REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Robotic
prostatectomy:
the
anesthetist’s
view
for
robotic
urological
surgeries,
a
prospective
study
夽
,
夽夽
Menekse
Oksar
a,∗,
Ziya
Akbulut
b,
Hakan
Ocal
a,
Mevlana
Derya
Balbay
b,
Orhan
Kanbak
aaDepartmentofAnesthesiologyandReanimation,AnkaraAtaturkTrainingandResearchHospital,Ankara,Turkey bDepartmentofUrology,AnkaraAtaturkTrainingandResearchHospital,Ankara,Turkey
Received30July2013;accepted31October2013 Availableonline11December2013
KEYWORDS
Roboticsurgery; Prostatectomy; Urologicalsurgery
Abstract
Backgroundandobjectives: Although many featuresof roboticprostatectomyaresimilar to thoseofconventionallaparoscopicurologicalprocedures(suchaslaparoscopicprostatectomy), theprocedureisassociatedwithsomedrawbacks,whichincludelimitedintravenousaccess, relativelylongoperatingtime,deepTrendelenburgposition,andhighintra-abdominalpressure. Theprimaryaimwastodescriberespiratoryandhemodynamicchallengesandthecomplications relatedtohighintra-abdominalpressureandthedeepTrendelenburgpositioninrobotic pros-tatectomypatients.Thesecondaryaimwastorevealsafedischargecriteriafromtheoperating room.
Methods:Fifty-threepatientswhounderwentroboticprostatectomybetweenDecember2009 andJanuary2011wereprospectivelyenrolled.Mainoutcomemeasureswerenon-invasive mon-itoring, invasivemonitoringandbloodgasanalysis performedatsupine(T0), Trendelenburg
(T1),Trendelenburg+pneumoperitoneum(T2),Trendelenburg-beforedesufflation(T3),
Trende-lenburg(afterdesufflation)(T4),andsupine(T5)positions.
Results:Fifty-threeroboticprostatectomypatientswereincludedinthestudy.Themain clin-icalchallengeinourstudygroupwasthechoiceofventilationstrategytomanagerespiratory acidosis,whichisdetectedthroughend-tidalcarbondioxidepressureandbloodgasanalysis. Furthermore,themeanarterialpressureremainedunchanged,theheartratedecreased sig-nificantlyandrequiredintervention.Thecentralvenouspressurevalueswerealsoabovethe normallimits.
Conclusion: Respiratoryacidosisand‘‘upperairwayobstruction-like’’clinicalsymptomswere themainchallengesassociatedwithroboticprostatectomyproceduresduringthisstudy. © 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
夽 ThestudywascarriedoutintheDepartmentofAnesthesiologyandReanimationofAnkaraAtaturkTrainingandResearchHospital. 夽夽PresentedinEuroanaesthesiaCongress,Paris,France,9---12June2012.
∗Correspondingauthor.
E-mail:[email protected](M.Oksar).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Cirurgiarobótica; Prostatectomia; Cirurgiaurológica
Prostatectomiarobótica:análiseanestesiológicadecirurgiasurológicasrobóticas: estudoprospectivo
Resumo
Justificativaeobjetivos: Embora muitas características da prostatectomia robótica sejam semelhantesàquelas de laparoscopiasurológicas convencionais(como aprostatectomiapor laparoscopia),oprocedimentoestáassociadoaalgunsinconvenientes,incluindoacesso intra-venosolimitado,tempocirúrgicorelativamentelongo,posic¸ãodeTrendelenburgprofundae pressãointra-abdominalalta.Oobjetivoprincipalfoi descreverasalterac¸ões respiratóriae hemodinâmicaeascomplicac¸õesrelacionadasàpressãointra-abdominalelevadaeàposic¸ão deTrendelenburgprofunda em pacientessubmetidos àprostatectomiarobótica.Oobjetivo secundáriofoirevelarcritériossegurosdealtadocentrocirúrgico.
Métodos: Foraminscritosprospectivamente53pacientessubmetidosàprostatectomiarobótica entredezembro de2009ejaneirode2011. Asmedidasdedesfechoprimário foram: moni-toramentonãoinvasivo,monitoramentoinvasivoegasometriafeitaemdecúbitodorsal(T0),
Trendelenburg (T1), Trendelenburg+pneumoperitônio (T2), Trendelenburg pré-desinsuflac¸ão
(T3),Trendelenburgpós-desinsuflac¸ão(T4)eposic¸õessupinas(T5).
Resultados: Oprincipaldesafioclínicoemnossogrupodeestudofoiaescolhadaestratégia deventilac¸ãoparacontrolaraacidoserespiratória,queédetectadapormeiodapressãode dióxidodecarbonoexpiradoedagasometria.Alémdisso,apressãoarterialmédiapermaneceu inalteradaeafrequênciacardíacadiminuiusignificativamenteeprecisoudeintervenc¸ão.Os valoresdapressãovenosacentraltambémestavamacimadoslimitesnormais.
