REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Anesthetic
requirements
measured
by
bilateral
bispectral
analysis
and
femoral
blockade
in
total
knee
arthroplasty
Maylin
Koo
∗,
Javier
Bocos,
Antoni
Sabaté,
Vinyet
López,
Carmina
Ribes
HospitalUniversitariodeBellvitge,ServiciodeAnestesiayMedicinaIntensiva,Barcelona,Spain
Received14January2016;accepted20July2016 Availableonline28August2016
KEYWORDS
Nerveblock; Painmanagement; Bispectralindex monitor; Levopubicaine hydrochloride; Kneearthroplasty
Abstract
Backgroundandobjectives: A continuous peripheralnerve blockade has proved benefits on
reducing postoperative morphineconsumption; thecombination ofa femoral blockadeand
generalanesthesiaonreducingintraoperativeanestheticrequirementshasnotbeenstudied. Theobjectiveofthisstudy wastodeterminetherelevanceoftimingintheperformanceof femoral blocktointraoperative anesthetic requirementsduringgeneralanesthesiafor total kneearthroplasty.
Methods:Asingle-center,prospectivecohortstudyonpatientsscheduledfortotalknee
arthro-plasty,weresequentiallyallocatedtoreceive20mLof2%mepivacainethroughoutafemoral catheter,priortoanesthesiainduction(Preoperative)orwhenskinclosurestarted (Postopera-tive).Analgorithmbasedonbispectralvaluesguidedintraoperativeanestheticmanagement. Postoperativeanalgesiawas donewithanelastomericpumpoflevobupivacaine0.125% con-nectedtothefemoralcatheterandcomplementedwithmorphinepatientcontrolanalgesiafor 48hours.TheKruskallWallisandthechi-squaretestswereusedtocomparevariables.Statistical significancewassetatp<0.05.
Results:Therewere94 patients,47preoperativeand47postoperative.Lowerfentanyland
sevofluranewereneededintraoperativelyinthePreoperativegroup;medianvaluesandrange: 250(100---600)vs450(200---600)gand21(12---48)vs32(18---67)mLp=0.001,respectively.There
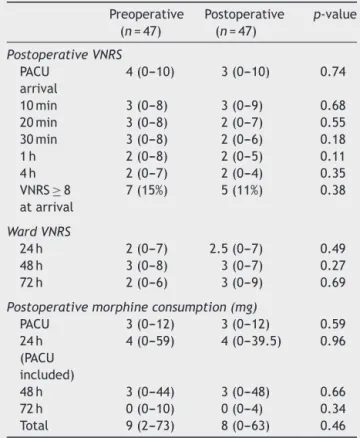
werenodifferencesinthemedianverbalnumericratingscalevalues4(0---10)vs3(0---10);and inmedianmorphineconsumption9(2---73)vs8(0---63)mgpostoperatively.
Conclusions:Apreoperativefemoralblockadeisusefulindecreasinganestheticrequirements
intotalkneearthroplastysurgerybutnoaddedeffectinthepostoperativeanalgesiccontrol. ©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeAnestesiologia. Thisisanopenaccess articleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](M.Koo).
http://dx.doi.org/10.1016/j.bjane.2016.07.013
PALAVRAS-CHAVE
Bloqueiodenervos; Tratamentodador; Monitordeíndice bispectral; Cloridratode levobupivacaína; Artroplastiadejoelho
Necessidadedeanestésicosavaliadacomaanálisedoíndicebispectralbilateral ebloqueiofemoralemartroplastiatotaldejoelho
Resumo
Justificativaeobjetivos: Obloqueiocontínuodenervosperiféricosprovouserbenéficopara
reduzir oconsumo de morfina no pós-operatório. A combinac¸ãode um bloqueiofemoral e
anestesia geral para reduzir anecessidade de anestésicosno intraoperatórioainda não foi avaliada.Oobjetivodesteestudofoideterminararelevânciadomomentopropíciodurantea realizac¸ãodobloqueiofemoralparaanecessidadedeanestésicosnointraoperatóriodurantea anestesiageralparaartroplastiatotaldejoelho(ATJ).
Métodos: EstudoprospectivodecoortedepacientesagendadosparaATJ.Ospacientesforam
sequencialmentealocadosemgrupospararecebermepivacaínaa2%(20mL)duranteainserc¸ão docateterfemoral,antesdainduc¸ãodaanestesia(pré-operatório)ounoiníciodofechamento
da pele(pós-operatório). Umalgoritmocom basenos valores doBISorientou omanejo da
anestesia no intraoperatório.Analgesiano pós-operatório foi administrada viabomba
elas-toméricadelevobupivacaína a0,125%conectadaao cateterfemoralecomplementada com
analgesia (morfina)controladapelopaciente durante48horas. Ostestes deKruskallWallis e do qui-quadrado foram usados para comparar as variáveis. A significância estatística foi estabelecidaemp<0,05.
