w w w . r b o . o r g . b r
Case
Report
Intraosseous
lipoma
of
the
iliac:
case
report
夽
Frederico
Barra
de
Moraes
∗,
Rodrigo
Marques
Paranahyba,
Rogério
Andrade
do
Amaral,
Vinícius
Mendes
Bonfim,
Nathalya
Ducarmo
Jordão,
Raimundo
Djalma
Souza
SchoolofMedicine,UniversidadeFederaldeGoiás,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24October2014
Accepted19February2015
Availableonline2January2016
Keywords:
Boneneoplasms/etiology
Boneneoplasms/diagnosis
Lipoma
a
b
s
t
r
a
c
t
Lipomasarebenigntumorsthatattackfatcellsandmostoftenaffectingsofttissuesin
adult-hood.Onrareoccasions,theymayaffectbones,preferentiallythemetaphysesofthelong
bone.Theyaregenerallyasymptomaticandradiographyshowsradiolucentlesionswitha
thinscleroticrimorradiodenselesionswithathickscleroticrim.Malignanttransformation
ofthesetumorsisrare,asistheirrecurrence,andthereisnoneedforsurgeryinmostcases.
Inthisreport,wepresentararecaseofintraosseouslipomaintheiliacbone.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Lipoma
intraósseo
do
ilíaco:
relato
de
caso
Palavras-chave:
Neoplasiasósseas/etiologia
Neoplasiasósseas/diagnóstico
Lipoma
r
e
s
u
m
o
Oslipomassãotumoresbenignosqueacometemcélulasadiposas,maiscomumenteafetam
ostecidos molesnaidadeadulta.Raramentepodemafetarosossos,preferencialmente
metáfisesdosossoslongos.Sãogeralmenteassintomáticos,naradiografiaverifica-selesão
radiotransparente,comumafinabordaescleróticaoulesãoradiodensacomumaespessa
bordaesclerótica.Atransformac¸ãomalignadotumorérara,assimcomoarecorrência,sem
necessidadecirúrgicanamaioriadoscasos.Nesterelatoapresentamosumcasorarode
lipomaintraósseodoilíaco.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Todososdireitosreservados.
夽
WorkperformedintheUniversidadeFederaldeGoiás,SchoolofMedicine,HospitaldasClínicas,DepartmentofOrthopedicsand
Traumatology,Goiânia,GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.deMoraes).
http://dx.doi.org/10.1016/j.rboe.2015.12.011
thattheydonotpreferentiallyaffecteithersex.Theagegroup
affected isverywide, and casescanbe foundbothamong
childrenandamongelderlypeople.Theyaremostcommonly
diagnosedinthefourthdecadeoflife.Theiretiologyremains
unknownandisamatterofcontroversy.2
Intraosseous lipomas may affect any part of the
skele-tonandaremostfrequentlylocatedinthetranstrochanteric
regionoftheproximalfemur(34%),tibia(13%),fibula(10%),
calcaneus(8%), iliac bone(8%) andhumerus and ribs(5%).
Theypreferentiallyaffectthemetaphysesoflongbonesand
presentassinglelesions.However,reportsofmultipletumors
scatteredaroundtheentireskeletonhavebeenmade.3
Lipomaspresentfew symptoms.Pain isthe commonest
ofthese,andthe absenceofspecificsymptomsmay cause
difficultyinmakingthediagnosis.Thereisaneedfortheaid
ofimagingexaminations.However,oncethelipomahasbeen
found,theprognosisisgenerallygoodandafullcurecanbe
achieved.4Theobjectiveofthisstudywastoreportonarare
caseofintraosseouslipomaoftheiliac.
Case
report
Thepatientwasa45-year-oldmanwhoreportedhaving
insid-iouspaininhisrighthipthathadstartedthreemonthsearlier.
Itwasunrelatedtotraumaanddidnothaveanyspecific
char-acteristics.Thepainscoreonavisualanaloguescale(VAS)
was5/10,anditimprovedthroughuseofnon-steroidal
anti-inflammatorydrugsandworsenedwithslighteffort.