Conclusão:A acidose respiratória e sintomas clínicos ‘‘semelhantes à obstruc¸ão das vias aéreas’’foramosprincipaisdesafiosassociadosaosprocedimentosdeprostatectomiarobótica. ©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Laparoscopic prostatectomy was first performed by Bhandarietal.in1997usinga transperitonealapproach.1
Anextraperitonealapproachwassubsequentlydescribedby
Raboyetal.,withthefirstclinicalcasesofextraperitoneal
laparoscopicradical prostatectomy usinga roboticsystem
developed and reported by Pruthi et al. in 2003.2,3 The
introductionofthedaVinciSurgicalSystemhastransformed
thefieldof robotic surgeryacross thecountry andsolved
someofthelimitationsoftraditionallaparoscopicurology.
Roboticprostatectomy(RP)hasenabledurologiststouse
amore controlled and accuratelaparoscopic approach to
radicalprostatectomy.Comparedtotheopenmethod,the
robotic-assistedapproachoffersmanyadvantagesincluding
bettervisualizationandamoreprecisemanipulationof
del-icatevesselsandnerves.4Thesurgeoncanbetterpreserve
theintegrityoftheneurovascularbundleswhichresultsin
improvedpostoperativeurinaryandsexualfunction.5Other
benefits include less postoperative pain, diminished
scar-ring,reducedbleedingandshorterhospitalstays.
Although many features of RP are similar to those of
conventional laparoscopic urological procedures (such as
laparoscopic prostatectomy), the procedure is associated
with some drawbacks, which include limited intravenous
access,relativelylongoperatingtime,deepTrendelenburg
position,andhighintra-abdominalpressure(IAP).
Insuffla-tionoftheabdomen withCO2 is notbenign.Lung volume
decreases,meanarterialpressureincreaseswhereascardiac
index decreases, and absorption of CO2 causes
hypercar-bia and a concomitant decrease in blood pH.6,7 Any of
thesealterationscan leadtosudden cardiopulmonary
dis-tress.In addition,unintentionalinjury tovesselscanlead
to massive hemorrhage or CO2 embolism requiring rapid
resuscitation.6---8 Routinecapnometry shouldbeusedin all
laparoscopiccasesasitallowstheadequacyofmechanical
ventilationtobeassessed.
Currently,mostoftheknowledgeaboutroboticurological
surgeryhasbeenderivedfromthegynaecologicprocedures
performedinaless-deepTrendelenburgpositionandunder
lowerIAPconditions;andstudiesoflaparoscopic
cholecys-tectomy surgeries that were performed under lower IAP,
witharelatively shortsurgicalduration, andinthe
head-upposition,which canhavedifferent effectsonpatients’
respiratory andhemodynamic parameters aswell astheir
riskofembolism.9Herein,weaimedtodescribethe
anes-theticchallenges in RP proceduresperformed underdeep
Trendelenburg positionand high IAP conditions.
Addition-ally, we aimed todescribe thecriteria for safe discharge
fromtheoperatingroom.
Methods
Studydesign
Ethicalapprovalfromthelocalinstitutionalcommitteeand
written informed consent from each consecutive patient
wereobtained.Fifty-threeconsecutivepatientsadmittedto
ourclinicandwhounderwentRPbetweenDecember2009
andJanuary2011wereprospectivelyenrolledinthestudy.
Non-invasivemonitoring(ECG,pulseoximetry,and
parameters), invasive monitoring (mean arterial pressure
and central venous pressure, and ventilator parameters)
(Infinity Delta patient monitor, Draeger Medical Systems,
Inc. Telford, PA 18969, USA) and blood gas analysis
were performed at supine (T0),Trendelenburg (T1),
Tren-delenburg+pneumoperitoneum(T2),Trendelenburg-before
desufflation (T3), Trendelenburg (after desufflation) (T4), andsupine(T5)positions.
Afteranesthesiainductionwithpentobarbital4---7mg/kg
and rocuronium 0.6mg/kg, endotracheal intubation was
performed. Anesthesia was maintained with remifentanil
(50mcg/mL)1mcg/kg/minina0.1mcg/kg/mininfusionand
with2MACsevoflurane,withadditionalbolusesof
rocuro-nium as needed. Each patient’s lungs were ventilated in
volume-controlledventilationmodeusing50%oxygeninair
withasettidalvolume(VT)and/orwithbreathingfrequency (f)toachieveanend-tidalcarbondioxidepressure(PET-CO2)
of25---30%,whichwasmonitoredwithbloodgasreportsin
parallel.Fluidmanagementwasconsideredintwointervals,
beforeandafterureteralanastomosis.Fluidwasrelatively
restrictedbeforeureteralanastomosis.Thesecondinterval
includedahigherinfusionratetoreach2---3mL/kg/hofthe
totalfluidamountthroughouttheoperation.
