SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Are
diaphyseal
clavicular
fractures
still
treated
traditionally
in
a
non-surgical
way?
夽
Pedro
José
Labronici
a,∗,
Fernando
Claudino
dos
Santos
Filho
b,
Tales
Bregalda
Reis
b,
Robinson
Esteves
Santos
Pires
c,
Adriano
Fernando
Mendes
Junior
d,
Kodi
Edson
Kojima
eaUniversidadeFederalFluminense,Niterói,RJ,Brazil
bHospitalSantaTeresa,Servic¸odeOrtopediaeTraumatologia,Petrópolis,RJ,Brazil cUniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
dUniversidadeFederaldeJuizdeFora,HospitalUniversitário,JuizdeFora,MinasGerais,Brazil
eUniversidadedeSãoPaulo,FaculdadedeMedicina,InstitutodeOrtopediaeTraumatologia,GrupodeTraumaOrtopédico,SãoPaulo,SP,
Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4November2015 Accepted24March2016 Availableonline8July2017
Keywords:
Fractures,bonesurgery Fractures,boneradiography Clavicule/surgery
Clavicule/radiography Boneplates
a
b
s
t
r
a
c
t
Objective:To evaluate thedecision oforthopedics surgeonsregardingwhich casesthey wouldindicatesurgeryornon-surgicaltreatment.
Methods:20 imagesof radiographswith fracture inthemiddlethird ofthecollarbone (AO/OTA15-B)inanteroposteriorviewwereanalyzed,anddividedintofourgroups:group1– fracturetypeAO/OTA15-B1withoutdisplacement;group2–fracturetypeAO/OTA15-B1with displacement;group3–fracturetypeAO/OTA15-B2;group4–fracturetypeAO/OTA15-B3. Theevaluatorwasrequestedtoindicatethechoiceoftreatment,surgicalornon-surgical.
Results:Therewasnostrongcorrelationbetweentheamountofsurgicalindicationsand theworkingexperienceorageofthemedicalevaluator.Itwasobservedthattheaverageof surgicalindicationsinthetotalsamplewas52%.Whenindicationswerestudiedindifferent areasofBrazil,therewasnosignificantdifferenceamongthem.NopatternfortheBrazilian regionsstudiedwasobservedinthecaseanalysis.Evenwithinagroup(casesofthesame complexity),nospecificpatternofsurgicalindicationwasobserved.
Conclusion:No association between surgical indication and the length of professional experiencewasfound.TheSouthernandSoutheasternregionswerethosethatmost rec-ommendedsurgeriesingroups2,3,and4.Innoregionthesamelevelofsurgicalindication forcasesofthesamecomplexityratewaskept.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalSantaTeresa,Petrópolis,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](P.J.Labronici).
http://dx.doi.org/10.1016/j.rboe.2017.06.012
Fraturas
da
diáfise
da
clavícula
ainda
são
tratadas
tradicionalmente,
de
forma
não
cirúrgica?
Palavras-chave:
Fraturasósseas/cirurgia Fraturasósseas/radiografia Clavícula/cirurgia Clavícula/radiografia Placasósseas
r
e
s
u
m
o
Objetivo:Avaliaradecisãodecirurgiõesortopédicossobreemquecasosindicariamacirurgia outratariamnãocirurgicamente.
Métodos: Foramanalisadas20 imagensde radiografiascomfraturadoterc¸o médioda clavícula(AO/OTA15-B)emincidênciaanteroposterior,queforamdivididasemquatro gru-pos:1–fraturadotipoAO/OTA15-B1semdesvio;2–fraturadotipoAO/OTA15-B1com desvio;3–fraturadotipoAO/OTA15-B2;4–fraturadotipoAO/OTA15-B3.Aoavaliador,foi solicitadoqueindicasseotipodetratamento:cirúrgicoounãocirúrgico.
