REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Histopathologic
comparison
of
dexmedetomidine’s
and
thiopental’s
cerebral
protective
effects
on
focal
cerebral
ischemia
in
rats
Ebru
C
¸anakc
¸ı
a,∗,
Sevilay
Akalp
Özmen
b,
Mustafa
Ferhat
C
¸olak
c,
Hüsnü
Kürs
¸ad
daOrduUniversity,TrainingandResearchHospital,ClinicofAnesthesiologyandReanimation,Ordu,Turkey bErzurumTrainingandResearchHospital,DepartmentofPathology,Erzurum,Turkey
cOrduStateHospital,ClinicofAnesthesiologyandReanimation,Ordu,Turkey
dAtatükUniversity,FacultyofMedicine,ResearchHospital,ClinicofAnesthesiologyandReanimation,Erzurum,Turkey
Received31December2014;accepted10March2015 Availableonline5February2016
KEYWORDS
Brainischemia; Dexmedetomidine; Thiopental; Neuroprotection
Abstract Thisstudy was designedtoinvestigate whetherdexmedetomidine andthiopental have cerebralprotectiveeffects after focalcerebralischemia inrats. Thirty maleSprague Dawley rats were randomly assigned to three groups: control group (Group C, n=10), dexmedetomidinegroup(GroupD,n=10),thiopentalgroup(GroupT,n=10).Afterallratswere anesthetized,theywereintubated,thenmechanicallyventilated.Acatheterwasinsertedinto therightfemoralarteryforcontinuousmeanarterialpressure,physiologicalparametersand bloodsamplingatbaseline,5minafterocclusionand20minafterreperfusion.Acatheterwas insertedintotheleftfemoralveinforintravenous(IV)medicationadministration.Right com-moncarotidarteryofeachratwasisolatedandclampedfor45min.Attheendoftheduration commoncarotid arterywereunclampedandthebrainreperfusion wasachievedfor90min. DexmedetomidinewasadministeredforGroupDIVinfusion,andGroupTreceivedthiopental IV.AccordingtohistopathologicscorescerebralischemiawasdocumentedinallratsinGroupC, butnoischemiawasfoundinthreeratsinGroupTandinfourratsinGroupD.Grade3cerebral ischemiawasdocumentedinthreeratsinGroupC,andinonlyoneratinbothgroupsTand D.ForhistopathologicgradesthedifferencebetweenGroupTandGroupDwasnotsignificant (p>0.05).ButthedifferencesbetweenGroupCandGroupT(p<0.05)andGroupCandGroup D(p<0.01)werestaticallysignificant.Inconclusion,wedemonstratedthatdexmedetomidine andthiopentalhaveexperimentalhistopathologiccerebralprotectiveeffectsonexperimental focalcerebralischemiainrats.
©2015SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](E.C¸anakc¸ı).
http://dx.doi.org/10.1016/j.bjane.2015.03.009
0104-0014/©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
PALAVRAS-CHAVE
Isquemiaencefálica; Dexmedetomidina; Tiopental;
Neuroprotec¸ão
Comparac¸ãohistopatológicadosefeitosprotetorescerebraisdedexmedetomidina etiopentalsobreisquemiacerebralfocalemratos
Resumo Esteestudofoidesenhadoparainvestigarsedexmedetomidinaetiopentalpossuem efeitosprotetorescerebraisapósisquemiacerebralfocalem ratos.Trintaratosdalinhagem
SpragueDawleyforamrandomicamentealocadosemtrêsgrupos:controle(GrupoC,n=10), dexmedetomidina(GrupoD, n=10)etiopental(GrupoT,n=10).Apósaanestesia,todosos ratosforamintubadoseventiladosmecanicamente.Umcateterfoiinseridonaartériafemoral direitaparamonitorac¸ãocontínuadapressãoarterialmédia(PAM),dosparâmetrosfisiológicos eparacoletadeamostrasdesanguenafasebasal,5minutosapósaoclusãoe20minutosapós areperfusão.Umcateterfoiinseridonaveiafemoralesquerdaparaadministrac¸ãointravenosa (IV) demedicamentos.A artériacarótida comumdireitadecadarato foiisoladae pinc¸ada durante45minutos.Ao finaldos45 minutos,opinc¸amento foiremovido eareperfusãodo cérebrofoiobtidapor90minutos.DexmedetomidinafoiadministradaporinfusãoIVnoGrupo DethiopentalnoGrupoT.Deacordocomaspontuac¸õeshistopatológicas,isquemiacerebral foiobservadaemtodososratosdoGrupoC,masnãofoiencontradaemtrêsratosdoGrupo TeemquatroratosdoGrupoD.Ograu3deisquemiacerebralfoiobservadoem trêsratos dogrupoCeemapenasumratodeambososgruposTeD.Paraosgraushistopatológicos,a diferenc¸aentreoGrupoTeoGrupoDnãofoisignificativa(p>0,05).Porém,asdiferenc¸asentre oGrupoCeoGrupoT(p<0,05)eentreoGrupoCeoGrupoD(p<0,01)foramestatisticamente significativas.Emconclusão,demonstramosquedexmedetomidinaetiopentalpossuemefeitos histopatológicosprotetorescerebraissobreisquemiacerebralfocalexperimentalemratos. ©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
It has been demonstrated by prospective epidemiological studiesconductedindevelopedwesterncountriesthat cere-brovascular diseases (CVDs)areresponsible for 10% of all deathsandarerankedthirdafterheartdiseasesandcancer asacause of mortality.1---3 About 75%of CVDsresult from thromboticoremboliccerebralinfarcts.2,4
Theinfarctmodelprovidedbyocclusionofexperimental middlecerebral artery(MCA) representingthe focal cere-bralinfarction which is themost common typeof CVD in clinical practice has been widely accepted.2,4,5 Rats bear avery closeresemblance to thehuman brain in terms of cerebrovascularanatomyandphysiologyandthus,theyare widelyusedincerebralischemiastudies.3Thevalidityofthis modelofcerebralischemiahighlydependsonstrictcontrol of physiological parameters which may causefluctuations andchangesintheresultssuchasbodytemperature,blood pressure,bloodgases,andglucoselevels.4
In clinicaluse, thereis stillnoidealmedication which bearsallthedesiredcharacteristicsandiseffectiveenough incerebralischemia.6,7Inordertorespondtoclinicalneeds, inanimal models,alargenumberofagentsfromdifferent chemicalgroupswhichisthoughttohavebeneficialeffects incerebralischemiaarestillbeingtestedandtheireffects oncerebralischemiaaremethodologicallyexamined.2,4The novel molecular-level information onthe pathophysiology of cerebral ischemia have led to the use of numerous potential therapeutic agents estimated or alleged to be effective onsuch pathophysiologic mechanismsin experi-mentalstudies.8,9
The effects of barbiturates as well as the thiopen-tal, an agent mostly used in anesthesia practice in this class,oncerebralbloodflowandcerebralmetabolismwere researchedandfoundtocauseadecreaseincerebralblood flow and cerebral metabolic rate depending on thedose. It has been observed that cerebral oxygen metabolism is reduced by55---60% at a barbituratedose causing isoelec-tricityinEEG;however,cerebralmetabolismproceededand thecerebral basalmetabolismthat isnecessary toensure physiologicalfunctionsandcellintegrityofneuronsdidnot depressedthroughafurtherincreaseoftheblood barbitu-ratesdose.10,11
Therearedifferentviewsaboutwhetherornot barbitu-ratesareneuroprotective.Inpost-traumaticfocalcerebral ischemia; theyarefound to reduce hyperemia by making adeepdepressioninthecerebralmetabolicrate,improve theharmonyofflow&metabolism,increaseperfusioninthe low-flow regionand have brainprotective effectby mini-fyingtheinfarctedarea.12,13 Thiopentalandmethoheksital wereagainstudiedatdifferentdosesinthemodelsoffocal cerebralischemiainratsandwerehistopathologicallyshown toreduceinfarctvolumeatdosescausingburstsuppression inEEG.14
cerebralbloodflowandthecerebrovascularreactivityisstill unclear.