An arterial catheter was inserted in the left radial
artery and central venous catheterizationwas performed
through the right internal jugular vein to measure the
central venous pressure(CVP). CVP was zeroedand
mea-suredonthemid-axillarylineat the4thintercostalspace
in the supine position. The peripheral intravenous access
andarterialaccesswerelengthenedvialines.Ondansetron
4mgwasadministeredintravenously,andorogastrictubing
wasinserted withthe patient in thesupine position.The
intraperitonealpressurewasadjustedto18mmHg.Cerebral
protection was assured by administering dexamethasone
sodiumphosphate 8mg at the beginning of the operation
andfurosemide40mg.
Duringextubation,thepatientsweretakenintoareverse
Trendelenburg position, and diuretic administration was
repeatedtodecreaseupperairwayedemamightbecaused
bythe prolongeduse of thedeepTrendelenburgposition.
Extubation was approved after a blood gas analysis
con-firmednormocapniaduringminimallyassistedspontaneous
breathingandduringspontaneousbreathingof10L/minof
ventilationonaverage, intheabsenceofor withreduced
conjunctival,upperairwayandtongueedema,withreversal
oftheneuromuscularblockade,andatabodytemperature
of35◦Cormore.
Safe extubation wasperformed in the operating room
according to our discharge criteria and was properly
managedasnotedinTable1.Complicationsfromdeep
Tren-delenburgpositioningandanesthesiawererecordedduring
andaftersurgery.Thepatientswereclassifiedaccordingto
their arterial pH levels at T5 as pH<7.35 (the ones with acidosisattheendofsurgery)andpH>7.35(theoneswith improvedacidosis)classes.Inthesegroups,typesofacidosis
developedintraoperativelyandthemanagementofacidosis
weredocumented.
Statisticalanalysis
Data were analyzed using the IBM Statistical Package for
SocialSciences19.0(SPSSInc.,Chicago,IL).Paired-sample
Table 1 An integrated checklist for the safe extubation and dischargeofrobotic prostatectomypatients fromthe operatingroom/recoveryroom.
Beforeextubation
Adequatebreathing
Reversalofneuromuscularblock
Noorimprovedheadandneckhyperemia Noorimprovedrespiratoryacidosis Noorimprovedtongueedema
Noorimprovedswollenand/orwhiteanddull-appearing tongue
Noorimprovedconjunctivaledema
Normocapniainbloodgasanalysisand10L/minMMVon averageduringspontaneousventilation
Afterextubationintheoperatingroom
Nosnoringduringeitherinspirationorexpiration(or whenthepatientisawake,nosignofbeingaffectedby theneuromuscularblock)
Noloudinspiration(whenthepatientisawake)andno signthatthepatientisaffectedbytheneuromuscular block
Noinspiratorydifficultyordistress,(intercostal retraction,supraclavicularretraction,orretractionof thealaenasiduringinspiration)
MMV,meanminuteventilation.
t-testswereusedtoassessthedifferencesbetweengroups. Chi-square test was carried out to compare the nominal variables.
Results
Fifty-threeroboticprostatectomypatients(53males)were includedinthestudy.Themeanagewas60.12±7.33,body massindex (BMI) was27.30±3.97, basal metabolicindex was 27.30±3.97, and American Society of Anesthesiolo-gists(ASA)scorewas1.72±0.59forthestudygroup.Asfor thesurgicalvariables,surgicaltimewas217.04±80.73min, Trendelenburg time was 262.45±75.93min, blood loss was 262.60±50.00mL, total fluids administered was 1680.00±404.71mL. NaHCO3 was administered in 20% of thepatients,andatropinewasadministeredin78.6%ofthe patients.Thenumberof patientswhopresentedpH<7.35 was 35, while the number of patients who presented pH≥7.35was18.
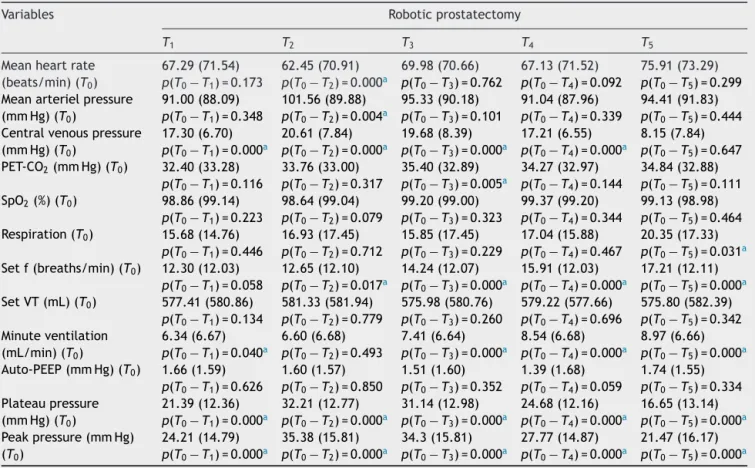
Table2showstheT0valueandtheT1,T2,T3,T4,andT5
valuesforthehemodynamicandrespiratorydata,and
ven-tilatorysettings.Theheartratesweresignificantlydifferent betweenT0andT2(p=0.0001),withalowerHRatT2thanat
T0.Themeanarterialpressure(MAP)valuewassignificantly higheratT2thanT0(p=0.004).ThemeanCVPvaluewas sig-nificantlyhigheratT1,T2,T3,andT4thanatT0(p=0.0001 foralltimepoints).ThemeanPET-CO2valueatT3was sig-nificantlyhigherthanT0(p=0.005).The meanrespiratory rate at T5 was significantly higher than at T0 (p=0.031). Themeanfvaluesat T2,T3,T4,andT5weresignificantly higherthanT0(p=0.017,p=0.0001,p=0.0001,p=0.0001,
Table2 Hemodynamicandrespiratorydataandventilatorysettingsintheroboticprostatectomy.
