r e v b r a s o r t o p . 2016;51(3):374–377
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
report
Stress
fracture
in
acetabular
roof
due
to
motocross:
case
report
夽
Alexandre
de
Paiva
Luciano
∗,
Nelson
Franco
Filho
DisciplineofOrthopedicsandTraumatology,SchoolofMedicine,UniversidadedeTaubaté,Taubaté,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14May2015
Accepted11June2015
Availableonline2April2016
Keywords:
Stressfracture
Acetabulum
Athleticinjuries
a
b
s
t
r
a
c
t
Oneofthefirststepstobetakeninordertoreducesportsinjuriessuchasstressfracturesis
tohavein-depthknowledgeofthenatureandextentofthesepathologicalconditions.We
presentacasereportofastressfractureoftheacetabularroofcausedthroughmotocross.
Thistypeofcaseisconsideredrareintheliterature.Thedescriptionoftheclinicalcaseisas
follows.Thepatientwasa27-year-oldmalewhostartedtohavemedicalfollow-upbecause
ofuncharacteristicpaininhislefthip,whichwasconcentratedmainlyintheinguinalregion
ofthelefthipduringmotocrosspractice.Afterclinicalinvestigationandcomplementary
tests,hewasdiagnosedwithastressfractureoftheacetabularroof.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia
eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Fratura
de
estresse
no
teto
acetabular
por
motocross:
relato
de
caso
Palavras-chave:
Fraturasdeestresse
Acetábulo
Traumatismosematletas
r
e
s
u
m
o
Umdosprimeirospassosparasereduziremlesões,comoafraturadeestressenoesporte,
éconhecermosenosaprofundarmosnoestudodanaturezaeextensãodessapatologia.
Aseguirapresentamosumrelatodecasodefraturadeestressenotetoacetabularpor
motocross.Casoconsideradoraronaliteraturaconsultada.Descric¸ãodoquadroclínico:
pacientede 27anos; masculino, iniciouseguimentomédicopor dores incaracterísticas
noquadrilesquerdo,concentradasprincipalmentenaregiãoinguinaldoquadrilesquerdo
duranteapráticademotocross.Apósinvestigac¸ãoclínicaeporexamescomplementares,
diagnosticou-sefraturadeestressenotetoacetabular.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade
OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudycarriedoutattheDisciplineofOrthopedicsandTraumatology,FaculdadedeMedicina,UniversidadedeTaubaté,Taubaté,SP,
Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.dePaivaLuciano).
http://dx.doi.org/10.1016/j.rboe.2016.03.004
2255-4971/©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopediaeTraumatologia.Thisisanopen
rev bras ortop.2016;51(3):374–377
375
Introduction
Stressfracture isaboneinjurycausedbytheinability ofa
bonetowithstandchronicoverload,amongotherreasons.1,2
Itdiffersfromtraumaticfracturesinosteoporoticbones.We
canalsodefinestressfractureasaninadequateadaptationof
theboneinresponsetothemechanicalloads.3Microscopic
fis-suresinbonemorphology,withoutrestfrommechanicalloads
andwithoutadequatetimefortheirrepair,mayresultinstress
fracture.3
The first clinical description of stress fractures was
reportedbyBreithaupt,aGermanmilitarysurgeonin1855,
apudArmstrongetal.4Stechowreported,in1897,apud
Arm-strong et al.,4 the first radiographic confirmation ofstress
fracturesinmilitaryrecruits,thefractureofametatarsalbone.
ThediagnosisremainedonlyamongthemilitaryuntilPirker
apudArmstrongetal.,4IwamotoandTakeda5reportedthefirst
stressfracturediagnosisinathletes,atransversefractureof
thefemoraldiaphysisin1934.