Resultados: Foramestudados94pacientes,47nopré-operatórioe47nopós-operatório.Houve
menosnecessidadedefentanilesevofluranoduranteoperíodointraoperatórionogrupo pré-operatório;medianasevariac¸õesdosvalores:250(100---600)vs.450(200---600)ge21(12---48)
vs.32(18---67)mLp=0,001,respectivamente.Nãohouvediferenc¸asnasmedianasdosvalores dasescalasdeclassificac¸ãonuméricaeverbal,4(0---10)vs.3(0---10),enasmedianasdoconsumo demorfina,9(2---73)vs.8(0---63)mgnopós-operatório.
Conclusões: O bloqueio femoral no pré-operatório é útil para diminuir a necessidade de
anestésicosemATJ,masnãotemefeitoadicionalnocontroledaanalgesianopós-operatório. ©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradeAnestesiologia. Este ´eum artigo Open Access sob umalicenc¸aCC BY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
The incidence of primary total knee arthroplasty (TKA) reported annually ranges from 30 to 199 per 100,000 inhabitants.1 Different anesthesia techniques have been usedtoperformTKA,includinggeneralanesthesiaand dif-ferent forms of regional anesthesia: neuraxial blockade and peripheral nerve blockade of lower extremity.2 TKA producesseverepaininthepostoperativeperiod,and treat-ment of this complication is challenging for both patient comfort and early rehabilitation. Standard care for ade-quate analgesia in TKA consists of balanced intravenous administrationofopioidscombinedwithnonsteroidal anti-inflammatorydrugs.Recently,continuousperipheral nerve block has been demonstrated to be beneficial, basically throughreducingpostoperativemorphineconsumptionand consequently,morphine-relatedsideeffects.3,4
A femoralcathetercan beplaced inpatients undergo-ingTKAbeforeanesthesiainductionoraftertheconclusion of the surgery. Performing the block prior to surgery is intendedtopreventpain;however,ithasnotshownaclear benefit.5---7Theassociationofaneuraxialblockandgeneral anesthesiahasbeen shown toreduce hypnoticand opioid requirements,8---10andtoproducebetterpostoperativepain control.11 Nevertheless, the combination of a continuous femoralblockandgeneralanesthesiahasnotbeenstudied.
The hypothesis this study addressed was that a pre-surgery incision femoral block would reduce the general anestheticrequirements duringthe procedure, andwould reduce pain andanalgesic consumption in the postopera-tive period. The principal objective of the study was to determinethe relevanceof thetiming ofa femoralblock to intraoperative anesthetic requirements during general anesthesiafor kneereplacement surgery. We alsostudied whetherthetimingofthefemoralblockadeinfluenced post-operativevariables,suchaspain,opioid consumptionand bloodloss.
Methods
Thiswasasingle-center,prospectivecohortstudy.Patients wereallocatedtooneof twogroups; theanesthesiologist incharge ofthe patientwasnotblinded.All thepatients werealwaysmanaged duringthe intraoperativeperiodby astrict anesthesiaprotocol. Surgeons andphysicians that followeduponpatients,aswellasnursesfromthe Postop-erativeAnesthesiaCareUnit(PACU)andwardwereblinded topatientallocation.
BIS<40 BIS 40-60 BIS >60
Blood pressure <90 mmHg
Every 4 minutes
Decrease sevoflurane 0.4%
Decrease sevoflurane 0.4%
Urapidil 2.5 mg
Ephedrine 5 mg
Normal hemodynamic values BIS=40-60
Fentany1
1 μg .kg–1
Fentany1
1 μg .kg–1
Every 4 minutes
Every 4 minutes
Every 4 minutes
Increase Sevoflurane 0.4% 250 ml crystalloids
CAM>1.3 Blood pressure
>165 mmHg Increase Sevoflurane 0.4% Every
4 minutes
Every 4 minutes
Every 4 minutes Blood pressure
>165 mmHg
Blood pressure >165 mmHg
Blood pressure >165 mmHg Blood pressure
<90 mmHg
Blood pressure <90 mmHg
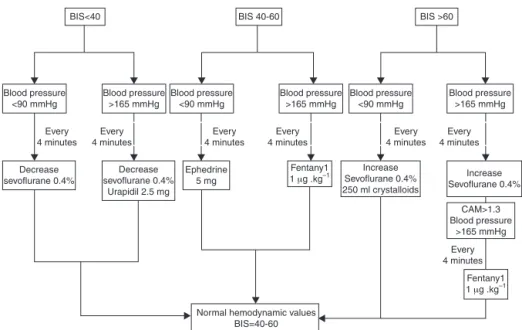
Figure1 Anestheticintraoperativemanagement.
fromBarcelona,onDecember10th,2009:protocolnumber EPA020/09.