It hasbeen observed that administering dexmedetomi-dineinfocalcerebralischemiareducestheinfarctvolume in the cortexby 40% and in additionto this,causes min-imal hyperglycemia and hypotension.15 It has been also observedthat,throughadministrationofdexmedetomidine inincompletecerebralischemia,theplasmacatecholamine levelswere decreased andthe histopathological improve-mentbecamebetterthancontrol,dependingonthedose.16 Besides, in terms of the infarct volume after temporary occlusion (15mcg/kg), a 31% decrease in cortexand 20% decreasein striatumwerereportedin rats giventhehigh dose of dexmedetomidine.17 It has been also reported that, while circulating catecholamines were decreasing during cerebral ischemia, the noradrenaline and gluta-mate concentrations in the brain were not affected by dexmedetomidine.18The␣-2adrenoceptorsubtypescausing neuroprotectiveeffectswerereportedtobe␣-2A.19
Purpose
The purpose of this study is to histopathologically study whetherornotthiopentalanddexmedetomidinewhichare amongtheintravenousanestheticshavecerebralprotective effectsonfocalcerebralischemiainrats.
Materials
and
methods
This study was carried out in Atatürk University, Experi-mentalMedicalResearchandApplicationCenter(ATADEM) withpermissionfromtheethicscommitteeestablishedby AtatürkUniversity,theOfficeoftheDeanoftheFacultyof Medicine.Thefive-month-oldSpragueDawley-type30male ratswhichare250---300ginweightwereobtainedfrom ATA-DEM.
Forthesakeofhavingsafeandhealthyresearchresults, particularattentionwaspaidtoselectsubjectswhichwere not used in a study before and were not exposed to any medicationaswell aswhich didnothaveany diseaseand werefullyhealthyduringourexperiments.
Nosubjectsincludedinthestudywerefed12---16hbefore thestudyinordertokeepthemhungry.Inthemeantime, eachsubject’sweightwasdeterminedandrecorded.Then theratswere randomlydividedintothreegroups: control group(GroupC,n=10);dexmedetomidinegroup(GroupD, n=10);thiopentalgroup(GroupT,n=10).
All subjects were anesthetized with 5% isoflurane (ForanefJ,Abbott,Istanbul,Turkey)intheglassvasethrough theanesthesiamachineintheresearchlaboratoryof ATA-DEM. Neck regions of the subjects in the supine position wereshaved and thesterilization of the surgical sitewas achieved.Theirheadswereslightlyextendedandthe mid-line pretrachealsurgicalincisionwasmade.Subsequently, thetracheawasintubated(Fig.1)andtheirlungsbeganto bemechanicallyventilated.Alongwiththeventilation,2% isoflurane,30%oxygenand70%nitrousoxidewasgivento subjects.Ventilationwasappliedina waytofixthe num-ber of breaths per minute to 60 and the tidalvolume to 12mL/kg.Ventilationwascontinuedbyachieving35mmHg of end-tidal carbondioxide. A catheterwas inserted into
Figure1 Oneoftheratsusedandintubatedinthestudy.
Figure2 Oneoftheratstowhicharightcarotidartery dis-sectionwasperformed.
Figure3 Therattowhicharightcarotidarteryocclusionwas performed.
Figure 4 The intubated rat to which right carotid artery occlusionwasperformedandtheanesthesiaapparatusused.
Immediatelyafterischemiawasdeveloped,allsubjects werekilledbydecapitationunderanesthesiaandwere sac-rificed. For histopathological examination, all the brains removedinwholeweretreatedinthefollowingsequence: The brains were put in 10% phosphate-buffered formalin
for durationof 48h. Hippocampuscornuammonis1 (CA1) zone was detected (inthe coronal plane, 3300m poste-riortoBregma).Thetissuesamplestakenweredehydrated withethanolandwereembeddedintoparaffinblocksafter passingthroughxylol;then,4mmthickcoronalsliceswere collected; they werestained with hematoxylin---eosin and 5mmcoronalsliceswerecollected,theanalysiswas evalu-ated,through400×magnification,byapathologyspecialist experienced in this field who had no knowledge of the groups. Based histopathologically on the Nissl substance loss,increaseincytoplasmiceosinophiliaandthepresence ofpyknotichomogenousnucleus,theischemicneuronswere evaluatedasGradeO=ischemicneurons,Grade1=presence of ischemic neurons less than 10%, Grade 2=presence of ischemic neurons between 10% and 50% and Grade 3=presenceofischemic neuronsmorethan50% according tothefrequencyofischemicneuronsinCA1.