There has been an exponential growth of motocross
practice throughout the world, with an increase also in
the number of amateur practitioners. Due to the extreme
physical and physiological demands associated to worse
physicalfitness,amateurridersoftensufferfromfatigue.A
localizedmusclefatiguemay resultininadequate function
on demands that are specific to the sports modality, thus
affectingthe performanceand resultinginmusculoskeletal
injuries.6
Motocrosscompetitionsare usuallycarriedoutinclosed
tracks with distances that can reach 1500m. These tracks
incorporatenaturalterrainfeatureswithvaryingnumbersof
jumpsandcurves.Peopleunfamiliartothesportoftenassume
thatthepilotdoesnothingmorethandriveamotorized
vehi-clearoundafield.However,motocrossplacesahighdegree
ofphysicalstresson the upperlimbsand gluteusmuscles
(Fig.1).
Wereportacaseofstressfractureoftheacetabularroof
duetomotocrosspractice.
Fig.1–Motocrossbiomechanics,jumpsandcurves.
Clinical
case
description
A27-year-oldmaleamateurmotocrossrider,searched
med-ical attention due to uncharacteristic pain in his left hip,
concentratedintheinguinalregionduringmotocrosspractice
duringamonth.Hedeniedchronicmedicationuse,previous
surgeriesorpreviouslydiagnosedchronicdiseases.
Thepatientcompetedinamateurclosed-circuitraces,with
distances ranging from 1200 to2500m, including frequent
jumps,alwayswhilewearingpersonalprotectiveequipment.
Hehadtrainingsessionsthreetimesaweekandcompetitions
ontheweekends,whichlastedbetween15and30min.
Physicalexaminationatadmissionshowedweight70kg,
height1.75m,BMI=22.87,withnoabnormalfacies.
Physicalexaminationofthelefthip:
• Inspection:mildlimpingduringgait;withoutatrophies. • Palpation:nopainonpalpationofboneandsofttissue
struc-turesoftheanterior,lateral,posteriorandmedialregionsof
thelefthip;
• Specific tests: Trendelenburg: negative; Ludloff: negative;
Thomas:negative;Ober:negative.
• Degreeofmobility:extension0◦–30◦,flexion0◦–120◦,lateral
rotation0◦–45◦, medialrotation 0◦–35◦, abduction0◦–50◦,
adduction0◦–30◦.
• Neurologicalstrengthtest:GradeV:fullmotionagainstgravity
andagainstgreatresistance.
Concomitantly, imagingtestswererequested:hip
radio-graphy on 03/03/2011 disclosed no signs of fracture, no
abnormalitiesintheacetabularversionangle,andno
defor-mities.Duetothelackofrelevantinformationsobtainedby
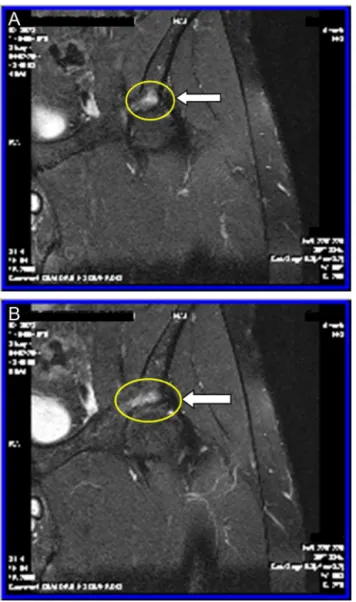
radiographies,hipMRIwasrequestedandperformedonthe
sameday(Fig.2).
Discussion
Publicationsonthephysicalandphysiologicalstressobserved
inmotocrosspilotsafteranofficialcompetitionand/or
tech-nicalandtacticaltrainingarestillscarce.Thus,tounderstand
theneuromuscularandbiomechanicalvariablesofthissports
modalitycanbeoneofthefirststepstoreduceinjuriessuch
asstressfractures.
Stressfractureshavebeendescribedinmanysports
modal-ities,suchasathletics,tennis,basketball,volleyball,football
andbaseball.7,8However,wefoundnoarticlesintheliterature
onstressfracturesintheacetabularroofcausedbymotocross
practice,whichdemonstratestherarityofthereportedcase.
