www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Vestibular
migraine:
comparative
analysis
between
diagnostic
criteria
夽
Márcio
Cavalcante
Salmito
a,∗,
Lígia
Oliveira
Gonc
¸alves
Morganti
a,
Bruno
Higa
Nakao
a,
Juliana
Caminha
Simões
a,
Juliana
Antoniolli
Duarte
a,
Fernando
Freitas
Gananc
¸a
baUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
bOtoneurologyOutpatientClinic,DepartmentofOtorhinolaryngologyandHeadandNeckSurgery,UniversidadeFederaldeSão
Paulo(UNIFESP),SãoPaulo,SP,Brazil
Received26February2014;accepted4October2014 Availableonline21July2015
KEYWORDS Migrainedisorders; Vertigo;
Dizziness;
Diagnostictechniques andprocedures
Abstract
Introduction:Thereisastrongassociationbetweenvertigoandmigraine.Vestibularmigraine (VM)wasdescribedin1999,anddiagnosticcriteriawereproposedin2001andrevisedin2012.
Objective: TocomparethediagnosticcriteriaforVMproposedin2001with2012criteriawith respecttotheirdiagnosticpowerandtherapeuticeffectofVMprophylaxis.
Methods:ClinicalchartreviewofpatientsattendedtoinaVMclinic.
Results:The2012criteriamadethediagnosismorespecific,restrictingthediagnosisofVMto asmallernumberofpatients,suchthat87.7%ofpatientsmet2001criteriaand77.8%met2012 criteria.ProphylaxisforVMwaseffectivebothforpatientsdiagnosedbyeithersetofcriteria andforthosewhodidnotmeetanyofthecriteria.
Conclusions: The2012diagnosticcriteriaforVMlimitedthediagnosisofthediseasetoasmaller numberofpatients,mainlybecauseofthetype,intensity,anddurationofdizziness.Patients diagnosedwithmigraineandassociateddizzinessdemonstratedimprovementafterprophylactic treatmentofVM,evenwhentheydidnotmeetdiagnosticcriteria.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:SalmitoMC,MorgantiLOG,NakaoBH,SimõesJC,DuarteJA,Gananc¸aFF.Vestibularmigraine:comparative
analysisbetweendiagnosticcriteria.BrazJOtorhinolaryngol.2015;81:485---90.
∗Correspondingauthor.
E-mail:[email protected](M.C.Salmito).
http://dx.doi.org/10.1016/j.bjorl.2015.07.007
PALAVRAS-CHAVE Transtornosde enxaqueca; Vertigem; Tontura; Diagnóstico
Migrâneavestibular:análisecomparativaentrecritériosdiagnósticos
Resumo
Introduc¸ão:Háforteassociac¸ãoentrevertigemeenxaqueca.Amigrâneavestibular(MV)foi descritaem1999ecritériosdiagnósticosforampropostosem2001erevisadosem2012.
Objetivo:Comparar os critérios diagnósticos para MV propostos em 2001 com os de 2012, atravésdeseupoderdiagnósticoeefeitoterapêuticodaprofilaxiadaMV.
Método: RevisãodeprontuáriosdepacientesatendidosemumaclínicadeMV.
Resultados: Oscritériosde2012tornaramodiagnósticomaisespecífico,restringindoaMVaum númeromenordepacientes,sendoque87,7%dospacientespreencheramoscritériosde2001e 77,8%preencheramoscritériosde2012.OtratamentoprofiláticoparaMVfoieficaztantopara pacientesdiagnosticadosporalgumdoscritériosquantoparaaquelesquenãoseenquadravam emqualquercritério.
