w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Swimming
and
cycling
do
not
cause
positive
effects
on
bone
mineral
density:
a
systematic
review
Odilon
Abrahin
a,b,∗,
Rejane
Pequeno
Rodrigues
a,b,
Anderson
Carlos
Marc¸al
a,
Erik
Artur
Cortinhas
Alves
b,
Rosa
Costa
Figueiredo
b,
Evitom
Corrêa
de
Sousa
baPostgraduatePrograminPhysicalEducation,UniversidadeFederaldeSergipe,SãoCristóvão,SE,Brazil bResistiveExerciseandHealthLaboratory(Leres),UniversidadedoEstadodoPará,Belém,PA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1December2014 Accepted17September2015 Availableonline11March2016
Keywords:
Osteoporosis Osteopenia Bonedensity Exercise Physicalactivity
a
b
s
t
r
a
c
t
Osteoporosisisconsideredacommonmetabolicbonediseaseanditsprevalenceis increas-ingworldwide.Inthiscontext,physicalactivityhasbeenusedasanon-pharmacologicaltool forpreventionandauxiliarytreatmentofthisdisease.Theaimofthissystematicreviewwas toevaluatetheeffectsofcyclingandswimmingpracticeonbonemineraldensity(BMD).This researchwasconductedinaccordancewiththerecommendationsoutlinedbythePreferred ReportingItemsforSystematicReviewsandMeta-Analyses.Thestudieswereconsultedin theperiodfrom2004to2014,throughmajorelectronicdatabases:PubMed®,SciELO®and
LILACS®.TenstudiesevaluatedtheeffectsofcyclingonBMD,andtheresultsshowedthat
ninestudieshavelinkedthepracticeofprofessionalcyclingwithlowlevelsofBMD.Another 18studieshavereportedthatswimminghasnopositiveeffectsonbonemass.Weconclude thatcyclingandswimmingdonotcausepositiveeffectsonBMD;thus,thesearenotthe mostsuitableexercisesforpreventionandtreatmentofosteoporosis.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Natac¸ão
e
ciclismo
não
causam
efeitos
positivos
na
densidade
mineral
óssea:
uma
revisão
sistemática
Palavras-chave:
Osteoporose Osteopenia Densidadeóssea Exercíciofísico Atividadefísica
r
e
s
u
m
o
Aosteoporoseéconsideradaumadoenc¸aosteometabólicacomumesuaprevalênciaestá aumentandomundialmente.Nessecontexto,aatividadefísicatemsidousadacomo ferra-mentanãofarmacológicaparaprevenireauxiliarnotratamentodessadoenc¸a.Oobjetivo destarevisãosistemáticafoiavaliarosefeitosdapráticadociclismoedanatac¸ãona den-sidademineralóssea(DMO).Estapesquisafoifeitadeacordocomasrecomendac¸õesdo Preferred ReportingItemsforSystematicReviewsandMeta-Analyses.Osestudosforam consultados entre 2004 e 2014, por meio de importantes bases de dados eletrônicas: PubMed®,SciELO®eLilacs®.DezpesquisasavaliaramosefeitosdociclismosobreaDMO,os
∗ Correspondingauthor.
E-mail:[email protected](O.Abrahin).
http://dx.doi.org/10.1016/j.rbre.2016.02.013
resultadosdemonstraramquenoveestudosassociaramapráticadociclismoprofissional combaixosníveisdeDMO.Outros18estudosrelataramqueanatac¸ãonãotemefeitos posi-tivossobreamassaóssea.Conclui-sequeociclismoeanatac¸ãonãocausamefeitospositivos naDMO.Assim,nãosãoosexercíciosmaisindicadosparaaprevenc¸ãoeotratamentoda osteoporose.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoporosisisadiseasecharacterizedbyadecreaseinbone mineraldensity(BMD) andbyamicroarchitectural deterio-rationofbonetissue,leadingtoenhancedbonefragilityand increasedriskoffractures.1Atpresent,osteoporosisis
con-sideredthemostcommonmetabolicbonedisease,affecting
mainlyolderpeople,andwithahigherincidenceinwomen, especiallyaftermenopause.2
AccordingtotheInternationalOsteoporosisFoundation,3
about200 millionwomenworldwideare affectedby
osteo-porosis.IntheEuropeanCommunity,fromthose25million
people affected by this disease, about 80% are female.4 In
Brazil,astudywitharepresentativesamplefounda preva-lenceoffracturesin15.1%and12.8%inwomenandmenover 40years,respectively.5
Themainriskfactorsfordevelopingosteoporosisinclude: genetic predisposition,6 advanced age in association with
morphologicalchanges2(e.g.,adecreaseinboneandmuscle
mass),asedentarylifestyleespeciallyinchildhoodand ado-lescence(takingintoaccountthattheseareimportantstages toobtainapeakbonemass),7andnutritionaldeficits.8Inthis
regard,itisnotedthatalargeportionofrisksfactorsare modi-fiable(behavioral).Thus,healthyhabitsandadequatelevelsof physicalactivitycontributetothepreventionofthisdisease.