Thereare severalfactorsforriskofstressfracture. They
aredividedintointrinsic(gender,age,ethnicity,andmuscle
strength),extrinsic(trainingregimen,footwear,training
sur-faceandtypeofsport),biochemical(bonemineraldensityand
bonegeometry),anatomical(footmorphology,leglength
dis-crepancyandkneealignment),hormonal(delayedmenarche,
menstrualdisorders and contraceptiveuse)and nutritional
376
rev bras ortop.2016;51(3):374–377Fig.2–LinearhyperintenseimageonT2andSTIR sequences,surroundedbyareaofedemawithpoorly definedlimits;acetabularroofstressfractureissuggested.
Stressfracturesusuallyoccuringroupsofyoung
individ-ualssubmittedtointensephysicalactivities.Thetibiaisthe
mostcommonsiteofinvolvementinathletesandaccounts
for50%ofthetotalcases.However,thefracturelocationvaries
dependingonthesportsmodalitypracticed.8
Theplainradiography isthe first imagingmethod used
inmostcasesand allowsassessingprobableabnormalities
on the acetabular version angle, an important differential
diagnosis forthe stress fracture. However, Magnetic
Reso-nanceImaging(MRI) isthe superior diagnosticmethod for
assessmentofstressfractures, withcomparablesensitivity
andhigherspecificitythanscintigraphy.Itcandemonstrate
the presence of fracture in cases where the conventional
radiographyisconsiderednormal.9MRIismorespecificthan
scintigraphyindetectinghipstressfractures,differentiating
themfromothercausesofboneandsofttissuepain,suchas
avascularnecrosis,bursitisandiliopsoastendonitis.9–11
Williamsetal.12demonstratedtheimportanceofmagnetic
resonanceimagingandscintigraphyinthediagnosisofstress
fracturesoftheacetabularroof.Theyevaluated178active
mil-itary personnel witha history of hip pain associatedwith
physical activity through plainhip and pelvis radiographs,
whichwereinterpretedasnormal.MRIandbonescintigraphy
showed that12of178patients (6.7%)hadimagingfindings
compatiblewithacetabularstressfracture.Twopatternswere
identified.Sevenofthe12(58%)patientshadstressfractures
ofthe acetabularroof. Inthis group,two casesofbilateral
stressfractureoftheacetabularroofwereidentified.Andfive
of12(42%)patientshadanteriorcolumnacetabularfractures,
whichrarelyoccurinisolationandalmostalwayswithastress
fractureofthelowerpubicramus.12Thisdemonstratesthe
rar-ityandhowdifficultisthediagnosisofstressfractureofthe
acetabularroof.
Thediagnosisofhipstressfracturesmustbeconsideredin
anyathletewithhipand/ortheproximalportionofthethigh
pain,especiallyinsportsinvolvingjointimpact.Stress
frac-turescanalsobeobservedinthesacrumandtheischialramus,
neartheinsertionofthesemimembranosus,semitendinosus
andbicepsfemoristendons.10,11
Wedidnotfindaconsensusregardingthetreatmentof
stress fractures of the acetabular roof in the assessed
lit-erature. Therefore, forthiscase,weadoptedthe treatment
protocol formost of stress fractures in athletes. The
frac-turedescribedinthiscasewasconsideredtobeoflowrisk,
similar tomoststressfractures.13,14 These fracturescanbe
treatedwithatwo-stageprotocol.13,14Stage1ischaracterized
bypaincontrolthroughtheprescriptionofanalgesics,
reduc-tion oreliminationofsportsgesturesthatcausesymptoms
andintroductionofphysicaltherapymodalities.Ifthe
indi-vidualisunabletowalkwithoutpain,he/sheshouldremain
immobilized,forinstance,witharemovablestabilizing
ortho-sisand/orapairofcrutches.