Physicalexaminationdidnotshowanylimitationof
move-mentsofthepelvis,lumbarspineorrighthip.Radiography
wasthenperformedonthepelvisinanteroposteriorview.A
circumferentialosteolyticlesioninthewingoftherightiliac,
ofapproximately3cmindiameter,withwell-definededges,
wasobserved(Fig.1A).Becauseofthenonspecificnatureofthe
imageobtainedthroughradiography,tomographywith
three-dimensionalreconstructionwasrequested.Alesionaffecting
theposteriorcorticalboneofthewingoftherightiliaccould
beseen(Fig.1B).
Acoronalslice forabonewindow(Fig.2A)andanaxial
sliceforasoft-tissuewindow(Fig.2B)showedthatthelesion
extendedthroughthemedullarytissue,fromthe
anterome-dialtotheposterolateralregionoftherightiliacbone.Inthis
region,therewasfracturingofthecorticalbone,ofosteolytic
andinsufflativenature.
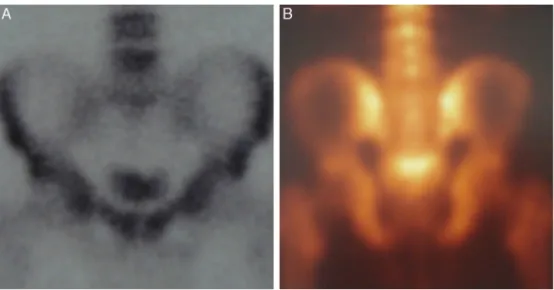
Bonescintigraphywithtechnetiumwasperformedanddid
notshowthelesion(Fig.3AandB),whichsuggestedthatthe
lesionwasofbenignnature.Tocomplementtheevaluation,
magneticresonancewasperformedonthepelvis.Inthis,T1
coronalimaging showeda lesion withhyposignal, without
invasionofsoft tissues(Fig.4A).T2coronalimagingofthe
pelvis(Fig.4B)showedalesionwithhypersignalintheright
iliac.
nityinthematerial.Thesuspicionofbenigntumorformation
wasthusconfirmedanditwasdiagnosedasanintraosseous
lipoma.Aroundthreemonthsaftertheprocedure,thepatient
nolongerpresentedpainandtherewasnorecurrenceofthe
lesion.
Discussion
Intraosseouslipomaisarare benigntypeofbonetumor.It
mainlyaffectsthemetaphysisoflong bonesandis
asymp-tomatic inapproximatelyhalf ofthe cases.5,6 Itaffects the
sexesalmostequally,suchthatitisslightlymoreprevalent
amongmales.6Itoccursinallagegroups,anditslightlymore
prevalentinthefourthandfifthdecadesoflife.5Involvement
oftheiliacboneisevenrarer.6,7
Dhalincalculatedtheincidenceofintraosseouslipomasas
oneinevery1000bonetumors.8However,theincidencemay
begreaterbecauseofthedifficultyindiagnosingcasesofthis
typeoflipoma.Itiscommonforsuchdiagnosestobemade
accidentallythroughimagingexaminations.5,9
Thefirstreportofintraosseouslipomaoftheiliacbonewas
madebyBuckleyandBurkus10in1988.Sincethen,duemainly
todevelopmentofdiagnostictechniques,thenumberofcases
of intraosseous lipoma reported has increased.
Nonethe-less,alocation intheiliac bonecontinuestobeextremely
rare.11
When intraosseouslipomas are symptomatic,they may
generateclinicalmanifestationssuchaspain,localswelling
and pathological fractures.5,6 Thelack ofsigns and
symp-toms differsintraosseouslipomasfrom other bonetumors
and this is a difficulty that is found in diagnosing this
type of tumor.5,7 Its etiology is a matter of controversy.9
However, there are reports in the literature of patients
withhyperlipoproteinemiaandmacrodystrophialipomatosa
whodevelopedmultipleintraosseouslipomas.12,13Sauerand
Ozonoff14demonstratedapossiblerelationshipbetween
con-genitalboneabnormalitiesandlipomas.Anotherreasonwhy
diagnosingintraosseouslipomasmaybedifficult,whichhas
beenreportedintheliterature,isthatitsradiologicalimages
maybeconfoundedwithboneinfarction,osteoblastomasand,
morerarely,enchondromas.9
AccordingtoMilgram’sclassification,intraosseouslipomas
aredividedintothreestages.StageIcomprisessolidtumors
withviableadipocytes;stageIIcomprisescasesoffocal
tran-sitioninwhichfattynecrosisandfocalcalcificationareseen,
alongwithregionswithviableadipocytes;andlastly,stageIII
consistsoflate-stagecasesinwhichthereisfattynecrosis,
cystformation,calcificationandreactiveformationofanew
bonestructure.Mostofthelesionsthathavebeendescribed
areinstageI.Thesestagechangesresultfromaprocessof
involutionandinfarctionthattheselesionsundergowiththe
passageoftime.6Lesionsattheinitialstagescause
Fig.1–Radiographofthepelvisinanteroposteriorview,showingcircumferentialosteolyticlesionsinthewingoftheright
iliac,ofapproximately3cmindiameter,withwell-definedborders(A).Tomographywiththree-dimensionalreconstruction,
inwhichalesionaffectingtheposteriorcorticalboneofthewingoftherightiliacisobserved(B).