Resultados:Nãohouvecorrelac¸ãoforteentreaquantidadedeindicac¸õescirúrgicaseotempo deatuac¸ãodomédicoavaliadorousuaidade.Verificou-sequeamédiadeindicac¸ãode cirurgiasnototaldaamostrafoide52%.Quandoestudadasasindicac¸õespordiferentes regiõesdoBrasil,nãohouvediferenc¸asignificativa.Nãofoiverificadoqualquerpadrãopara asregiõesbrasileirasnaanáliseporcaso.Mesmodentrodeumgrupo(casosdemesma complexidade),nãofoiverificadoumpadrãoespecíficodeindicac¸ãocirúrgica.
Conclusão: Nãofoiverificadaassociac¸ãoentreaindicac¸ãocirúrgicaeotempodeatuac¸ão doprofissional.AsregiõesSuleSudestesãoasquemaisrecomendamacirurgiadosgrupos 2,3e4.Verificou-sequeemnenhumaregiãofoimantidoomesmoníveldeindicac¸ãode cirurgiasparacasosdomesmograudecomplexidade.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Claviclefracturesarecommoninjuriesandoccurin2.6%–4% ofadults.Theyaccountfor44%ofshouldergirdlefractures,1–3
as this is the thinnest region of the clavicle and is not protected by muscle tissue. Conservative treatment has beenrecommended; it presents lowratesof pseudoarthro-sis(lessthan1%ofcases).4,5 However,recentliteraturehas
shownnonunionratesabove15%andunsatisfactoryresults between23%and31%.6–9 Theseresultscanbeexplainedby
changesinfollow-up,improvementofdiagnostictechniques, changes in results criteria, and the increasing severity of fractures.10
Surgicaltreatmentisrecommendedincertainsituations, such as in cases with a high degree of displacement or withmorethan20mmshortening.11Withsurgicaltreatment,
pseudoarthrosisratesrangefrom2%to3%withtheuse of platesandfrom0%to10%withintramedullaryrods. Nonethe-less,therateofunsatisfactoryresultsstillrangesfrom5%to 36%.12–14
Severalrandomizedtrialscomparedresultsof conserva-tiveandsurgicaltreatment.8,15–19Xuetal.19andMcKeeetal.20
conductedameta-analysestodeterminethepreferred treat-ment.Theseauthorsfoundhighratesofpseudarthrosisand malunionafterconservativetreatment.
Thisstudy aimedtoevaluatethedecisionamong ortho-pedicsurgeons regardingwhich cases theywould perform surgeryortreatconservatively.Thehypotheseswere:
Hypothesis1. Toevaluatewhetherlessexperiencedsurgeons
indicatesurgeriesmorefrequently.
Hypothesis 2. Toevaluatewhetherthereisadifferencein
treatmentindicationindifferentregionsofBrazil.
Hypothesis3. Toevaluatewhetherdifferenttypesoffracture
influencetreatmentindication.
Material
and
methods
Acomputerprogramwas developed;it contained20 radio-graphsoffracturesofthemiddlethirdoftheclavicle(AO/OTA 15-B).Alltheimageswereofacutefracturesin anteroposte-riorview,andweredividedintofourgroups:1–AO/OTA15-B1 fractureswithoutdeviation;2–AO/OTA15-B1fractureswith deviation; 3–AO/OTA 15-B2 fractures;and 4–AO/OTA 15-B3fractures.Eachgroupcontainedfiverandomlydistributed images.Theevaluatorwasaskedtoindicateatypeof treat-ment,whetherconservativeorsurgical.Thesoftwareincluded onlyimagesoffracturesofthemiddlethirdoftheclaviclein patientsagedbetween18and60years.Imagesofpatientswith previous,exposed,orpathologicalfractureswereexcluded,as wellasthoseofpatientswithpreviousmorbidityaffectingthe upperlimb(includingthescapulargirdleandthepresenceof neurovascularinvolvement).Thisstudyclassifiedphysicians asexperiencedwhentheyhad≥20yearsofpractice,andas
newthosewith<20yearsofpractice.
Table1–Numberofparticipants,meanage,meantimeofprofessionalactivity,andgeneralpercentageofsurgical
indications,byregionofBrazil.