Thebrainsfromratsinallgroupsweregivencode num-bers and put into bottles containing 4% formaldehyde in ordertoensurefixation.Thenthetissueswerewashedunder streamingwaterandpassedthroughrespectively70%,80%, 96% and 100% alcohol series for dehydration. In the next step,thetissueswerepassedthroughxyleneseriesfor trans-parency.Finally,theywerekeptinparaffinat60◦Cheated oven and embedded into paraffinblocks.5m-thick slices weretaken fromtheparaffin blocksobtained andkept in an oven at 60◦Cfor durationof 45min. Then,they were passedthroughxylenefor2timesandgradedalcoholseries for 4times(respectively 100%,96%,80%, 70%);washedin streaming waterandplungedintoacidalcoholafterbeing stainedwithhematoxylinfor 30s. Thentheywerestained witheosinfor1min,washedagainandtreatedwithxylene afterpassingthroughtheseriesofalcohol.Atthelaststage, Entellan (Merc)was dropped onthem and they were put underlamella.Then,stereologicalcountingwasstarted.
Basedonthedataobtainedfromtwo-dimensional projec-tionsofthree-dimensionalobjects,stereologyisadiscipline thatenablesustoobtaininformationonrealpropertiesand numericalvaluesofbiologicalstructures(size,number, sur-facearea,volume,etc.).20Thereareseveralmethodsused instereology.Amongthemisthefractionatormethodwhich we usedin ourstudy. Throughthis method,we can learn manydetailsaboutthestructureonhand(surfacearea, den-sity,etc.).Inthisstudy,wecalculatedthenumericaldensity ofneuronsforallgroups.20
Figure5 Counted neuronsareseenintheunbiased count-ingframe atamagnification of40in theStereo-Investigator (version6.0,MicroBrightField,Colchester,VT).Starsindicate intactneuronsandcirclesindicatenecroticneurons.
150---150minthex---yplaneand75m×75minthearea oftheunbiasedcountingframe.Then,theunbiased count-ingframewasplacedontothesection(thesoftwareinthe computerenablesthis)andtheintactanddamagedneurons inthecortexwerecountedbyusingdifferentmarkersand in accordance with the stereological rules. Each animal’s stereologicallynumericaldensityofneuronswascalculated (Fig.5).
Statisticalanalysis
For statistical analysis of the data between groups, Windows-compatibleSPSS(version10.0)programwasused. Cerebralischemiascoresbetweengroupsandtheweightsof thesubjectswerestatisticallyevaluatedusingrespectively chi-squaretestinthe4×2contingencytableand indepen-dentsamplet-test.ANOVA(TwoWayVarianceAnalysis)was usedforstatisticalevaluationofphysiologicalparameters. Whilecomparingthegroupswitheachother,‘‘p-value’’was obtainedandinterpretedusingtheLSD(LeastSquare Differ-ence)method.p<0.05wasconsideredassignificant.
Thedataobtainedbystereologicalviewswereuploaded to the SSPS version 15.0. Data of the intact group and thatofthenecroticgroupwerecomparedwitheachother. Mann---WhitneyUtestwasusedforstatisticalanalysis.Inthe comparisonbetweenthedataofintactgroupandthatofthe necroticgroup,itwasfoundtobestatisticallysignificantin threegroups.
Findings
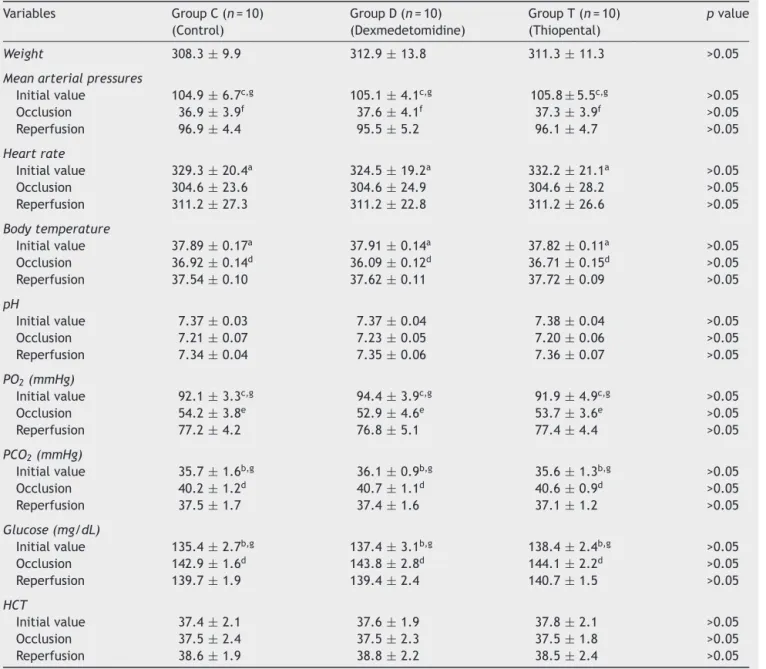
Theirphysical data of the subjects areshown in Table 1. No statistical difference was found between the weights ofallsubjects(p>0.05).Whenthetable wasexaminedin detail, nostatistical differencewas found between mean arterial pressure, heart rate, body temperature, hemat-ocrit,blood glucose,HCT, PO2,PCO2 andpHatthestages
ofstartbeforeischemiaandocclusionandreperfusionafter ischemiabetweenthethreegroups(p>0.05).Forinstance, initial valuesof mean arterial pressure were found tobe 104.9±6.7inthecontrolgroup(GroupC),105.1±4.1inthe dexmedetomidine group (Group D) and 105.8±5.5 in the thiopental group (Group T). When compared statistically, nodifferences were observed in these values.Again, the occlusionvaluesofthemeanarterialpressurewerefoundto be136.9±3.9inthecontrolgroup(GroupC),37.1±4.1in thedexmedetomidinegroup(GroupD)and37.3±3.9inthe thiopentalgroup(GroupT).Inreperfusion,however,these valueswerefoundtoberespectively96.9±4.4,95.5±5.2 and96.1±4.7.Whencomparedstatistically,nodifferences wereobservedinthesevalues.