Conclusões:Oscritériosdiagnósticosde2012paraMVrestringiramodiagnósticodadoenc¸apara ummenornúmerodepacientes,principalmenteporcausadotipodetontura,asuaintensidade edurac¸ão.Pacientescomenxaquecadiagnosticadaetonturaassociadaapresentarammelhora apósotratamentoprofiláticodaMVmesmoquandonãopreenchemcritériosdiagnósticos. ©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Dizzinessis one ofthe mostcommon complaintsin medi-calpractice,especiallyinthegeriatricagegroup,withan incidenceofupto30% peryear.1 Despitetheclinical pre-sentation,whichoftenmanifestsitselfvaguely,andthefact thatmanydoctorsstillfeelinsecureinthemanagementof patientswithdizziness, itispossibletoreachan accurate diagnosisinmostcases.2
Vestibular disorders are the most prevalent causes of dizziness.Among them,themost commonare,in descen-ding order, benign paroxysmal positional vertigo (BPPV), endolymphatichydrops,andvestibularmigraine(VM).This latter condition represents more than 11% of the causes ofvestibulardiseases, present in about 1%of thegeneral population.2,3
Migraineisamultifactorialchronicdisease,commonin geneticallysusceptibleindividuals,4andcharacterizedbya throbbingunilateralheadacheassociatedwithphotophobia, phonophobia,nausea,andvomiting.5VMcanbeadisabling illness thataffects about 18% of women and6% of men,5 coursing with otoneurological symptoms such as vertigo, hearing loss, tinnitus, and aural fullness; during a crisis, many patients exhibit these symptoms in the absence of headache.5
Theassociationbetweenmigraineanddizzinesshasbeen knownfora longtimeand occursthreetimes moreoften than if it was caused only by chance.6 VM as a particu-larentity, however, wasonlyrecently described(in 1999) by Dieterich and Brandt,7 characterized by vertigo and migraineattacks.Todate,itsdefinitionisnotuniformamong authors. Diagnostic criteria (Table 1) were proposed by Neuhauserin20018andrevisedin2012bytheBárány Soci-etyandtheInternationalHeadacheSociety(IHD),3andwere includedinthethirdversionoftheInternational Classifica-tionofHeadacheDisorders(ICHD-3).9
ThetreatmentofVMinvolvestwosituations10:
1. Crisisofmigraine-associated vertigo:for thetreatment of dizziness spells, recommended drugs are the same used for other acute attacks of vertigo: meclizine or dimenhydrinate,forexample.
2. Intercrisisperiod:prophylacticdrugsareused.The indi-cation for prophylaxis is the intensity or frequency of symptoms, or even the patient’s will. To date, drugs usedforthispurposearethesameusedfornon-dizziness migraine prophylaxis: beta-blockers, antidepressants, and anticonvulsants. The choice of drug is based on the patient’s profile: hypertensive patients can use beta-blockers;anxiousanddepressivepatientscan use antidepressants, especially tricyclic depressants and venlafaxine;patientswithoutcomorbiditiesmayreceive anticonvulsants, especiallytopiramateandsodium val-proate.
Objective
Theaimofthisstudywastocomparethediagnosticcriteria for VM proposed by Neuhauser in 2001 against the crite-ria reviewed by the Bárány Society and the International HeadacheSociety in2012,withanevaluationof the diag-nosticpowerandthetherapeuticeffectofVMprophylaxis in patients seen at Vestibular Migraine Outpatient Clinic, UniversidadeFederaldeSãoPaulo(UNIFESP).
Methods
Table1 Diagnosticcriteriaforvestibularmigraineproposedby(1)Neuhauser,20018and(2)theBáránySocietyandthethird
InternationalClassificationofHeadacheDisorders(ICHD-3),2012.3,9
1.Neuhauser,2001 2.BáránySocietyandICHD-3,2012
Vestibularmigraine,defined Vestibularmigraine
