(withMCIversushealthysubjects), demon-stratingthatvisualdeprivationwassignificantlyassociated witha greater body displacement seen in theMCI group, mainlyinAPdirection.
Another hypothesis that may explain the greater need of visual information in the MCI group is the relationship betweenthissensoryinformationandcognition.Itisknown thatthevisualafferentsareanimportantsourceof informa-tionfortheformationofposturalorientation.Thereduction ofsuchinformationwouldleadtoagreaterneedofcognitive involvementinsensorimotorprocessing.38
Attentional and executive resources play an important role in the decline of spatial memory, usually associated withthehealthyagingprocess.However,studiespointtoa greaterdecreaseofthisspatialmemoryinolderadultswith MCI.Inaddition,changesinparietalwhitematter, entorhi-nalcortex,andposteriorcingulatemayadverselyaffectthe successfuluseof attentionalresources topostural control intheseelderlypatientswithMCI.39
Therelationshipbetweencognitiveperformancethrough MMSE and total trajectory in sensory conditions (OE and CE) for all participants was established through a corre-lation analysis. One can observe a moderate correlation between MMSEand OE, anda strong correlation between MMSEandCE.ThisfindingshowsthatincreasesinMMSEscore arecoincidentwithdecreasesintotaltrajectoryvalue,i.e. those elderly participants with a better cognitive perfor-manceexhibitedlessoscillationinthestandingposture.This associationwasalsoobservedinotherstudies.26,40,41These resultsindicatethat cognitivefunctionisa criticalaspect fortheseelderlypeople,andcomparedtotraditionaltests of cognitivefunction, motor performanceevaluations can besensitive,toidentifypeopleaffectedintheearlystages ofcognitivedysfunction.
Itshouldbenotedthatthedecreasedbalanceinelderly peoplewithMCI hasaclinical significancebeyondtherisk offalls.Evidencesuggeststhatthisdeclineisrelatedtoan increasedriskofAD.28ItmaybethatpeoplewithMCImay havegreaterphysiologicalimpairmentcomparedto individ-uals notaffected by this condition, because of structural andfunctionalbrainabnormalities.42
Althoughclinicalassessmentscalesareusedforbalance assessment,someofthesetestsmaynotbeassensitiveto
detectlowlevelsofbalancedysfunctionsuchasthatfound intheearlystagesofcognitiveimpairment.29 Newer tech-nologies using magnetic transducers todetect body sway andweighttransferduringstaticordynamicpostureprovide moresensitivemeasurementstoevaluatesmallchangesin balance.9
In this regard,several studies have assessed body bal-anceusingthethree-dimensionalsystemofelectromagnetic sensors.10---17Theuseofthistoolinourstudyproveduseful indefiningtherehabilitationgoalsandobtainingimportant information about the monitoring of therapeutic results. Someofitsbiggestadvantages arethatthesystem canbe transportedtodifferent locations,hasa low implementa-tioncost,andalsoprovidessimpledataforitsanalysisand interpretation.
The clinical implication of this study is that the risk assessmentoffalls shouldbeakeycomponentinthe clin-icalmanagementofelderlypatientswithMCI.Specifically, studies suggest the inclusion of body sway measures for this population.33 It may be that changes in stabilomet-ric parameters, particularly in AP direction, may be an early sign of impaired postural control, and evaluations in an CE environment maybe useful to better differenti-ate between those small postural instabilities associated with aging and pathological processes that affect pos-turalcontrol. Earlydetection ofabnormalities in postural control, followed by an appropriate rehabilitation, envi-ronmentalchanges,andappropriaterecommendations,can help prevent falls and improve the quality of life of the elderly.
Conclusion
The assessments showed a decrease of body balance in elderlysubjectswithMCI.Inaddition,APdisplacementmay beanearlysignofposturalcontrolimpairment,anda vision-restricted evaluation maybe useful in detecting cases of smallposturalinstability.
Conflict
of
interests
Theauthorsdeclarenoconflictsofinterest.
References
1.LacourM,Bernard-DemanzeL,DumitrescuM.Posturecontrol, aging, and attention resources: models and posture-analysis methods.NeurophysiolClin.2008;38:411---21.
2.TaylorME,DelbaereK,MikolaizakAS,LordSR,CloseJC.Gait parameter risk factors for falls under simple and dual task conditionsincognitivelyimpairedolderpeople.GaitPosture. 2013;37:126---30.
3.Shin BM, HanSJ, Jung JH, KimJE, Fregni F. Effect of mild cognitive impairment on balance. J Neurol Sci. 2011;305: 121---5.