Table1alsoprovidesstatisticalcomparisonofsubjects’
physiological values between start, occlusion and reper-fusionvalueswithineachgroup.
Itwasfoundoutthatwhiletheinitialvalueofthemean arterial pressurewas found to be 104.9±6.7 in the con-trolgroup(GroupC),itdecreasedto36.9±3.9inocclusion andraisedto96.9±4.4againduringthereperfusion.When the values for this group were statistically compared, a statisticallysignificant differencewas found between the initialvalueof themeanarterialpressureandthatofthe occlusionvalue aswell asthe value of occlusionand the value of reperfusion (p<0.001). A significant difference was also found between the initial value and the value of reperfusion (p<0.05). However, similar statistical dif-ferenceswere found to bebetween the initial, occlusion and reperfusion values of mean arterial pressure in the dexmedetomidineandthiopentalgroups.
While the initial value of heart rate was 329.3±20.4 in the control group (Group C) 329.3±20.4, they were found tohave decreased to 304.9±23.6 in occlusionand to311.2±27.3inreperfusion.Astatisticallysignificant dif-ference was detected between the initial, occlusion and reperfusionvaluesoftheheartrate(p<0.05).Againinthe dexmedetomidineandthiopentalgroups,similarstatistical differenceswerefoundbetween theinitial,occlusionand reperfusionvaluesoftheheartrate.
Itwasfoundoutthatwhiletheinitialvalueofthebody temperature was found to be 37.89±0.17 in the control group(GroupC),it decreasedto36.92±0.14inocclusion andreached to37.54±0.10again duringthereperfusion. Whenthevaluesforthisgroupwerestatisticallycompared, astatisticallysignificantdifferencewasfoundbetweenthe initialvalueofthebodytemperatureandthatofthe occlu-sionvalueaswellasthevalueofocclusionandthevalueof reperfusion(p<0.05).No significant differencewasfound between the initial value and the value of reperfusion. However,similar statistical differences were found tobe between the initial, occlusion and reperfusion values of bodytemperaturein thedexmedetomidineandthiopental groups.
Asignificantdifferencewasalsoobservedbetweenthe ini-tial value andthe value of reperfusion (p<0.001).Again, similar statistical differences were found to be between theinitial, occlusionandreperfusionvalues ofpO2 inthe dexmedetomidineandthiopentalgroups.
It was found out that while the initial value of pCO2 was found to be 35.7±1.6 in the control group (Group C),itreached to40.2±1.2in occlusionanddecreased to 37.5±1.7againduringthereperfusion.Whenthevaluesfor thisgroupwerestatisticallycompared,astatistically signif-icantdifferencewasfoundbetweentheinitialvalueofthe pCO2andthatoftheocclusionvalueaswellasthevalueof occlusionandthevalueof reperfusion(p<0.01).A signifi-cantdifferencewasalsoobservedbetweentheinitialvalue andthevalue ofreperfusion(p<0.05).Again, similar sta-tistical differenceswere found tobe betweenthe initial, occlusionandreperfusionvaluesofpCO2inthe dexmedeto-midineandthiopentalgroups.
Itwasfound outthatwhile theinitial valueof glucose was found to be 135.4±2.7 in the control group (Group C),itreachedto142.9±1.6inocclusionanddecreasedto 139.7±1.9againduringthe reperfusion.Whenthe values for this group were statistically compared, a statistically significantdifferencewasfound between theinitial value oftheglucoseandthatoftheocclusionvalueaswellasthe valueofocclusionandthevalueofreperfusion(p<0.01).A significantdifferencewasalsoobservedbetweentheinitial value and the value of reperfusion (p<0.05). Again, sim-ilar statistical differences were found tobe between the initial, occlusionand reperfusionvalues of glucosein the dexmedetomidineandthiopentalgroups.
WhiletheinitialvalueofHctwasfoundtobe37.4±2.1in thecontrolgroup(GroupC),itwasobservedtobe37.5±2.4 inocclusion and38.6±1.9 in reperfusion.Nostatistically significantdifferencewasfoundbetweentheinitial, occlu-sionandreperfusionvaluesofHct(p>0.05).Again,similar statisticaldifferenceswerefoundtobebetweentheinitial, occlusionandreperfusionvaluesofHctinthe dexmedeto-midineandthiopentalgroups(Table1).
Histopathologicalscores
Histopathologicalscoresofallthethreegroupsareshownin
Fig.6.Accordingtothehistopathologicalscore,therewas ischemiainallsubjectsintheGroupC.Therewasno cere-bralischemiain4subjectsintheGroupDandin3subjects intheGroupT.WhileGrade1cerebralischemiawasfound tobein2subjectsintheGroup Candin4subjectsinthe Group D,it wasobserved in5 subjectsin Group T.Grade 2cerebralischemiawasonly foundin3 subjectsinGroup CandinonesubjectinGroupDandGroupT.Yet,Grade3 cerebralischemiawasfound in3 subjectsinGroup Cand onlyinonesubjectinGroupDandGroupT.
No statistically significant difference was observed betweenGroupDandGroupTintermsofhistopathological scores(p>0.05).However,astatisticallysignificant differ-encewasfoundbetweenGroupCandGroupD(p<0.05)and GroupCandGroupT(p<0.01)inthisrespect.
The microscopic images of score obtained through histopathologicexaminationareshown inFig.6(Grade0, Grade1,Grade2andGrade3).
Stereologicalresults
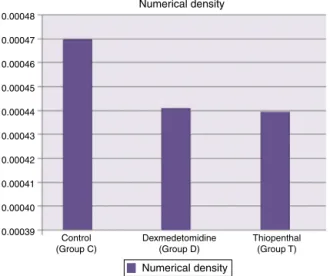
In Fig. 7, the numerical density of necrotic neurons in the control group as well as in the groups treated with dexmedetomidine and thiopental. In the study, it was observed that the average numerical density of necrotic neuronswasveryhighinthecontrolgroup(0.00047n/m3) whileitwaslessinthegroupstreatedwith dexmedetomi-dine(0.00044n/m3)andthiopental(0.00044n/m3).
In Fig. 8, numerical density of intact neurons was given for the control group and the groups treated with dexmedetomidine and thiopental. The number of intact neurons was observed to be (0.00055n/m3) in the group treated with dexmedetomidine and higher (0.00053n/m3)inthegrouptreatedwiththiopentalwhile less(0.00038n/m3)inthecontrolgroup.