Eligible participants were all adult patients who were scheduled for TKA. All the candidates were capable of understanding the analgesic protocol. Exclusion criteria were:thepresenceofneurologicdisease,theuseof medi-cationactingonthecentralnervoussystem,intoleranceor allergytononsteroidalanti-inflammatorydrugs, allergyto localanesthetics,ahistoryofuncontrolleddiabeticdisease, difficultairwaymanagement,ahistoryofasthmaticdisease, ahistoryofarterialvascularlimbsurgeryorhighriskdeep venousthrombosis,ahistoryofseverecardiacdiseaseand theinabilitytouseaPatient-ControlledAnalgesia(PCA) sys-tem.The studywasexplainedtoallthepatientsandthey werealsogivenwritteninformation.Theywereenrolledif theygavesignedconsent.Studyrecruitmenttookplacefrom January2010toJune2011.
All the patients were admitted onthe day of surgery. Beforeanesthesiainduction, acatheter(Pajunk Stimulong Bonus216×64mm2set)wasplaced,withasepticmeasures,
closetothefemoralnerve,usinganultrasoundtechnique (Ultrasound scanner S-Nerve Sonosite,) for localization of thenerveandwithoutnervestimulation.The injectionof 3---5mL of dextrose serum around the nerve was used to confirmthecatheterplacement.
Patientsweresequentiallyallocatedinblocksoffourto eachfemoralgroup.Threeanesthesiologistswhowerenot blindedtotherandomsequenceparticipatedinthe alloca-tionandintheintraoperativemanagementofthepatients. Oncethecatheterwasplaced,thepatientsreceived20mL of mepivacaine 2% 5min prior to anesthesia induction (Group: Preoperative) or the same volumeof local anes-theticattheendofthesurgery,whenskinclosurestarted (Group:Postoperative).Again,theanesthesiaadministrator wasnotblindtothegroupallocation.
Oxygenwasgivenfor5minbeforeanesthesiainduction, whichwasaccomplishedwith3g.kg−1offentanylfollowed by2mg.kg−1ofpropofol,toobtainaBispectralScore(BIS)of <60,androcuronium0.6mg.kg−1.Aftertrachealintubation,
sevofluraneconcentrationsweresettoachieveBISvaluesof 40---60.Anesthesiamaintenancewasstartedwithaninspired fraction of sevoflurane(FISEVO) concentration of 2.5% in a freshgasflowof4L.min−1for4mintoreachaMinimum Alve-olarConcentration(MAC)of1.3,inordertomaintaintheBIS valuesbetween40and60.Oncethisobjectivewasachieved, the fresh gas flow was decreased to2L.min−1 and there-fore,thesevofluranevaporizerwasincreasedordecreased in0.4%stepstoreachthepredeterminedBISvalues(Fig.1). Thelungswereventilatedtomaintaintheend-tidalcarbon dioxideconcentration(ETCO2)at30---35mmHg.Rocurorium bolus wasadministeredat 0.15mg.kg−1 ifthereweretwo responses on the Train Of Four ratio (TOF) or when the patientshowedsignsofinadequateneuromuscularblockade for surgery suchas ventilatorasynchrony or clear patient movement.Oncesurgeryended,theneuromuscular block-ade wasreversed with an adequate dose of neostigmine. Tracheal extubationwasperformed when thepatientwas consciousandbreathingcomfortablywithanoxygen satura-tionofabove92%.
Allpatientswerewarmedwithasystemofheat convec-tion(Warmtouch,Mallinckrodt, St.Louis,MO)tomaintain bodytemperaturebetween35.5◦Cand36.5◦C.Monitoring included pulseoximetry, esophageal temperature,ETCO2, TOF,BIS,compositevariableindex(CVI)andFISEVO−FESEVO ofsevoflurane(DatexOhmedasystem).
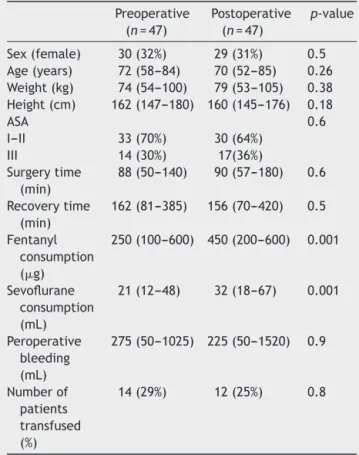
Table1 Patientcharacteristicsandintraoperativedata.