Region Numberof participants
Meanage (years)
Meantimeof professional activity(years)
Overallpercentage ofsurgery indications
Brazil 193 43 17.5 52
Mid-West 7 44 13 46
Northeast 19 46 21 48
North 6 41 14 43
Southeast 130 50 23 52
South 31 43 18 55
Source:AOtraumacourses,Brazil,2014.
Table2–Percentageofprofessionalswhoindicatethesurgery,stratifiedbytimeofprofessionalactivity.
Group Case Timeofprofessionalactivity
Upto2years 3–6years 7–10years 11–20years Over20years
1 1 9.1 0.0 4.5 1.7 6.0
2 0.0 4.5 0.0 1.7 1.5
3 13.6 0.0 4.5 15.0 7.5
4 18.2 0.0 4.5 18.3 13.4
5 9.1 13.6 4.5 8.3 9.0
2 1 40.9 50.0 50.0 63.3 59.7
2 90.9 100 95.5 100 95.5
3 68.2 63.6 77.3 66.7 80.6
4 86.4 54.5 86.4 65.0 76.1
5 100 90.9 95.5 93.3 97.0
3 1 77.3 68.2 68.2 73.3 82.1
2 27.3 9.1 4.5 23.3 23.9
3 4.5 4.5 0.0 1.7 0.0
4 95.5 95.5 90.9 96.7 95.5
5 36.4 27.3 27.3 31.7 37.3
4 1 86.4 95.5 90.9 90.0 92.5
2 68.2 40.9 45.5 58.3 56.7
3 86.4 90.9 86.4 83.3 88.1
4 77.3 59.1 77.3 78.3 86.6
5 86.4 54.5 63.6 61.7 71.6
Source:CoursesAOtraumaBrazil2014.
Tables1–3showthedescriptionofthe193evaluators,mean age,meantimeofprofessionalactivity,andoverallpercentage ofsurgicalindicationsbyregionofBrazil.
Results
Verificationofhypotheses
The authors investigated the possibility of a relationship betweenevaluators’ responses and their age, and between evaluators’responseandtheirprofessionalexperience.The research was based on two methodologies: (1) analysis of the Spearman correlation between the number of surgical indicationsfromanevaluatorandhis/herageand between the number ofsurgical indicationsfrom an evaluator and his/hertimeofprofessionalexperience;and(2)chi-squared testtoevaluatedthesignificantassociationbetweentheage groupandtheresponsetoeachquestion.Table4showsthe resultofthecorrelationanalysis;nostrongcorrelationwas observedbetweenthenumberofsurgicalindicationsandthe
52
Surgical indication (%)
46 48 43
52 55
Brazil
Mid-West Northeast North
Southeast South 0
20 40 60 80 100
Fig.1–Overallpercentageofsurgicalindicationsbyregion ofBrazil.
Source:AOtraumaBrazilcourses,2014.
evaluators’experienceorage.Thechi-squaredtestalsodid not present significantassociations betweenthe responses andagegroupinthe20assessments.
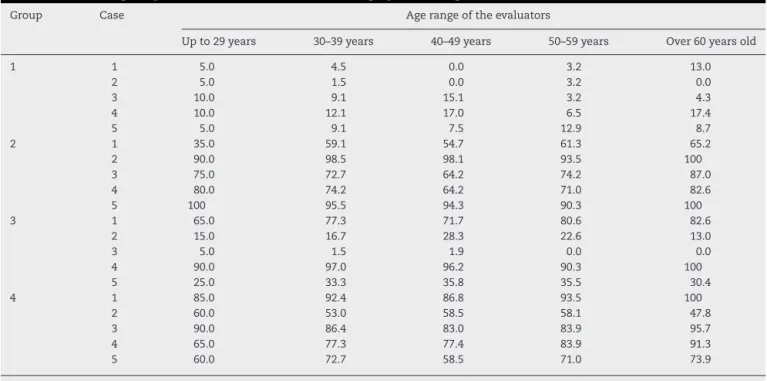
Table3–Percentageofprofessionalswhoindicatethesurgeryineachagebracketofevaluators.