A.Vestibularsymptomsatleastofmoderateintensity A.Atleastfiveepisodeswithvestibularsymptomsofmoderate orsevereintensity,lastingfrom5minto72h
B.Currentorpasthistoryofmigraine,accordingto InternationalHeadacheSocietycriteria
B.Currentorpasthistoryofmigrainewithorwithoutaura, accordingtoInternationalHeadacheSocietycriteria C.Oneofthefollowingmigrainesymptomsduringat
leasttwoattacksofvertigo:migraine,photophobia, phonophobia,visualorotherauras
C.Oneormoreofmigrainesymptomsinatleast50%of vestibularepisodes:
-headachewithatleasttwoofthefollowingfeatures: unilaterallocation,pulsatingquality,intensityofpain (moderatetosevere),worsenedbyphysicalactivity -photophobiaandphonophobia
-visualaura
D.Othercausesruledoutbyanappropriateresearch D.Cannotbebetteraccountedforbyanother vestibulardiseaseoradiagnosisoftheICHD-3
Comment:
Vestibularsymptomsincludespinningdizzinessor anothermovementorpositionillusion.Theymaybe spontaneousorpositional.Vestibularsymptomsare ‘‘moderate’’iftheyinterfere,butdonotprevent, dailyactivities,and‘‘marked’’ifthepatientis unabletocarryouthis/herdailyactivities
Probablevestibularmigraine Probablevestibularmigraine
A.Vestibularsymptomsofatleastmoderateintensity A.Atleastfiveepisodeswithvestibularsymptomsofmoderate orsevereintensitylastingfrom5minto72h
B.Oneofthefollowing:(a)Currentorpasthistoryof migraineaccordingto2004criteriaofthe
InternationalHeadacheSociety;(b)migraine symptomsduringvestibularsymptoms;(c)migraine precipitantsofvertigoinmorethan50%ofattacks: foodtriggers,sleepproblems,hormonalchanges;and (d)responsetoanti-migrainedrugsinmorethan50% ofattacks
B.OnlyoneofthecriteriaBandCforvestibularmigraineis fulfilled(historyofmigraineormigrainesymptomsduringthe episode)
C.Othercausesruledoutbyappropriateresearch C.Cannotbebetteraccountedforbyanothervestibular diseaseoradiagnosisoftheICHD-3
and Head and Neck Surgery, UNIFESP) since its inception from 2011 until June 2013. This study was approved by the Research Ethics Committee of UNIFESP, under code 19615313.13.5.0000.5505.
All clinical recordsof patients withVM wereincluded, andthefollowinginformationwastakenintoaccount:
• Epidemiologicaldata:name,gender,age,profession,and placeofbirth;
• Clinicalfeaturesofthedisease;
• Pastmedicalhistory;
• Resultsoftreatmentsevaluatedbyavisualanaloguescale (VAS).
The medical records of patients with other disorders causingdizzinessand/orheadacheandthosewithillegible recordsor withincompleteor divergent informationwere excluded.
The information obtained allowed for classification of patients according to the diagnostic criteria proposed in
2001and2012. Accordingtothesecriteria, patientswere classifiedashavingdefinitiveorprobableVM.
Patients were classified into subgroups to assess their improvement in symptoms (Table 2). A VAS was used for headacheanddizziness.EachpatientwasevaluatedbyVAS inthe pre-prophylaxis period andagain by VAS after pro-phylactic treatment with different drugs. The estimated treatment timeranged fromthreetosix months.Clinical improvement was determined by the difference between thesescores,termed‘‘gain.’’
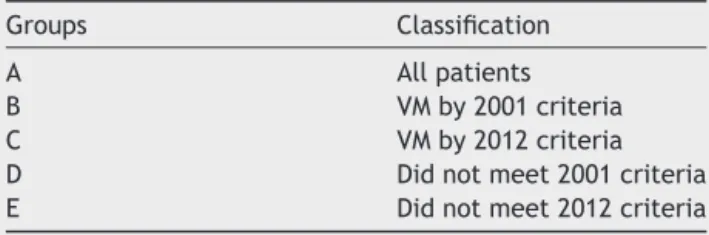
Table2 Classificationofpatientsusingthe2001and2012 criteriaforvestibularmigraine(VM)diagnosis.
Groups Classification
A Allpatients
B VMby2001criteria
C VMby2012criteria
Table3 Distributionofvestibularmigraineoutpatientsaccordingtoformerandcurrentdiagnosticcriteria.
Criteria 2001 2012 p-value
n % n %
Present 71 87.7% 63 77.8% 0.096
Absent 10 12.3% 18 22.2%
p-value <0.001 <0.001
Table4 Distributionofdrugsusedforvestibularmigraineprophylaxisaccordingtothegroup.