Preoperative (n=47)
Postoperative (n=47)
p-value
Sex(female) 30(32%) 29(31%) 0.5
Age(years) 72(58---84) 70(52---85) 0.26
Weight(kg) 74(54---100) 79(53---105) 0.38
Height(cm) 162(147---180) 160(145---176) 0.18
ASA 0.6
I---II 33(70%) 30(64%)
III 14(30%) 17(36%)
Surgerytime (min)
88(50---140) 90(57---180) 0.6
Recoverytime (min)
162(81---385) 156(70---420) 0.5
Fentanyl consumption (g)
250(100---600) 450(200---600) 0.001
Sevoflurane consumption (mL)
21(12---48) 32(18---67) 0.001
Peroperative bleeding (mL)
275(50---1025) 225(50---1520) 0.9
Numberof
patients transfused (%)
14(29%) 12(25%) 0.8
Data expressed as number and (percentage) or median and (range).
runningRugloopdatacollectionsoftwarethatcomputedthe synchronizationoftheinformationfromtheBISVISTA mon-itorandtheDatexOhmedapatientmonitor.Cliniciansused the Rugloop softwareto recordthe following times, used forcomparativeanalysis:basalsituation;1minafter anes-thesiainduction;5minaftercuffischemiapriortosurgery starts;5minafterskinincision;5minafterunlockingofcuff ischemia;endofsurgery;andafterclosureofthe sevoflu-rane vaporizer when the patient was able to respond to oral commandsand the tracheal tube was removed. The totaldoseoffentanylandthetotalofsevoflurane consump-tionwererecordedattheendoftheprocedure.Thelatter wasobtainedfromthe valueregistered by theanesthesia machineinmLconsumedduringthetotalprocedure.
Abasalbloodsamplewasextractedfromthepatientat anesthesiainduction andanothersamplewastakenat the endofthesurgery,toperformthefollowingdeterminations: acid base status, lactate, glucose, creatinine, creatinine phosphokinaseandpotassium.
In orderto ensure the homogeneity and safety of the anesthetic management, a specific intraoperative anes-thetic protocol (Fig.1) was implemented.Blood pressure was measured every 5min. If the Systolic BloodPressure (SBP) waslowerthan90mmHgandtheBISvalueswerein the range of 40---60, a repeatbolus of 5mg of ephedrine wasadministeredintravenously.IftheSBPwaslowerthan 90mmHgandtheBISvaluewaslowerthan40,the sevoflu-rane vaporizer was decreased by 0.4%, until a BIS value of 40 or more was achieved. If the SBP was higher than
165mmHgandthe BISvalue wasover60, thesevoflurane vaporizerwasincreasedby0.4%,untilaBISvalueof60or less was achieved. If the SBP washigher than 165mmHg and the BIS values were in the range of 40---60, a bolus of 1g.kg−1 of fentanyl was administered until adequate SBP was achieved, assuming inadequate hypnosis as the mainreasonofhypertension.Ifheart ratewaslowerthan 50 beats per minute, 1mg of atropine was administered intravenously.
Forthepostoperativeanalgesicprotocol,priorto recov-ery from the anesthesia, all patients in both groups receivedanelastomericpumpwithlevobupivacaine0.125% atan infusion rateof 7mL.h−1,connectedtothefemoral catheter,and1gofparacetamoland50mgofdexketoprofen intravenously.
OncethepatientreachedthePACU,thenurseincharge, who was unaware of the timing of the local anesthetic administration, started a PCA system (GemstarSiete Ter-apias, Hospira, Madrid, Spain) with morphine. Pain was assessedusingaVerbalNumericRatingScale(VNRS)(0=no pain;1---3=mildpain;4---7,moderatepain;and8---10,severe pain).Intravenousmorphinebolusesof2mgwereinjected every5minuntiltheVNRSscorewas<4;thereafter,thePCA system delivereda 0.5mg dose of morphine with a 5min lockouttime.Oncethepatientsreachedthestandards,the nurseinchargesentthepatienttoawardwiththePCA sys-temconnectedtoanintravenousline andtheelastomeric pumpwithlevobupivacaine0.125%connectedtothefemoral catheter.Bothinfusion systemsweremaintained for 48h. Afterthat,theanalgesicregimenconsistedin4mgof sub-cutaneousmorphineadministeredonpatientdemand.The VNRSvaluesandtotaldoseofmorphinewererecordeduntil theendoftheinfusion.
