www.jped.com.br
ORIGINAL
ARTICLE
Risk
of
recurrence
after
a
first
unprovoked
seizure
in
children
夽
Catarina
Maia
a,∗,
Ana
Raquel
Moreira
b,
Tânia
Lopes
b,
Cecília
Martins
baCentroHospitalardeVilaNovadeGaia/Espinho,Servic¸odePediatria,VilaNovadeGaia,Portugal
bCentroHospitalardoMédioAve,Servic¸odePediatria,Famalicão,Portugal
Received17April2016;accepted11July2016 Availableonline7October2016
KEYWORDS
Seizures; Firstunprovoked seizure;
Recurrence; Child
Abstract
Objectives: Thisstudyaimedtoevaluatethefirstepisodeofunprovokedepilepticseizurein
childrenandassessrecurrenceriskfactors.
Methods: Thiswasaretrospectiveobservationalstudy,basedontheanalysisofmedicalrecords
ofpatientsadmittedbetween2003and2014,withfirstepilepticseizure,atthepediatricservice
ofasecondaryhospital.ThedatawereanalyzedusingtheSPSS20.0program.
Results: Of the103patients, 52.4% wereboys. Themedian ageatthefirst seizurewas 59
(1---211)months.About93%ofchildrenweresubmittedtoanelectroencephalogramatthefirst
episodeand47%underwentneuroimagingassessment.Treatmentwithanantiepilepticdrugwas
startedin46%ofpatients.Therecurrenceratewas38%andofthese,80%hadthesecondseizure
withinsixmonths afterthefirstevent.Oftheassessedriskfactors,therewasastatistically
significantassociationbetweenseizureduringsleepandrecurrence(p=0.004),andbetween
remotesymptomaticetiologyseizureandoccurrenceofnewseizure(p=0.02).Thepresenceof
electroencephalogramabnormalitieswasalsoassociatedwiththeoccurrenceofnewseizures
(p=0.021).Noassociationwasfoundbetweenage,durationoftheseizure,andfamilyhistory
ofepilepsywithincreasedriskofrecurrence.
Conclusions: Mostchildrenwithafirstunprovokedepilepticseizurehadnorecurrences.Therisk
ofrecurrencewashigherinpatientswithseizureoccurringduringsleeporremotesymptomatic
onesandthosewithabnormalelectroencephalogramresults.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:MaiaC,MoreiraAR,LopesT,MartinsC.Riskofrecurrenceafterafirstunprovokedseizureinchildren.JPediatr (RioJ).2017;93:281---6.
∗Correspondingauthor.
E-mail:[email protected](C.Maia).
http://dx.doi.org/10.1016/j.jped.2016.07.001
PALAVRAS-CHAVE
Convulsão; Primeiracrisenão provocada; Recorrência; Crianc¸a
Riscoderecorrênciaapósumaprimeiracriseepiléticanãoprovocadaemidade
pediátrica
Resumo
Objetivos: Estetrabalhotevecomoobjetivosestudaroprimeiroepisódiodecriseepiléticanão
provocadaemidadepediátricaeavaliarosfatoresderiscoderecorrência.
Métodos: Estudo observacionalretrospectivo, baseado naanálisedosprocessos clínicos dos
pacientesinternadosentre2003e2014,numservic¸odepediatriadeum hospitaldenível2,
comprimeiracriseepilética.OsdadosforamtrabalhadoscomoprogramaSPSSStatistics20.0.
Resultados: Dos103 pacientes,52,4% erammeninos.A mediana daidadedaprimeira crise
foi59(1-211)meses.Cercade93%dascrianc¸asrealizarameletroencefalogramanoprimeiro
episódioe47%realizaramneuroimagem.Otratamentocomfármacoantiepiléticofoiinstituído
em46%dospacientes.Ataxaderecorrência foi38%e,destes,80%tiveramasegundacrise
nos6mesesseguintesapósoprimeiroevento.Dosfatoresderiscoestudadosverificou-seuma
relac¸ãoestatisticamentesignificativaentreacriseduranteosonoearecorrência(p=0,004),
assim como entreas crisesde etiologiasintomática remota e aocorrência denovas crises
(p=0,02).A presenc¸adeanormalidadesnoeletroencefalogramatambémesteveassociadaà
ocorrênciadenovascrises(p=0,021).Nãoseencontrourelac¸ãoentreidade,durac¸ãodacrise
ehistóriafamiliardeepilepsiacomriscoaumentadoderecorrência.