Group Amitriptyline Nortriptyline Fluoxetine Venlafaxine Topiramate Valproate Flunarizine Propranolol
A 22(27.2%) 2(2.5%) 3(3.7%) 4(4.9%) 18(22.2%) 7(8.6%) 13(16.0%) 12(14.8%) B 19(26.7%) 1(1.4%) 2(2.8%) 3(4.2%) 17(23.9%) 6(8.5%) 13(18.3%) 10(14.1%) C 17(26.9%) 1(1.6%) 2(3.2%) 2(3.2%) 13(20.6%) 5(7.9%) 13(20.6%) 10(15.8%) D 4(40%) 1(10%) 1(10%) 1(10%) 1(10%) 0 0 2(20%) E 7(38.9%) 1(5.6%) 1(5.6%) 2(11.1%) 4(22.2%) 1(5.6%) 0 2(11.1%)
The results were statistically analyzed, and Student’s
t and ANOVA tests were performed for quantitative variables. The significance level of 5% was adopted; therefore,values ofp≤0.05 wereconsidered statistically
significant.
Results
Ninety-fourclinical recordsfrom theVM outpatientclinic wereanalyzed,ofwhich81wereeligible.Thirteenclinical recordswithouttheinformationsoughtorpresenting incon-sistencies were excluded. Of the 81 patients, 76 (93.8%) werefemale.Theaverageagewas46years.
Among the 81 patients, 67 (82.7%) fully metthe diag-nosticcriteriaproposedin2001 fordefinitiveVM andfour
(4.9%)forprobableVM.Thus,71ofthe81patients(87.7%) metoneofthetwocriteria(Table3).Theothertenpatients hadmigraine(accordingtoICHD-3criteria)3andvestibular symptoms,butdidnotmeetthediagnosticcriteriaforVM, evenafterrulingoutothercausesofdizziness.
Regarding 2012 criteria, 60 (74.1%) were classified as definitive VM, and three(3.1%) as probable VM. Thus, 63 ofthe81patients(77.8%)metcriteriaforVM(Table3).
Ofthosetenpatientswhodidnotmeet2001diagnostic criteria, four(40%)hadnon-vertigodizziness(i.e.withno illusionofmovementorposition),andeight(80%)hadmild dizziness.
Of those 18 patients who did not meet 2012 diagnos-ticcriteria, fourpatients (22%)had non-vertigodizziness, eightpatients (44%) hadmild dizziness, and 13(72%) had
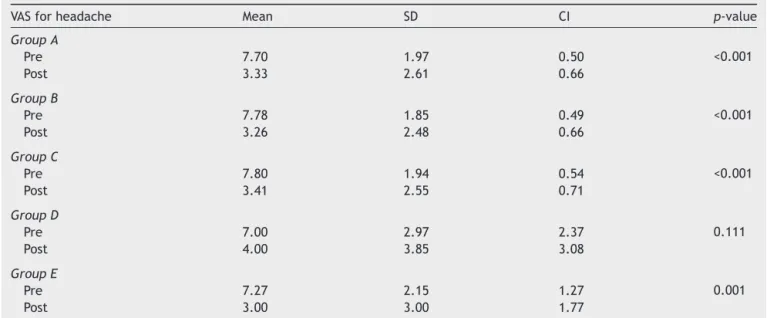
Table5 Meanscoresofthevisualanaloguescaleforheadachebysubgroupofpatients.
VASforheadache Mean SD CI p-value
GroupA
Pre 7.70 1.97 0.50 <0.001
Post 3.33 2.61 0.66
GroupB
Pre 7.78 1.85 0.49 <0.001
Post 3.26 2.48 0.66
GroupC
Pre 7.80 1.94 0.54 <0.001
Post 3.41 2.55 0.71
GroupD
Pre 7.00 2.97 2.37 0.111
Post 4.00 3.85 3.08
GroupE
Pre 7.27 2.15 1.27 0.001
Post 3.00 3.00 1.77
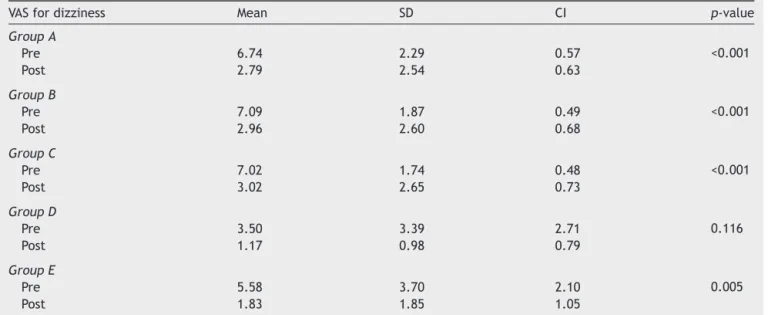
Table6 Meanscoresofthevisualanaloguescalefordizzinessbysubgroupofpatients.