Amongthenon-pharmacologicalapproachesfor
preven-tionandtreatmentofosteoporosis,physicalactivityhasbeen
recommended.However,the benefitspromoted byphysical
activityonBMDaredueinparttotheintensityandtypeof exercise,9aswellastothecontrolofthebiologicalprinciples
oftraining.7
Previousstudieshaveshownthatdifferenttypesof phys-icalactivity10 (swimming, cycling)as well as its intensity9
(enduranceandsprint)canevenaffectnegativelyBMD.Thus, theaimofthisstudywastoevaluatetheeffectsofcyclingand swimmingpracticeonbonemineraldensity,duetothehigh numberofpractitioners11ofthesemodalities,theirpopularity
andalsoconsideringtheirindicationbyhealthprofessionals.
Methods
Thissystematicreviewwasconductedinaccordancewiththe recommendationsandcriteriasetbythePreferredReporting ItemsforSystematicReviewsandMeta-Analyses(PRISMA).12
Thestudies wereaccessedfrom2004to2014,througha
survey in electronic databases: PubMed® (http://www.ncbi.
nlm.nih.gov/pubmed), SciELO® (http://www.scielo .org) and
LILACS®(http://www.bireme.br).
Electronicsearchindatabases
Thefollowingtermswereadoptedinacombinedand/or indi-vidualwaytosearchforarticles:osteoporosis,bonedensity, bonemineraldensity,cyclingandswimming.InSciELO®and
LILACS®databasesthetermsmentionedabovewereentered
inPortuguese.
Studyselectionanddataextraction
Theevaluationofthestudieswasperformedbytworeviewers, andwhennecessary,athirdreviewerresolveddisagreements.
Inclusioncriteria:
1) Typesofstudy:descriptive,cross-sectional, longitudinal, randomizedcontrolledandnon-randomizedcontrolled tri-alsevaluatingtheeffectsofcyclingandswimmingonBMD. 2) Typesofparticipants:adolescents,adultsandolder
sub-jects.Therewasnorestrictionastogender.
3) Types of results evaluated: whole body BMD with
sub-regions (upper limbs or arms and lower limbs or legs),
lumbar spine, and hip with sub-regions (femoral neck,
trochanter,intertrochantericregion,andWard’striangle).
Exclusioncriteria:
1) Studies in other languages than English, Portuguese or
Spanish.
2) Studieswithanimalmodels.
Results
Initially 281relevantarticles wereidentified. Afterthe title
and abstract review, and with eventual duplicates already
discarded,thetotalwasreducedto49potentiallyrelevant doc-uments. Ofthesearticles, 29metthe selectioncriteria and wereincludedinthisstudy(Fig.1).
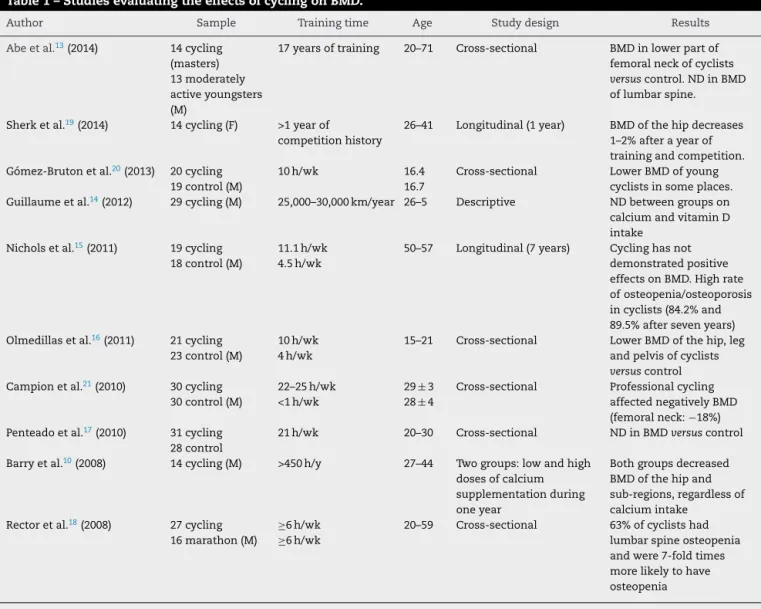
Tenstudies10,13–21evaluatingtheeffectsofcyclingonBMD
(Table 1) were found. The results showed that nine stud-ieshaveassociatedthepracticeofprofessionalcyclingwith
low levels ofBMD. Furthermore,mostof the studies
com-paredBMDofcyclistsandcontrolgroups,suggestingthatthis sportcanbeconsideredariskfactorforearlydevelopmentof osteopenia/osteoporosis.