Discussion
Inordertocreateexperimentallythemostrealisticcerebral ischemiamodel,varioustechniques22,25 werecreatedfrom variousanimalgroups.21---25Inourstudy,wepreferredtouse ratsforobviousreasonssuchthattheircerebralcirculatory systemisverysimilartothatofhumansandtheyarereadily availableandinexpensive.
Inthisstudy,theneckregionofthesubjectsinthesupine positioninsupinepositionwasshavedandthesterilization ofthesurgicalsitewasachieved.Theirheadswereslightly extendedandthemidlinepretrachealsurgicalincisionwas made.Reachingthetrachea,therightcarotidarteryinthe posterolateralofthetrachea,vagusnerveandcervical sym-pathetic plexus were maintained and then explored and, they were fixed with a suture for being clamped subse-quently.5min afteradministrating 30units ofheparinfor thepurposeofanticoagulation,about3---5mLofbloodwas collectedinacontrolledmannerthroughinjectorfromthe femoral artery in orderto producehemorrhagic hypoten-sion.Carotidarterieswasoccludedwithvascularclampfor a duration of 45min when mean arterial pressure (MAP) reachedto35mmHg.Duringthisperiod,MAPwaskeptfixed at35---40mmHg.Theclampswereremovedattheendofthe periodandbrainreperfusionwasachievedfor90min.
Inclinicalpractice,theimportanceofischemiahasled researchers to create and develop experimental models forcerebral ischemia.Invariousmodelsapplied,wholeor regional,completeorincompleteandpermanentor tempo-raryischemiawereproduced.
Table1 Allsubjects’weights,meanarterialpressures5minbeforeischemiaandduringocclusionandreperfusion,heartrate, bodytemperature,pH,PO2,PCO2,glucoseandhematocritvaluesandtheirstatisticalcomparison.
Variables GroupC(n=10) (Control)
GroupD(n=10) (Dexmedetomidine)
GroupT(n=10) (Thiopental)
pvalue
Weight 308.3±9.9 312.9±13.8 311.3±11.3 >0.05
Meanarterialpressures
Initialvalue 104.9±6.7c,g 105.1±4.1c,g 105.8±5.5c,g >0.05
Occlusion 36.9±3.9f 37.6
±4.1f 37.3
±3.9f >0.05
Reperfusion 96.9±4.4 95.5±5.2 96.1±4.7 >0.05
Heartrate
Initialvalue 329.3±20.4a 324.5±19.2a 332.2±21.1a >0.05
Occlusion 304.6±23.6 304.6±24.9 304.6±28.2 >0.05
Reperfusion 311.2±27.3 311.2±22.8 311.2±26.6 >0.05
Bodytemperature
Initialvalue 37.89±0.17a 37.91±0.14a 37.82±0.11a >0.05
Occlusion 36.92±0.14d 36.09±0.12d 36.71±0.15d >0.05
Reperfusion 37.54±0.10 37.62±0.11 37.72±0.09 >0.05
pH
Initialvalue 7.37±0.03 7.37±0.04 7.38±0.04 >0.05
Occlusion 7.21±0.07 7.23±0.05 7.20±0.06 >0.05
Reperfusion 7.34±0.04 7.35±0.06 7.36±0.07 >0.05
PO2(mmHg)
Initialvalue 92.1±3.3c,g 94.4±3.9c,g 91.9±4.9c,g >0.05
Occlusion 54.2±3.8e 52.9
±4.6e 53.7
±3.6e >0.05
Reperfusion 77.2±4.2 76.8±5.1 77.4±4.4 >0.05
PCO2(mmHg)
Initialvalue 35.7±1.6b,g 36.1±0.9b,g 35.6±1.3b,g >0.05
Occlusion 40.2±1.2d 40.7±1.1d 40.6±0.9d >0.05
Reperfusion 37.5±1.7 37.4±1.6 37.1±1.2 >0.05
Glucose(mg/dL)
Initialvalue 135.4±2.7b,g 137.4
±3.1b,g 138.4
±2.4b,g >0.05
Occlusion 142.9±1.6d 143.8±2.8d 144.1±2.2d >0.05
Reperfusion 139.7±1.9 139.4±2.4 140.7±1.5 >0.05
HCT
Initialvalue 37.4±2.1 37.6±1.9 37.8±2.1 >0.05
Occlusion 37.5±2.4 37.5±2.3 37.5±1.8 >0.05
Reperfusion 38.6±1.9 38.8±2.2 38.5±2.4 >0.05
Significantdifferencesbetweenthevaluesatthebeginningandduringocclusion.ap<0.05,bp<0.01vecp<0.001.
Significantdifferencesbetweenthevaluesduringocclusionandreperfusion.dp<0.05veep<0.01,fp<0.001.
Significantdifferencesbetweenthevaluesatthebeginningandduringreperfusion.gp<0.05,hp<0.01,ip<0.001.
ACMocclusioninratsleadstotheformationoffocal cere-bralischemia followedby a infarct region.ACMocclusion hasbeenwidelyusedsince1975.27Thismodelwasusedfor manytimesin thefocalcerebralischemiastudiesandhas alreadyprovenitself.24---29
In order to eliminate the confusion that may occur during interpretation of theresults obtained from incom-plete cerebral ischemia; the subjects in all three groups receivethesameanestheticagentsuntiltheendofa.carotis unilateralcommunisocclusion(theendofischemia).All sub-jectsinourstudyunderwentisofluraneanesthesiauntilthe end ofunilateral arteriacarotiscommunis occlusiondue to the presence of studies indicating that isoflurane has no
histopathologicallyprotectiveeffectafterincomplete cere-bralischemia.
Grade 3
Histopathological scores
∗
Grade 2
Grade 1
Grade 0
123456789 10
Control group Dexmedetomidine group Thiopenthal group
123456789 10 123456789 10
Figure6 HistopathologicalscoreresultsintheHippocampuscornuammonis1(CA1)Area:Grade0(yellow)=noischemicneurons, Grade1(green)=presenceofischemicneuronslessthan10%,Grade2(blue)=presenceoftheischemicneuronsbetween10and 50%,Grade3(red)=presenceofischemicneuronsmorethan50%(*p<0.01betweenGroupCandGroupDandGroupCandGroupT).