4.SuttanonP,HillKD,SaidCM,LogiudiceD,LautenschlagerNT, DoddKJ.Balanceandmobilitydysfunctionandfallsriskinolder peoplewithmildtomoderateAlzheimerdisease.AmJPhysMed Rehabil.2012;91:12---23.
incommunity-dwellingolderpeople.AmJGeriatrPsychiatry. 2012;20:845---53.
6.PetersenRC,SmithGE,WaringSC,IvnikRJ,TangalosEG, Kok-menE.Mildcognitiveimpairment:clinicalcharacterizationand outcome.ArchNeurol.1999;56:303---8.
7.Boyle PA,Buchman AS,WilsonRS, Leurgans SE,BennettDA. Physicalfrailtyisassociatedwithincidentmildcognitive impair-ment in community-based older persons.J Am Geriatr Soc. 2010;58:248---55.
8.Nagamatsu LS, Chan A, Davis JC, Beattie BL, Graf P, Voss MW, et al. Physical activity improves verbal and spatial memory inolderadultswithprobable mildcognitive impair-ment: a 6-month randomized controlled trial. J Aging Res. 2013;2013:861893.
9.Duarte M, Freitas SM. Revision of posturography based on forceplateforbalanceevaluation.BrazJPhysTher.2010;14: 183---92.
10.CarneiroJA, Santos-PontelliTE,Colafêmina JF, CarneiroAA, FerriolliE.Apilotstudyontheevaluationofpostural strate-gies in young and elderly subjects using a tridimensional electromagnetic system. Braz J Otorhinolaryngol. 2013;79: 219---25.
11.Carneiro JA, Santos-Pontelli TEG, Vilac¸a KH, Pfrimer K, ColafêminaJF,CarneiroAA,etal.Obeseelderlywomenexhibit lowposturalstability:anovelthree-dimensionalevaluation sys-tem.Clinics(USP.Impresso).2012;67:475---81.
12.VarelaDG,CarneiroJAO,ColafêminaJF.Staticposturalbalance studyinpatientswithvestibulardisordersusingathree dimen-sionalelectromagneticsensorsystem.BrazJOtorhinolaryngol. 2012;78:7---13.
13.Abreu DC, Trevisan DC, Costa GC, Vasconcelos FM, Gomes MM, Carneiro AA. The association between osteoporosis and static balance in elderly women. Osteoporos Int. 2010;21: 1487---91.
14.Carneiro JAO, Santos-Pontelli TEG, Colafêmina JF, Carneiro AAO, Ferriolli E. Analysis of static postural balance using a 3d electromagnetic system. Braz J Otorhinolaryngol. 2010;76:783---8.
15.Accornero N, Capozza M, Rinalduzzi S, Manfredi GW. Clinical multisegmental posturography: age-related changes in stance control. Electroencephalogr Clin Neurophysiol. 1997;105:213---9.
16.BohannonRW,HarrisonS,Kinsella-ShawJ.Reliabilityand valid-ityofpendulumtestmeasuresofspasticityobtainedwiththe Polhemustrackingsystemfrompatientswithchronicstroke.J NeuroengRehabil.2009;6:30.
17.Melo PS, Ferreira TP, Santos-Pontelli TEG, Carneiro JAO, CarneiroAAO,ColafêminaJF.Comparac¸ãodaoscilac¸ãopostural estáticanaposic¸ãosentadaentrejovenseidosossaudáveis.Rev BrasFisioter.2009;13:549---54.
18.GillJ,AllumJH,CarpenterMG,Held-ZiolkowskaM,AdkinAL, Honegger F,et al.Trunk sway measuresof posturalstability duringclinicalbalancetests:effectsofage.JGerontolA:Biol SciMedSci.2001;56:M438---47.
19.PetersenRC,DoodyR,KurzA,MohsRC,MorrisJC,RabinsPV, etal.Currentconceptsinmildcognitiveimpairment.Arch Neu-rol.2001;58:1985---92.
20.ValeFAC,Balieiro-JúniorAP,Silva-FilhoJH.Manualde Proced-imentos de Rotina --- Revisado (MPR-Rev) do Ambulatório de Neurologia Comportamentaldo HospitaldasClínicas da Fac-uldadedeMedicinadeRibeirãoPretodaUniversidadedeSão Paulo. Ribeirão Preto:Ambulatório de Neurologia Comporta-mentaldoHospitaldasClínicasdaFaculdadedeMedicinade RibeirãoPreto(ANCC-HCFMRP);2006.
21.LambSE,Jorstad-SteinEC,HauerK, BeckerC,Preventionof FallsNetworkEuropeandOutcomesConsensusGroup. Develop-mentofacommonoutcomedatasetforfallinjuryprevention
trials:thepreventionoffallsnetworkEuropeconsensus.JAm GeriatrSoc.2005;53:1618---22.