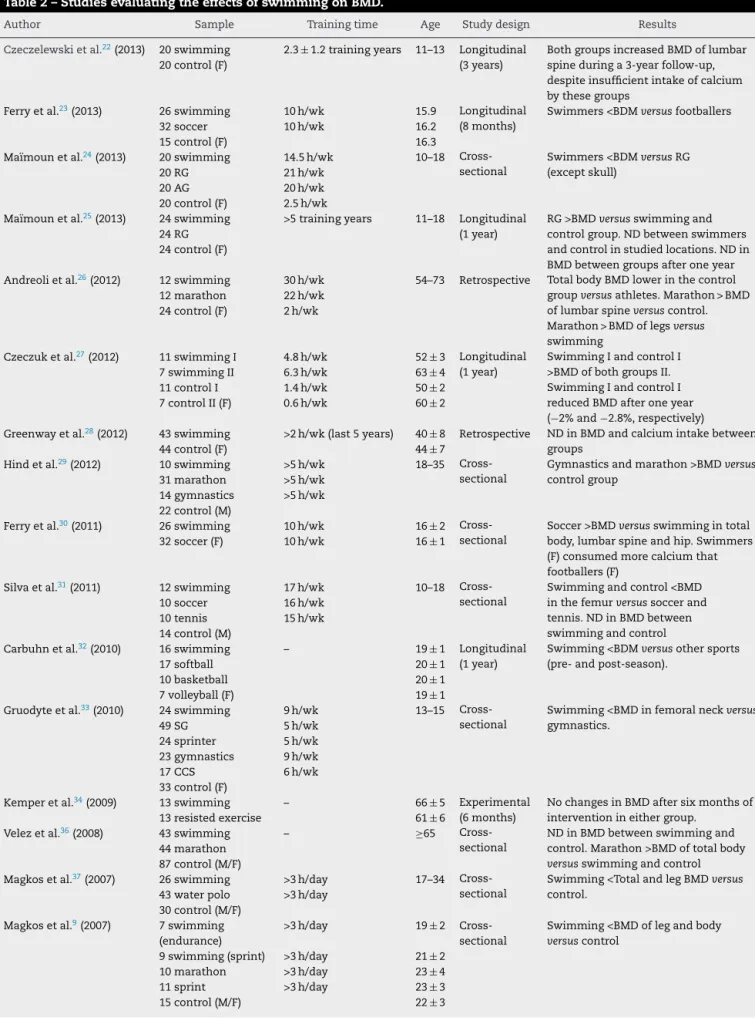
Nineteenstudies9,22–39evaluatedtheeffectsofswimming
onBMD(Table2).Theresultsshowedthatswimminghasno positiveeffectsonbonemass.Somecross-sectionalstudies
Table1–StudiesevaluatingtheeffectsofcyclingonBMD.
Author Sample Trainingtime Age Studydesign Results
Abeetal.13(2014) 14cycling (masters) 13moderately activeyoungsters (M)
17yearsoftraining 20–71 Cross-sectional BMDinlowerpartof femoralneckofcyclists
versuscontrol.NDinBMD oflumbarspine.