Theprimaryendpointwasthetotalintraoperative con-sumption of sevoflurane (mL). The secondary outcomes measured were:the fentanyl administeredduring surgery (mL);theVNRSatfixedintervals(0h,10min,20min,30min, 1h,4h,24h,48h and72h) afterthe endof surgery;the postoperativedosesofmorphineinthePACU,andat 24h, 48h and72h;peroperative bleeding, this wasthesum of the intraoperative bleeding and the postoperative blood drainrecordedinthePACU;thepercentageofpatientsthat requiredpackedred blood units;and recoverytime, esti-matedastheperiodfromtheendofsurgerytoadmittance ontheward.
A sample size of a minimum of 40 patients in each groupwascalculated,takingintoconsiderationan˛-value of0.05, a ˇerror of 0.2, anda differencein sevoflurane consumptionof35%betweenthegroups(primaryoutcome variable).
SurgeonsandnursesfromthePACUunitandward,who recordedthe VNRSvalues, where keptblinded topatient allocation.Physicianswhofolloweduponpatientswerealso blindedtothefemoralgroupassignment.
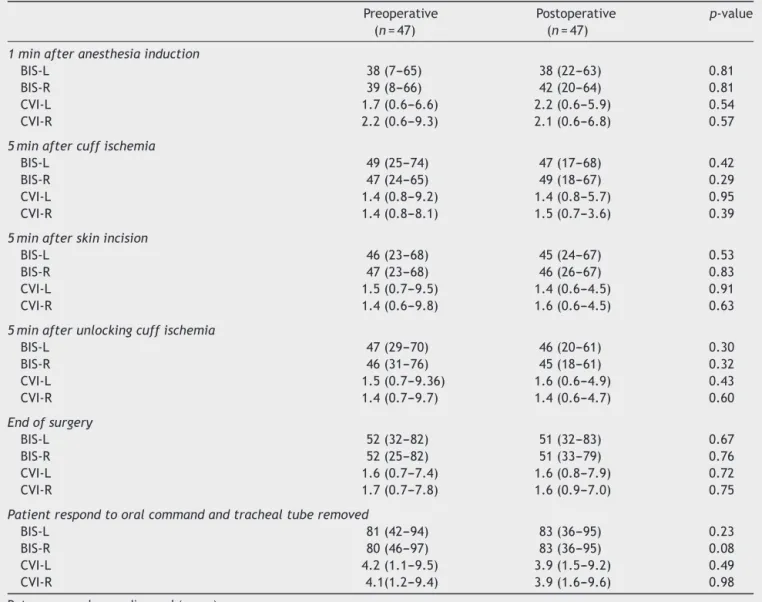
Table2 Electroencephalographicvalues.
Preoperative (n=47)
Postoperative (n=47)
p-value
1minafteranesthesiainduction
BIS-L 38(7---65) 38(22---63) 0.81
BIS-R 39(8---66) 42(20---64) 0.81
CVI-L 1.7(0.6---6.6) 2.2(0.6---5.9) 0.54
CVI-R 2.2(0.6---9.3) 2.1(0.6---6.8) 0.57
5minaftercuffischemia
BIS-L 49(25---74) 47(17---68) 0.42
BIS-R 47(24---65) 49(18---67) 0.29
CVI-L 1.4(0.8---9.2) 1.4(0.8---5.7) 0.95
CVI-R 1.4(0.8---8.1) 1.5(0.7---3.6) 0.39
5minafterskinincision
BIS-L 46(23---68) 45(24---67) 0.53
BIS-R 47(23---68) 46(26---67) 0.83
CVI-L 1.5(0.7---9.5) 1.4(0.6---4.5) 0.91
CVI-R 1.4(0.6---9.8) 1.6(0.6---4.5) 0.63
5minafterunlockingcuffischemia
BIS-L 47(29---70) 46(20---61) 0.30
BIS-R 46(31---76) 45(18---61) 0.32
CVI-L 1.5(0.7---9.36) 1.6(0.6---4.9) 0.43
CVI-R 1.4(0.7---9.7) 1.4(0.6---4.7) 0.60
Endofsurgery
BIS-L 52(32---82) 51(32---83) 0.67
BIS-R 52(25---82) 51(33---79) 0.76
CVI-L 1.6(0.7---7.4) 1.6(0.8---7.9) 0.72
CVI-R 1.7(0.7---7.8) 1.6(0.9---7.0) 0.75
Patientrespondtooralcommandandtrachealtuberemoved
BIS-L 81(42---94) 83(36---95) 0.23
BIS-R 80(46---97) 83(36---95) 0.08
CVI-L 4.2(1.1---9.5) 3.9(1.5---9.2) 0.49
CVI-R 4.1(1.2---9.4) 3.9(1.6---9.6) 0.98
Dataexpressedasmedianand(range).
BIS-R,rightbispectralindex;BIS-L,leftbispectralindex;CVI-L,leftcompositevariableindex;CVI-R,rightcompositevariableindex.