Numerical density Numerical density
0.00039 0.00040 0.00041 0.00042 0.00043 0.00044 0.00045 0.00046 0.00047 0.00048
Control (Group C)
Thiopenthal (Group T) Dexmedetomidine
(Group D)
Figure7 Numerical densityofnecrotic neuron inthe con-trolgroupandthegroupstreatedwithdexmedetomidine and thiopental.
inratswiththiopentalandmethoheksital and pentobarbi-tal controls, Cole etal.14 found that the initial values of pH, PaO2, PaCO2, mean arterialpressure, hematocrit and glucoselevelsweresimilarinall4groupstheystudied.
Ontheotherhand,Drummondetal.11 couldnotdetect any differences in initial physiological parameters of 4 groupsin theirstudies where theycomparedthecerebral protectivepropertiesofetomidate,isoflurane,and thiopen-tal. The above results seem to verify the results of this study.
In this study, the mean arterial pressure, body tem-perature, heart rate, pH and PO2 values were found to significantlydecrease inthe occlusionand raisedagain in thereperfusioninthreegroupswhencomparedtothe ini-tialvalues.However,glucoseandpCO2valueswerefoundto raiseintheocclusionanddecreaseagaininthereperfusion inthreegroupswhencomparedtotheinitialvalues.
Numerical density Numerical density
0.00000 0.00010 0.00020 0.00030 0.00040 0.00050 0.00060
Control (Group C)
Thiopenthal (Group T) Dexmedetomidine
(Group D)
Figure 8 Numerical density of intact neurons in the con-trolgroupandthegroupstreatedwithdexmedetomidineand thiopental.
Kuhmonenetal.30 studiedtheeffectsof dexmedetomi-dine after temporary and permanent occlusion of middle cerebral artery in rats. They administered 0.9% NaCl intravenously to the control group; these researchers reportedthatmeanarterialpressure,PO2andPCO2values decreasedafterischemiainbothtemporaryandpermanent occlusal groups, however, the pH and body temperature remainedthesame.Nevertheless,theyfoundthatthe glu-coseincreased.
neurotransmitter concentrations during cerebral ischemia inrats.Intheirstudies,theydemonstratedthatthemean arterialpressurevaluedecreasedinischemiacomparedits initialvalueandthen,raisedagaininthereperfusion.
Jolkkonen et al.15 researched in their in vitro studies theeffectsofdexmedetomidine,NBQXandCGS-19755after the occlusion and reperfusion of middle cerebral artery accordingtoaninfarctvolume.Theyadministered0.9%NaCl intravenouslytothe control group.They found theinitial valuesofthemeanarterialpressure,PO2,PaCO2,pHandof glucosesimilarinallthefourgroups.Theyalsofoundthat PO2andPaCO2decreasedduringocclusionandreperfusion inall groups whileraisingin thedexmedetomidine group. Theresultsofthisstudyandtheresultsoftheabovestudies werefoundtobepartiallyincompliance.
The cause of the cerebral ischemia is the increase in catecholamine concentration in the circulation and the extracellular space. The inventions reducing sympathetic tonus improves neurological outcome.33,34 Therefore, a treatmentadministeredwithagentsthatreducetherelease of norepinephrineinthe brain(i.e.␣2-agonists)may pro-vide protection against the damaging effects of cerebral ischemia. It has been showed in numerous studies con-ducted,thatdexmedetomidineimproves neuronalsurvival in transient global or focal ischemia in rats.16,30,35 The mechanism concerning the neuroprotective effect of ␣2-agonistsisnotclearyet.Engelhardetal.hasdemonstrated thatdexmedetomidinedoesnotsuppresscerebral extracel-lular catecholamine increase during ischemia and argued thattheneuroprotectiveeffectofdexmedetomidineresults frommodulationofthebalancebetweenproapoptoticand anti-apoptoticproteins.31,32Manystudieshasshownthat ␣2-adrenoceptoragonists decrease the excitatory neurotrans-mitterrelease(i.e.,glutamate).36,37Asisknown,high gluta-matelevelsdepolarizestheneuronalmembraneandallows calcium toget into the cell. Andthis triggers a seriesof eventscausingcellulardamage.Therefore,agentsreducing glutamate release are considered to be neuroprotective. It has been observed that administration of dexmedeto-midine in focal cerebral ischemia reducesinfarct volume by 40% in the cortex, and causes minimal hyperglycemia andhypotension.15Inincompletecerebralischemia,itwas observedthat,throughadministrationofdexmedetomidine, adecreaseoccurredintheplasmacatecholamineleveland histopathologicalimprovementbecamebetterthancontrol, dependingonthedose.16Adecreaseby31%inthecortexand 20%inthestriatumwasreportedintheinfarctvolumeafter transient occlusion (15gkg−1) in rats given a high dose of dexmedetomidine.17 It wasreportedthat, during cere-bral ischemia, circulating catecholamine decreased while noradrenaline and glutamate concentrations in the brain remained unaffected by dexmedetomidine.18 In addition, dexmedetomidinewasreportedtohave aneuroprotective effect in the neonatal period and to prevent excitotoxic lesions in the cortex and white matter.19 Similarly, there are many studies indicating that barbiturates reduce the spreadofbraininjuriaasaresultoftransientfocalcerebral ischemia.Whilesomeresearchershasstatedthatthiopental hasaprotectiveeffect14,20someotherreportedthatithas noprotectiveeffects.21,38
This study wasdesigned to examine whether thiopen-talanddexmedetomidinewhichareamongtheintravenous
anesthetics have cerebral protective effects in focal cerebralischemiainratsandwhichmedicationhasthemost protectiveeffect.
According to the histopathological score, there was ischemia in all subjects in the control group. There was no cerebral ischemia in 4 subjects in the dexmedetomi-dinegroupandin3subjectsinthethiopentalgroup.While Grade 1 cerebral ischemia was present in 2 subjects in thecontrol group and in 4 subjects in the dexmedetomi-dinegroup,itwasobservedin5subjectsinthethiopental group.Grade2cerebralischemiawasfoundtobein3 sub-jectsin the control group and only in one subjectin the dexmedetomidineandthiopentalgroup.Still,Grade3 cere-bralischemiawasfoundtobein3subjectsinthecontrol groupandonlyinonesubjectinthedexmedetomidineand thiopentalgroup.Therewasnostatisticallysignificant dif-ferencebetweendexmedetomidineandthiopentalgroupin termsofhistopathologicalscores.However,therewasa dif-ference between thecontrol group and thesetwo groups (dexmedetomidinegroupandthiopentalgroup).