Sherketal.19(2014) 14cycling(F) >1yearof
competitionhistory
26–41 Longitudinal(1year) BMDofthehipdecreases 1–2%afterayearof trainingandcompetition. Gómez-Brutonetal.20(2013) 20cycling
19control(M)
10h/wk 16.4
16.7
Cross-sectional LowerBMDofyoung cyclistsinsomeplaces. Guillaumeetal.14(2012) 29cycling(M) 25,000–30,000km/year 26–5 Descriptive NDbetweengroupson calciumandvitaminD intake
Nicholsetal.15(2011) 19cycling 18control(M)
11.1h/wk 4.5h/wk
50–57 Longitudinal(7years) Cyclinghasnot demonstratedpositive effectsonBMD.Highrate ofosteopenia/osteoporosis incyclists(84.2%and 89.5%aftersevenyears) Olmedillasetal.16(2011) 21cycling
23control(M)
10h/wk 4h/wk
15–21 Cross-sectional LowerBMDofthehip,leg andpelvisofcyclists
versuscontrol Campionetal.21(2010) 30cycling
30control(M)
22–25h/wk <1h/wk
29±3 28±4
Cross-sectional Professionalcycling affectednegativelyBMD (femoralneck:−18%) Penteadoetal.17(2010) 31cycling
28control
21h/wk 20–30 Cross-sectional NDinBMDversuscontrol
Barryetal.10(2008) 14cycling(M) >450h/y 27–44 Twogroups:lowandhigh dosesofcalcium supplementationduring oneyear
Bothgroupsdecreased BMDofthehipand sub-regions,regardlessof calciumintake
Rectoretal.18(2008) 27cycling 16marathon(M)
≥6h/wk
≥6h/wk
20–59 Cross-sectional 63%ofcyclistshad lumbarspineosteopenia andwere7-foldtimes morelikelytohave osteopenia
BMD,bonemineraldensity;F,female;h/wk,hoursperweek;h/y,hoursperyear;M,male;ND,nodifference.
281 articles found in databases
49 potentially relevant articles
20 studies excluded
29 studies selected - 179 PubMed
- 1 SciELO - 101 LILACS
Fig.1–Flowchartforidentificationofstudiesincluded.
groups,andtheirfindingsshowednosignificantdifferences
betweengroups.
Discussion
Cycling
Cycling is widely practiced as a non-weight-bearing,
low-impactexercise;inadditionthebicycleisusedasavehicle formillions ofpeopleinseveral countries, representingan importantpartofdailyphysicalactivity.40 However,
profes-sionalcycling,orevencyclingcarriedoutwithahightraining volume,isassociatedwithlowlevelsofBMD,increasingthe likelihoodofdevelopingosteoporosisandosteopenia.10,13–21
Astudy10examinedBMDofamateurcyclists(regional-level
competitors) divided into two groups: those supplemented
dailywith 1500mgor 250mgofcalcium duringthe period
ofninemonthsofcompetition,andthreemonthsafterthe
Table2–StudiesevaluatingtheeffectsofswimmingonBMD.
Author Sample Trainingtime Age Studydesign Results
Czeczelewskietal.22(2013) 20swimming 20control(F)
2.3±1.2trainingyears 11–13 Longitudinal (3years)
BothgroupsincreasedBMDoflumbar spineduringa3-yearfollow-up, despiteinsufficientintakeofcalcium bythesegroups
Ferryetal.23(2013) 26swimming 10h/wk 15.9 Longitudinal (8months)
Swimmers<BDMversusfootballers
32soccer 10h/wk 16.2
15control(F) 16.3
Maïmounetal.24(2013) 20swimming 14.5h/wk 10–18 Cross-sectional
Swimmers<BDMversusRG (exceptskull)
20RG 21h/wk
20AG 20h/wk
20control(F) 2.5h/wk Maïmounetal.25(2013) 24swimming
24RG 24control(F)
>5trainingyears 11–18 Longitudinal (1year)
RG>BMDversusswimmingand controlgroup.NDbetweenswimmers andcontrolinstudiedlocations.NDin BMDbetweengroupsafteroneyear Andreolietal.26(2012) 12swimming 30h/wk 54–73 Retrospective TotalbodyBMDlowerinthecontrol
groupversusathletes.Marathon>BMD oflumbarspineversuscontrol. Marathon>BMDoflegsversus
swimming 12marathon 22h/wk
24control(F) 2h/wk
Czeczuketal.27(2012) 11swimmingI 4.8h/wk 52±3 Longitudinal (1year)
SwimmingIandcontrolI >BMDofbothgroupsII. SwimmingIandcontrolI reducedBMDafteroneyear (−2%and−2.8%,respectively) 7swimmingII 6.3h/wk 63±4
11controlI 1.4h/wk 50±2 7controlII(F) 0.6h/wk 60±2
Greenwayetal.28(2012) 43swimming >2h/wk(last5years) 40±8 Retrospective NDinBMDandcalciumintakebetween groups
44control(F) 44±7
Hindetal.29(2012) 10swimming >5h/wk 18–35 Cross-sectional
Gymnasticsandmarathon>BMDversus
controlgroup 31marathon >5h/wk
14gymnastics >5h/wk 22control(M)
Ferryetal.30(2011) 26swimming 10h/wk 16±2 Cross-sectional
Soccer>BMDversusswimmingintotal body,lumbarspineandhip.Swimmers (F)consumedmorecalciumthat footballers(F)
32soccer(F) 10h/wk 16±1
Silvaetal.31(2011) 12swimming 17h/wk 10–18 Cross-sectional
Swimmingandcontrol<BMD inthefemurversussoccerand tennis.NDinBMDbetween swimmingandcontrol 10soccer 16h/wk
10tennis 15h/wk 14control(M)
Carbuhnetal.32(2010) 16swimming – 19±1 Longitudinal (1year)
Swimming<BDMversusothersports (pre-andpost-season).