Variables Roboticprostatectomy
T1 T2 T3 T4 T5
Meanheartrate (beats/min)(T0)
67.29(71.54) 62.45(70.91) 69.98(70.66) 67.13(71.52) 75.91(73.29)
p(T0−T1)=0.173 p(T0−T2)=0.000a p(T0− T3)=0.762 p(T0− T4)=0.092 p(T0− T5)=0.299
Meanarterielpressure (mmHg)(T0)
91.00(88.09) 101.56(89.88) 95.33(90.18) 91.04(87.96) 94.41(91.83)
p(T0− T1)=0.348 p(T0− T2)=0.004a p(T0− T3)=0.101 p(T0− T4)=0.339 p(T0− T5)=0.444
Centralvenouspressure (mmHg)(T0)
17.30(6.70) 20.61(7.84) 19.68(8.39) 17.21(6.55) 8.15(7.84)
p(T0− T1)=0.000a p(T0− T2)=0.000a p(T0− T3)=0.000a p(T0− T4)=0.000a p(T0− T5)=0.647
PET-CO2(mmHg)(T0) 32.40(33.28) 33.76(33.00) 35.40(32.89) 34.27(32.97) 34.84(32.88)
p(T0− T1)=0.116 p(T0− T2)=0.317 p(T0− T3)=0.005a p(T0− T4)=0.144 p(T0− T5)=0.111
SpO2(%)(T0) 98.86(99.14) 98.64(99.04) 99.20(99.00) 99.37(99.20) 99.13(98.98)
p(T0−T1)=0.223 p(T0−T2)=0.079 p(T0−T3)=0.323 p(T0−T4)=0.344 p(T0−T5)=0.464
Respiration(T0) 15.68(14.76) 16.93(17.45) 15.85(17.45) 17.04(15.88) 20.35(17.33)
p(T0−T1)=0.446 p(T0−T2)=0.712 p(T0−T3)=0.229 p(T0−T4)=0.467 p(T0−T5)=0.031a
Setf(breaths/min)(T0) 12.30(12.03) 12.65(12.10) 14.24(12.07) 15.91(12.03) 17.21(12.11)
p(T0−T1)=0.058 p(T0−T2)=0.017a p(T0−T3)=0.000a p(T0−T4)=0.000a p(T0−T5)=0.000a
SetVT(mL)(T0) 577.41(580.86) 581.33(581.94) 575.98(580.76) 579.22(577.66) 575.80(582.39)
p(T0−T1)=0.134 p(T0−T2)=0.779 p(T0−T3)=0.260 p(T0−T4)=0.696 p(T0−T5)=0.342
Minuteventilation (mL/min)(T0)
6.34(6.67) 6.60(6.68) 7.41(6.64) 8.54(6.68) 8.97(6.66)
p(T0−T1)=0.040a p(T0−T2)=0.493 p(T0−T3)=0.000a p(T0−T4)=0.000a p(T0−T5)=0.000a
Auto-PEEP(mmHg)(T0) 1.66(1.59) 1.60(1.57) 1.51(1.60) 1.39(1.68) 1.74(1.55)
p(T0− T1)=0.626 p(T0− T2)=0.850 p(T0− T3)=0.352 p(T0− T4)=0.059 p(T0− T5)=0.334
Plateaupressure (mmHg)(T0)
21.39(12.36) 32.21(12.77) 31.14(12.98) 24.68(12.16) 16.65(13.14)
p(T0− T1)=0.000a p(T0− T2)=0.000a p(T0− T3)=0.000a p(T0− T4)=0.000a p(T0− T5)=0.000a
Peakpressure(mmHg) (T0)
24.21(14.79) 35.38(15.81) 34.3(15.81) 27.77(14.87) 21.47(16.17)
p(T0− T1)=0.000a p(T0− T2)=0.000a p(T0− T3)=0.000a p(T0− T4)=0.000a p(T0− T5)=0.000a
PET-CO2, endtidalcarbondioxidepressure;SPO2, saturationofperipheraloxygen;setf,setbreathingfrequency;setVT,settidal
volume.
ap<0.05.
T3,T4,andT5weresignificantlyhigherthanT0(p=0.040,
p=0.0001,p=0.0001, p=0.0001, respectively).The mean
plateau pressures and peak pressures at T1, T2, T3, T4, andT5weresignificantlyhigherthanthemeanvalueatT0 (p=0.0001foralltimepoints).Nosignificantdifferencein
theSPO2 valuesandin the PEEPvalues atany timepoint
comparedwithT0wasobserved(p>0.05).