VASfordizziness Mean SD CI p-value
GroupA
Pre 6.74 2.29 0.57 <0.001
Post 2.79 2.54 0.63
GroupB
Pre 7.09 1.87 0.49 <0.001
Post 2.96 2.60 0.68
GroupC
Pre 7.02 1.74 0.48 <0.001
Post 3.02 2.65 0.73
GroupD
Pre 3.50 3.39 2.71 0.116
Post 1.17 0.98 0.79
GroupE
Pre 5.58 3.70 2.10 0.005
Post 1.83 1.85 1.05
SD,standarddeviation;CI,confidenceinterval;GroupA,allpatients;GroupB,patientswhometoneofthe2001criteriaforvestibular migraine;GroupC,patientswhometoneofthe2012criteriavestibularmigraine;GroupD,patientswhodidnotmeetanyofoldcriteria; GroupE,patientswhodidnotmeetanyofthenewcriteria.
Table7 Meanofgainforvisualanaloguescalescoresforheadacheanddizzinessbysubgroupsofpatients.
VAS Mean SD CI p-value
Headache
GroupA −4.37 3.00 0.76 0.846
GroupB −4.52 2.91 0.77
GroupC −4.39 3.00 0.84
GroupD −3.00 3.79 3.04
GroupE −4.27 3.17 1.87
Dizziness
GroupA −3.95 3.27 0.81 0.794
GroupB −4.13 3.28 0.86
GroupC −4.00 3.19 0.88
GroupD −2.33 3.01 2.41
GroupE −3.75 3.74 2.12
SD,standarddeviation;CI,confidenceinterval;GroupA,allpatients;GroupB,patientswhometoneofthe2001criteriaforvestibular migraine;GroupC,patientswhometoneofthe2012criteriavestibularmigraine;GroupD,patientswhodidnotmeetanyofoldcriteria; GroupE,patientswhodidnotmeetanyofthenewcriteria.
symptoms of dizziness only for a few seconds. All ten patientswhodidnotmeet2001diagnosticcriteriaalsocould notreceiveadiagnosisofVMaccordingtocurrentcriteria (2012).
The treatment given included antidepressants, anti-convulsants, calcium channel inhibitors, and -blockers (Table 4). The medication was chosen considering the patient’sprofile,asrecommendedintheliterature.
VASscoresforpre-treatmentheadacherangedfrom2to 10,withameanof7to7.8betweengroups.Conversely,VAS scores for headache after prophylactic treatment ranged from0to9,withameanof3to4betweengroups(Table5). VASscores forpretreatment dizzinessrangedfrom0to 10,withameanof3.5to7.09betweengroups.VASscores fordizzinessafterprophylactictreatmentrangedfrom0to 8,withameanof1.17to3.02betweengroups(Table6).
Forheadache,themeanvaluesofgainrangedfrom−3.00 to−4.52.Fordizziness,themeanvaluesofgainrangedfrom −2.33 to−4.13. Whencompared betweengroups, in nei-ther case didgain values for headaches andfor dizziness demonstrateastatisticallysignificantdifference(Table7).
Discussion
VMisaheterogeneouscondition,usuallyepisodicandwith varyingsymptoms;however,thisdiseasecanbechronic,as canmigrainewithoutdizziness.11Thisisaprevalent condi-tioninwomeninthethirdandfourthdecadesoflife4;this wasalsoobservedintheresultsofthisstudy.
2012, in comparison with those of 2001. The diagnostic criteriaof2012wereproposedbytheBáránySocietyin con-junctionwiththeInternationalHeadacheSociety.Regarding this publication, it can be observed that the principal controversy occurred with respect to the sensitivity and specificity of the criteria, considering that very specific criteriawouldincreasethenumberoffalse-negativecases; however,verysensitivecriteriawouldincreasethenumber offalse-positivecases.3Consideringthissample,itwasclear thatthenewcriteriaaremorespecific,becausetheyrestrict thediagnosistoasmallernumberofpatients.