Results
Participantflow
One hundred and sixteen patients were assessed for eli-gibilityafter excluding, in accordance withthe exclusion criteria,22patients.Ofthese116,9didnotagreeto par-ticipateinthestudy;and13hadcontraindicationsrelated tomedicaldisease.So,atotalof94patientswereincluded. In47patients,thefemoralcatheterwasusedpriortothe surgery;theseformedthePreoperativegroup.Incontrast, 47 patients had the femoral catheter usedat the end of surgery;theyformedthePostoperativegroup(Fig.2).
There were no differences in patient characteristics, surgeryand recovery time between the groups (Table 1). Neitherwerethereanydifferencesinthebiochemical deter-minations.
Outcomesandestimation
Significantlylessfentanylandsevofluranewereused intra-operatively in the Preoperative group (Table 1). The
116 patients were assessed for eligibility
22 patients were no eligible:
- 5 expected difficult airway
management
- 2 neurologic disease
- 2 patients with renal dysfunction
- 4 patients with SAOS and home
CPAP
- 9 patients didn’t accept to
participate
94 underwent randomization
47 recieved postoperative
mepivacaine were included in
intention to treat analysis
47 recieved preopetrative
mepivacaine were included in
intentiontotreatanalysis
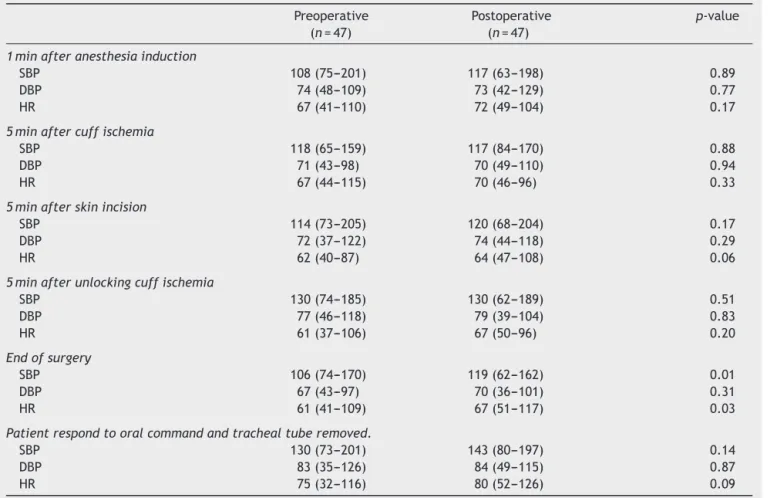
Table3 Hemodynamicvalues.
Preoperative (n=47)
Postoperative (n=47)
p-value
1minafteranesthesiainduction
SBP 108(75---201) 117(63---198) 0.89
DBP 74(48---109) 73(42---129) 0.77
HR 67(41---110) 72(49---104) 0.17
5minaftercuffischemia
SBP 118(65---159) 117(84---170) 0.88
DBP 71(43---98) 70(49---110) 0.94
HR 67(44---115) 70(46---96) 0.33
5minafterskinincision
SBP 114(73---205) 120(68---204) 0.17
DBP 72(37---122) 74(44---118) 0.29
HR 62(40---87) 64(47---108) 0.06
5minafterunlockingcuffischemia
SBP 130(74---185) 130(62---189) 0.51
DBP 77(46---118) 79(39---104) 0.83
HR 61(37---106) 67(50---96) 0.20
Endofsurgery
SBP 106(74---170) 119(62---162) 0.01
DBP 67(43---97) 70(36---101) 0.31
HR 61(41---109) 67(51---117) 0.03
Patientrespondtooralcommandandtrachealtuberemoved.
SBP 130(73---201) 143(80---197) 0.14
DBP 83(35---126) 84(49---115) 0.87
HR 75(32---116) 80(52---126) 0.09
Dataexpressedasmedianand(range).
SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HR,heartrate.
hemodynamicandBISvaluesregisteredduringsurgerywere similarinthe2groups(Tables2and3).Therewereno dif-ferencesbetweenthegroupsinanyofthemeasuredVNRS valuesor inmorphineconsumption(Table4).Peroperative bleeding and the percentage of patients transfused were similar.