17softball 20±1
10basketball 20±1
7volleyball(F) 19±1
Gruodyteetal.33(2010) 24swimming 9h/wk 13–15 Cross-sectional
Swimming<BMDinfemoralneckversus
gymnastics.
49SG 5h/wk
24sprinter 5h/wk 23gymnastics 9h/wk
17CCS 6h/wk
33control(F)
Kemperetal.34(2009) 13swimming – 66±5 Experimental (6months)
NochangesinBMDaftersixmonthsof interventionineithergroup.
13resistedexercise 61±6 Velezetal.36(2008) 43swimming – ≥65
Cross-sectional
NDinBMDbetweenswimmingand control.Marathon>BMDoftotalbody
versusswimmingandcontrol 44marathon
87control(M/F)
Magkosetal.37(2007) 26swimming >3h/day 17–34 Cross-sectional
Swimming<TotalandlegBMDversus
control. 43waterpolo >3h/day
30control(M/F) Magkosetal.9(2007) 7swimming
(endurance)
>3h/day 19±2 Cross-sectional
Swimming<BMDoflegandbody
versuscontrol 9swimming(sprint) >3h/day 21±2
10marathon >3h/day 23±4 11sprint >3h/day 23±3
Table2–(Continued)
Author Sample Trainingtime Age Studydesign Results
Muddetal.38(2007) 9swimming – 20±1 Cross-sectional
Swimming<BMDoflegversusother sports(exceptmarathonandrowing). 8gymnastics
14softball 25marathon 8sprinter 10hockey 10soccer 15rowing(F)
Maïmounetal.39(2004) 13swimming 10h/wk 18–39 Cross-sectional
NDinBMDbetweengroups.Cyclists consumedmorecalciumversuscontrol group.
11cycling 10h/wk 14triathlon 15h/wk 10control(M)
CCS,cross-countryskiing;BMD,bonemineraldensity;SG,sportgame(basketball,volleyball,badminton);F,female;AG,artisticgymnastics;RG, rhythmicgymnastics;h/wk,hoursperweek;M,male;NDnodifference;Sprinter,shortdistancerunners>800m.
Olmedillas et al.16 evaluated the BMD of professional
cyclists aged >17 versus <17 years. These groups had a mean training time of 2.7and 4.4 years,respectively. The
results revealed that both cyclist groups had lower BMD
when compared to control groups. The authors suggested
thatprofessionalcyclingperformedduringadolescencemay
negatively affect BMD; this is due in part to a reduced
acquisitionofpeakbonemassatthisstage,sincethisisa non-weight-bearing, low-impactactivity.Sherk et al.19 followed
professionalfemalecyclistsduringoneyear;themainfinding inthisstudywasalossof1–2%ofBMDofthehipafteroneyear oftrainingandcompetition.Anotherstudyindicatedthatthis professionalsportsmodalityincreasesseven-foldthechances ofearlydevelopmentofosteopenia.18
Another study followed master male cyclists for seven
years;theresultsshowedthatthissportwasassociatedwith adecreaseinBMD,accompaniedbyanincreaseintheriskof fracturesresultingfrompotentialfalls.15Accordingtothese
authors,coachesandhealthprofessionalswhointeractwith professional cyclists need topromote alternative exercises likeplyometrics, resistancetraining orother higher-impact activity asa complementto this modality,thus helping to minimizebonelossinthisgroup.