Patients with a pH<7.35 exhibited significantly higher
PaCO2 levels, compared with those with pH>7.35at T5
(p=0.034).Base excesslevelsin patientswithapH<7.35
were significantly lower when compared with those with
pH>7.35 at T5 (p=0.024). Lactateand HCO3 levels at T5 didnotshowsignificantdifferencesbetweenpatientswitha pH<7.35atT5andpatientswithapH>7.35atT5(p=0.367, andp=0.073, respectively) (Table 3). There were no sig-nificantdifferencesinthesettidalvolume(setVT)orthe setbreathingfrequency(setf)atanytimepointduringthe
operationbetweenthepatientswithapH<7.35andthose
withapH>7.35(Table4).
Anesthesia-andposition-relatedcomplicationsobserved
includedconjunctivaledema(60.4%),regurgitation(15.1%),
swollen tongue(15.1%), arrhythmia(bradycardia) (15.1%),
head and neck edema (13.2%), loud inspiration (13.2),
hyperemiaoftheheadandneck(5.7%),difficultyon
inspi-ration(3.8%),andneuropraxia(1.9%).TheneedforICUwas
observedin9.3%ofthestudygrouppostoperatively.
Discussion
In the present study, we aimed to describe the
anes-thetic challenges related to the high IAP and deep
Trendelenburg positioning in RP patients. Although deep
TrendelenburgpositioningandaprolongedIAPof18mmHg
Table3 ArterialbloodgasreportsbasedacidosisdeterminantsinbothpH<7.35andpH>7.35casesoftherobotic prostatec-tomyatT5.
Determinants pH<7.35atT5(n=35) pH≥7.35atT5(n=18) pValue
PaCO2(mmHg) 4485±7.55 33.93±3.15 0.034
Baseexcess(mEq/L) ---5.46±1.57 ---3.66±1.53 0.024
Lactate(mg/dL) 13±8.41 12.63±4.17 0.367
Table4 IntraoperativechangesinthesetbreathingfrequencyandsettidalvolumeatpH≥7.35andpH<7.35casesatT5.
pH<7.35atT5(n=35) pH≥7.35atT5(n=18) pValue
Settidalvolume(mL) 553.81±53.75 547.77±78.82 0.446
Setbreathingfrequency(breaths/min) 16.27±4.02 16.85±4.12 0.342
can produceadverse cardiovascular, respiratory, and neu-rological effects, Kalmar et al. have reported that the hemodynamic andpulmonary parametersremainedwithin physiological limitsin theirRP study,whichindicates that theTrendelenburgpositioningandCO2pneumoperitoneum werewelltolerated.7Theresultsofourstudydemonstrate
thatourhemodynamicandrespiratorydatadifferfromthose
reportedbyKalmaretal.Thedifferencemighthaveresulted
fromourrelativelylargerclinicalstudyof53patientswho
underwentRP proceduresinasimilardeepTrendelenburg
positionandahighmeanIAPof18mm.
Changes in respiratory parameters require intense
adjustments.Accordingly,theobservedincreasesinthe
PET-CO2 caused bydecreases inthe VT, whichmayhave been
duetothedeepTrendelenburgpositioningand
pneumoperi-toneum,werecompensatedbyincreasesinthefandminute
ventilation in order to prevent respiratory acidosis. The
plateaupressuresandpeakpressures,whichexceededthe
normal limitsdueto both deepTrendelenburgpositioning
andpneumoperitoneum, wereloweredby increasingthef
conservatively, toavoid generating auto-PEEP.Changes in
the intrathoracicpressure and themechanical ventilation
settingsalsocouldhave ledtoPEEP generation.The high
plateau and peak pressures observed in our study group
at the end of the operations in the supine position may
have been relatedtothepatients’ spontaneousbreathing
efforts and/or possible residual pneumoperitoneum. The
mainclinicalchallengeinourstudygroupwasthechoiceof
ventilationstrategy tomanagerespiratoryacidosis,which
is detected through PET-CO2 and blood gas analysis. First
of all,increasing thebreathing frequency toincrease the
MMV,whichreducedthePET-CO2values,wasrequired
dur-ingTrendelenburgpositioningwithpneumoperitoneum.This
resultdemonstratesthat the increasein the PET-CO2 was
notduetoahigherASAscoreor pulmonarycomplications
butrathertoanincreaseinthePaCO2valuecausedbyCO2
pneumoperitoneum.Secondly,theplateaupressure(sumof
thetotalPEEPandthedrivingpressure)wasmonitoredto
avoidgoingbeyonda35mmHglimit.Inthedeep
Trendelen-burgposition,thepatientstendedtodevelopauto-PEEPand
intrathoracic pressures with high airway pressures, which
may have compromised the VT through auto- or
exces-sivePEEPand/orareduceddrivingpressure.Itisunknown
whetherahighIAPinadeepTrendelenburgpositionplaced
limitationsonthedrivingpressurewithorwithouthigh
air-waypressures,whichmighthavecompromisedtheVT.The
effectsofdeepTrendelenburgpositioningandahighIAPon
lungmechanicsarealsounknown.TheVTwasadjustedto
provideadequateventilationwithoutexceedingapeak
air-waypressureof40cmH2O.AsVTwasreducedinthedeep
Trendelenburgposition, an adjustment toMMV was made
usingf.Toavoidor minimizeauto-PEEP,thebreathing
fre-quencywasadjustedtoallowcompleteexhalation,withan
inspiration-to-expirationratio(I/E)of1/2.