Discussion
In agreement with expectations, a preoperative femoral blockwith20mLofmepivacaine2%reducedsevofluraneand fentanylconsumptioninpatientsundergoingTKA.This intu-itiveresultconfirmsthatthefemoralblockhadananalgesic effectandreducednociceptionstressduringsurgery. Nev-ertheless,theonlyprevious publishedstudy thatexplored the influence of femoral blockade on anesthesia require-ments,inpatientsundergoinganendoscopicpatellartendon anterior cruciate ligament reconstruction, found no dif-ferences in opioid consumption. However, the lack of a hemodynamicmanagementprotocollimitsthevalueofthat study.7Incontrast,peridurallidocaine2%hasbeen success-fulinreducingsevofluranerequirementsandalsoleadstoa reductioninstresshormones.10Astudycomparingepidural administrationofsaline,ropivacaine0.2%andropivacaine 1%foundagreaterreductionofend-tidalsevofluraneinthe
Table 4 Postoperative VNRS values and morphine consumption.
Preoperative (n=47)
Postoperative (n=47)
p-value
PostoperativeVNRS
PACU arrival
4(0---10) 3(0---10) 0.74
10min 3(0---8) 3(0---9) 0.68
20min 3(0---8) 2(0---7) 0.55
30min 3(0---8) 2(0---6) 0.18
1h 2(0---8) 2(0---5) 0.11
4h 2(0---7) 2(0---4) 0.35
VNRS≥8
atarrival
7(15%) 5(11%) 0.38
WardVNRS
24h 2(0---7) 2.5(0---7) 0.49
48h 3(0---8) 3(0---7) 0.27
72h 2(0---6) 3(0---9) 0.69
Postoperativemorphineconsumption(mg)
PACU 3(0---12) 3(0---12) 0.59
24h (PACU included)
4(0---59) 4(0---39.5) 0.96
48h 3(0---44) 3(0---48) 0.66
72h 0(0---10) 0(0---4) 0.34
Total 9(2---73) 8(0---63) 0.46
Dataexpressedasmedianand(range).
VNRS,verbalnumericratingscale;PACU,postanesthesiacare unit.
betweenthedecreaseininflammatorymediatorsand anal-gesicrequirements,asdidotherauthors.18Theadditionofa sciaticnerveblocktoacontinuousfemoralnerveblockhas beendemonstratedtobemoreeffectiveatreducing poste-riorandanteriorkneepainforupto8h,butnobeyondthat periodoftime.Therefore, thatwould notinfluence anal-gesicrequirementsontheward.19Wedidnotaddthesciatic nerveblock, because theaim of this study was to exam-inetheanalgesicrequirementsupto72hpostoperatively.A randomizedstudycomparingasinglefemoralblockin addi-tiontoaspinalanesthesiabeforeorafterkneereplacement surgery5 found no significant difference in morphine con-sumptionbetween groups.Barreveld andcoworkers,6 ina systematicreview, documenteda reduction of postopera-tivepainwhena peripheralnerveblock wascomparedto placebo or PCA; but the timing of the block,pre or post incision,didnotappeartobeofclinicalsignificance.In addi-tion,theyfoundpreventiveanalgesiaactionbyintravenous administrationof lidocaine, questioning the net effectof localanestheticonthenerveblockade.6Anothersystematic reviewofperipheralnerveblockadefoundlimitedevidence ofapositiveeffectofpreemptiveanalgesia.20
Inourstudy,theBISvaluesweresimilarinthe2groups, asexpectedinrelationtothemethodologyusedinthestudy. Nevertheless,nodifferenceswerefoundbetweenrightand leftBISvalues.ThedevelopmentoftheCVIisbasedonthe variabilityofBISandfacialEMG,andincreasesduring inad-equateanesthesiawith high-intensitynociceptivestimuli.
This indexhelpstoidentifyinadequatelevelsofanalgesia withacceptablesensitivityandspecificity.12Inourstudy,CVI valuesdidnotdifferentiatethegroupwithhigheropioid con-sumptionduringsurgery,inagreementtoDincklageetal.21 whofoundnopredictivepositiveornegativeresponseofCVI toskinincisionorlaryngealmaskinsertion.
Thelimitationsofthisstudyincludethatthethree anes-thesiologistsinchargeofintraoperativemanagementwere notblindedtothegroups;buttheanestheticmanagement protocolwasdefinedtousesevofluraneandfentanyl accord-ingtostrictrules.Incontrast,BISandhemodynamicswere similarinthe2groups,andalsotherewerenodifferences inthebiochemicaldeterminationsduringthesurgical proce-dure(datanotshown).Otherwise,surgeonsandnurseswere blindedtotheanestheticmanagement,whichconfirmsthe valueofthedataobtainedinthestudy.
Weconcludethatapreoperativefemoralblockadeis use-fulindecreasinganestheticrequirementsduringthesurgical procedurebutdoesnothaveotherbeneficialeffectsin post-operativeanalgesiccontrol.