22.DennisRJ.UsingtheFreiburgAcuityandContrastTestto mea-surevisualperformanceinUSAFpersonnelafterPRK.OptomVis Sci.2004;81:516---24.
23.SargentEW,BankaitisAE,HollenbeakCS,CurrensJW.Mastoid oscillationincanalithrepositioningfor paroxysmal positional vertigo.OtolNeurotol.2001;22:205---9.
24.NakanoMM[Dissertac¸ãodeMestrado]VersãoBrasileiradaShort Physical Performance Battery --- SPPB: adaptac¸ão cultural e estudodeconfiabilidade.Campinas:UniversidadeEstadualde Campinas;2007.
25.GuerrazM,Shallo-HoffmanJ,YarrowK,ThiloKV,BrosteinAM, Gresty MA. Visual control of postural orientation and equi-librium in congenital nystagmus. Invest Ophthalmol Vis Sci. 2000;41:3798---804.
26.Leandri M,Cammisuli S, Cammarata S, BarattoL, Campbell J, Simonini M, et al. Balance features in Alzheimer’s dis-easeandamnesticmildcognitiveimpairment.AlzheimersDis. 2009;16:113---20.
27.Merlo A, Zemp D, Zanda E, Rocchi S, Meroni F, Tettamanti M,et al.Postural stability and history offallsin cognitively able older adults: the Canton Ticino study. Gait Posture. 2012;36:662---6.
28.AggarwalNT,WilsonRS,BeckTL,BieniasJL,BennettDA.Motor dysfunctioninmildcognitiveimpairmentandtheriskof inci-dentAlzheimerdisease.ArchNeurol.2006;63:1763---9. 29.Franssen EH, Souren LE, Torossian CL, Reisberg B.
Equilib-rium and limb coordination in mild cognitive impairment and mild Alzheimer’s disease. J Am Geriatr Soc. 1999;47: 463---9.
30.Kluger A, Gianutsos JG, Golomb J, Ferris SH, George AE, FranssenE,etal.Patternsofmotorimpairmentinnormalaging, mildcognitivedecline,andearlyAlzheimer’sdisease.J Geron-tolB:PsycholSciSocSci.1997;52:28---39.
31.TaylorME,LordSR,DelbaereK,MikolaizakAS,CloseJC. Physi-ologicalfallriskfactorsincognitivelyimpaired olderpeople: a one-year prospective study. Dement Geriatr Cogn Disord. 2012;34:181---9.
32.BoylePA,WilsonRS,BuchmanAS,AggarwalNT,TangY, Arvani-takisZ,etal.Lowerextremitymotorfunctionanddisabilityin mildcognitiveimpairment.ExpAgingRes.2007;33:355---71. 33.Liu-AmbroseT,AsheMC,GrafP,BeattieBL,KhanKM.Mild
cogni-tiveimpairmentincreasesfallsriskinoldercommunity-dwelling women.PhysTher.2008;88:1482---91.
34.WuJ,YangJ,YuY,LiQ,NakamuraN,ShenY,etal.Delayed audiovisualintegrationofpatientswithmildcognitive impair-ment and Alzheimer’s disease compared with normal aged controls.JAlzheimersDis.2012;32:317---28.
35.SarabonN,Panjan A, LatashM.The effects ofaging onthe ramblingandtremblingcomponentsofposturalsway:effectsof motorandsensorychallenges.GaitPosture.2013;38:637---42. 36.PrioliAC,CardozoAS,FreitasJúniorPB,BarelaJA.Taskdemand
effects on postural control in older adults. Hum Mov Sci. 2006;25:435---46.
37.FujitaT,NakamuraS,OhueM, FujiiY,Miyauchi A, Takagi Y, etal. Effect ofageonbodysway assessedbycomputerized posturography.JBoneMinerMetab.2005;23:152---6.
38.Jamet M, Deviterne D, Gauchard GC, Vanc¸on G, Perrin PP. Age-relatedpart taken byattentional cognitiveprocesses in standingposturalcontrolinadual-taskcontext.GaitPosture. 2007;25:179---84.
40.AyanC,CancelaJM,GutiérrezA,PrietoI.Influenceofthe cog-nitiveimpairmentlevelontheperformanceoftheTimedUp& GoTest(TUG)inelderlyinstitutionalizedpeople.ArchGerontol Geriatr.2013;56:44---9.
41.Bruce-Keller AJ, Brouillette RM, Tudor-Locke C, Foil HC, GahanWP,CorreaJ,etal.Assessmentofcognition,physical
performance,andgaitinthecontextofmildcognitive impair-mentanddementia.JAmGeriatrSoc.2012;60:176---7. 42.KidoT,TabaraY,IgaseM,OchiN,UetaniE,NagaiT,etal.