Cole et al.14 used 6---20 week-old 80 male rats weigh-ing 375---425g in their studies in which they compared thiopental, methoheksital and pentobarbital controls in earlyfocalcerebralischemicinjure.Duringthisstudy,EEG wascontinuouslyrecordedthroughplatinumneedlesplaced on the bitemporal configuration. A two-part medication regimen was administered to rats. This first part of the study (EEG burst-suppression) was performed on 40 rats. Eachgroupconsistedof10rats.0.9%NaClwasadministered intravenously to the controls. As a result of this part, the volumeof cerebral injure wasfound to besimilar in the control group (133±17mm3), in the methoheksital group (126±19mm3) and in the pentobarbital group (130±17mm3). However, a lower cerebral injure volume was detected in the thiopental group (88±14mm3). In otherwords,thiopentalwasobservedtohavethemost pro-tectiveeffectthat reducesthevolumeof cerebral injury. Incontrast,inthesecondpartofthestudyconductedwith barbiturates at a dose of 40%, they significantly reduced onlytheinfarctvolumeofmethoheksitalgroupamongthe groupscreated similarly. Asaresultof thesecond partof thestudy,the volumeof cerebral injure wasfound tobe similarinthecontrolgroup(124±22mm3),inthe thiopen-tal group (118±15mm3) and in the pentobarbital group (121±20mm3).However,alowervolumeofcerebralinjure wasdetectedinthemethoheksitalgroup(70±20mm3).
Elsaesseretal.39 administeredhalothaneto30 Sprague-Dawleyratsbycreatinganocclusionofthemiddlecerebral artery.Theyalsoadministeredintravenouslylowand high-dose thiopental to the other twogroups. They evaluated theinfarctvolumeafter3hofreperfusion.Whenthey com-paredthemwiththecontrols,theyhavefoundthatlow-dose thiopentalreducedtheinfarctvolumeby28%andthe high-dose thiopental reduced the infarct volume by 29%. The authors have indicated that thiopental has cerebral pro-tection and thereis no need for extremely high doses in providingthis.
Xue et al.40 created brain ischemia through oxygen-glucosedeprivation(OGD)modelincerebralcorticalslices inmaleSprague-Dawleyratsweighting90---120g.They com-paredtheeffectsofketamine,midazolam,thiopentaland propofolonthiscerebralischemia.Theevaluatedtheslices by ELISA method. These researchers have found out that these4differentIVanesthetics hasdifferent effects,low andhighdosesofketamineinhibitsOGDInjury,highdoses ofmidazolam(10mol/L)andthiopental(400mol/L) sup-portpartiallythisdecreaseandagain,highdoseofpropofol (100mol/L)alsopromotesthisdecrease.Asaconclusion, theyhavereportedthatketamine,midazolaminhighdoses andthiopentalhaveneuroprotectiveeffectsonOGDinjuria inthecorticalslicesoftherats.
Lianhuaetal.41exposedmaleSprague-Dawleyratsto24h reperfusionand3hmiddlecerebralarteryocclusion.Then, theycomparetheinfarctvolumeinrats’brainsthrough giv-ingthemmidazolam,thiopentalandpropofol.Thediscussed theneurologicaloutcomesovera0---5gradingsystem.They haveobservedthatischemicscorewasrelativelylowinthe ratstowhichmidazolamandpropofolwereadministered. Thus,theyhavereportedthatmidazolamandpropofolhave protectiveeffectsagainstreperfusioninjurybutthiopental showsnoprotectiveeffect.
Inconclusion,wehistopathologicallydiscussedwhether thiopentalanddexmedetomidinewhichareamongthe intra-venousanestheticshavecerebralprotectiveeffectsonfocal cerebralischemiainrats.Wehavedetectedthatthiopental anddexmedetomidinearemoreneuroprotectivecompared tothecontrols.Wehaveshownintheexperimentalmodel of focal cerebral ischemia in rats that dexmedetomidine andthiopentalhavehistopathologicallycerebralprotective effects.However,theclinical accuracy ofthese effectsis not clear yet. Further studies areneeded withregard to theuseofdexmedetomidineandthiopentalinappropriately selectedpatientpopulationsandspecificprocedures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GrahamDI.Focalcerebralinfarction.JCerebBloodFlowMetab. 1988;8:769---73.
2.McIlraithDM,CöteR.Epidemiologyandetiologyofstroke.Curr OpinNeurolNeurosurg.1991;4:31---7.
3.Analysis of neuronal damage resulting in the focal cerebral infarct model induced by middle cerebral artery occlusion in rats and Ginkgo Biloba extract’s effects on this. Bursa:
UludagUniversityFacultyofMedicine,Departmentof Neurol-ogy.ExpertiseThesis;1994.
4.GinsbergMD, Busto R. Rodent models of cerebral ischemia. Stroke.1989;20:1627---42.
5.Garcia JH. Experimental ischemic stroke: a review. Stroke. 1984;15:5---14.
6.GrottaJC.Currentmedicalandsurgicaltherapyfor cerebrovas-culardisease.NEnglJMed.1987;317:1505---16.
7.BarsanWG,BrottTG,OlingerCP,MarlerJR.Earlytreatmentfor acuteischemicstroke.AnnIntMed.1989;111:449---51.
8.AlbersGW,GoldgergMP,ChoiDW.NMDAantagonists:readyfor clinicaltrialinbrainischemia?AnnNeurol.1989;25:398---403.
9.WongMCW, HaleyECJr.Calciumantagonists:stroke therapy comingofage.Stroke.1990;21:494---501.
10.WilliamF.Brainmetabolism.In:CottrellJE,SmithDS,editors. Anesthesia and neurosurgery.third ed. St Louis: Mosby-Year Book;1994.p.1---16.
11.DrummondJC,ShipiroHM.Cerebralphysiology.In:MillerRD, editor.Anesthesia.fourthed.Churchill:Livingstone;1994.p. 689---729.