Funding
FinancialsourceswereprovidedbytheAnesthesia Depart-ment.AspectMedicalSystemInc.Natick,MAprovidedthe BilateralBISelectrodesforBISVistamonitor.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Vielgut I, Kastner N, Pichler K, et al. Application and sur-gical technique of total knee arthroplasties: a systematic comparative analysis using worldwide registers. Int Orthop. 2013;37:1465---9.
2.MacfarlaneAJ,PrasadGA,ChanVW,etal.Doesregional anes-thesiaimproveoutcomeaftertotalkneearthroplasty?Orthop RelatRes.2009;467:2379---402.
3.KadicL,BoonstraMC,MalefijtMC.Continuousfemoralnerve blockaftertotalkneearthroplasty?ActaAnaesthesiolScand. 2009;53:914---20.
4.ChanEY,FransenM,SathappanS,etal.Comparingtheanalgesia effectsofsingle-injectionandcontinuousfemoralnerveblocks withpatientcontrolledanalgesiaaftertotalkneearthroplasty. JArthroplasty.2013;28:608---13.
5.ChanMH,ChenWH,TungYW, etal.Single-injectionfemoral nerveblocklackspreemptiveeffectonpostoperativepainand morphineconsumptionintotalkneearthroplasty.Acta Anaes-thesiolTaiwan.2012;50:54---8.
6.Barreveld A, Witte J, Chahal H, et al. Preventive analgesia bylocalanesthetics: thereduction of postoperativepainby peripheralnerveblocksandintravenousdrugs.AnesthAnalg. 2013;116:1141---61.
7.MatavaMJ,PrickettWD,KhodamoradiS,etal.Femoralnerve blockade as a preemptive anesthetic in patients undergoing anteriorcruciateligamentreconstruction:aprospective, ran-domized,double-blinded,placebo-controlledstudy.AmJSports Med.2009;37:78---86.
concentrationsandbispectralindexvaluesatthreeclinicalend points.JClinAnesth.2006;18:409---14.
9.ZhangJ,ZhangW,LiB.Theeffectofepiduralanesthesiawith differentconcentrationsofropivacaineonsevoflurane require-ments.AnesthAnalg.2007;104:984---6.
10.ShonoA,SakuraS,SaitoY,etal.Comparisonof1%and2% lido-caineepiduralanaesthesiacombinedwithsevofluranegeneral anaesthesiautilizingaconstantbispectralindex.BrJAnaesth. 2003;91:825---9.
11.Lavand’homme P, De Kock M, Waterloos H. Intraoperative epiduralanalgesiacombinedwithketamineprovideseffective preventive analgesia in patients undergoing major digestive surgery.Anesthesiology.2005;103:813---20.
12.EllerkmannRK,GrassA,HoeftA, etal. Theresponseofthe composite variability index to a standardized noxious stim-ulus during propofol-remifentanil anesthesia. Anesth Analg. 2013;116:580---8.
13.Ishiyama T, Kashimoto S, Oguchi T, et al. Epidural ropiva-caine anesthesia decreases the bispectral index during the awakephaseandsevofluranegeneralanesthesia.AnesthAnalg. 2005;100:728---32.
14.HampT, KrammelM, WeberU, et al. Theeffectof a bolus doseofintravenouslidocaineontheminimumalveolar concen-tration of sevoflurane: a prospective, randomized, double-blinded, placebo-controlled trial. Anesth Analg. 2013;117: 323---8.
15.Lavand’homme P. From preemptive to preventive analgesia: timetoreconsidertheroleofperioperativeperipheralnerve blocks?RegAnesthPainMed.2011;36:4---6.
16.Chan EY,FransenM, ParkerDA, etal. Femoralnerve blocks foracutepostoperativepainafterkneereplacementsurgery. CochraneDatabaseSystRev.2014;13:5.
17.MartinF,MartinezV,MazoitJX,etal.Antiinflammatoryeffect ofperipheralnerveblocksafterkneesurgery:clinicaland bio-logicsevaluation.Anesthesiology.2008;109:484---90.
18.CarvalhoB,AleshiP,HorstmanDJ,etal.Effectofapreemptive femoralnerve blockoncytokine releaseand hyperalgesiain experimentallyinflamedskinofhumanvolunteers.RegAnesth PainMed.2010;35:514---9.
19.AbdallahFW,ChanVWS,GandhiR,etal.Theanalgesiceffectsof proximal,distal,ornosciaticnerveblockonposteriorkneepain aftertotalkneearthroplasty.adouble-blindplacebo-controlled randomizedtrial.Anesthesiology.2014;121:1302---10.
20.MøinicheS,KehletH,DahlJB.Aqualitativeandquantitative systematic reviewofpreemptive analgesiafor postoperative pain relief: the role of timing of analgesia. Anesthesiology. 2002;96:725---41.