Amodifiedactivitythatcanmaintainthephysicalstrength
andfitness,butwithreducedimpact,isprescribed.Activities
suchasrunningintheswimmingpool,ellipticalexercises,free
andstationarybicyclecanmaintainthephysicalstrengthand
fitness, beforethereintroductionofimpactexercises.
Exer-cisesinwaterandanti-gravityonescanbeusedasaresource
tograduallyreintroducesportsgestures.13,14
Phase 2ischaracterizedbyphase1interventionsplusa
gradualreturntosportspractice,tobestartedwhenthe
ath-lete has no pain and normal mobility, around 10–14 days
aftersymptomonset.Thetimetoresumethesports
move-mentsdependsonmanyfactors,includingtheseverityand
chronicity of the injury and functional morbidity level of
theathlete.13,14Forthispatient,treatmentstartedwithpain
control through analgesic prescription, discontinuation of
motocrosspracticeandanyimpactactivity,followedby
phys-icaltherapy.Reintroductionofthesportsgesturebeganafter
symptomssubsidedandMRIcontrolwasperformed90days
aftersymptomonset,withgoodprogression.Heresumedfull
trainingafter120daysandreturntoraces180daysafter
begin-ningtreatment.
Conflicts
of
interest
rev bras ortop.2016;51(3):374–377
377
r
e
f
e
r
e
n
c
e
s
1. GarrettWEJr,SafranMR,SeaberAV,GlissonRR,RibbeckBM. Biomechanicalcomparisonofstimulatedandnonstimulated skeletalmusclepulledtofailure.AmJSportsMed.
1987;15(5):448–54.
2. O’BrienFJ,TaylorD,CliveLeeT.Theeffectofbone
microstructureontheinitiationandgrowthofmicrocracks.J OrthopRes.2005;23(2):475–80.
3. BurrD,MigromC.Musculoskeletalfatigueandstress fractures.BocaRaton,FL:CRCPress;2001.
4. ArmstrongDW3rd,RueJP,WilckensJH,FrassicaFJ.Stress fractureinjuryinyoungmilitarymenandwomen.Bone. 2004;35(3):806–16.
5. IwamotoJ,TakedaT.Stressfracturesinathletes:reviewof196 cases.JOrthopSci.2003;8(3):273–8.
6. AvelaJ,KyröläinenH,KomiPV.Neuromuscularchangesafter long-lastingmechanicallyandelectricallyelicitedfatigue.Eur JApplPhysiol.2001;85(3–4):317–25.
7. BergerFH,deJongeMC,MaasM.Stressfracturesinthelower extremity.Theimportanceofincreasingawarenessamongst radiologists.EurJRadiol.2007;62(1):16–26.
8.NattivA,PufferJC,CasperJ.Stressfractureriskfactors, incidence,anddistribution:a3yearprospectivestudyin collegiaterunners.MedSciSportsExerc.2000;32Suppl. 5:S347.
9.StollerDW,MaloneyWT,GlickJM.Thehip.In:StollerDW, editor.Magneticresonanceimaginginorthopaedics&sports medicine.SanFrancisco:Lippincott;1997.p.93–202.
10.KneelandJB.MRimagingofsportsinjuriesofthehip.Magn ResonImagingClinNAm.1999;7(1):105–15.
11.ResnickD,KangHS.Pelvisandhip.In:ResnickD,KangHS, editors.Internalderangementofjoints.SanDiego:Saunders; 1997.p.473–554.
12.WilliamsTR,PuckettML,DenisonG,ShinAY,GormanJD. Acetabularstressfracturesinmilitaryenduranceathletes andrecruits:incidenceandMRIandscintigraphicfindings. SkeletRadiol.2002;31(5):277–81.
13.BodenBP,OsbahrDC,JimenezC.Low-riskstressfractures. AmJSportsMed.2001;29(1):100–11.