Conclusões: Amaioriadascrianc¸ascomumaprimeiracriseepiléticanãoprovocadanãoteve
recorrências.Oriscoderecorrênciafoisuperiornospacientescomcriseduranteosonooucrise
sintomáticaremotaenaquelescomeletroencefalogramaalterado.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Epilepticseizures areoneofthe mostcommon neurologi-calproblemsinchildren.Itisestimatedthatapproximately 50%ofchildrenandadolescentswhohaveafirstepileptic seizurewillhaveonerecurrence.1 Knowledgeofthe
natu-ralhistoryafterafirstunprovokedepilepticseizureandrisk
factorsfor recurrenceareessentialtoestablishtreatment
andfollow-upcriteria.Overtheyears,severalauthorshave
suggestedrecurrencepredictors,2---4suchasageatthefirst
seizure,gender, familyandperinatalhistory,seizure
char-acteristics,andelectroencephalogram(EEG)results,among
others.However,thestudiesarenotalwaysconsensualand
thosefoundinPortugalonthistopicarestillscarce.Pereira
etal.5evaluated200childrenwithafirstepisodeof
unpro-vokedepilepticseizureduringa15-yearperiod.According
totheirstudy,whichwascarriedoutinPortugal,30%ofthe
children developed epilepsy, with focal seizures and EEG
alterations being associated with increased risk of
recur-rence.Theseauthorsfoundnoassociationbetweenhistory
offebrileseizures,neonatalcomplications,andfamily
his-toryofepilepsywithincreasedriskofrecurrence.
The present study aimedto assess thefirst episode of
unprovokedepilepticseizureinpediatricpatients,aswell
astherecurrenceriskfactors.
Methods
Studydesignandpopulationsample
Thiswasaretrospectiveobservationalstudy,basedonthe assessment of medical records of patients admitted to a
secondary hospitalin Portugal betweenOctober 2003 and June 2014. This study included patients at the pediatric age range (<18 years) with a suspected first episode of epilepticseizure.Patientsyoungerthan28daysoflifeand thoseinwhomanacutecausativefactorfortheseizurewas identifiedwereexcluded.Childrenwithseizureswith symp-tomaticetiologyinwhomanacutecausativefactorwasnot identifiedwereincluded.
Studyprotocol
The definitions usedwere based onthe criteriaand clas-sifications published by the International League Against Epilepsy(ILAE),6aftersomeadjustments.Thediagnosis of
first unprovoked epileptic seizure was established by the
physicianwhotreatedthechild,consideringthedescribed
and/ordisplayedsignsandsymptoms.Theseizurewas
clas-sifiedasunprovokedwhenanacutecausativefactorwasnot
identifiedfortheseizure(e.g.,headtrauma,fever,
hypona-tremia,hypocalcemia,andtoxinexposure,amongothers).A
seizurewasconsideredasremotesymptomaticwhenthere
was no immediate cause, but the child had a prior
his-toryofneurologicalinjury,suchaschronicnon-progressive
encephalopathyorstroke,leadingtoastaticlesion.Itwas
notpossibletoretrospectivelydistinguishbetweenan
idio-pathicandacryptogenicseizureinallchildren.