Peritonealinsufflationinduces significant alterations in hemodynamics.10,11Inourstudy,theincreasedPET-CO
2may
havebeen duetothe use of alarge amount of total CO2
duringinsufflationpriortoextubationandmayhave been
duetoinspirationand/or exhalationdifficulties.
Maintain-ingthe PET-CO2 between 32.40 and 35.40mmHg resulted
inPaCO2valuesof33.23---41.60.Theseresultssuggestthat
the patients’ conditions had no negative effects on CO2
removal.Additionally,asanon-invasive,indirect
measure-ment,PET-CO2is anaccuratemeansofmonitoring PaCO2,
anddeep Trendelenburg positioning does not diminish its
usefulness.12,13 In their RP study, Kalmar et al. reported
higherPET-CO2 andPaCO2 valuesthan ours, withPET-CO2
valuesbetween3.40and4.66kPa,whichresultedinaPaCO2
between4.66and6.00kPa.7Therewerenochangesinthe
PET-CO2,SpO2,orrespirationastheMMVwasincreasedby
increasingbreathingfrequencytoprovidetheCO2removal
and the neuromuscular block was reversed properly in
thisstudy.Although the plateauand peakpressures were
reduced by the use of the supine position at the end of
theoperations, thesepressures remainedhigh during the
procedures. However, both pressures reached their
high-estvaluesduringthedeepTrendelenburgpositioningwith
pneumoperitoneum.
Although an increase in arterial pressure and slightly
increasedHRareassociatedwithperitonealinsufflation,a
drop in cardiac output has been also reported in the
lit-erature,whether the patient is placed in the head-down
orhead-up position.12,14---16 In ourstudy,although theMAP
remained unchanged, the HR decreased significantly and
requiredintervention.TheCVPvalueswerealsoabovethe
normallimits.Thesehighvaluesmightbeduetothe
Tren-delenburgpositioningastheyreturnedtotheirinitialvalues
by the end of the operation. Although the most obvious
effectsof the RP procedureson HR,MAP, andCVP inour
studyoccurredimmediatelyafterthepatientsweremoved
into the Trendelenburg position with pneumoperitoneum,
thesemeasurementscontinued tobe affectedto alesser
degreeuntilthesupinepositioningattheendofthe
proce-dures.ThemostobviouschangeswereobservedintheCVP.
Thelactatedidnotincrease;therefore,therewasno
indi-cationthatanaerobic metabolismoccurredor contributed
totheacidosis.Inastudyof18ASA-1statuspatients,
Tor-rielliet al. reportedthat increasingthe IAP to10mm Hg
wasassociated witha decrease in the cardiac indexthat
returnedtoitsinitialvalueafter10minof10◦Trendelenburg
positioning.TheyalsoreportedthatelevatedIAPwas
asso-ciatedwithincreasesintheMAPandthesystemicvascular
resistance,andthesevaluesdidnotreturntonormalafter
peritonealexsufflation.14Inthepresentstudy,weobserved
theacuteeffectsof Trendelenburgpositioningwith
pneu-moperitoneum asan increase in the MAP and a decrease
similar high-ASA related findings.7 Kordan et al. demon-stratedthatTrendelenburgpositioningsignificantlyincrease MAP.17Inthepresentstudy,theMAPincreasedsignificantly
atthe beginningof theTrendelenburgpositioningwithno
pneumoperitoneum.TheincreasesintheCVPvaluesinboth
deepTrendelenburgand5◦Trendelenburgpositioning,with
andwithoutpneumoperitoneum, andthedecreasesinthe
CVPvaluestobaselineattheendoftheoperationindicate
acloserelationshipbetweenCVPvaluesandTrendelenburg
positioningaloneorwithIAP.
Althoughthebloodgasanalyseswereusedtoassessboth
respiratoryandmetabolicproblemsatallthetimepoints,
thepresenceofacidosiswasdeterminedas‘‘pH<7.35′′and
normal as ‘‘pH>7.35′′ based on the blood gas reports at
theendoftheoperation(T5).Inthisstudy,atallthetime
points,the diagnosedacidosis types were respiratoryand
metabolic acidosis. Increases in the set VT or the set f
reflectedrespiratoryacidosismanagementduringthe
oper-ation.Therespiratoryproblemsdeterminedinthepresent
studyincludedthedecreaseinarterialpHduetothehigh
PaCO2pressure,andupper-airwayandtongueedemadueto
thedeepTrendelenburgpositionandendotrachealcuff
pres-sureonthetonguebase.Themanagementstrategyfocused
onavoidinganyadditionaldecreaseinthepH,whichcould
haveworsenedthebloodgasparameterstoward7.20pHand
18mmol/LHCO3.Normocarbiaandmaintenanceofan
ade-quateMMVwerethemaingoalsinthebloodgasmonitoring
duringthesurgicalproceduresandextubationassessment.