Thedata referredto these studies suggest that cycling, particularly the professional modality, is associated with decreasesinBMDevenwhenthepractitionersingestadequate
amounts of calcium.10,17 Among the possible causes, one
canmention thatthis isanon-weight-bearing, low-impact
exercise,beingusuallyconductedinanenvironmentof high-volumeoftraining.Thisfactorisassociatedwithanexcessive lossofcalciumthroughtheskinduringexerciseandwithan increasedproductionofsubstancesknowntostimulatebone resorption,suchascortisolandpro-inflammatorycytokines (e.g.,interleukin-6).10Overtrainingcanalsoleadtolow
produc-tionofhormoneswithosteoblasticactivity,suchasestrogen andtestosterone.41
Thus, professional cycling is not associated with an
increase/maintenanceofBMD.Inthiscase,thisactivityshould notbeperformedbyosteopenic/osteoporoticindividuals aim-ingatpreserving/increasingBMD, sincethis sportdoes not
haveapositiveeffectonBMD.Additionally,coachesand exer-cisephysiologistsshouldindicate complementaryactivities thathelpinthecontrol/maintenanceofbonemassin profes-sionalcyclists.
Swimming
Swimmingisanon-impactphysicalactivity,and isusually
recommended inthe rehabilitationprocess and forspecial
populations,mainlytheelderly.Forthisreason,many stud-ieshaveexaminedtheeffectsofswimmingasanadjuvantin thepreventionandtreatmentofosteoporosis;however,these trialsshowednoevidenceofpositiveeffectsofswimmingon bonemass.9,23–34,36–38
Kemperetal.34 evaluatedtheeffectsofswimming
prac-ticed three times a week for six months with intensities
between60and90%ofheartratereserveinpostmenopausal olderwomen;theirresultsshowedthattherewerenochanges inBMDinthefemoralneckandlumbarspineafterthis train-ingperiod.
Muddetal.38comparedBMDofwomenathletesinvarious
sportmodalities.Accordingtotheseauthors,theswimmers hadthelowestmeanvaluesofBMDinlowerlimbswhen com-paredtoathletes ofother sports,forinstance, gymnastics, hockey,footballandshort-distancerunners.
Aninterestingstudy9 foundlower BMDvaluesin
swim-mers’ lower limbs versus sedentary individuals (−9.8%).
However, when these authors divided the swimmers in
enduranceandsprintathletes,theendurancegroupshowed
BDMvaluesevensmallerinlowerlimbscomparedtothe con-trol(−14.8%).
AstudypublishedbyBrazilianinvestigatorsmeasuredBMD ofseveraladolescentmaleathletes(swimmers,tennisplayers andfootballers)andofthecontrolgroup.Themainfindings
ofthisstudydemonstratedthatswimmersandcontrolshad
lowerBMDofthefemurinrelationtoothersports.31According
Otherlongitudinalstudies23,25,27,32showedthatevenwhen
swimmingwascarried out forlong periods(one year),this
method did not provide a positive effect on bone mass.
Interestingly,comparativeBMDbetweencontrolgroupversus
swimmersshowednosignificantintergroupdifference.
Basedonthesefindings,professionalswimming,oreven
that practiced inascenario ofhigh-volume training,is an activitythatdoesnotpromoteincreaseinBMD,takinginto accountthatthatthisisanon-impactphysicalactivity.These resultssuggestthathealthprofessionalsshouldnotindicate swimmingasanon-pharmacologicaltooltopreventortreat osteoporosis.
Limitations
Inourstudyweevaluatedtheeffectsofcyclingandswimming
practice on BMD; however, some benefits of these
activi-ties,suchasimprovedaerobicfitness,mitochondrialdensity, andbalance,amongothers,cannotberuledout.Most stud-ies analyzed in this systematicreview had cross-sectional design(specificallyinathletes).Itisalsosuggestedthatnew randomized,controlled,longitudinalexperimentalstudiesbe conductedtoevaluatetheeffectsofswimmingandcyclingon BMD,toimproveourunderstandingontheseresults.
Conclusion
Theresultsofthisstudyindicatethatcyclingandswimming donotcausepositiveeffectsonBMDand,therefore,arenot themostsuitableexercisesforthepreventionandtreatment ofosteoporosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. Osteoporosisprevention,diagnosis,andtherapy.NIH ConsensStatement.2000;17(1):1–45.
2. FinkelsteinJS,BrockwellSE,MehtaV,GreendaleGA,Sowers MR,EttingerB,etal.Bonemineraldensitychangesduringthe menopausetransitioninamultiethniccohortofwomen.J ClinEndocrinolMetab.2008;93(3):861–8.