Regarding the type of seizure, they were classified as
focal (which were differentiated into focal without
con-sciousnessalterations,focalwithconsciousnessalterations,
and focal with secondary generalization) or generalized
seizures (differentiated into absenceseizures, myoclonic,
clonic,tonic,tonic---clonic,andatonic seizures).Aseizure
Generalized Focal Undetermined
<5 minutes
5-15 minutes
>15 minutes 5.8%
29.1%
65.0%
37.0% 15.2%
47.8%
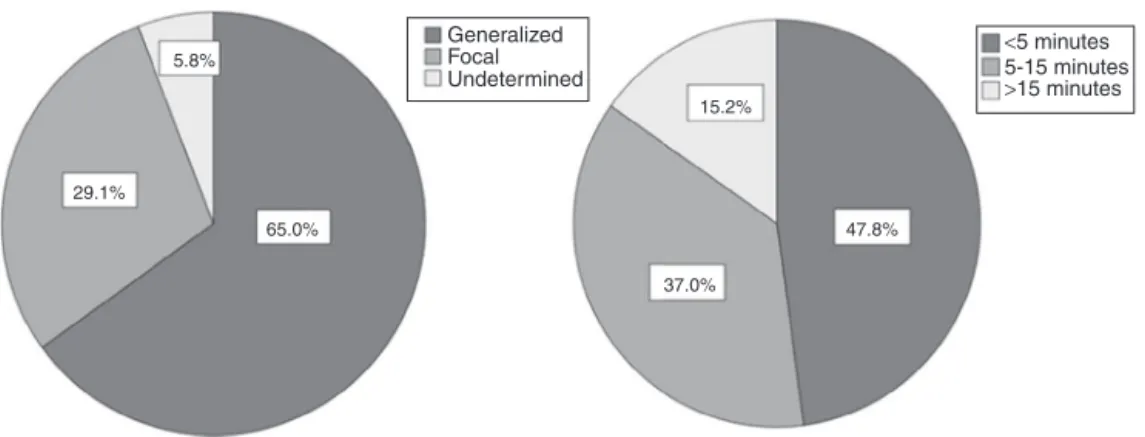
Figure1 Seizurecharacterizationandduration.
medicalrecords,itwasnotpossibletoestablishthe classi-ficationbetweenfocalandgeneralizedseizure.Recurrence wasdefined asan unprovokedseizure occurring over 24h afterthefirstevent.
Thestudywasapprovedbytheethicscommitteeofthe institution where it was conducted (Centro Hospitalar do Médio Ave). As this wasa retrospective study,it was not necessary toobtain a signed informedconsent formfrom thepatients’legalguardians.
Analyzedclinical,demographicandanalytical variables
Gender,ageat thefirstepilepticseizure,personal history (including information on prenatal and perinatal history, psychomotordevelopmentandhistoryoffebrileseizures), familyhistory(mainlyrelatedtohistoryofepilepsy,febrile seizures and cognitive delay), type of seizure, objective examination, complementary diagnostic tests, treatment, andfollow-upwereanalyzed.
Statisticalanalysis
Thechi-squaredtestforindependencewasusedfor compar-isonsbetweengroups,basedoncategoricalvariables.Where it wasnotpossible tousethe chi-squaredtest, the exact testresultswereused.Thet-testforindependentsamples wasusedtocomparetwogroupsbasedoncontinuous varia-bles.StatisticalanalysiswasperformedusingtheSPSS(IBM SPSS Statistics for Windows, version 20.0, USA). A type I errorprobability(˛)of0.05wasconsideredinallinferential
analyses.
Results
Populationsampledescription
Duringthestudyperiod,atotalof103patientswere admit-ted, aged 1 month to 18 years, diagnosed with a first episodeofunprovokedepilepticseizure.Ofthe103assessed patients, 52.4% were males. The median age at the first seizureepisodewas59(1---211)monthsandthemeanwas 74months;35%wereyoungerthan2yearsand25.2%older
than10years.Ofthesechildren,12(11.7%)hadahistoryof prematurity,five(4.9%)wereresuscitatedafterbirth,and 15(14.6%)had delayedpsychomotor developmentor cog-nitiveimpairment.Sevenpatients(6.8%)hadapriorbrain alterationandnine(8.7%)hadahistoryoffebrileseizures. Afamily history of epilepsywaspositive in 44% of cases. Approximately3.4%ofthepatientshadafamilyhistoryof febrileseizuresand7%hadfamilymemberswithcognitive delay.
Characteristicsofthefirstseizure
Theseizurewasclassifiedasremotesymptomaticinseven cases (one case of brain calcifications and chorioretinitis duetocongenitalinfectionbycytomegalovirus,twocasesof polymalformationsyndromes,twocasesofhypoxic-ischemic encephalopathy,onecaseofstrokeaftercardiacsurgeryin theperinatalperiod,andonecaseofmeningitis).Regarding symptomatology,theseizurewasgeneralizedin65%ofcases (mainlytonic-clonic),focalin29.1%(mainlyfocalwith con-sciousness alteration), and undetermined in 5.8% of the childrenandadolescents.Durationwaslessthan5minin48% ofpatientsandlongerthan15minin15%(Fig.1).