Because the PaO2 and SPO2 did not decrease to critical
values,nopatientsineithergrouprequiredadditional inter-ventions.
Pruthi et al. reported6.1h of surgical time for
cysto-prostatectomyandameanbloodlossof313mL.3Themean
surgical time reported for their RP cases was similar to
ours.Inastudyofthetransfusionrequirementsinopenand
robotic-assistedlaparoscopicradicalprostatectomies,
Kor-danetal.demonstratedthatRPwasassociatedwithlower
bloodlossandasmallerchangeinhematocritthantheopen
prostatectomy group.17 In our study,none ofthe patients
requiredtransfusions.
In a study by Bhandari et al., the perioperative
complications during robotic RP included one
anesthesia-related complication out of a total of 16 complications
in 300 patients who underwent RP.1 It has been
estab-lished that deep Trendelenburg positioning can cause
decreases in functional residual capacity, total lung
vol-ume, and pulmonary compliance and may facilitate the
development of atelectasis.18 In our study, the most
frequent anesthesia- and position-related complications
were conjunctival edema, regurgitation and ‘‘upper
air-way obstruction-like’’ clinical symptoms that might lead
to or worsen respiratory acidosis. Phong et al. reported
theclinicalsignsofupperairwayedemaviaareductionin
thevenousoutflow fromthehead causedby
pneumoperi-toneumduringprolonged,deepTrendelenburgpositioning.8
Weobservedenlargedanddull,edematoustongues,snoring,
loudinspiration,inspiratorydifficulty, alae nasiretraction
andsupraclavicularretractionintercostalretractionswhen
thepatientsawakened andwereextubated. Endotracheal
cuffpressure on the tongue base can cause and enhance
tongue edema by preventing the lymphatic and venous
drainageofthetongue.Theuseofthehead-uprightposition
priortoextubation,diureticusewhennecessaryand
extu-bation itself improved these symptoms. Our criteria for
dischargefromtheoperatingroom,inadditiontoAlderete
scoring,includedimprovementsintheseupperairwaysigns
andsymptoms. Thecomplications duetodeep
Trendelen-burgpositioningand/orpneumoperitoneumwerelimitedto
the operating room for most of the patients, the
major-ity of whom didnot demonstrate any need for admission
to the ICU. In their study of perioperative complications
duringRP,Bhandarietal.demonstratedanoverall
complica-tionrateof5.3%andamajorcomplicationrateoflessthan
2%intheirseries,usingthemethodofClavientetal.1,19 In
thepresent study,neurologiccomplicationswererareand
temporary, andtheywere recordedon thefirst day
post-operativelyin theward.The onlyneurologiccomplication
observed in thepresent study wasa temporaryunilateral
sensoryandmotorneuropraxiaintherightarmdetermined
onthe1stpostoperativedaythatlastedfor3days,similarto acomplicationobservedinthereportbyYeeetal.20
Arrhyth-miacanbeinducedbyseveralcausesinlaparoscopiccases.
Inourstudy,bradycardiaaccountedformostofthe
arrhyth-mia cases during RP procedures, and these complications
occurred immediatelyafter thepatients weremovedinto
the Trendelenburg position and/or preceding the surgical
procedure.Weinterpretedthistimingasindicatingthatthe
arrhythmiaresultedfromtheTrendelenburgpositionand/or
thereflexesinducedbythesuddenstretchingofthe
pneu-moperitoneum,whichmayhavecausedanincreaseinvagal
tone.Additionally,theremifentanilinfusionmayhavearole
inbradycardiainthesecases.However,thebradycardiawas
notobservedduringtheremifentanilinfusionsinanyother
partsofthesurgicalprocedures.
Themainpurposeofthepresent studywastodescribe
theanestheticchallengesrelatedtothehighIAPanddeep
TrendelenburgpositioninginRPpatients.However,thehigh
IAP utilized in the present report could be responsible
for several complications adding the deep Trendelenburg
positioning. In animal studies, intraperitoneal pressures
>20mmHg resulted in intraabdominal venous collapse,
whichoccurred atlowerlevelsofintraperitonealpressure
in thepresenceof hypovolemia.21 Thus,relativevariation
in intraperitoneal pressureand peripheral vesselsmay be
themaindeterminantsofvascularwallmovements
respon-sible for venous collapse and opening, and there could
be situations that facilitate gas embolization. Increasing
intraperitonealpressuremightreduceriskofgasembolism,
but it couldcause hemodynamic andrespiratory
instabil-ityinthatposition.Therefore,thechallengeforclinicians
istoobtainanoptimalintraperitonealpressuretobalance
between therisksof gas embolismandhemodynamic and
respiratoryinstabilityduringlaparoscopicradical prostatec-tomy.