Group Case Agerangeoftheevaluators
Upto29years 30–39years 40–49years 50–59years Over60yearsold
1 1 5.0 4.5 0.0 3.2 13.0
2 5.0 1.5 0.0 3.2 0.0
3 10.0 9.1 15.1 3.2 4.3
4 10.0 12.1 17.0 6.5 17.4
5 5.0 9.1 7.5 12.9 8.7
2 1 35.0 59.1 54.7 61.3 65.2
2 90.0 98.5 98.1 93.5 100
3 75.0 72.7 64.2 74.2 87.0
4 80.0 74.2 64.2 71.0 82.6
5 100 95.5 94.3 90.3 100
3 1 65.0 77.3 71.7 80.6 82.6
2 15.0 16.7 28.3 22.6 13.0
3 5.0 1.5 1.9 0.0 0.0
4 90.0 97.0 96.2 90.3 100
5 25.0 33.3 35.8 35.5 30.4
4 1 85.0 92.4 86.8 93.5 100
2 60.0 53.0 58.5 58.1 47.8
3 90.0 86.4 83.0 83.9 95.7
4 65.0 77.3 77.4 83.9 91.3
5 60.0 72.7 58.5 71.0 73.9
Source:CoursesAOtraumaBrazil2014.
Table4–Spearmancorrelationindexbetweennumber
ofsurgicalindicationsanddurationofsurgery,aswell
asbetweenthenumberofsurgicalindicationsandage.
Timeofoperation Age
Numberofindications forgroup1cases
−0.01 0.01
Numberofindications forgroup2cases
0.08 0.08
Numberofindications forgroup3cases
0.03 0.11
Numberofindications forgroup4cases
0.04 0.09
Numberofindications intotalcases
0.05 0.10
Source:CoursesAOtraumaBrazil2014.
52%.Nosignificantdifferenceswereobservedwhensurgical indicationswerestratifiedbydifferentregionsofBrazil.
Figs.2–5showtheincidenceofsurgeryindicationforthe differentfracturegroups.
Fig.6showsthatforbothglobalandregionalanalyses,the proportionofsurgicalrecommendation wasmuchlower in group1,asexpected.Casesfromgroup2receivedmore sur-gicalindicationsthanthoseofgroup3inallregionsofBrazil; onlyintheMid-WestandNorthregionstheydidnotsurpass thepercentageofsurgicalindicationsofgroup4(higher com-plexity).
Fig.7showsthat,inanoverallanalysis,higherpercentages ofsurgicalindicationwereobservedfromphysiciansfromthe SouthandSoutheastregionsforalltheradiographsofgroups 2,3,and4.
Inthecaseanalysis,nopatterncouldbeidentifiedforthe Brazilianregions.Evenwithinagroup(casesofthesame com-plexity),nospecificpatternofindicationwasverifiedinthe regionsofBrazil.
Discussion
Inthisstudy,theauthorsaimedtoanswerthequestion:are diaphysealclavicularfracturesstilltreatedtraditionallyina non-surgicalway?
Throughthreehypotheses,theauthorsdemonstratedthat surgical indication was uniform for both the less experi-encedandthemoreexperiencedevaluators.Despitethelarge socioeconomicdifferences,thedifferentregionsofthe coun-try presentedapatternforsurgicalindication.Through the radiographiccharacteristicsofthefracture,itwasnot possi-bletoestablishhowdeviationsize,angulation,andseverity candefinetreatment.
Generalliteraturesuggeststhatallclavicularfractureshave goodresultswithconservativetreatment.4,5 Reportspriorto
Hippocrateshadalreadyobservedthat“whentheclavicle frac-ture issimple and transverse,treatmentis easier; inturn, whenitisoblique,thetreatmentbecomesmoredifficult.”21
Recentstudieshaveshownthatsurgicaltreatmentispreferred inspecificcases(especiallydisplacedfractures).6,9 The
cur-rentliterature,whencomparingtreatments,hasreportedthat surgicaltreatmentreducesnonunionratesandsymptomatic malunion, leading tobetter functional outcomes and early returntoactivity.17,20,22Pieskeetal.23publishedtheresultsof
0
7 11
Surgical indication (%) 2 3 7 10 20
40 60 80 100
Brazil
Mid-West Northeast North
Southeast South
Fig.2–Overallpercentageofsurgicalindicationsforgroup1–AO/OTA15-B1fracturewithoutdeviation,byregionofBrazil. Representativeradiographofthegroup.