Approx-imately 25% of the children had their first seizure during
sleep.In5%ofchildren,theinitialpresentationwasstatus
epilepticusand30%hadmorethanoneseizurewithinthe
first24h.
Studyandtreatment
60
50
40
30
P
ercentage
20
10
0
0 6 12
Time (months)
18 24
Figure2 Timeuntilrecurrenceafterthefirstseizure.
Recurrencerateandrespectiveriskfactors
Ofthe103assessedpatients,17(threewithremote symp-tomaticetiology)werelosttofollow-upandthus,itwasnot possibletoevaluatetheirrecurrencerate.Oftheremaining 86cases,26werefollowedforoverfiveyears,35were fol-lowedbetweentwoandfiveyears,and25hadafollow-up period<2yearsatthetimeofthestudy.Therecurrencerate was38%and,ofthese,80%hadthesecondseizurewithinsix monthsafterthefirstevent.Onlyonechildhadthesecond seizuremorethanoneyearafterthefirstevent(Fig.2).
Of the assessed recurrence risk factors, there was a
statisticallysignificant association between seizure
occur-ring during sleep and the occurrence of new seizures
(p=0.004), as well as between remote symptomatic
eti-ology seizures and recurrence (p=0.020). The presence
of electroencephalogram abnormalities was also
associ-ated with the occurrence of new seizures (p=0.021). No
associationwasfoundbetweengender,age,pre-and
perina-talcomplications,duration,andtypeofseizure(generalized
vs.focal),personalhistoryoffebrileseizures,orfamily
his-toryofepilepsyandincreasedriskofrecurrence(Table1).
Discussion
Seizures are one of the most common neurological disor-ders in children. The first episode of epileptic seizure is always an anxiety-causingevent for parents andit is the health professional’s dutytoknow the bestapproachand recommendationstouseineachcase.
Studies of recurrence after a first unprovoked seizure haveshownpercentagesbetween33%and61%overamedian follow-upof 2years.2,3,7---9 Inthepresentstudy,the
recur-renceratewas38%,withahigherprobabilityofrecurrence
within the first months after the first seizure and very
low after the first year, which is consistent with the
lit-erature and with another study conducted in Portugal.5
Althoughfollow-updurationwasnotthesameforall
chil-dren,mostwerefollowed-upforover2years,whichappears
to indicate that the time interval without seizures after
the first epileptic seizure influences the risk of
recur-rence.
Shinnaretal.9andWinckleretal.10investigatedtherisk
factors associated with unprovoked seizure recurrence in
children.Accordingtotheseauthors,themeanageatfirst
seizurewas6years,whichisinagreementwiththeresultsof
thepresentstudy.Theageatthefirstseizurewasnot
associ-atedwithincreasedriskofrecurrenceinthepresentstudy,
whichisconsistentwiththeresultsbyWinckleretal.10
Regardingtheinfluenceoffamilyhistoryofepilepsyon
the recurrence risk, some studies in the literature have
foundapositiveassociation.3,10,11Thatwasnotobservedin
thepresentstudynorinthatbyPereiraetal.5
The studies developed in the 1980s onseizures
occur-ring in children reported a predominance of generalized
seizures,12,13 which isinaccordancewiththerecent study
byWinckler etal.10 andthepresentstudy.However,most
articlesandtherecentliteraturedescribeahighernumber
offocalseizures.14,15Thisdiscrepancycanbeexplainedby
differences in study samples or the fact thatthe present
Table1 Analysisofrecurrenceriskfactors.