It must be clearly stated that the use of a lower IAP
could certainly determine lower anesthetic complications
suchasrespiratoryacidosis,metabolicacid-basedisorders,
fluid management issues, position-related ‘‘upper airway
obstruction-like’’ clinical symptoms, the maintenance of
normocarbia, and the provision of adequate MMV. These
respiratory problems may cause decreased arterial blood
pH, and require specialattention to preventa worsening
inacidosis,whichexhibitedmuchgreatermetabolic
ventilatorysettingsshouldbemanagedcarefully.Itis
criti-caltomonitorfluidinfusionregimens(tomanagemetabolic
asidosis),andthePET-CO2andbloodgasestomaintain
nor-mocarbiaandanadequateMMV.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Bhandari A, McIntire L, Kaul SA, et al. Perioperative complicationsofroboticradicalprostatectomyafterthe learn-ingcurve.JUrol.2005;174:915---8.
2.RaboyA,FerzliG,AlbertP.Initialexperiencewith extraperi-tonealendoscopicradical retropubicprostatectomy.Urology. 1997;50:849---53.
3.PruthiRS,NielsenME,NixJ,etal.Roboticradicalcystectomy forbladdercancer:surgicalandpathologicaloutcomesin100 consecutivecases.JUrol.2010;183:510---4.
4.SandlinD.Roboticassistedprostatectomy.JPerianesthNurs. 2004;19:114---6.
5.Menon M, Hemal AK, Tewari A, et al. Nerve-sparing robot-assistedradicalcystoprostatectomyandurinarydiversion.BJU Int.2003;92:232---6.
6.GoodaleRL,BeebeDS,McNevinMP,etal.Hemodynamic, respi-ratory,andmetaboliceffectsoflaparoscopiccholecystectomy. AmJSurg.1993;166:533---7.
7.KalmarAF,FoubertL, HendrickxJF,etal. Influenceofsteep TrendelenburgpositionandCO2pneumoperitoneumon
cardio-vascular,cerebrovascular,and respiratoryhomeostasisduring roboticprostatectomy.BrJAnaesth.2010;104:433---9.
8.Phong SV, Koh LK. Anaesthesia for robotic-assisted radi-cal prostatectomy: considerations for laparoscopy in the Trendelenburg position. Anaesth Intensive Care. 2007;35: 281---5.
9.CunninghamAJ,BrullSJ.Laparoscopiccholecystectomy: anes-theticimplications.AnesthAnalg.1993;76:1120---33.
10.Struthers AD, Cuschieri A. Cardiovascular consequences of laparoscopicsurgery.Lancet.1998;352:568---70.
11.KoivusaloAM,LindgrenL.Effectsofcarbondioxide pneumoperi-toneum for laparoscopic cholecystectomy. Acta Anaesthesiol Scand.2000;44:834---41.
12.Hirvonen EA, Nuutinen LS, Kauko M. Hemodynamic changes due to Trendelenburg positioning and pneumoperitoneum during laparoscopic hysterectomy. Acta Anaesthesiol Scand. 1995;39:949---55.
13.Odeberg S, Ljungqvist O, Svenberg T, et al. Haemodynamic effects of pneumoperitoneum and the influence of posture duringanaesthesiaforlaparoscopicsurgery.ActaAnaesthesiol Scand.1994;38:276---83.
14.TorrielliR,CesariniM,WinnockS,etal.Hemodynamicchanges during celioscopy: a study carried out using thoracic elec-tricbioimpedance. Can JAnaesth.1990;37:46---51[article in French].
15.Walder AD, Aitkenhead AR. Role of vasopressin in the haemodynamicresponsetolaparoscopiccholecystectomy.BrJ Anaesth.1997;78:264---6.
16.JorisJL,ChicheJD, CanivetJL,etal.Hemodynamicchanges inducedbylaparoscopyandtheirendocrinecorrelates:effects ofclonidine.JAmCollCardiol.1998;32:1389---96.
17.Kordan Y, Barocas DA, Altamar HO, et al. Comparison of transfusion requirements between open and robotic-assisted laparoscopicradicalprostatectomy.BJUInt.2010;106:1036---40.
18.HazebroekEJ,BonjerHJ.Effectofpatientpositionon cardio-vascularandpulmonaryfunction.In:WhelanRL,FleshmanJW, FowlerDL,editors.TheSagesmanualofperioperativecarein minimallyinvasivesurgery.NewYork:Springer;2006.p.410---7.
19.ClavienPA,SanabriaJR,StrasbergSM.Proposedclassification ofcomplicationsofsurgerywithexamplesofutilityin chole-cystectomy.Surgery.1992;111:518---26.
20.Yee DS, Katz DJ, Godoy G, et al. Extended pelvic lymph node dissection in robotic-assisted radical prostatectomy: surgical technique and initial experience. Urology. 2010;75: 1199---204.