Fig.2–Tomographicslicesincoronalviewforabonewindow(A)andinaxialviewforasoft-tissuewindow(B),showing
thatthelesionextendsthroughthemedullarytissue,fromtheanteromedialtotheposterolateralregionoftherightiliac
bone.Inthisregion,therewasfracturingofthecorticalbone,ofosteolyticandinsufflativenature.
Fig.3–Bonescintigraphywithtechnetium,whichdidnotshowthelesion(AandB),thussuggestingthatitwasofbenign
Fig.4–Magneticresonanceimagingofthepelvis,inwhichtheT1coronalimageshowedalesionwithhyposignal,without
soft-tissueinvasion(A),andinT2(B)withhypersignalintherightiliac.
Because of the different presentational stages of
intraosseous lipomas, they may appear on radiographs
bothasradiolucentlesionswithathinscleroticborderandas
radiodenselesionswithathickscleroticborder.7From
radio-graphy,thedifferentialdiagnosisalsodependsonthecurrent
stageoftheintraosseouslipoma.Themaindifferential
diag-nosesreportedintheliteratureare:bonepseudocyst, bone
infarction, fibrous dysplasia, osteoblastoma, enchondroma,
chondroblastoma, chondrosarcoma, non-ossifying fibroma
andgiant-cellbonetumor.16,17
Itisbelieved thatcomputedtomography(CT)scansand
magnetic resonance imaging (MRI) are the most complete
examinationsforissuingadiagnosis,sincethesearecapable
ofrevealingstageIlesionsandthefatringsthatare
character-isticofstageIIandIIIlesions.7Moreover,becauseofthelarge
numberofdifferentialdiagnosesgiventhroughradiography,
asseenearlier,manyauthorshaverecommendedthatCTand
MRIshouldbeusedtoruleoutotherhypotheses.
CTisusefulindiagnosingintraosseouslipomasbecauseit
revealsanattenuationthatischaracteristicofadiposetissue.
Thetissuedensitycanbecalculatedthroughthe“Hounsfield
index”.6Adiposetissuepresentslowerdensitythanfibrous
tissueandcellularneoplasmsand,forthisreason,isespecially
radiolucent.17Insomecases,CTimagesmaybeverytypicalof
intraosseouslipomas,whichhasledmanyauthorstosuggest
thatbiopsycanbedoneawaywith.15–18
OnCT, stageIlesions are characterizedbyreabsorption
ofthe bonetrabeculae and byboneexpansion. Anarea of
attenuationcorrespondingtotheareaofradiolucencyofthe
radiographcanbeseen.StageIIisdemonstratedthroughareas
ofattenuationtogetherwithareasofcalcificationandfatty
necrosis.StageIIIlipomasaretheonesthataremostdifficult
todiagnosebecauseoftheossification,calcification,necrosis
andcystformation.7
UseofMRIfordiagnosingintraosseouslipomasis
impor-tantbecause thedensity oftheselesions issimilartothat
ofsubcutaneoustissue,bothinT1and inT2.MRIonstage
I lesions shows that they have the same density as the
subcutaneous tissue in T1 and shows hyposignal in T2.
IN stage II, areas of hyposignal are shown in the central
regionofT1andT2,whichareconsistentwiththeareasof
calcification.Inaddition,aringofsclerosiscanbeviewed.In
stageIII,athinringoffatcanbeseen,alongwithanareaof
centralcalcificationandawideringofsclerosisthatpresents
hyposignal inT1and T2. Theareas offatty necrosisshow
variablesignalinT1andhypersignalinT2.7
Histologically,thelesionsarecharacterizedbythepresence
ofmaturefattytissueandatrophiedbonetrabeculae.