Riskfactors Recurrence
n=33
Norecurrence
n=53
p
Femalegender 17(51.5%) 36(67.9%) NS
Age<2years 12(36.3%) 30(56.6%) NS
Prematurity 2(6%) 7(13%) NS
Remotesymptomaticetiology 4(12.1%) 0 0.02
Delayedpsychomotordevelopment 6(18.1%) 7(13.2%) NS
Partialseizure 10(30%) 9(17%) NS
Statusepilepticus 0 4(7.5%) NS
Durationofseizure>15min 3(9.1%) 11(20.8%) NS
Seizuresduringsleep 14(42.4%) 8(15.1%) 0.004
ParoxysmalactivityintheEEG 18(54.5%) 19(35.8%) 0.021
Personalhistoryoffebrileseizures 3(9.1%) 6(11.3%) NS
Familyhistoryofepilepsy 13(39.4%) 34(67.9%) NS
is a retrospective study, where the cases were assessed andrecordedbyseveralphysicians,whichcannotexcludea biasinthesemiologicalclassification(itisknownthatfocal motorseizuresareoftenclassifiedasgeneralizedseizures). Regardingtheinfluenceoftheseizuretypeonthe recur-rencerisk,WincklerandRotta2foundasix-foldhigherrisk
of new seizures if the first one wasfocal. Similar results
werereportedbyotherauthors.16 Incontrast,similarlyto
the present study, other studies3,10 found no association.
However,aspreviouslyexplained,thepossibilityofa
semi-ologicalclassificationbiascannotbediscarded;therefore,
theseresultshavetobeconfirmedbyprospectivestudies.
As previously reported, there was a predominance of
short-duration seizures and of those that occurred when
the child was wake. The recurrence risk in the present
studywashigherinseizuresthatoccurredduringsleep,as
described inother studies.9,17 According tothe literature,
thisassociation appearstobeindependentfromthe
asso-ciationofcertainepilepticsyndromeswithseizuresduring
sleep.18 Someauthorssuggestthatseizuresthatoccur
dur-ingsleepcannotbeidentifiedearlyand,thus,theexistence
ofotherseizurespriortotheonethatwasdetectedwould
explain the higher risk of recurrence in these children.4
Nonetheless,theexplanationforthisassociationisstill
con-troversial.
Over the years, several authors have mentioned the
importance of an EEG with epileptiform activity for the
riskofrecurrence.5,10,19,20Thepresentstudyconfirmedthe
increased risk of recurrence when the first EEG showed
paroxysmal activity.As the EEGis anoninvasive and
low-costtest,withanimportantroleintheassessmentofseizure
recurrence,theauthorssuggest thatitberequested after
thefirstunprovokedseizure.
As expected, thegroup of children withremote
symp-tomatic etiology (which included the three cases with
abnormalbrainMRI)showedagreaterriskofrecurrence.
It is known that antiepileptictreatment after the first
seizure reduces recurrencein the firsttwo years.21
How-ever,thelong-termevolutionofchildrentreatedafterthe
second episodeis similartothatof childrentreated after
thefirstseizure,1,21 andtreatment withantiepileptic (AE)
drugsdoes notreduce theriskofepilepsy.Therefore,and
takingintoaccountthatthetreatmentwithAEdrugsisnot
harmless,thelatterisgenerallyrecommendedonlyaftera
secondeventor,inspecialcases,afterthefirstseizure.In
thepresentstudy,inaccordancewiththerecommendations
intheliterature,22 antiepileptictherapy wasimplemented
afterthefirstseizure,afterdiscussionwithparents,onlyin
children withneurological deficits,when the EEGshowed
unequivocal epileptic activity or when neuroimaging
dis-closedthepresenceofastructuralabnormality.
This study has some limitations. One is related to the
loss of follow-up of some children after the first seizure.
Furthermore, as this was a retrospective study, in some
casesit wasnotpossible toverifysome demographicand
clinical data thatcould have influencedthe predictionof
recurrencerisk.Aspreviouslymentioned,semiological
clas-sification bias cannot be ruled out. Finally, the fact that
antiepileptictreatmentwasinstitutedinasignificant
pro-portionofchildrendoesnotallowforinferringwhatwould
haveoccurredifthesechildrenhadnotbeentreated.
How-ever,itallowsfortheassessmentofthenaturalhistoryand
riskfactorsforrecurrenceafterafirstepilepticseizurein
thepediatricpopulation,includingspecificcaseswith
treat-mentindicationafterthefirstseizure.