0 79
66 79
60
80 81
20 40 60 80 100
Surgical indication (%)
Brazil
Mid-West Northeast North
Southeast South
Fig.3–Overallpercentageofsurgicalindicationsforgroup2–AO/OTA15-B1fracturewithdeviation,byregionofBrazil. Representativeradiographofthegroup.
0 20
45 40 39 43 46 48
40 60 80 100
Surgical indication (%)
Brazil
Mid-West Northeast North
Southeast South
Fig.4–Overallpercentageofsurgicalindicationsforgroup3–AO/OTA15-B2fracture,byregionofBrazil.Representative radiographofthegroup.
etal.10showedthatsurgicaltreatmentwasrecommendedin
56%ofcasesandselectedin60%,probablyduetheircase selec-tion,withalargeproportionofdisplacedfractures.However, thestudyhasshownastrongtendencyforsurgicaltreatment tobecomemorewidelyused.
Thehypothesisraisedwaswhetherexperiencedevaluators wouldindicateconservativetreatmentmoreoftenthanthose lessexperienced,astherewasaconsensusinbothtextbooks andarticlesaboutthenotionthat“claviclefracturesare tra-ditionallytreatednon-surgically.”Moreover,lessexperienced
76
69 71 67
76 81
20
0 40 60 80 100
Surgical indication (%)
Brazil
Mid-West Northeast North
Southeast South
100 90 80 70 60 50 40 30 20 10 0
Surgical indication (%
)
Brazil
Group 1 Group 2 Group 3 Group 4
Mid West
Northeast North Southeast South
Fig.6–Percentageofsurgeonswhowouldindicatesurgery inBrazilforeachgroupofimages,definedaccordingtothe complexityinBrazilandbyregionofBrazil.
Source:AOtraumacourses,Brazil,2014.
evaluatorswould,intheory,indicatesurgeriesmoreoften,due tothedevelopmentofnewtechnologies,amongothercauses. Inthisstudy,thehypothesesofarelationshipbetweenthe evaluators’responsesandtheir ageaswellasbetweenthe evaluators’responseandtheirprofessionalexperiencewere rejected.Asshownintheresults,nosignificanttrendor asso-ciationwasobservedbetweenthemostexperiencedandthe youngest(inrelationtoage)orlessexperienced(relativeto timeinpractice).Theindicationforsurgicaltreatmentinthis studywas52%,whichisinagreementwithHeueretal.10The
percentageofprofessionalswhoindicatesurgery,the evalu-ators’timeofprofessionalexperience,andtheagegroupof evaluatorsareshowninTables2and3.
Anotherhypothesisraisedwaswhetherincertainregions ofthecountry,withmoresocioeconomicdifficulties, indica-tionforsurgerycouldvary.Thishypothesiswasalsorejected. Intheglobalanalysis,evenwithinthesamegroup(casesof thesamecomplexity),nospecificpatternofindicationwas verifiedinthe regionsofBrazil.Evaluatorsfrom the South andSoutheastregionsstoodoutforindicatingmore surger-ies.However,forthecasesofsimplefracture,theMid-West
region presentedthe highestpercentageofsurgical indica-tions(11%),whiletheNortheastandNorthregionspresented percentagesof3%and2%,respectively.TheMid-West,North, andNortheastregionspresentedpercentagesofsurgical indi-cationsbelowtheglobalproportion,exceptingroup1cases, whereMid-Westevaluatorsindicatedsurgerymorefrequently thantheglobalproportion(11%vs.7%,respectively).A rele-vantobservationwasthelackofastandardfortheBrazilian regionsintheanalysisofcasesofthesamecomplexity.Each regionalgroupofevaluatorswasexpectedtopresent percent-agesofsurgicalindicationswithoutmuchvariabilitywithina singlegroup,sincetheimagesfromthesamegrouppresented thesamedegreeofcomplexity.However,ahighvariabilityin surgicalindicationswasobservedwithinthesamecomplexity group.