3. InternationalOsteoporosisFoundation.Factsandstatistics aboutosteoporosisanditsimpact.IntOsteoporosFound. 2009.
4. USDepartmentofHealthandHumanServices.Bonehealth andosteoporosis:areportoftheSurgeonGeneral.USHealth andHumanServices;2004.p.437.
5. PinheiroMM,CiconelliRM,MartiniLA,FerrazMB.Clinical riskfactorsforosteoporoticfracturesinBrazilianwomenand men:theBrazilianOsteoporosisStudy(BRAZOS).Osteoporos Int.2009;20(3):399–408.
6. FroesNDTC,PereiraES,NegrelliWF.Fatoresderiscoda osteoporose:prevenc¸ãoedetecc¸ãoatravésdomonitoramento clínicoegenético.ActaOrtopBras.2002;10(1):52–7.
7. Guadalupe-GrauA,FuentesT,GuerraB,CalbetJAL.Exercise andbonemassinadults.SportsMed.2009;39(6):439–68.
8.Bischoff-FerrariHA,ReesJR,GrauMV,BarryE,GuiJ,BaronJA. Effectofcalciumsupplementationonfracturerisk:a double-blindrandomizedcontrolledtrial.AmJClinNutr. 2008;87(6):1945–51.
9.MagkosF,YannakouliaM,KavourasSA,SidossisLS.Thetype andintensityofexercisehaveindependentandadditive effectsonbonemineraldensity.IntJSportsMed. 2007;28(9):773–9.
10.BarryDW,KohrtWM.BMDdecreasesoverthecourseofayear incompetitivemalecyclists.JBoneMinerRes.
2008;23(4):484–91.
11.MelloMT,FernandezAC,TufikS.Levantamento
epidemiológicodapráticadeatividadefísicanacidadedeSão Paulo.RevBrasMedEsporte.2000;6(4):119–24.
12.LiberatiA,AltmanDG,TetzlaffJ,MulrowC,GøtzschePC, IoannidisJPA,etal.ThePRISMAstatementforreporting systematicreviewsandmeta-analysesofstudiesthat evaluatehealthcareinterventions:explanationand elaboration.BMJ.2009;339:b2700.
13.AbeT,NaharVK,YoungKC,PattersonKM,StoverCD,Lajza DG,etal.Skeletalmusclemass,bonemineraldensity,and walkingperformanceinmasterscyclists.RejuvenatRes. 2014;17(3):291–6.
14.GuillaumeG,ChappardD,AudranM.Evaluationofthebone statusinhigh-levelcyclists.JClinDensitom.2012;15(1): 103–7.
15.NicholsJF,RauhMJ.Longitudinalchangesinbonemineral densityinmalemastercyclistsandnonathletes.JStrength CondRes.2011;25(3):727–34.
16.OlmedillasH,González-AgüeroA,MorenoLA,CasajúsJA, Vicente-RodríguezG.Bonerelatedhealthstatusinadolescent cyclists.PLoSONE.2011;6(9):e24841.
17.PenteadoVS,CastroCH,PinheiroMM,SantanaM,BertolinoS, MelloMT,etal.Diet,bodycomposition,andbonemassin well-trainedcyclists.JClinDensitom.2010;13(1):43–50.
18.RectorRS,RogersR,RuebelM,HintonPS.Participationin roadcyclingvsrunningisassociatedwithlowerbonemineral densityinmen.Metabolism.2008;57(2):226–32.
19.SherkVD,BarryDW,VillalonKL,HansenKC,WolfeP,Kohrt WM.Bonelossover1yearoftrainingandcompetitionin femalecyclists.ClinJSportMed.2014;24(4):331–6.
20.Gómez-BrutonA,González-AgüeroA,OlmedillasH, Gómez-CabelloA,Matute-LlorenteA,Julián-AlmárceguiC, etal.DocalciumandvitaminDintakeinfluencetheeffectof cyclingonbonemassthroughadolescence?NutrHosp. 2013;28(3):1136–9.
21.CampionF,NevillAM,KarlssonMK,LounanaJ,ShabaniM, FardelloneP,etal.Bonestatusinprofessionalcyclists.IntJ SportsMed.2010;31(7):511–5.
22.CzeczelewskiJ,Długoł ˛eckaB,CzeczelewskaE,Raczy ´nskaB. Intakesofselectednutrients,bonemineralisationand densityofadolescentfemaleswimmersoverathree-year period.BiolSport.2013;30(1):17–20.