Thetypeofdizzinessanditsdurationandintensitywere themainculpritsforthisreductioninthenumberofpatients withadiagnosisof VMbythenewcriteria. Thediagnostic criteriaof2012restrictedthesecharacteristics;withtheir applicationinthisseries,eightof71patients(11.3%)were excluded.Thishasresultedinamorespecific,butless sen-sitive,diagnosis.
AlthoughdiagnosedwithmigrainebyICHD-3criteria,ten patients (12%) did not fit the classification of VM either by 2001 or 2012 criteria. Thus, these patients would no longerreceiveanetiologicdiagnosis.Infact,theywouldbe diagnosedwithavestibularsyndrometobeclarified. Never-theless,thesepatientswerenotexcludedfromthisclinic, becauseofotherdiagnostictips,forexample,astrong fam-ilyhistoryofmigraineorahistoryofmotionsickness;and, inaddition,theyshowedagoodtherapeuticresponse.
PatientsdiagnosedwithVMbythe2001,butnotby2012 criteria,respondedtodrugtherapy inasimilarmanner to patientsin groups Band C,witha statistically significant improvementseenintheVASscale.Thisindicatesthe pos-sibility that thesepatients areactually suffering VM, and therefore would beconsidered asfalse-negative cases by 2012diagnosticcriteria.
The use of diagnostic criteria for the determination of diseases has great scientific value, because this strat-egystandardizes diagnostics,mainly forscientific studies. However,their valuetomedicalpracticeshouldbeputin perspective,asthereareother, oftenvariables inthe art ofestablishingadiagnosisthatarenotquantifiable.Inthe presentsample, theresults ofthe prophylactictreatment ofpatientsassessed byVASshowednostatistically signifi-cantdifferencebetweenpost-treatmentscoresofpatients whometvs. thosewhodidnotmeet thediagnostic crite-ria.Therearetwopossibleexplanationsforthisfinding:the diagnosis of VM was correct--- even in cases that didnot fitthediagnosticcriteria;ortheprophylactictreatmentof VMimprovedthecasesofvestibulardisordersnotresulting frommigraine.However,noliteraturereportsofanti-vertigo
effectforantidepressantor anticonvulsantdrugscouldbe found. Additionalstudiesareneeded sothat amore thor-oughunderstandingofthisproblemisobtained.
Conclusions
The2012diagnosticcriteriaforVMrestrictthediagnosisof thisdiseasetoalessernumberofpatients.Thekeyfeatures responsibleforthisreductionwerethetypeofdizziness,and itsintensityandduration.
Patientsdiagnosedwithmigraineandwithcomplaintsof anassociateddizzinessshowedimprovementofdizziness(by VAS),afterdrugprophylaxisforVM.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LeeATH.Diagnosingthecauseofvertigo:apracticalapproach. HongKongMedJ.2012;18:327---32.
2.StruppM,BrandtT.Peripheralvestibulardisorders.CurrOpin Neurol.2013;26:81---9.
3.Lempert T, Olesen J, Furman J, Waterston J, Seemungal B, CareyJ,etal.Vestibularmigraine:diagnosticcriteria.JVestib Res.2012;22:167---72.
4.BolayH,BayazitYA,GündüzB,UgurAK,Akc¸aliD,AltunyayS, etal. Subclinical dysfunction ofcochlea and cochlear effer-entsinmigraine:anotoacousticemissionstudy.Cephalalgia. 2008;28:309---17.
5.Dash AK, Panda N, Khandelwal G, Lal V, Mann SS. Migraine andaudiovestibulardysfunction: isthereacorrelation?AmJ Otolaryngol.2008;29:295---9.
6.Jensen R, Stovner LJ. Epidemiology and comorbidity of headache.LancetNeurol.2008;7:354---61.
7.DieterichM,BrandtT.Episodicvertigorelatedtomigraine(90 cases):vestibularmigraine.JNeurol.1999;246:883---92. 8.NeuhauserH,LeopoldM,VonBrevernM,ArnoldG,LempertT.
Theinterrelationsofmigraine,vertigo,andmigrainousvertigo. Neurology.2001;56:436---41.
9.Headache Classification Committee of the International Headache Society (IHS). The International Classification of HeadacheDisorders,3rdedition (betaversion).Cephalalgia. 2013;33:629808.
10.BisdorffAR.Managementofvestibularmigraine.TherAdv Neu-rolDisord.2011;4:183---91.