In conclusion, most children with a first unprovoked
epileptic seizure did not present recurrence; therefore,
itis important toreassure thechild/adolescent andtheir
parentsandtrytominimize,asmuchaspossible,the
anx-iety that these events generate in the family. The risk
of recurrence was significantly higher in patients with a
seizureoccurringduringsleeporremotesymptomatic
etiol-ogyseizureandinindividualswithanabnormalEEG.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Manjón-Cabeza RA. Primera crisis epiléptica. Protocolos de neurologia AEPED; 2008. Available from: www.aeped.es/ protocolos/[cited15.04.16].
2.WincklerMI,RottaNT.Prognosticfactorsforrecurrenceofafirst seizureduringchildhood.ArqNeuropsiquiatr.1997;55:749---56. 3.Scotoni AE, Guerreiro MM, De Abreu HJ. First epileptic cri-sis.Analysisofriskfactorsforrecurrence.ArqNeuropsiquiatr. 1999;57:392---400.
4.BergAT. Risk ofrecurrence afterafirst unprovoked seizure. Epilepsia.2008;49:13---8.
5.PereiraC,ResendeC,FinezaI,RobaloC.A15-yearfollow-upof firstunprovokedseizures:aprospectivestudyof200children. EpilepticDisord.2014;16:50---5.
6.ShorvonSD.Theetiologicclassificationofepilepsy.Epilepsia. 2011;52:1052---7.
7.ZupancML.Updateonepilepsyinpediatricpatients.MayoClin Proc.1996;71:899---916.
8.Hirtz D,AshwalS, BergA, Bettis D,CamfieldC,CamfieldP, etal.Practiceparameter:evaluatingafirstnonfebrileseizure inchildren:reportofthequalitystandardssubcommitteeofthe AmericanAcademyofNeurology,TheChildNeurologySociety, andTheAmericanEpilepsySociety.Neurology.2000;55:616---23. 9.ShinnarS,BergAT,MosheSL,O’DellC,AlemanyM,Newstein D, et al. The riskof seizure recurrence after a first unpro-voked afebrile seizure in childhood: an extended follow-up. Pediatrics.1996;98:216---25.
10.Winckler MI, Rotta NT. Clinical and electroencephalographic follow-up after a first unprovoked seizure. Pediatr Neurol. 2004;30:201---6.
11.MonettiVC,GranieriE,CasettaI,TolaMR,PaolinoE,Malagù S, et al. Risk factors for idiopathic generalized seizures: a population-basedcasecontrolstudyinCopparo,Italy.Epilepsia. 1995;36:224---9.
12.Cavazzuti GB. Epidemiology of different types of epilepsy in school age children of Modena, Italy.Epilepsia. 1980;21: 57---62.
13.LearyPM,Morris S.Recurrentseizuresinchildhood. Western Capeprofile.SAfrMedJ.1988;74:579---81.
14.Group CAROLE. Epilepsies and time to diagnosis. Descrip-tive results of the CAROLE survey. Rev Neurol (Paris). 2000;156:481---90.
15.Camfield P, Camfield C. Incidence, prevalence and aetiol-ogy of seizures and epilepsy in children. Epileptic Disord. 2015;17:117---23.
17.Ramos Lizana J, Cassinello Garciá E, Carrasco Marina LL, VázquezLópezM,MartínGonzálezM,Mu˜nozHoyosA.Seizure recurrence after a first unprovoked seizure in childhood: a prospectivestudy.Epilepsia.2000;41:1005---13.
18.GrispanZ,ShinnarS.Managementofpatientswithfirstseizure andearlyepilepsy.In:ShorvonS,GuerriniR,CookM,Lhatoo S,editors.Oxfordtextbookofepilepsyandepilepticseizures. Oxford:OxfordUniversityPress;2013.p.245.
19.Dlugos DJ. An EEG should not be obtained routinely after first unprovoked seizure in childhood. Neurology. 2000;55: 898---9.
20.Nicole-CarvalhoV,Henriques-SouzaAM.Conduta noprimeiro episódiodecriseconvulsiva.JPediatr(RioJ).2002;78:S14---8. 21.MarsonA,JacobyA,JohnsonA,KimL,GambleC,ChadwickD,
etal.Immediateversusdeferredantiepilepticdrugtreatment forearlyepilepsyandsingleseizures:arandomisedcontrolled trial.Lancet.2005;365:2007---13.