Differ-entiationbetweenneoplasticandnon-neoplasticadiposecells
isfundamental,althoughcomplicated.Anincreasednumber
ofbloodvesselsmaybeoneoftheindicatorsofmalignity.In
histologicalanalysesonlipomas,itisalsocommontoobserve
mucinousdegenerationand,becauseofthis,microscopicand
macroscopiccystsmayalsobeobserved.6,19
Evenhistologically, itisdifficulttodifferentiatebetween
lipomasandboneinfarctions,butcertaincharacteristicsmay
assistinthis.Ininfarctions,thelackofcalcificationscanbe
highlighted.Inlipomas,diminutionofthetrabecular
struc-tures,expansionofthecorticalboneandpossiblepresenceof
cystscanbehighlighted.15
Regarding treatment of intraosseous lipomas, surgery
is not indicated in most cases of asymptomatic patients.
For symptomatic patients, the tumor can be treated with
curettageandimplantationofabonegraft.5,6Malignant
trans-formationofthetumorisrare,asisrecurrence.5,6,19
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
2. FochesattoLQ,SchwankeR,KaramFC,SerafiniAO.Lipoma intraósseodocalcâneo:relatodecaso.RevBrasOrtop. 1998;33(1):917–8.
3. VargasCSV,GonzalezC,AtencioE,CellamareO,FuenmayorJ, NietoO.Lipomaintraóseodelcalcâneo.Apropósitodeun casoclínico.AcadBiomDigital.2011;48:987.
4. ÖztekinÖ,ArginM,OktayA,ArkunR.Intraosseouslipoma: radiologicalfindings.RadiolBras.2008;41(2):81–6.
5. MilgramJW.Intraosseouslipomas:radiologicandpathologic manifestations.Radiology.1988;167(1):155–60.
6. MilgramJW.Intraosseouslipomas:aclinicpathologicstudy of66cases.ClinOrthopRelatRes.1988;231:277–301.
7. PropeckT,BullardM,LinJ,DoiK,MartelW.
Radiologic-pathologiccorrelationofintraosseouslipomas. AJRAmJRoentgenol.2000;175(3):673–8.
8. UnniK.Lipomaandliposarcoma.In:UnniK,editor.Dahlin’s bonetumors:generalaspectsanddataon11087cases. Philadelphia:Lippincott-Raven;1996.p.349–53.
9. ChowLT,LeeKC.Intraosseouslipoma.Aclinicpathologic studyofninecases.AmJSurgPathol.1992;16:401–10.
10.BuckleySL,BurkusJK.Intraosseouslipomaoftheilium.A casereport.ClinOrthopRelatRes.1988;(228):297–301.
11.GotoT,KojimaT,IijimaT,YokokuraS,MotoiT,KawanoH, etal.Intraosseouslipoma:aclinicalstudyof12patients.J OrthopSci.2002;7(2):274–80.
12.RehaniB,WissmanR.Multipleintraosseouslipomatosis:a casereport.CasesJ.2009;2:7399.
13.DohlerR,PoserHL,HarmsD,WiedemannHR.Systemic lipomatosisofbone.JBoneJointSurgBr.1982;(6491): 84–7.
14.SauerJM,OzonoffMB.Congenitalboneanomaliesassociated withlipomas.SkeletalRadiol.1985;13(4):276–9.
15.WilliamsCE,ClosePJ,MeaneyJ,RitchieD,CogleyD,CartyAT. Intraosseouslipomas.ClinRadiol.1993;47(5):348–50.
16.GoldmanAB,MarcoveRC,HuvosAG,SmithJ.Casereport280: intraosseouslipomaofthetibia.SkeletalRadiol.
1984;12(3):209–12.
17.OnguruO,Pabuc¸cuY,CelasunB.Intraosseouslipomaofthe fibula.ClinImaging.2002;26(1):55–7.
18.SchatzSG,DipaolaJD,D’AgostinoA,HannaR,QuinnSF. Intraosseouslipomaofthecalcaneus.JFootSurg. 1992;31(4):381–4.