23.FerryB,LespessaillesE,RochcongarP,DuclosM,CourteixD. Bonehealthduringlateadolescence:effectsofan8-month trainingprogramonbonegeometryinfemaleathletes.Joint BoneSpine.2013;80(1):57–63.
24.MaïmounL,CosteO,PhilibertP,BriotK,MuraT,GaltierF, etal.Peripubertalfemaleathletesinhigh-impactsportsshow improvedbonemassacquisitionandbonegeometry. Metabolism.2013;62(8):1088–98.
25.MaïmounL,CosteO,MuraT,PhilibertP,GaltierF,
Mariano-GoulartD,etal.Specificbonemassacquisitionin elitefemaleathletes.JClinEndocrinolMetab.
2013;98(7):2844–53.
26.AndreoliA,CeliM,VolpeSL,SorgeR,TarantinoU.Long-term effectofexerciseonbonemineraldensityandbody
27.CzeczukA,Huk-WieliczukE,MichalskaA,BylinaD,SołtanJ, ZofiaD.Theeffectofmenopauseonbonetissueinformer swimmersandinnon-athletes.AdvClinExpMed. 2012;21(5):645–52.
28.GreenwayKG,WalkleyJW,RichPA.Doeslong-term
swimmingparticipationhaveadeleteriouseffectontheadult femaleskeleton?EurJApplPhysiol.2012;112(9):3217–25.
29.HindK,GannonL,WhatleyE,CookeC,TruscottJ.Bone cross-sectionalgeometryinmalerunners,gymnasts, swimmersandnon-athleticcontrols:ahip-structural analysisstudy.EurJApplPhysiol.2012;112(2):535–41.
30.FerryB,DuclosM,BurtL,TherreP,LeGallF,JaffréC,etal. Bonegeometryandstrengthadaptationstophysical constraintsinherentindifferentsports:comparisonbetween elitefemalesoccerplayersandswimmers.JBoneMiner Metab.2011;29(3):342–51.
31.SilvaCC,GoldbergTBL,TeixeiraAS,DalmasJC.Theimpactof differenttypesofphysicalactivityontotalandregionalbone mineraldensityinyoungBrazilianathletes.JSportsSci. 2011;29(3):227–34.
32.CarbuhnAF,FernandezTE,BraggAF,GreenJS,CrouseSF. Sportandtraininginfluenceboneandbodycompositionin womencollegiateathletes.JStrengthCondRes.
2010;24(7):1710–7.
33.Gruodyt ˙eR,JürimäeJ,CicchellaA,StefanelliC,PassarielloC, JürimäeT.Adipocytokinesandbonemineraldensityin adolescentfemaleathletes.ActaPædiatrica.
2010;99(12):1879–84.
34.KemperC,OliveiraRJ,BottaroM,MorenoR,BezerraLMA, GuidoM,etal.Effectsofswimmingandresistancetraining onbonemineraldensityofolderwomen.RevBrasMed Esporte.2009;15(1):10–3.
35.DermanO,CinemreA,KanburN,Do ˘ganM,Kilic¸M, KaradumanE.Effectofswimmingonbonemetabolismin adolescents.TurkJPediatr.2008;50(2):149–54.
36.VelezNF,ZhangA,StoneB,PereraS,MillerM,GreenspanSL. Theeffectofmoderateimpactexerciseonskeletalintegrity inmasterathletes.OsteoporosInt.2008;19(10):1457–64.
37.MagkosF,KavourasSA,YannakouliaM,KaripidouM,Sidossi S,SidossisLS.Theboneresponsetonon-weight-bearing exerciseissport-,site-,andsex-specific.ClinJSportMed. 2007;17(2):123–8.
38.MuddLM,FornettiW,PivarnikJM.Bonemineraldensityin collegiatefemaleathletes:comparisonsamongsports.JAthl Train.2007;42(3):403–8.
39.MaïmounL,Mariano-GoulartD,CouretI,ManettaJ,Peruchon E,MicallefJP,etal.Effectsofphysicalactivitiesthatinduce moderateexternalloadingonbonemetabolisminmale athletes.JSportsSci.2004;22(9):875–83.
40.OlmedillasH,González-AgüeroA,MorenoLA,CasajusJA, Vicente-RodríguezG.Cyclingandbonehealth:asystematic review.BMCMed.2012;10(1):168.