Thenexthypothesiswaswhetherdifferenttypesof frac-tureswouldpresentdifferenttreatmentindications(whether thedegreeofcomplexityguidesthetypeoftreatment);that is,whetherthemorecomplexthefracture,thehigherthe sur-gicalindicationindex.
BothintheoverallsampleandintheBrazilianregions stud-ied,thehypothesiswasnotconfirmed,asintheglobalanalysis andintheregionsstudied,theproportionofsurgical recom-mendationwasmuchlower,asexpectedingroup1.Thecases ofgroup 2(simpledeviated fractures) receivedmore surgi-calindicationsthanthecasesofgroup3inallregions,and onlydidnotsurpass thepercentageofsurgicalindications ofgroup4(greater complexity)in theMid-West and North regions.
Thisstudyhassomelimitations,amongthemtheselection ofevaluators. Theauthors analyzedinformationfrom gen-eralorthopedicsurgeons,notthosespecializedintraumaorin shouldersurgery.Anotherlimitationwasthelackof informa-tionaboutgender,age,andcauseofthefracture,whichmight haveinfluenced the indication.However,this lackof infor-mationwasintentional,sincethepurposeofthestudywas toevaluatethetreatmentindicationsbasedonradiographic criteria.Anotherimportantpointthatneedstobetakeninto accountisthelownumberofevaluatorsfromtheMid-West andNorthregionsofthecountry.
100
90
80
70
60
50
40
30
20
10
0
Surgical indication (%
)
Brazil
Group 1 7 11
2 3 7 10
79
66 79
60 80 81
45 40 3943 46
48 76
697167 7681
5246 48 43
5255
Group 2 Group 3 Group 4 Global
Mid-West Northeast North Southeast South
Fig.7–Percentageofsurgeonswhoindicatesurgeryforeachgroupofimages,definedaccordingtothecomplexityinBrazil andbyregionofBrazil.
Conclusion
There was no association between surgicalindication and timeofprofessionalpractice.
TheSouthand Southeastregions were those that most recommendsurgeryforgroups2,3,and4.For group1,the evaluatorsfromthe Mid-Westregionwere thosewho most recommendsurgery.Furthermore,nocharacteristicpattern fortheBrazilianregionswasverifiedinthecaseanalysis.
Evenwithingroups(casesofthesamecomplexity),no spe-cificpatternofindicationwasverifiedperregionofBrazil.
Itwasobservedthatnoregionmaintainedthesamelevel ofsurgicalindicationforcaseswiththesamedegreeof com-plexity.
The authors believe that fractures of the middle third ofthe clavicle should be treated according to clinical and radiographiccriteriatoachievebestresults,contrary tothe recommendationfrommostarticlesandtextbooksthat frac-turesofthemiddlethirdoftheclaviclearetraditionallytreated non-surgically.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RobinsonCM.Fracturesoftheclavicleintheadult. Epidemiologyandclassification.JBoneJointSurgBr. 1998;80(3):476–84.
2. NordqvistA,PeterssonC.Theincidenceoffracturesofthe clavicle.ClinOrthopRelatRes.1994;(300):127–32.
3. PostacchiniF,GuminaS,DeSantisP,AlboF.Epidemiologyof claviclefractures.JShoulderElbowSurg.2002;11(5):452–6.
4. NeerCS2nd.Nonunionoftheclavicle.JAmMedAssoc. 1960;172:1006–11.
5. RoweCR.Anatlasofanatomyandtreatmentofmidclavicular fractures.ClinOrthopRelatRes.1968;58:29–42.
6. CanadianOrthopaedicTraumaSociety.Nonoperative treatmentcomparedwithplatefixationofdisplacedmidshaft clavicularfractures.Amulticenter,randomizedclinicaltrial.J BoneJointSurgAm.2007;89(1):1–10.