12.HoffmanWE,Charbel FT,EdelmanG, AusmanJI. Thiopental anddesfluranetreatmentforbrainprotection.Neurosurgery. 1998;43:1050---3.
13.SanoT,PatelPM,DrummondJC,ColeDJ.Acomparisonofthe cerebralprotectiveeffectsofetomidate,thiopentaland isoflu-raneinamodelofforebrainischemiaintherat.AnesthAnalg. 1993;76:990---7.
14.ColeDJ,CrossLM,DrummondJC,etal.Thiopentoneand metho-hexital, butnotpentobarbitone, reduceearlyfocalcerebral ischemicinjuryinrats.CanJAnaesth.2001;48:807---14.
15.JolkkonenJ,PuurunenK,KoistinahoJ,etal.Neuroprotection bythealpha-2adrenoceptoragonist,dexmedetomidine,inrat focalcerebralischemia.EurJPharmacol.1999;372:31---6.
16.Hoffman WE, Kochs E, Werner C, Thomas C, Albrecht RF. Dexmedetomidineimproves neurologicoutcome from incom-pleteischemiaintherat.Reversalbythealpha2adrenergic antagonistatipamezole.Anesthesiology.1991;75:328---32.
17.KuhnomenJ,HaapalinnaA,SiveniusJ.Effectsof dexmedeto-midineonCO2reactivityandcerebralautoregulationinhealthy volunteers.In:ASAmeetingAbstractNumberA-341.2001.
18.LaudenbachV,MantzJ,EvrardP,GrassensP.Dexmedetomidine protectagainstneonatalexitotoxicbraininjury.In:ASAmeeting AbstractNumberA732.2000.
19.Ma D, Hossain M, Franks NP, Maze M. Role of the alpha-2a adrenoceptor subtype in the neuroprotective effect of dexmedetomidine. In: ASA meeting Abstract Number A-832. 2003.
20.SterioDC.Theunbiasedestimationofnumberandsizesof arbi-traryparticlesusingthedissector.JMicrosc.1984;134:127---36.
21.Drummond JC, Cole DJ, Patel PM, Reynolds LW. Focal cerabralischemiaduringanesthesiawithetomidate,isoflurane, orthiopental:a comparison of theextent ofcerabral injury. Neurosurgery.1995;37:472---9.
22.Coyle P. Middle cerebral artery occlusionin the young rat. Stroke.1982;13:855---8.
23.Zervas NT, Hori H, Negora M, et al. Reduction of brain dopamine followingexperimental cerebralischemia. Nature. 1974;247:283---4.
24.HilleredL,HallströmA,SegersuardS,etal.Dynamicsof extra-cellularmetabolitesinthestriatumaftermiddlecerebralartery occlusionintheratmonitoredbyintracerebralmicrodialysis.J CerebBloodFlowMetab.1989;9:607---16.
25.MakarenkoNV.Highernervousactivityindogsreanimatedafter longperiodsofclinicaldeathfromdrowningandlossofblood. ZurnalVyssejNervnojDejatelvnosti.1972;22:82---8.
27.BedersonBJ,PittsHL. Ratmiddlecerebral arteryocclusion; evaluationofthemodelanddevelopmentofaneurologic exam-ination.Stroke.1986;17:472---6.
28.KogureK.Molecularand biochemicaleventswithinthebrain subjectedtocerebralischemia(targetsfortherapeutical inter-vention).ClinNeurosci.1997;4:179---83.
29.IshiyamaT, DohiS,IidaH,WatanabeY, ShimonakaH. Mech-anisms of dexmedetomidine-induced cerebrovascular effects in canine in vivo experiments. Anesth Analg. 1995;81: 1208---15.
30.KuhmonenJ,HaapalinnaA,SiveniusJ.Effectsof dexmedeto-midineaftertransientandpermanentocclusionofthemiddle cerebral artery in the rat. J Neural Transm. 2001;108: 261---71.
31.Engelhard K, Werner C, Kaspar S, et al. Effect of the ␣2
agonist dexmedetomidine on cerebral neurotransmitter con-centrationsduringcerebral ischemiain rats.Anesthesiology. 2002;96:450---7.
32.EngelhardK,WernwerC,KasparS,etal.Theeffectofthe␣2
agonistdexmedetomidineandtheN-methyl-aspartateagonists S+-ketamineontheexpressionofapoptosis-regulatingproteins afterincomplete cerebral ischemia and reperfusion in rats. AnesthAnalg.2003;96:524---31.
33.GlobusMJ,Busto R,Dietrich WD,Martines E,ValdezI, Gins-bergMD.Directevidenceforacuteandmassivenorepinephrine releaseinthehippocampusduringtransientischemia.JCereb BloodFlowMetab.1989;9:892---6.
34.Kuhmonen J, PokornyJ, MiettinenR, et al. Neuroprotective effects ofdexmedetomidine inthegerbilhippocampus after transientglobalischemia.Anesthesiology.1997;87:371---7.
35.MaierC,SteinbergGK,SunGH,ZhiGT,MazeM. Neuroprotec-tionbythe␣2-adrenoceptoragonistdexmedetomidineinafocal
modelofcerebralischemia.Anesthesiology.1993;79:306---12.
36.Chen Y, Zhao Z, Code WE, Hertz L. A correlation between dexmedetomidine-induced biphasic increases in free cyto-soliccalciumconcentrationandenergymetabolismastrocytes. AnesthAnalg.2000;91:353---7.
37.TalkeP,ChenR,ThomasB,etal.Thehemodynamicand adren-ergiceffectsofperioperativedexmedetomidineinfusionafter vascularsurgery.AnesthAnalg.2000;90:834---9.
38.SteenPA,MildeJH, MichenfelderJD. Nobarbiturate protec-tioninadogmodelofcompletecerebralischemia.AnnNeurol. 1979;5:343---9.
39.ElsaesserRS,SchröderM,zausingerS,HungerhuberE, Baeth-mann A, Reulen HJ. EEG burst suppression is not necessary formaximumbarbiturateprotectionintransientfocalcerabral ischemiainarat.JNeurologicalSci.1999;162:14---9.
40.XueQ, YuB,WangZ,etal.Effectsofketamine,midazolam, thiopental,andpropofolonbrainischemiainjuryinratcerebral corticalslices.ActaPharmacolSin.2004;25:115---20.