7. HillJM,McGuireMH,CrosbyLA.Closedtreatmentof displacedmiddle-thirdfracturesoftheclaviclegivespoor results.JBoneJointSurgBr.1997;79(4):537–9.
8. McKeeMD,PedersenEM,JonesC,StephenDJ,KrederHJ, SchemitschEH,etal.Deficitsfollowingnonoperative treatmentofdisplacedmidshaftclavicularfractures.JBone JointSurgAm.2006;88(1):35–40.
9. ZlowodzkiM,ZelleBA,ColePA,JerayK,McKeeMD, Evidence-BasedOrthopaedicTraumaWorkingGroup. Treatmentofacutemidshaftclaviclefractures:systematic
reviewof2144fractures:onbehalfoftheEvidence-Based OrthopaedicTraumaWorkingGroup.JOrthopTrauma. 2005;19(7):504–7.
10.HeuerHJ,BoykinRE,PetitCJ,HardtJ,MillettPJ.
Decision-makinginthetreatmentofdiaphysealclavicle fractures:isthereagreementamongsurgeons?Resultsofa surveyonsurgeons’treatmentpreferences.JShoulderElbow Surg.2014;23(2):e23–33.
11.McKeeMD.Claviclefracturesin2010:sling/swatheoropen reductionandinternalfixation?OrthopClinNorthAm. 2010;41(2):225–31.
12.KettlerM,SchiekerM,BraunsteinV,KönigM,MutschlerW. Flexibleintramedullarynailingforstabilizationofdisplaced midshaftclaviclefractures:techniqueandresultsin87 patients.ActaOrthop.2007;78(3):424–9.
13.MillettPJ,HurstJM,HoranMP,HawkinsRJ.Complicationsof claviclefracturestreatedwithintramedullaryfixation.J ShoulderElbowSurg.2011;20(1):86–91.
14.MuellerM,RanggerC,StriepensN,BurgerC.Minimally invasiveintramedullarynailingofmidshaftclavicular fracturesusingtitaniumelasticnails.JTrauma. 2008;64(6):1528–34.
15.NowakJ,HolgerssonM,LarssonS.Sequelaefromclavicular fracturesarecommon:aprospectivestudyof222patients. ActaOrthop.2005;76(4):496–502.
16.RehnCH,KirkegaardM,VibergB,LarsenMS.Operativeversus nonoperativetreatmentofdisplacedmidshaftclavicle fracturesinadults:asystematicreview.EurJOrthopSurg Traumatol.2014;24(7):1047–53.
17.RobinsonCM,GoudieEB,MurrayIR,JenkinsPJ,AhktarMA, ReadEO,etal.Openreductionandplatefixationversus nonoperativetreatmentfordisplacedmidshaftclavicular fractures:amulticenter,randomized,controlledtrial.JBone JointSurgAm.2013;95(17):1576–84.
18.VirtanenKJ,RemesV,PajarinenJ,SavolainenV,Björkenheim JM,PaavolaM.Slingcomparedwithplateosteosynthesisfor treatmentofdisplacedmidshaftclavicularfractures:a randomizedclinicaltrial.JBoneJointSurgAm. 2012;94(17):1546–53.
19.XuCP,LiX,CuiZ,DiaoXC,YuB.Shoulddisplacedmidshaft clavicularfracturesbetreatedsurgically?Ameta-analysis basedoncurrentevidence.EurJOrthopSurgTraumatol. 2013;23(6):621–9.
20.McKeeRC,WhelanDB,SchemitschEH,McKeeMD.Operative versusnonoperativecareofdisplacedmidshaftclavicular fractures:ameta-analysisofrandomizedclinicaltrials.JBone JointSurgAm.2012;94(8):675–84.
21.Hippocratesonthearticulations.400B.C.E.OpenOrthopJ. 2013;7Suppl.3M6:329–33.Availableat:http://classics. mit.edu/Hippocrates/artic.14.14.html.
22.SohnHS,KimWJ,ShonMS.Comparisonbetweenopen platingversusminimallyinvasiveplateosteosynthesisfor acutedisplacedclavicularshaftfractures.Injury.
2015;46(8):1577–84.